
Abstract
Visual approaches to health information reduce complexity and may bridge challenges in health literacy. But the mechanisms and meanings of using animated video in communication with patients undergoing surgery are not well described. By comparing two versions of a two-dimensional animated video on spinal anesthesia, this study tested the patient–avatar identification within two different narrative models. To explore the perspectives of total hip arthroplasty, we employed qualitative methods of interviews and ethnographic observation. The animated presentation of the spinal anesthesia procedure was immediately recognized by all participants as reflecting their experience of the procedure independent of the narrative form. The avatar gender did not affect this identification. We found no preference for either narrative form. This study supports the potential of animation video in health informatics as a didactic model for qualifying patient behavior. Animation video creates a high degree of identification that may work to reduce pre-surgical anxiety.
Keywords
Introduction
Health informatics using virtually mediated expressions has a potential to transform learning in the health care sector. New social technologies and animations are virtual mediations that create new opportunities for therapeutic and behavioral intervention with a positive impact on patient empowerment, engagement, knowledge and self-efficacy.1–7
Surgical patients in particular, patients undergoing fast-track procedures, experience increasing demands for patient engagement,8,9 which consequently places high educational, physical and mental demands on the patients. Extensive preoperative information has shown to enhance the patients’ knowledge, their quality of life and satisfaction with treatment; reduce preoperative anxiety; improve preoperative anesthesia procedure and reduce postoperative use of analgesic.10–15 However, low health literacy may be a barrier in providing sufficient information and care. 16 Communicational interventions in surgical settings should take this into account, which was a key objective for working with animation video in this study.
In surgical patients, preoperative Internet-based education, instructional digital videos and animation videos have been shown to enhance patients’ operative experience as well as increase the retained knowledge and sufficiency of knowledge in patients irrespective of health literacy3,17–20 and patient preparedness for engaging in postoperative care activities. 21 A recent randomized controlled trial (RCT) documents a reduction in preoperative anxiety in bowel surgical patients watching a two-dimensional (2D) animation video information. 2 The visual approach in animated health education optimizes the acquisition of knowledge in the patient by reducing the complexity of the information 3 and has been found to reduce anxiety and prepare patients for the operating procedures.2,22 A recent RCT study in diabetes patients found health information delivered by animation video to increase the acquisition of knowledge on diabetes health in patients with inadequate health literacy. 23
Animation videos employ advertising techniques such as color, size and music to positively affect the patients’ attentiveness to the displayed information and their production of knowledge.21,24 In comparison with traditional photographic video-assisted patient education, animation videos have the ability to visually highlight the important points of a given procedure or mechanism 3 and be more acceptable to patients who do not wish to watch realistic depictions of medical interventions.3,25 Through the visual presentations in animation videos, patients adapt images of given procedures or health behaviors that support their understanding of these given procedures or behaviors. It is still unclear how this affects knowledge retention in patients. 2 However, previous work on the use of animation in teaching complex processes has shown increased knowledge retention in students. 26
Little is known, however, of the mechanisms and meanings of virtually mediated and animated communication with patients. In response to the increasing educational, physical and psychological demands placed on patients undergoing fast-track surgery, the Elective Surgery Centre at Silkeborg Regional Hospital developed and introduced an animation video on a web-based platform to patients undergoing first-time total hip arthroplasty (THA) surgery, describing the procedure of fast-track THA and with information and directions for postoperative physical exercise at home. The effect of that intervention is currently being studied.
To supplement that inquiry, this study aimed to address the existing knowledge gap on the mechanisms and meanings of virtually mediated and animated educational interactions with THA patients, serving as a feasibility study for developing future patient information interventions using animation video. Particular attention was given to the meaning of patient–avatar identification. Hereby, we explored how the experience of spinal anesthesia conveyed by the avatar in the animation video was recognized by and resonated with the experience of patients. This sought to elucidate the potential of using targeted avatar communication in animation videos in patient education in fast-track surgical procedures to produce experience-based knowledge in the patients that may be able to counter or reduce preoperative anxiety in relation to THA procedures.
Theoretical framework
The virtual space, independent of its technological shape, is characterized by the possibility to navigate the borderlands between the actual and the potential. 27 In the context of animation videos in patient information, the animated avatars in a video express deliberations and behaviors, which resonates with the actual circumstance and conditions of patients’ everyday life. The virtual space of the animated video in this way holds the possibility to mediate the difference between the actual circumstances of a patient (e.g. a state of illness or pain) and a potentially new situation, where the patient has the opportunity to perform actions that are not possible within the actual everyday frame. The virtual space is therefore a potentially unique learning space, where the understanding of correlations and possibilities may be taught and challenged. This thinking draws on ideas from social learning theory, 28 to propose the animated avatars in patient communication as models for patient behavior through “vicarious reinforcement.” 28 This vicarious reinforcement stimulated by animated avatars in patient information is central to the potential for their use. In this sense, it is not learning by doing but learning by observing how one reacts to animated depictions of actual life, rather than actual life as such. 29
Furthermore, we draw on existential theories of storytelling as an intersubjective intersection between the public discourse and the private experience. 30 Patients do make decisions based on factual knowledge, but personal experience information from others is broadly used to identify possibilities, assess and choose between such possibilities and support coping strategies. 31 Fast-track surgery, though, challenges the possibility for interaction between patients, as they hardly get a chance to meet other patients through their short admission to hospital. The animated avatar may have a particular potential as a model for engaging the personal experience information in patient communication as a kind of peer-tutoring.
By employing these theories, we sought to translate existing understandings of the use and meaning of personal experience information between patients to the mediated interaction of patient experience through animated avatars. This was understood as the framework for producing social learning, as a basis for the learning and empowerment of patients by an animation video prior to a large, elective surgical intervention.
Method
Design and setting
We employed qualitative methods of interviews and ethnographic observation. Initially drawing on data from previous ethnographic work carried out among THA patients in the centre, we identified the lack of personal experience conversation between patients in fast-track procedures as an area of interest for our study to work with the narrative form in the animation videos and test patient experience information in relation to existing animated information. Information on spinal anesthesia was selected as the case in focus for developing and testing the use of different narrative models in animated video patient education, as it is known to be a procedure associated with a high level of anxiety in orthopedic patients.32–36
The study was approved by the Danish Data Protection Agency (No. 1-16-02-278-13) and by the Regional Research Ethical Committee (No. 1-10-72-197-13).
Animation video
The existing animation video used with THA patients in the Elective Surgery Centre was further developed and used for this test. The 2D animation video is a 12-min film consisting of 10 sequences explaining the THA surgery procedure from initial symptoms to post-surgical rehabilitation at home. The animation video shows a patient avatar as a middle-aged woman going through THA surgery (Figures 1 and 2) while a male voice speaker explains about the procedures.

The avatar model—the animation anesthesia study, Silkeborg Regional Hospital, Denmark, 2013.

Pre-surgical, anesthetic interaction between avatar patient and avatar health providers—the animation anesthesia study, Silkeborg Regional Hospital, Denmark, 2013.
Two 2-minute animation videos focusing on the sequence of spinal anesthesia were tested with 15 persons in this study—the original with a general narrative model, described above, and a new animation video with a patient experience narrative model. Both had the same length and used the same 2D animation sequence of spinal anesthesia; only the narrative shared in the video was different. Since the avatar is a middle-aged woman, the speaker in the patient experience narrative was a female of the appropriate age.
Sampling
Since use of the full animation video employing the general narrative was implemented in the clinic from May 2013, participants for this study were recruited among persons who had undergone THA surgery prior to that date. THA patients undergoing a first-time THA surgery early June 2012 through April 2013 and who were included in an ongoing mixed-methods study in this period were eligible for our study (n = 120).
From this group, those who had been interviewed for the mixed-methods study were excluded (n = 15). Furthermore, one patient who had previously opted out of further contact from the hospital was excluded. From the remaining group (n = 104), we selected the patients who had a baseline Visual Analog Scale for Anxiety (VAS-A)37,38 score ≥30 (n = 27) measured just following the preoperative consultation with the anesthesiologist, as this was assessed as an indication of anxiety.
All eligible participants (n = 27) received an invitation to participate by mail. A total of 15 persons agreed to participate in the study. Five persons declined participation, and the remaining 7 did not answer any of our three recruitment phone calls. Socio-demographic background information was obtained from all participants (Table 1). Level of education was classified by the International Standard Classification of Education (ISCED) standard (levels 0–8). 39 All participants provided written, informed consent for the study.
Baseline socio-demographic characteristics of 15 total hip arthroplasty (THA) patients in the animation anesthesia study, Silkeborg Regional Hospital, Denmark, 2013.
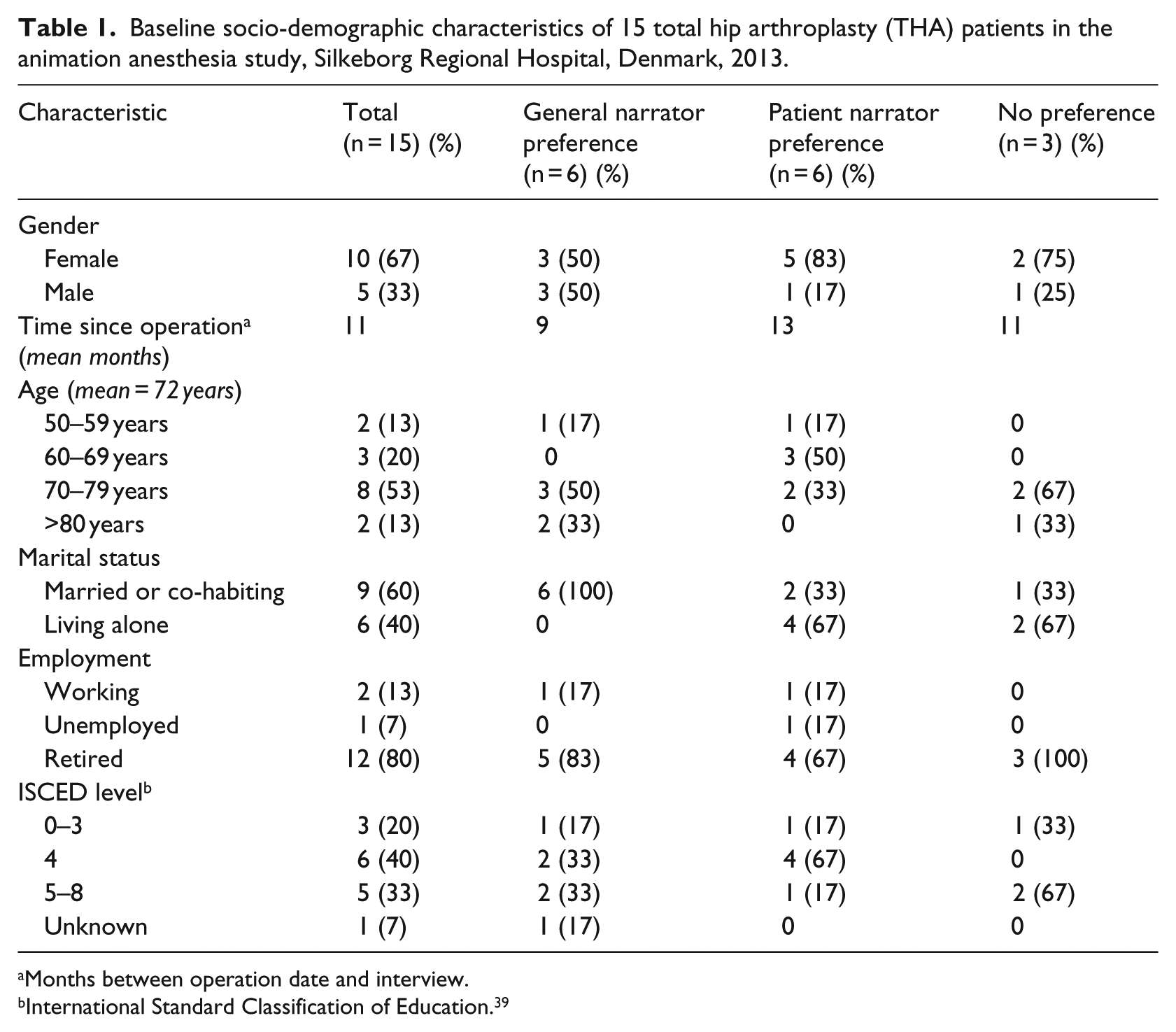
Months between operation date and interview.
International Standard Classification of Education. 39
Data collection
The study used ethnographic methods, 40 combining participant observation, open-ended interviews and “think-aloud” strategies. 41 We studied the participants’ assessment of the animated avatar during screening of the two short videos, with particular attention to the experience of identification and presence with the narrative of the video in either form.
As part of their clinical assessment prior to surgery and as part of the ongoing mixed-methods research study, all patients had provided baseline scores on VAS-A,37,38 EuroQual health related quality of life (EQ-5D-3L)42–44 and General Self-Efficacy.45,46 These measures were accessible to our study for analytical integration with the interview data. Although the study did not have the power allowing for elaborate statistical modeling, we used the scores as additional information on the participants and searched for possible patterns in the scores using the preference typology for comparison.
Testing and interview procedure
A researcher (M.T.H.) visited participants in their homes for screening the two animated videos and interview. Inspired by think-aloud strategies, 41 participants were encouraged to comment on the video as they watched. Following the screening, participants were interviewed on their assessment of the avatar and the two different narrative models. Concluding the interview session, participants were asked, focusing on one animation video at a time, to select from a set of 13 words the 4 most fitting to their experience of either narrative model. The 13 words were: credible, informative, recognizable, human, engaging, frivolous, unclear, comforting, unreliable, irrelevant, unrecognizable, clear and relevant.
Analysis
An ethnographic analysis was conducted 40 identifying repeating and deviating patterns in the material. All interviews were transcribed followed by interpretative reading and organizing. Cross-sectional indexing was used, 47 based on similarities and variations in the experience of identification in participants of the two animated narrative models (general narrator and patient narrator), to produce an overview of the thematic indicators and analytical categories. Based on these inductive categories, a preference typology of patient perspectives on the identification with animated avatars in health education animated video information was developed as a strategy for analytical generalization.40,48 The typology was integrated with the baseline measure of the participants to explore a possible relation between the scores and the patient–avatar identification.
Results
Identification
The animated presentation of the spinal anesthesia procedure was immediately recognized by all participants as reflecting their experience of the procedure independent of the narrative form. This was reflected in expressions immediately following the screening such as “Well, that was exactly how it was” (Patient 2); “That there is really completely like seeing me” (Patient 14). This suggests an overall success of the animation video to produce avatar identification, understood as the personal identification with the experience recounted through the animation video storyline.
Preference typologies
The preference typologies developed in the analysis reflected the patients’ preferences of narrative form in the animation video. The avatar gender did not affect this identification, as male participants also spontaneously identified with the experience of the avatar despite her opposite gender. One female participant, although recognizing her experience of spinal anesthesia in the avatar, stated that a less slim body image of the avatar (Figure 1) might increase her level of identification: “if she was just a bit more, you know, not fat, but just rounder, like the majority of us, I might identify more with her” (Patient 5).
We found no preference for either narrative form among participants. Our preference typology developed three types of patient–avatar identifications along the lines of the narrative models: the “general narrator preference” (n = 6), the “patient experience narrator preference” (n = 6) and the “no preference (I really can’t tell a difference)” (n = 3). Each typology was characterized by recurrent themes across the material.
The majority of participants in the “general narrator preference” stressed the fact-based clarity of the general narrative model. One participant described it like this:
Well there’s absolutely no doubt that the first [general narrator model] is my preferred choice, and that’s because when I get that story it’s clear to see that what I’m told is correct. It’s the professionals speaking: “we do like this and it works like that and so on and so forth.” The other one is more of a recount of something someone experienced, and it gives a nice picture and recounts what it was all about and what happened, but I would really still go for the first, since, well, I would probably feel more safe viewing that one and that’s the correct, fact-based explanation. (Patient 4)
Another participant preferring the same narrative model said,
Really, you might as well tell it as it is and what it is you want to do. […] I just can’t be sure you know … she says [the patient experience narrative model] it takes about 10 minutes, well maybe it did, but then what if it’s only two minutes in my case, right? Or you’ll wait for 10 minutes then, and nothing happens, because it’s just so different [how patients respond to spinal anesthesia]. Then the first is really more like “this is the time it takes” or “this is what it does” and then you have something clear to go on. (Patient 2)
Prioritizing the words to describe their preferred narrative model, the most frequently chosen words in the group with the “general narrator preference” were “credible; human; informative; comforting,” with five of six or six of six choosing these characterizations. However, the exact same four words were the top priorities (with the same frequency) to describe their preferred narrative model in the “patient experience narrator preference.” This suggests these as key elements in the achievement of the communication delivered through the animation video, regardless of narrative model preference in the patient–avatar identification. The two groups disagree on the fifth most commonly prioritized word, which in the “general narrator preference” group was “relevant” and in the “patient experience narrator preference” was “engaging.”
The majority of patients in the “patient experience narrator preference” highlighted the engaging presence of a co-patient as reassuring of the information delivery. One patient said,
Well, that’s really what I searched for or said afterwards that I had lacked, it was someone to talk to who had gone through it before me. Because you can have a whole heap of doctors and nurses explaining all kinds of things, but if they haven’t tried it themselves … well, it’s just all those small things. I realize it’s the exact same information you are told [in the two narrative models], but it’s just that here it’s told to you by a patient and that means, that ahem, well, then it’s probably not too bad anyway, right. (Patient 3)
Sense of presence in animation video
Participants continuously compared the two narrative models in the animation videos and pointed out their differences:
Yes, the second one [general narrator model] seemed shorter somehow, or well, a bit more precise, so to say, while the first [the patient experience narrative model] was more kind of emotional hubbub. But other than that they were basically the same. […] But I find that it’s probably better if it is like the one having had surgery done who tells the story, because that’s comforting and you know that she’ll not just say “oh, that wasn’t a big deal.” You know she went through the experience and says that it’s alright. That’s more comforting I would say, it calms you down. (Patient 15)
This reflects that the patient experience narrative avatar was successful in achieving a sense of presence in the participants, who did not at any point question the credibility of the avatar experience. Furthermore, the patient experience narrative avatar was described as highly engaging by patients as it strongly revived their own experience:
Well I do like the first one [the patient experience narrative model] because that was what she really felt, right, and sensed. And that’s good. It’s completely like what I went through except she didn’t say “ouch” when the needle came, as I did. Well, I found it exciting, not that it has to be, but that was how I experienced it. (Patient 14)
Integration with baseline measure
When we compared the typologies with the baseline scores there was one apparent difference between the three groups on their VAS-A37,38 score prior to surgery (Table 2), where participants preferring the patient experience model scored higher than the other two groups (63 compared to 39 in the other two groups). This could indicate a relation between higher anxiety in relation to the anesthesia procedure and the preference for patient experience information. However, our sample does not have the statistical strength to confirm this. Furthermore, the “no preference” group reported lower health-related quality of life prior to surgery on the EQ-5D-3L,42–44 reflecting lower functional levels and higher perception of pain in this group (Table 2). The “no preference” group further reported lower self-efficacy than the two other groups. This could be related to higher age in this group (Table 1).
Psychometric baseline scores of 15 total hip arthroplasty (THA) patients prior to surgery in the animation anesthesia study, Silkeborg Regional Hospital, Denmark, 2013.
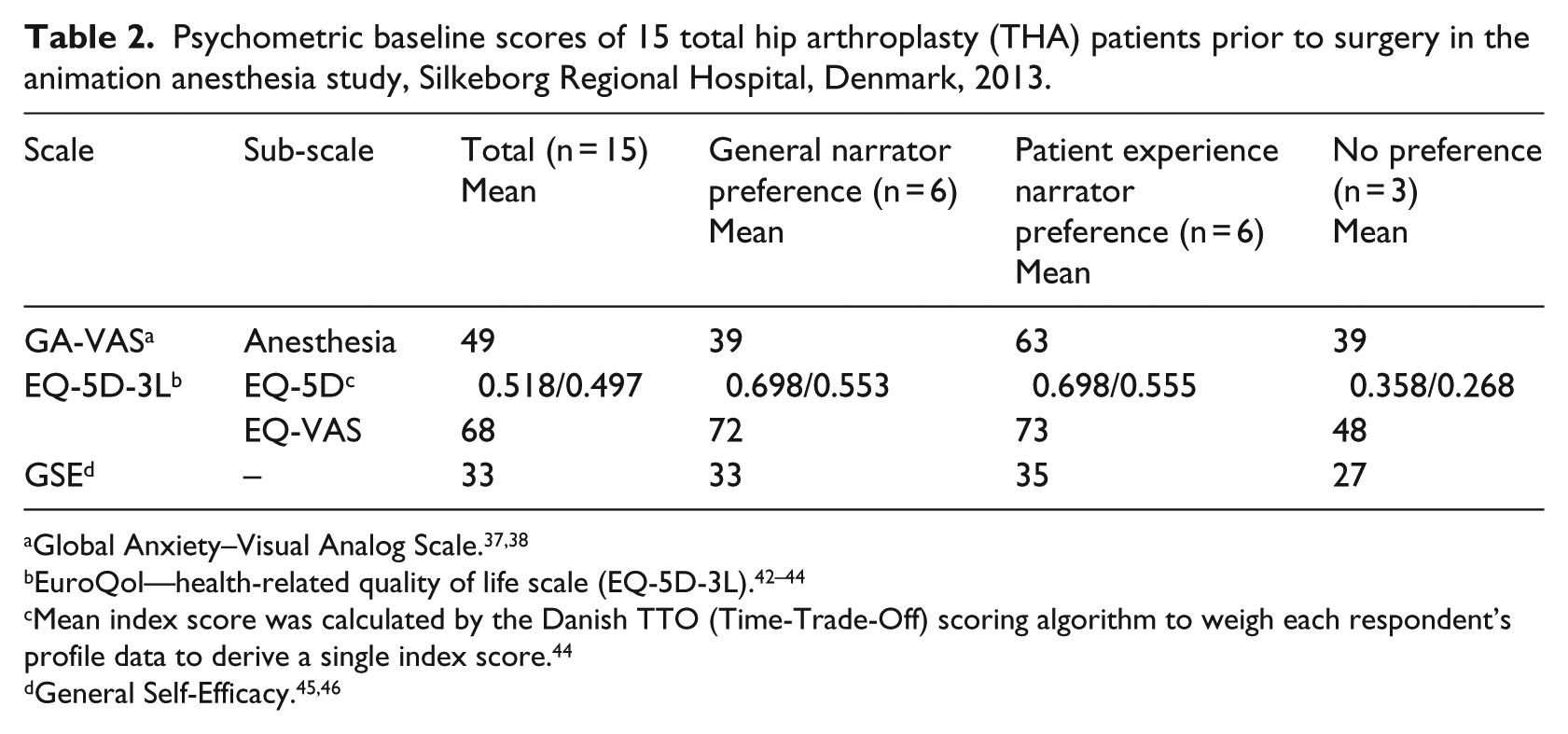
Mean index score was calculated by the Danish TTO (Time-Trade-Off) scoring algorithm to weigh each respondent’s profile data to derive a single index score. 44
Identification modeling pre-surgical behavior
The ability of the animation video to visually highlight the important points of the spinal anesthesia procedure was perceived as highly informative by the majority of participants. One patient noted,
It’s very close to what really happens, so to say, and I could definitely have used that before my surgery. I must admit. Because exactly that I didn’t know. I knew that I was getting anesthesia in my spine, but how exactly it happened, I didn’t know, right. Well, of course you’re a bit nervous … to undergo surgery on that day, but actually it’s mostly what I didn’t know anything about that I feared. (Patient 3) It’s like, then you would know … and well, that would probably just take the top off, you know. You had to score how you felt on a scale from 1–10 right, and then you go all the way straight to the top because you feel lousy, and that I think, that scale, well that would have been different if I had seen this video first. (Patient 1)
One participant, however, found the anesthesia procedure shown in the animation video, with a visual look of the needles entering the spine (Figure 3) to be quite disturbing, to the extent that she reacted with clear physical discomfort:
[…] that needle going all the way in … that’s really not pleasant to watch. […] At least it’s not for me. The first needle in the back with the local anesthesia, that’s fine, but the next one where the full lower body is anaesthetized, well, how should I say it. … You see the needle and that’s intense. I really do think so, well, now I’m saying it like it is—but I’m happy I didn’t know that. (Patient 12)
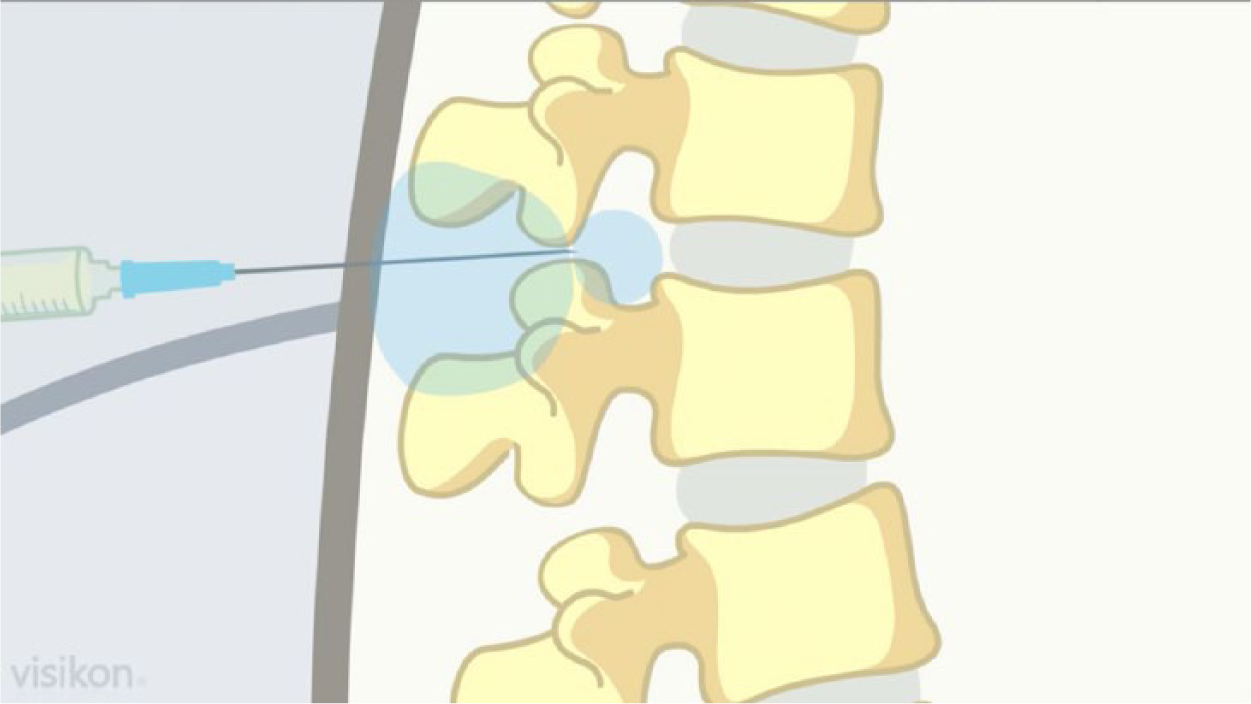
Spinal aesthetical procedure as visualized in the animation anesthesia study, Silkeborg Regional Hospital, Denmark, 2013.
This suggests that patient–avatar identification in the animation video could support social learning models for pre-surgical behavior. However, despite the simple 2D images in the animation used in this study, some patients still found the visualization of spinal anesthesia and surgery procedures very intense and difficult to watch.
Discussion
We found the animation video to create a high degree of identification with the avatar and the information model provided, which may work to reduce pre-surgical anxiety, regardless of preference for any of the narrative models tested in this study. The reporting of immediate recognition from participants in this study suggests a potential for working with the patient–avatar identification as a point of vicarious reinforcement for learning. 28 As the avatar in the animated video through the visual or narrated expression showed deliberations and behaviors, it resonated with the actual circumstance and conditions of the patients. The virtual space of the animation video is thereby a potentially unique learning space, where the understanding of correlations and possibilities may be taught and challenged.
These are important mechanisms and meanings of the use of animation video in patient communication that may explain some of the underlying causes for the positive effects on reduction in anxiety reported in a recent RCT study. 2 The high sense of comfort, credibility and humanness reported by patients in this study in response to viewing the animation videos may point to some of the key social cognitive factors produced by such media that motivate reductions in anxiety. Our study, however, was not designed to measure anxiety reduction and therefore cannot verify such potential effects.
Our finding that the animation video was perceived to be highly informative across the two narrative models is in line with outcomes from a previous RCT reporting increased knowledge of anesthesia in the video group. 3 A previous study found that patient comprehension of anesthetic procedures and postoperative complications was increased by use of an interactive animation video. 20 In this way communication delivery by animation video may support and increase health literacy as suggested by a previous study. 24 The sense of presence and humanness experienced by patients in this study speaks to some of the possible mechanisms in producing these positive outcomes previously reported.
Our findings elucidate a potential social learning model of using targeted communication in animation videos in patient education to produce experience-based knowledge in the patients that may be able to counter or reduce preoperative anxiety in relation to surgical procedures. The visual effectiveness of animated information transcends some of the key challenges of health literacy in health communication3,21,24,49 and may exceed some of the limitations of text-based information in delivering pre-surgical knowledge and understanding. 23 The strong emotional reaction of one participant in this study to certain visualizations points out an important area of concern for the development of animation video health communication; however, a general assessment of how this should be incorporated in development is not possible based on our study.
A limitation of this study is the post-surgical recruitment of participants that limits their ability to assess how the animation videos could have affected their knowledge and served as a behavioral model. Also, it provides only a retrospective view on the information needs of the THA patient group. However, the sampling within this post-surgical group was made on both practical and ethical grounds. Furthermore, our sample size does not provide an opportunity for larger generalizations about knowledge obtained through animation video use. However, our engagement of the theoretical framework of social learning theory and the development of a preference typology allow for an analytical generalization, as is common to qualitative research.48,50 The advantages of this study are the combination of qualitative methods and integration with baseline socio-demographic and psychological measures—measures that made it possible to guide our sampling toward a selection of patients who reported heightened levels of pre-surgical anxiety. Furthermore, our study is one of the very first to engage with the questions of mechanisms and meanings of the use of animated video patient education, where most previous studies have been focused on efficacy in patient outcomes.2,3,20,23,24 This is an important contribution to the development of this research field, as understanding the mechanisms and meanings of use is central to further developing and optimizing animation video education in health and selecting relevant outcomes.
Conclusion
The study supports the potential of using animation video in health informatics as a didactic model for qualifying patient behavior. The ability of the animation video to produce a sense of presence and engagement in patients holds an important perspective for learning in the context of health informatics.
Footnotes
Acknowledgements
We wish to thank the THA patients who took time to participate and share their views. Furthermore, we wish to thank the creative thinkers and animators, Uffe Danielsen and Anders Nejsum at Visikon Inc., who produced the two versions of the animation video used in this work. Finally, we wish to thank Maria Haahr Uhd and Bente Risvig for assistance with interview transcription, data management and score calculation.
Declaration of Conflicting Interests
M.V. is a co-founder and partner of Visikon Inc. that produced the animation video used in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by Animation Hub, Region of Central Denmark and Silkeborg Regional Hospital, Denmark.