
Abstract
Increasingly, the adoption and use of radio frequency identification systems in hospital settings is gaining prominence. However, despite the transformative impact that radio frequency identification has in healthcare settings, few studies have examined how and why this change may occur. The purpose of this study is to systematically understand how radio frequency identification can transform work practices in an operational process that directly impacts cost and operational efficiency and indirectly contributes to impacting patient safety and quality of care. We leverage an interdisciplinary framework to explore the contextual characteristics that shape the assimilation of radio frequency identification in healthcare settings. By linking the use of radio frequency identification with specific contextual dimensions in healthcare settings, we provide a data-driven account of how and why radio frequency identification can be useful in inventory management in this setting. In doing so, we also contribute to recent work by information systems scholars who argue for a reconfiguration of conventional assumptions regarding the role of technology in contemporary organizations.
Introduction
As the cost of healthcare continues to rise in the United States, hospitals across the country have investigated different mechanisms for cutting costs in clinical settings. Although the healthcare industry as a whole is notoriously slow to adopt information technology, recent evidence from practitioner literature suggests that this may be changing.1,2 More recently, small- to mid-sized hospitals have acquired sophisticated information technology (IT) systems, such as radio frequency identification (RFID) systems, to reduce costs and improve quality of care. 3 Despite the apparent benefits of deploying RFID technology, its implementation in a hospital setting has not always been seamless. RFID implementation and adoption has been fraught with issues related to high costs, incompatibility with existing hospital systems, and, most notably, resistance to use among doctors, nurses, and other staff members. 4 As a result of these conflicting reports of its usefulness, there exists a rather large gap in our collective understanding of how and why RFID can be beneficial in a healthcare context.
A systematic understanding of how and why RFID systems might, or might not, act as a transformative technology in healthcare settings warrants a keen focus on the contextual characteristics that differentiates healthcare settings from other more general contexts. The healthcare information systems (IS) and health informatics literature have acknowledged the importance of context in investigating healthcare IS–related issues.5–7 In doing so researchers have focused on a variety of topics, including patient-care systems, 8 telemedicine, 9 inventory management, 10 and hospital IS. 11 Among the various research streams within the healthcare IS domain, a group of researchers has also illustrated the difficulties associated with implementing IS in the healthcare context.12,13 Chiasson and Davidson 14 argue that the healthcare context is unique because of the existence of a classic duopoly between administration’s management on one hand and practitioners’ duties on the other, 15 a situation which gives rise to possible tensions between the various centers of power in hospital settings. As a result, inertial forces in the hospital environment become exaggerated, and such complexities have important implications for resistance to change and innovation. In addition, decision-making is often shaped by constraints that are particularly salient in a healthcare setting, such as situational urgency, patient safety, satisfaction, and quality of life issues, that are distinct from typical cost management considerations. 14 This gives rise to the classic problem of optimizing the effectiveness of service delivery (quality) while improving operational efficiency (cost).14,16 Furthermore, the level of compliance necessary to enforce safety standards in healthcare settings is enormous. 14 The healthcare industry, in general, is on the higher side of the institutionalization and regulatory oversight spectrum, 17 making the adherence to regulatory compliance yet another important issue in the healthcare context. 14
Given these considerations, our study focuses on the use of RFID within a bounded set of activities and work processes in the healthcare industry. Namely, we focus on inventory management processes that support the delivery of a particular type of healthcare service, specifically those that exist in cardiac catheterization labs (CCLs) in three large US hospitals. Recognizing the importance of context for understanding the use of IS in healthcare operational processes, we examine the following research question: What are the key contextual characteristics that are relevant to inventory management in healthcare settings? We also recognize that the role that ISs play in enabling certain situational aspects and suppressing others is not always clear. Essentially, the question of how IT interacts with the characteristics of a specific healthcare context remains unanswered. This gap in the existing literature leads to our second research question: How does RFID technology interact with contextual characteristics in healthcare settings?
In order to understand how and why RFID technology is assimilated in healthcare work processes in ways that may be different from other industry and institutional settings—and to highlight those contrasts—we are encouraged by the motivation for applying and the contribution to understanding contextualization offered in Rousseau and Fried. 18 In their article, Rousseau and Fried 18 note that contextual factors need not always be measured quantitatively for contextualization to occur and that the essence of contextualization is the provision of richer description of the research setting to communicate to readers and succeeding researchers the factors that are motivating the researcher’s observations. Below, we outline our approach to contextualizing the assimilation of RFID technology in this study by drawing on concepts from Johns’ 19 framework including the dimensions of context and the reporting of context. Our objective is to identify constructs and depict through rich description how these constructs interact in a healthcare IS context as a foundation for subsequent research that tests hypotheses regarding the influence of contextual variables on organizational attitudes and behaviors in similar settings. In doing so, we provide a data-driven account regarding the efficacy of RFID use within the inventory management function of healthcare providers.
Our article is organized as follows. In the next section, we provide the research background for our study through a review of relevant literature. This section is followed by a discussion of the methodology used in this study and the development of our conceptual model. We conclude by providing a discussion of the study’s findings and the implications for future research.
Research background
Researchers posit that the unique aspects of the healthcare context 13 impact the potential use of IT systems and their accompanying governance structures. 20 One of the primary considerations in a healthcare context is that various groups within the hospital setting can have entrenched self-interests, which can contribute to various social structures and associated politics in the implementation of a new system. For instance, Yajiong et al. 15 showed that hospitals involve a complicated hierarchy that has various governance duopolies and monarchies: top management monarchy, top management–IT duopoly, IT monarchy, administration monarchy, administration–IT duopoly, professional monarchy, and professional–IT duopoly. These social structures can contribute to power-politics not only in the adoption decisions of a new system but also during the implementation (or usage) of it. Findings from Smith et al. 21 also underscore the relevance of social structures and hierarchy in hospitals. The study findings indicate that hospitals that have Chief Information Officers (CIOs) as part of the upper echelons of management are more likely to have a sophisticated electronic medical record (EMR) system. 21 This provides further evidence that the dynamics between various groups in hospitals can play a significant role in the deployment of an IT system.
Contextual constraints in terms of physician involvement and preferences can also play a significant role in influencing the implementation of a new IT system in hospital settings. Kohli et al. 22 conducted a case study of a hospital setting and found that institutional pressures had a great influence on the implementation of a patient profiling system (PPS). They show that physician involvement in the PPS contributed to the collaborative outcomes in the hospital such as improved efficiency of clinical operations and improved patient satisfaction. In addition, prior research also shows that perceived threat to professional autonomy of physicians can have a negative influence on the intention to use the IT system (Walter and Lopez, 2008). 23 Similarly, Hu et al. 24 also show that performance expectancy and effort expectancy explained the physician’s intention to use Clinical Diagnostic Support System (CDSS) and actual use behavior, while social influence marginally impacted physician intention to adopt the system. Angst and Agarwal 25 also highlight the importance of contextual characteristics, as concern for privacy “interacts” with arguments to predict adoption behavior of the system. Similar results extolling the uniqueness of the context affecting physician behavior are also reported by other studies.21,26,27
Furthermore, hospital environments are generally slow to adopt new technology systems and require key capabilities to surmount such inertial forces. 28 For instance, Davidson and Chismar 29 found that technology-related organizational change can only be achieved by aligning two complementary capabilities, namely, social structures (the interdependency, multidisciplinary cooperation and standardization among clinical departments) and technology capabilities in the implementation of a computerized physician order entry system. Taken together, these findings suggest that contextual characteristics could have an impact on specific healthcare-related processes, such as inventory management, and the corresponding IT systems and structures put in place.
Although several studies have documented these broad-ranging contextual characteristics in a healthcare setting, examination of the specific aspects of the context related to inventory management is likely to bring forth new factors. For instance, inventory management involves the interactions of the physicians with the inventory manager, which can reveal issues related to power-politics between them. In addition, inventory management can also reveal issues regarding product availability and utilization and the different perceptions of the stakeholders regarding carrying inventory in hospitals.
Therefore, understanding and documenting the unique contextual characteristics in a hospital setting for inventory management becomes an important consideration. Several researchers contend that studying the “context” surrounding a phenomenon is extremely important for gaining a deeper understanding of that phenomenon.19,30,31 Defined broadly, context refers to the set of environmental, political, and social factors that have the potential to define, shape, and add meaning to the phenomenon of interest.19,30 The theoretical underpinning for studying context in an organizational setting is provided by Johns. 19 In his seminal work, Johns 19 provides an overview of the impacts context has on a particular phenomenon of interest. According to Johns, 19 contextual variables can have different types of impacts on the phenomenon: a context can directly impact the phenomenon (main effect); it can be a part of the causal chain (mediator); or it can increase or decrease the effect of other independent variables (moderator). Contextual variables can enable or inhibit the underlying factors that shape behavior and can have an impact at multiple levels of analysis. In some situations, context can also reverse the causal direction of the hypothesized relationship. Because context can play such a strong role in shaping collective behavior, studying the contextual factors surrounding a particular phenomenon becomes extremely important to understand it fully. We suggest the identification and rich description of these constructs in their unique setting, as a preliminary stage to testing hypotheses including contextual variables.
In this study, we apply two key concepts from Johns 19 to provide a framework for our theorizing about contextual factors: omnibus context and discrete context. Specifically, the dimension of omnibus context provides the background or setting in which the research “story” unfolds. Johns 19 likens the handling of the omnibus context to the journalistic practice of putting a news story in context by recounting who (occupation), what (substantive content of the research), when (time), where (location), and why (rationale). Discrete context, on the other hand, refers to specific situational variables that directly impact (or moderate) organizational behavior, with the most prominent being: task, social, and physical context.
The purpose for applying this framing is to be able to manage the myriad elements that may be perceived as situational factors in understanding behaviors. 19 For example, early behavioral research identified thousands of trait names to describe people, and these have been refined to approximately five dimensions that are important for understanding organizational behaviors; yet, no similar distillation has occurred in the domain of organizational context. 19 We apply these concepts as an approach for structuring situational factors and for linking the more general level, omnibus context with the attitudes and behaviors of the more specific discrete context.
In addition to studying contextual characteristics, this study also seeks to study the interaction of contextual characteristics with the technology used for inventory management. Our specific focus in this study is on the use of RFID-enabled systems for inventory management. RFID has been applied across a wide range of contexts (supply chain management, logistics and retail, healthcare, manufacturing, etc.) and its range of applications continues to grow. 32 Since they are the world’s largest industry, RFID application in healthcare is most promising. 33 It is well understood that RFID has great potential for enabling innovation to occur in healthcare settings, from equipment and device tracking 34 to patient and staff identification,35,36 the potential uses are staggering. In addition to cost savings, an area ripe for improvement through RFID implementation is the prevention of medical incidents and the eradication of medical errors. 32 According to Wharton, 37 lack of quality communication, poor distribution practices, dose miscalculations, device-related problems, and insufficient patient education have all been commonly reported causes of medical malpractice. Recent studies do suggest that RFID may help to resolve some of these issues, 38 but there continues to be a lack of tangible evidence as to how and why such positive change will occur. Several researchers also argue that in order to understand the effects of technology on performance in diverse contexts, the technology’s process-level impacts need to be studied.39,40 Process-level impacts provide a means for understanding the underlying mechanisms through which the impacts of IT are related to performance. Therefore, in addition to understanding the contextual characteristics that impact inventory management practices in CCLs, it is also important to develop a more sophisticated understanding of the mechanisms through which RFID generates value in healthcare settings. To investigate our research questions, our study focused on three case studies, as described below.
Methodology
We adopted a qualitative multi-case study approach so we could explore the phenomenon of interest in a real-life setting. 41 We chose to study our three case sites in a linear fashion while guided by the principles of literal replication. 41 In doing so, we investigated key findings from the initial case in succeeding ones, allowing us to generate more robust and compelling support for our initial findings. To duplicate the design across all case sites, we needed to isolate a specialized service area within hospital settings, one where tasks and procedures would be similar across disparate hospitals. We decided to focus the study in CCLs for a couple of reasons. First, through early exploratory analysis, we learned that when compared to other specialties within hospitals, CCLs are early adopters of technology. Second, when CCL procedures are compared against those that occur in other areas, they are often considered expensive because of the supplies needed (stents, balloons, etc.). Consequently, the inventory management function within CCLs takes on a heightened level of importance relative to other areas within the hospital. To guide our data collection within cases, we were guided by the logic of within-case sampling, 42 which led us to interview individual decision-makers and users of RFID system (e.g. supply coordinators, purchasing managers, and technology specialists), along with those responsible for service delivery (e.g. nurses) in the CCLs.
Data collection
We utilized three data collection techniques to ensure that our findings maintained adequate validity.41,42 Semi-structured interviews were the primary source of data. We first conducted exploratory interviews with C-Level executives from an RFID solution provider. This enabled us to get a general lay of the land and understand at a deeper level the RFID technology that was being offered within hospital settings. After initial meetings, one executive became our project liaison, helping us to identify case sites and individuals within the organizations that could help us explore our research questions. Prior to conducting individual interviews, the project liaison obtained consent from the subjects after informing them of the study’s intent. Interviewees consent was validated through email when interview dates were coordinated and verbally at the beginning of each interview by the researchers, and their anonymity was guaranteed to protect confidentiality.
After initial discussions with key members from the solution provider, we identified our first case site, a CCL in a large Northeastern hospital. For literal replication, we wanted subsequent CCLs to be of a similar size and complexity. The second case site took place in a large Midwestern hospital; the final site was a large CCL in the Southeastern United States. Table 1 provides an overview of the organizations and the generic interviewee roles within each organization.
Overview of organizations and interviewees.
During interviews, the interviewees were asked to provide retrospective accounts of their experiences working with both barcode and RFID systems within the CCL. Our questioning was shaped by a semi-structured interview protocol that was designed to encourage open conversation related to specifics of the CCL context and how RFID seemed to impact work practices and process performance as compared to the barcode technology. Our protocol consisted of both targeted and open-ended questions, aimed at enabling the interviewees to effectively recall experiences while embedded in the CCL context. Other than initial conversations with the RFID provider, interviews lasted between 45 min and 1 h. A summary of questions from the interview protocol and their relation to major constructs in this study are provided in Table 2.
Protocol for data collection.
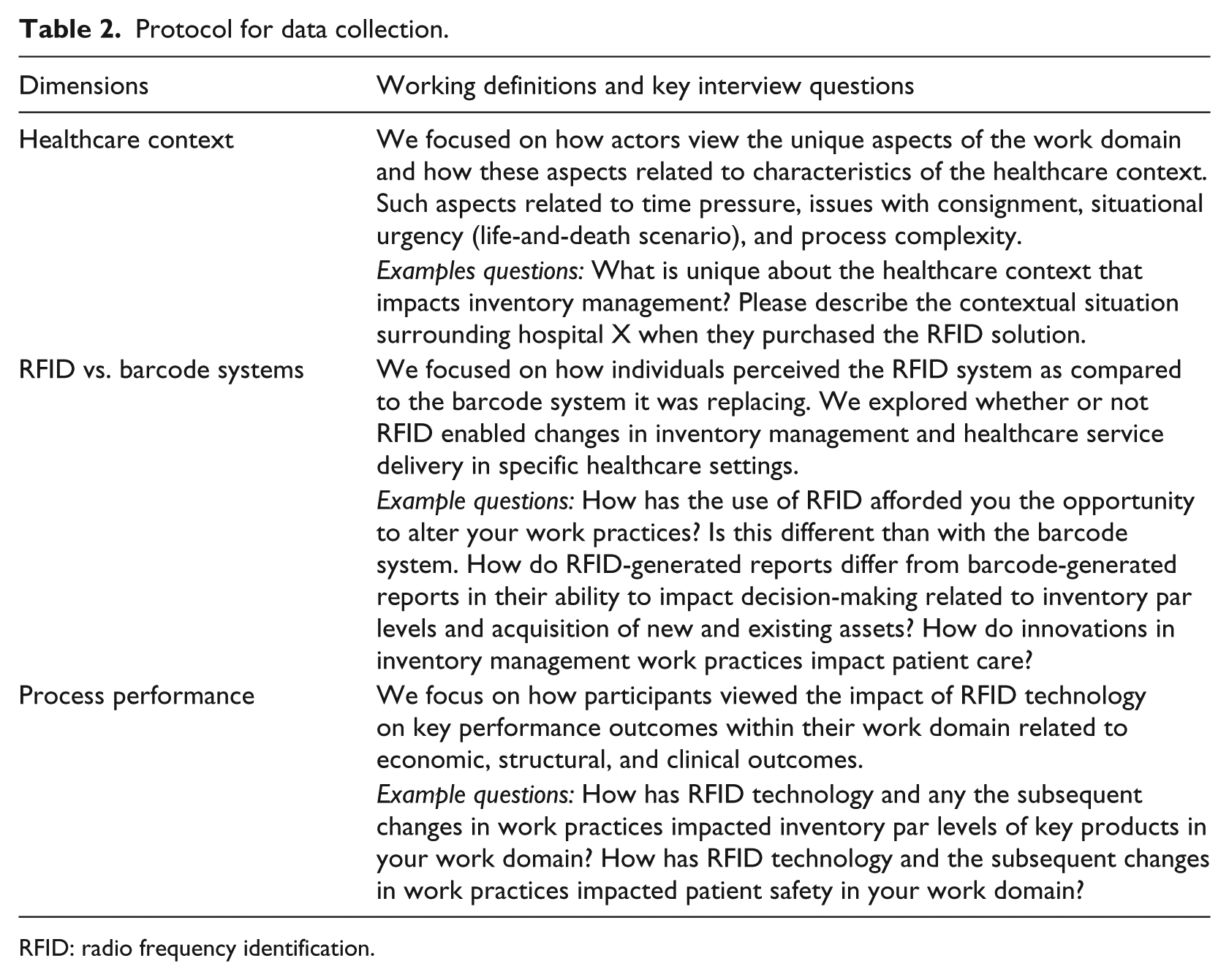
RFID: radio frequency identification.
To complement our interview data and enable triangulation during data analysis, we utilized direct observation.41,43 Direct observation was particularly useful because it allowed us to observe firsthand how the RFID system was used in the CCLs, how it changed inventory management practices that were previously supported solely by the barcode technology, and how inventory management practices were connected to CCL procedures. Direct observation is particularly useful for ensuring what people say during interviews is actually what they do in practice. Finally, we leveraged archival data to supplement our interview and observational data and to enhance validity of findings.
Data analysis
Both inductive and deductive coding techniques were used as part of a hybrid qualitative data analysis technique aimed at generating rich insight.14,44 The interviews were conducted by two of the authors. After each interview, they met in recap sessions to capture key insights and major themes that were discovered during the session. To get outside opinion and one that was not biased from the interview and observation experience, the other author was presented with the key insights and themes and offered his critique by referencing key theoretical points generated from the literature. In an iterative fashion, the research team read, coded, listened to, and discussed the data. 45 Doing so allowed the researchers to continuously alternate between the data and the thematic codes that were generated,42,45 while ensuring that we remained open to disconfirming evidence that was illuminated during ongoing discussion and reflection. We also circled back with the project liaison to validate findings as they were generated. Given the extensive experience within the hospital setting, insights of the project liaison proved valuable for helping us develop deep contextual understanding. At the conclusion of our inductive analysis, we isolated key contextual factors that were specific to CCLs and that challenged the inventory management function within this area. We then applied our deductive “contextual” frames as a means for making sense of our data-driven insights, which provided a means for organizing our findings as well as helping us to generate deeper understanding. At the conclusion of the inductive stage of analysis, it was clear that contextual factors specific to CCLs were exacerbating the tensions faced by the inventory management functions, but it was also clear that RFID technology was playing a role in mitigating these negative forces. In the final stage of analysis, we focused our attention on the unique aspects of the RFID technology as our object of inquiry, relative to barcode, to explore how such technological properties interacted with the contextual forces that were deemed responsible for bloating inventory within the CCLs. The combination of inductive and deductive analytical techniques led to the key findings that follow.
Case findings
In this section, we explore our research questions in the context of CCLs across three distinct hospitals in the United States.
Healthcare context
To explore our first research question, what are the key contextual characteristics that are relevant to inventory management in healthcare settings, we draw on the work of Johns 19 who offers two distinct dimensions of context. The first, the omnibus context, can be considered a higher order construct, as it operates at a higher level of analysis and comprises many features or aspects. Second, the discrete context refers to “the particular contextual variables or levers that shape behavior and attitudes” (p. 391). Together, both dimensions work in a tandem relationship to link the more general contextual attributes with the more specific contextual attributes. 19 The multi-dimensional contextual framework proved useful for our study, as it helped to classify our contextual findings at two levels.
Omnibus context—CCLs
According to Johns, 19 one should adopt a journalistic mentality when describing the omnibus dimensions of a context—describing who, where, when, and why. We used Johns’ framework to identify the relevant stakeholders who interacted with the inventory management functions. We found that across all three cases, there were similar job roles, though not identical, that were associated with such functions. In each case, there was one individual strictly responsible for inventory in the CCL. These individuals reported to business managers who oversaw the operational aspects of each laboratory, which was another common role across all cases. However, in two of the cases, this individual had broader responsibilities and was charged with managing the entire cardiovascular services area across a larger hospital network. To these managers, inventory management was one component of a much broader responsibility. For instance, these managers were not only responsible for ensuring that the requisite products were in the right place at the right time but also they were tasked with negotiating purchasing and consignment agreements with vendors.
We performed our study in three CCLs across the United States. Typically, CCLs use minimally invasive techniques to perform diagnostic procedures for treating vascular diseases. However, each device used in a procedure can easily be worth several thousand dollars, which explains why inventory management is so crucial for improving the financial performance of CCLs. A nurse from one hospital provided a more thorough explanation of what happened in CCLs:
These procedures are catheter-based. Access into a blood vessel, usually the femoral artery in the groin, is obtained by inserting a hollow needle into the blood vessel. A thin wire, usually 0.35–0.38″ in diameter is passed through the needle. A catheter, which is a hollow tube of varying lengths, shapes and size is placed over this guide wire and manipulated to the specific blood vessel that is to be studied. In the case of the CCL, this is most often the arteries that supply blood to the heart muscle.
Across all cases and interviews, one central theme was constant: namely, that CCLs deal with situations that put great pressure on every individual who is either directly or indirectly involved with inventory management in CCLs. As a Director of Supply Chain Management (SCM) commented:
Try to imagine you’re in a life-and-death situation. You’re the doctor; you’re the clinical person, attending. You know the person or patient needs this device. Had it been without that issue, it’s so easy to walk to the cabinets and grab the device. But I’ve observed, it’s a different scenario when there is this critical need. You would see … the blood rush that you must find that device.
Discrete context—task variability, social structure, and physical separation
Discrete contextual variables provide a link between the general omnibus characteristics and actual organizational behaviors and attitudes. 19 When we searched for actual examples of how the general context shapes behaviors that impact the inventory management function, we found recurring themes across the cases. When using Johns’ 19 dimensions of context as a sensitizing device to interpret our data, we were able to align our observations with his salient dimensions of discrete context, including task, social, and physical contexts.
Task variability (patient, procedure, and product)
We learned early on in our investigation that the inventory management function in CCLs has one core purpose: to ensure that doctors have the right supplies, at the right time and in the right location. In light of the life-or-death omnibus context in which our interviewees operated, we wanted to develop deeper insight into the factors that impacted their objectives in terms of products, time, and place. Our findings suggest that there were three key drivers of variability that impacted their ability to optimize inventory or balance their objectives with the need to lower costs. First, there appeared to be significant patient variability or changes in the number of specific patient procedures that would be performed on any given day. An inventory manager commented in regard to a recent experience:
The day started with 10 cases planned, we ended with 22 … so 12 cases were added on that day. There is a lot of variability in what we do.
The second factor related to procedural variability or distinctions in the type of procedure performed on a patient. Doctors are motivated in enhancing their clinical outcomes through innovative practices. As newer treatment options and techniques are preferred, the variability in the procedures becomes more pronounced in hospital settings. This contributes to issues regarding carrying a variety of medical devices. As another Director of SCM mentioned:
As the doctors keep on the cutting edge of the procedures, the complexity of the procedures increases. The supplies have grown much more than they used to be. For example, when we do a coronary angiogram—which is just a diagnostic angiogram—the supplies required for that are relatively cheap and are going to be fairly limited. But as we evolve into the angioplasty, those supplies have just boomeranged, and 90% of the CCL budget is supplies.
A technology specialist for one hospital reiterated this point when she distinguished the CCL from other areas of the hospital. She commented:
CCL is unique in the fact that not only do we have syringes, Band-Aids and needles to treat our patients, but we have catheters and stents and balloons and pacemaker devices and lots of interventional items … you go to surgery and the doctor opens a set of instruments, he goes in and takes out your gall bladder and you’re done.
The third factor that impacts the inventory manager’s ability to right size inventory relates to product variability. Product variability refers to the distinctiveness within a particular brand of a supply that a doctor can use during a procedure. Doctors have well-established preferences about the type of products that they would prefer to use during a particular procedure. However, the preference among different brands is likely to evolve over time and could be governed by intrinsic factors such as a doctor’s own research activities, as well as extrinsic factors such as industry preferences and hospital recommendations. Our findings suggest that initiatives to engage in vendor-sponsored research studies contribute to product variability, as there is a positive correlation between product variability and the number of studies they participate in. The same technology specialist commented:
We’re involved in a lot of research studies here, clinical research studies, so our physicians are well versed in all new technologies coming out and new drugs coming out and that kind of thing. Well, the down side to that is, you can have a lot of vendors in the lab and the downside of that is that you can have a lot of supplies.
In other words, vendor-sponsored studies provide doctors exposure to cutting-edge technologies and medical devices. Such exposure provides the clinicians with the opportunity to include innovative technologies and devices in their work practices. Therefore, as the preferences regarding medical devices continuously evolve due to more exposure, it has a direct influence on the variety of products carried in the inventory.
Social structure (power asymmetries)
Social structure is a key contextual dimension that was illuminated in Johns’
19
framework and evident in our findings. It manifested in terms of social influence across cases in two key ways: power asymmetry between doctors and between those responsible for managing inventory in the CCLs. It was clear throughout our investigation that there was a distinct ingroup/outgroup status between these social groups. As expected, those responsible for inventory management seemed to be focused on meeting the perceived needs of the doctors, even if they did not agree with them at times. An inventory manager highlights such a relationship:
I have a medical director that gives us medical direction for what we need to do. His favorite expression is “he’s the quarterback and it’s my job to catch the ball.” I keep trying to tell him there’s going to be a quarterback sack someday.
As a result of this power asymmetry between doctors and staff, inventory managers often find themselves in a position of reacting to the needs of the physicians rather than making decisions that are best for the organization. There is a distinct lack of a trusting relationship between the physicians and the inventory managers. The general sense that pervades in such situations is one of behaviors modeled after self-interests, which translates to equations of power-politics rather than trust-collaboration between the stakeholders. Although power-politics exist, there appears to be a consensus on the role and ability of inventory managers to make effective inventory decisions. Since inventory managers often have less biased positions, more access to useful data, and likely more time than doctors, they are often in a better position to make effective inventory decisions. However, the real or perceived power differentials between the physicians and the inventory managers, and the associated self-interests act as a major stumbling block and attenuate an inventory manager’s ability to make optimum inventory decisions.
Physical separation (product placement and procedural execution)
Johns
19
acknowledges a growing awareness by management scholars that the effect of the physical world on collective behavior is understudied in organizational research. Our findings illuminate the importance of paying attention to the physical context, as we continually detected the interrelationship between product placement and the execution of clinical procedures. For instance, a Director of SCM commented on the impact of physical location on the quality of care:
One of our focuses has been: How can we improve the delivery of care from a quality perspective? And my contribution to that can be limiting the number of times an employee leaves the room to gather products for this case.
One of the core objectives of inventory management is not only to have the right products in the inventory but also to ensure their availability at the right place and right time. As physicians seek product variety, the amount of products carried in close proximity to the operating table becomes increasingly difficult to manage. Often times, products that are essential are placed in further away cabinets from the operating room. This type of product placement runs counter to the tenets of good inventory management in hospitals. Therefore, procedural and product variability not only have a direct influence on inventory management practices but also indirectly influence product placement decisions, leading to significant pain points for inventory managers.
Influences of IT
Our second research question is focused on investigating the pathways that connect IT systems and performance.39,40,47 We realized early on in our investigation that there was an interesting distinction that needed to be understood. On the surface there seemed to be only slight differences between the RFID systems and the barcode technology that they replaced. Yet, we also detected major shifts in behavior that occurred across all three sites, which were seemingly the result of ongoing interactions with the new technology. We investigated what the real distinctions were, to understand why they were shaping these new behaviors. Instead of simply focusing on the technology itself, we sought to examine the complex linkages between the contextual dimensions which were identified through the investigation of our first research question, human action, and the technological systems under investigation. Through this analysis, we were able to uncover distinct differences between the RFID and barcode technologies, which helped to explain the performance improvements that were seen in each of the three sites.
Influence on task variability—automation versus manual processes
At a first glance, both RFID and barcode systems appear to have similar technological capabilities. Both these systems store information in electronically readable formats, use readers for accessing the information stores, and can be linked with database systems to capture live usage behaviors for further analysis. However, the fundamental capabilities enabled by these two systems are drastically different.
Barcode systems are line-of-sight technologies and require that the reader be placed in front of the code to be read. RFID systems work through RFID, thereby placing no such constraints on reader placement. Inventory managers and nurses do not need to scan each and every item they store or retrieve from shelves because the system automatically tracks such storage and retrieval. Even this relatively simple shift in the readability of codes between barcodes and RFID tags frees up valuable time and effort for inventory managers and nurses and has contributed significantly to labor savings. 48
RFID systems also provide higher order information visibility. While barcode systems demand constant manual inventory checking because managers cannot rely on workers accurately decrementing products during actual procedures, RFID systems provide automated, round-the-clock tracking of inventory. This information visibility can be used by inventory managers to make important decisions apart from checking inventory. 48 They can also be used for understanding and modifying inventory stock levels, solving inventory discrepancy problems, visualizing demand situations for patients based on usage patterns, and proactively predicting future trends.
Impact on task variability—real-time versus time-delayed representation
Compared to barcode systems which were passive technologies, the RFID system we investigated automatically counts inventory multiple times per day, creating the perception of real-time visibility of the products that were on hand, missing or nearing expiration. As individuals viewed the reports that were generated through the RFID system, they described feeling as though they were viewing the actual inventory through a digital lens. In fact, because of this new perception, they began to develop insight into how the inventory had changed over time. For instance, a Director of SCM commented:
But with the RFID technology—since it’s real time—it’s easy for him to go to the system, see what we have and see the movements of the product. That way, when he speaks with a vendor he can negotiate for volume and price.
As an example, an inventory manager commented:
I’ve been able to show them (vendors), because of consistent growth, that perhaps we should look at a consignment program …. So what we came to a resolution on, in that particular situation, was a shared program. You consign 50%. I’ll purchase 50%.
Therefore, pricing decisions with vendors, which are often hard to bargain, become increasingly easier due to the implementation of the RFID technology. In addition to offering an interesting counterpoint in negotiations, RFID systems also accurately reflect the clinical practice. Trends in the movement of products are accurately mapped, which helps the inventory manager respond proactively.
While continuing to probe these issues across the three cases, we noted that the RFID systems generated completely different perceptions of their impact on work processes and outcomes. If the barcode system was perceived to be used effectively (so that products were incremented and decremented when placed on or removed from a shelf), the data generated by that system would be nearly identical to that generated from the RFID system. Yet, both clinical and non-clinical staff perceived their interactions and outcomes to be different despite a high degree of correlation between the data generated by the two systems.
Influence on social structures
Our early findings revealed that individuals on the non-clinical side of the CCL were often in power struggles with two main constituencies that held positions of social influence: doctors and vendors. Consequently, we sought to explore how the use of RFID versus barcode systems influenced these relationships. Our findings indicate that compared to barcode systems, the information generated by the RFID systems gave the clinical staff confidence to approach and negotiate with the doctors and vendors. For instance, another inventory manager commented:
Sometimes I have to be the impetus for the change, or go to the physicians and say, “You know, based on your trend or the practice here, maybe we can try looking at another product category, or what do you think about this?”
A Director of SCM commented:
I had a physician come to me and request a product that he thought he needed. Yet, in looking at actual usage, I was able to show him that he hadn’t actually used that product in six months. This kept us from carrying a product that we didn’t even need.
Similarly, the Director of SCM for one hospital discussed how the technology is enabling her to interact with new vendors:
I did a report on usage and he’s (the vendor) coming back next week … he has to swap them (stints) out, so it frees up shelf space for product to come in from a new vendor.
While duopolies are consistently mentioned in extant research as one of the key contextual characteristics in hospitals, RFID systems provide a pathway for the inventory managers to build relationships with physicians. Clarifying the actual usage through the trends shown by the RFID system helps the physicians dispel any misconceptions regarding the intentions of the inventory managers. This helps reduce the power asymmetries between the physicians and the inventory managers, thereby helping in developing a more trusting relationship between them.
An important finding that emerges from these interactions is that inventory managers utilize RFID systems as a “mediator” of their relationship with the physicians. By way of common consensus on the features of the RFID system, inventory managers and physicians can coalesce around a common trusting theme, forgoing issues of entrenched self-interests. The RFID system, therefore, serves as an essential construct of change in the social structures in the hospital setting.
Influence on physical context
In the course of interviews and data analysis, we began to investigate how (if at all) the RFID systems influenced the relationship between human action and the inventory itself. Thus, we wanted to see whether and how the RFID technology allowed the physical location of inventory to be adjusted or moved in an effort to mitigate the effect of the physical context on operational processes. We found that RFID did have an impact, one that was a distinguishing feature compared to barcode systems and one that is likely to become more important in the near future, as new product innovations begin to enter the market. For instance, one hospital was beginning to pilot the use of mobile cabinets that could be easily moved around the CCL facility. By leveraging wireless technology, the mobile cabinet could continue to monitor inventory often and send updates to a central server wirelessly. Interestingly, the hospitals did not think that adding wireless cabinets would add to their existing fleet of stationary ones. Instead, as a Director of SCM suggested:
We’re not going to add cabinets. We are going to rationalize on how we use the system, and we just need to cut that number of cabinets in there. That way it will finance the mobile carts.
By being able to move supplies around, they were able to get better service while not requiring any additional inventory. Furthermore, the Director of SCM commented on how the mobile cabinets would allow them to put supplies closer to the patients, which would be especially beneficial for those in the direst circumstances. He said:
When you have a critically ill patient there is X amount of time from the time they pick up the patient until he is treated that must be met. That way, nothing bad is going to happen to the patient … there are some situations where if you fail to give the best medical attention, the patient’s brain or nerve or heart might be affected. So you have to meet that standard. So [the mobile cabinets] will be key for us to deliver that type of critical care.
Implications for healthcare settings
The primary objective of our research study is to explore the fundamental influences of the RFID-enabled systems in healthcare, looking specifically at one process—inventory management in CCLs. Through our literature review, we identified potential gaps in research. First, we sought to gain a thorough understanding of the “contextual issues” in our research, encouraged by the call of several researchers.19,30,49 Second, we sought to fill an important gap in the literature by gaining a thorough understanding of the interaction of RFID systems with the identified contextual dimensions in healthcare. Although prior research has advanced the notion of the interaction of systems and context, a systematic examination of the process by which such impacts occur—especially in the healthcare context—has not been given due consideration.
Consistent with the definitions of the omnibus and discrete context, 19 our findings indicate that contextual characteristics impact the inventory management process through multiple modalities (see Figure 1). At the omnibus context level, situational urgency places enormous burden on the inventory management function. This becomes especially salient in situations when personnel are tagged with multiple activities. For instance, nurses could be responsible for not only assisting in a procedure in an operating room but also removing inventory from cabinets. This dual-role expectation could exacerbate the already existing tensions related to life-and-death situations in hospital settings. At the discrete context level, task variability, social influence, and physical separation have enormous impacts on the inventory management function. Several different procedures could be performed in hospitals, even on the same day. Such increase in procedural (task) variability in turn increases the complexity in the inventory management function. Similarly, the existence of administration–practitioner duopoly15,50 and the resulting power asymmetry are found to play an important role in the ordering, placement, and utilization of inventory in hospitals. Our contribution to this extant research is in examining and documenting the specific contextual characteristics influencing inventory management in hospital settings. In addressing our second research question, we sought to examine how contextual characteristics and RFID systems interacted in practice. Prior research shows that RFID-enabled systems and their capabilities, arguably, can improve inventory management in specialty hospital settings. Such settings relate to practice areas where high-risk procedures are conducted and high-value (greater than US $2000) products are likely used. This is based on the fundamental premise that organizations can leverage the functionalities of IT resources to create capabilities, such as innovating business processes, shaping new strategy, and extending the enterprise network.39,51
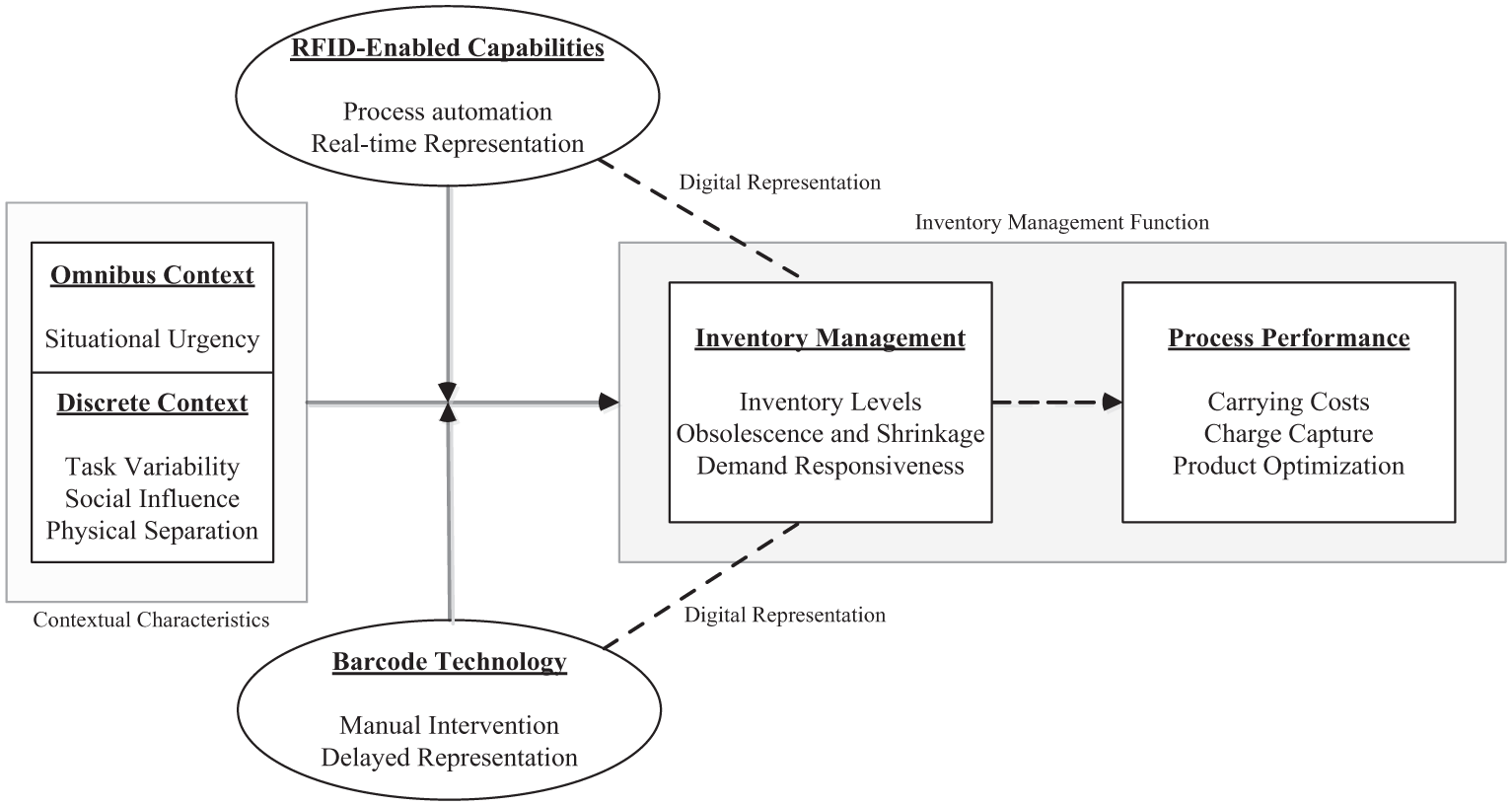
Conceptual model—context, information technology, and process performance.
Our research study shows that using RFID in hospital settings, the collection of information across activities—including those that are coordinated within a specialty process (such as CCLs)—is automated. This may impact work practices in the hospital setting, because it may increase reliability in the representation of information as compared to other legacy systems such as barcode technologies. As a result of the limited human intervention necessary for information collection, materials’ managers could potentially get a near real-time digital representation of material flow within practice areas. This newfound visibility may help mitigate the negative impacts of context such as power asymmetry and physical separation. By implementing RFID systems in the inventory management process, inventory managers may be better able to make important inventory decisions, effect better negotiations with partners, and highlight inventory usage details with their doctors and nurses. This information trait has helped the three hospitals in our study by consistently decreasing their inventory levels and inventory shrinkage and increasing their demand responsiveness. 48 In doing so, it has enabled hospitals to reduce carrying costs, increase charge capture rates, and ensure inventory is aligned to demand through product optimization. In addition, the implementation of the RFID system challenges the existing duopolies in the hospital setting, acting as a mediator of the relationship between the physicians and the inventory managers. In addition to serving as a construct of change, RFID systems also act as an effective counterpoint in the negotiations with vendors. Therefore, inventory managers are better equipped to discuss pricing decisions with vendors, providing effective savings for the hospitals. A key contribution from this study is in highlighting the role played by RFID systems in influencing social structures in hospitals.
Although our study makes important contributions, it has specific limitations. First, we drew on retrospective accounts of organizational situations from our interviewees. Such accounts can be subject to cognitive biases about what really happened in a particular situation. To address this concern, we tried to corroborate findings by interviewing multiple individuals about the same situation and collecting multiple types of data. Nevertheless, retrospective accounts can lead to confounded findings. Second, the choice of case study methodology and the nature of our research questions may impact the generalizability of our results. Although our results can inform future healthcare IS researchers, future studies that adopt new methods with larger sample sizes may provide a deeper explanation into the complicated linkages that connect IT use and process performance in distinct contexts.
Conclusion
Our findings provide practicing managers with important suggestions for improving their business practices. First, from the perspective of vendors of RFID solutions, we have provided a more detailed account of how RFID can be useful in hospital settings. By tying these observations to quantitative measures, managers can develop a more sophisticated model to explain the return on investment from RFID technology. Second, from the perspective of the inventory manager in a CCL, we have explicated and categorized the contextual dimensions that impact the inventory management function in these areas. In a sense, we have identified and described key levers that need to be paid attention too, so that technology can be used more effectively to adjust the task, social, and physical dimensions of a given context. These findings can assist managers as they seek to design more focused interventions to mitigate these potentially significant forces. Our study also provides avenues for future healthcare research, as it begins to discern the influences of context on how healthcare IT can create value in specific contexts. In doing so, we have begun to examine the black box that separates technology from the human aspects of organizing and have provided a context-based narrative to develop a deeper understanding of the linkages that impact the assimilation of RFID systems in urgent care setting.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.