
Abstract
Keywords
Introduction
Increased focus on patient involvement has highlighted the need for appropriate patient information and more standardized communication between patients and healthcare professionals. This includes patient information that is easy to access and available for as many patients as possible. However, ensuring updated health information can be challenging and expensive due to heterogeneous patient groups and frequent alterations in procedures and clinical guidelines. 1 This challenge has led to different digital approaches being tested and implemented to disseminate and update information more efficiently and in standardized ways. This has also been the case in Denmark, a leading country in digitalization, and digital health-related information is widely available to Danish patients.1,2
In Denmark, patient information is often delivered as extensive written information on digital platforms. This delivery method requires that patients understand the information but also that they can navigate on digital platforms. However, a pertinent challenge is the prevalence of low health literacy among patients. Studies have shown that up to 40% of all Danish adults have problems assessing, understanding, and using health information.3,4 Another study of 11 European countries found that 35% have poor health literacy. 5 Studies have also found associations between low health literacy and more hospitalization, poor treatment adherence, and higher morbidity and mortality.5–7 This speaks to the importance of delivering patient information in formats that are also understandable and accessible to patients with low health literacy. A possible solution to low health literacy could be patient information delivered through animated videos. Previous studies have found that animations can help patients better comprehend symptoms and treatment related to them and that animation can improve their ability to recall health information and instructions.8–13 In addition, animated videos can simultaneously be entertaining and educational, which helps sustain the viewer’s attention.8,14,15 The combination of animated videos and speech is advantageous when complex health information is communicated to patients with low health literacy. Thus, animated videos can support equality in comprehension between patients with high and low health literacy, respectively.8–10 Since the way to access the animated videos is through digital platforms, the patients’ digital health literacy could affect their comprehension of the animated video. Digital health literacy combines health literacy and digital literacy. It is the ability to seek, find, understand, and appraise health information from electronic sources and apply the knowledge gained to address or solve a health problem. Studies have found that high digital health literacy is associated with an enhanced understanding of disease and condition.16,17
It can be a lengthy and costly process to produce animated videos, especially if the animations contain many details and effects. A review found that some design choices, like the amount of motion, sound, and character, can affect the viewers’ attention through animation. Another study discussed how messages delivered in more exciting and colorful formats transmit the message more efficiently.15,18 However, knowledge needs to be improved on how the level of detail in animations affects patients’ ability to recall information from the animation. Also, it is unknown if using simple animations with a low level of detail harms information recall for patients with low digital health literacy.
Therefore, this study aimed to investigate the association between the level of detail in health animations and patients’ ability to recall information. Also, we wanted to investigate if the association was influenced by digital health literacy.
We hypothesized that simple health animations with a low level of detail compared to more detailed health animations would have an equal impact on patients’ information recall. We also hypothesized that for patients with low digital health literacy, the level of details could impact patients’ ability to recall information.
Method
Design and setting
This was a comparative experimental study without a control group. The study is reported according to the CONSORT guideline for randomized controlled trials. 19 The experimental nature of this study makes this the most suitable reporting guideline, although this is a non-randomized study. The study was conducted 6 months, from October 2021 to May 2022. The recruitment period was used to ensure participants were allocated into groups presented with either an animation with a low or high level of detail. In the first half of the recruitment period, participants were continuously included and presented with an animation with a low level of detail (sketch). The animation had a low level of detail, no motion, and was made with a nonprofessional speaker. Halfway through the recruitment period, participants were still included continuously and were now presented with an animation with a higher level of detail (finished). The finished animations had more details, motion, and a professional speaker. The sketch and finished animations differed in, for example, motion, color use, speaker, and textbox, though both versions were relatively simple (see Supplemental Appendix 1 for examples of differences between the animations). The length of all the animations in this study was approximately 2 min. Participants gave written consent to participate. According to Danish law, this study did not need ethics approval because human biological material was not included (Act on Research Ethics Review of Health Research Projects, section 14, October 2013). 20
Participants
The animations were distributed to two different groups of participants (presented below). Participants were recruited from three wards at public hospitals and a private hospital in Denmark. Due to the recruitment method, it is impossible to say anything about the non-responders.
Dysphagia
The first group of participants was patients at risk of dysphagia, which is persons above 65 years of age or relatives of patients with dysphagia. The participant’s knowledge about dysphagia was unknown at the recruitment time. Contact was made primarily through the Danish digital mailbox, the included hospital website or Facebook page, and local municipal health center flyers. Patients excluded from the Danish digital mailbox received an invitation to participate through postal mail. The participants did not receive information about dysphagia in any other way than through the animation.
The day of surgery
The second group of participants included patients with upcoming scheduled surgery. They received the animation through the Danish digital mailbox at the same time as their invitation for surgery. Patients excluded from the Danish digital mailbox received an invitation to participate through postal mail. The animation included important information and aimed to prepare the patients for the day of surgery. The patients would also receive the information at appointments at the hospital and as written information.
The two groups of participants received animations (sketched or finished) related to the topic (dysphagia or day of surgery), meaning four animations were developed and distributed. As described above, the recruitment period was used to allocate participants into sketch or finished animation, and the participants were excluded if they were under 18 years old, did not consent, or did not answer enough questions (under 10% of the questionnaire).
Measures
The participant’s ability to recall information was reported through a questionnaire distributed alongside the animations. The questionnaire consisted of demographics, information recall, and digital health literacy measured with the eHealth literacy assessment toolkit. 21
Sociodemographic characteristics
Data on sociodemographic characteristics included sex, age, education, marital status, chronic disease, and comorbidity.
Information recall
The participants’ information recall was evaluated with a ten-question questionnaire with three response options. The questions were about the health information included in the animations. The correct answer gave one point, and a score between 0–10 was possible. The questionnaires are available in Supplemental Appendixes 2 and 3. A cut-off point of ≤7 was used to indicate low information recall. The questionnaire was developed by the research team responsible for the project.
eHealth literacy assessment toolkit (eHLA toolkit)
Digital health literacy was measured using the eHLA toolkit, a validated toolkit measuring a combination of health literacy and digital literacy based on self-reported information and performance tests. 21 The toolkit consists of 7 tools, which in this study were divided into three categories evaluating: 1) The participants’ health competencies related to information processing and navigation in the health services (tools 1–2), 2) The participants’ familiarity and healthcare knowledge (tools 3–4), and 3) The participants’ familiarity with technology, technology confidence, and incentives for engaging with technology (tools 5–7).
We dichotomized participants into low (scoring below the median in at least one of the tools in each category) or medium/high (the remaining participants) digital health literacy.
One question in Tool 2 was omitted due to technical problems. However, a score can be calculated if more than 50% of the items are answered. Therefore, we kept the results from Tool 2 and considered the question unanswered.
Sample size
Based on previously conducted studies in which the ability to recall information from animations has been assessed,15,22–24 we anticipated a 15%-point difference in information recall between participants who had seen the animation with a low level of details (sketch) compared to a higher level of details (finished). To detect a 15%-point difference (power 0.80, alpha 0.05), a minimum of 276 participants (138 in each group) was needed.
Data management and analysis
All data were collected and managed electronically using the REDcap electronic data capture tool.25,26 STATA17 was used for all statistical analyses. Data analyses were separated equivalent to the two participant groups, meaning all analyses were performed separately for participants who had seen the animations about dysphagia and participants who had seen the animations about the day of surgery. Descriptive statistics (percentages, medians, means) were presented for the two groups of participants, divided into participants who had seen the sketch and the finished animation. The distribution of participants with high and low information recall was calculated and presented as proportions with a 95% confidence interval (CI) for the two participant groups (dysphagia and the day of surgery), respectively. This analysis revealed that for the group of participants who had seen animations about the day of surgery, a ceiling effect on the outcome (information recall) had occurred. Hence, we could not analyze the association between the level of details and information recall for this group of participants. In the participants who had seen the animations about dysphagia, the association between the level of details and information recall was analyzed using logistic regression, adjusted for sex, age, and educational level, and presented as OR (95% CI). Participants with missing values on the included variables were excluded. Stratified analysis was done by repeating the analysis for participants with low and medium/high digital health literacy.
In addition, a sensitivity analysis was performed, where we changed the cut-off point for information recall to ≤6 (10% lowest) and 10 (20% highest). Also, a sensitivity analysis was performed to explore if different classifications of digital health literacy would impact the results in the stratified analysis. This sensitivity analysis explored if the results would differ if the seven tools from eHLA were handled separately instead of as a dichotomized variable.
Results
Participant demographic characteristics and digital health literacy.
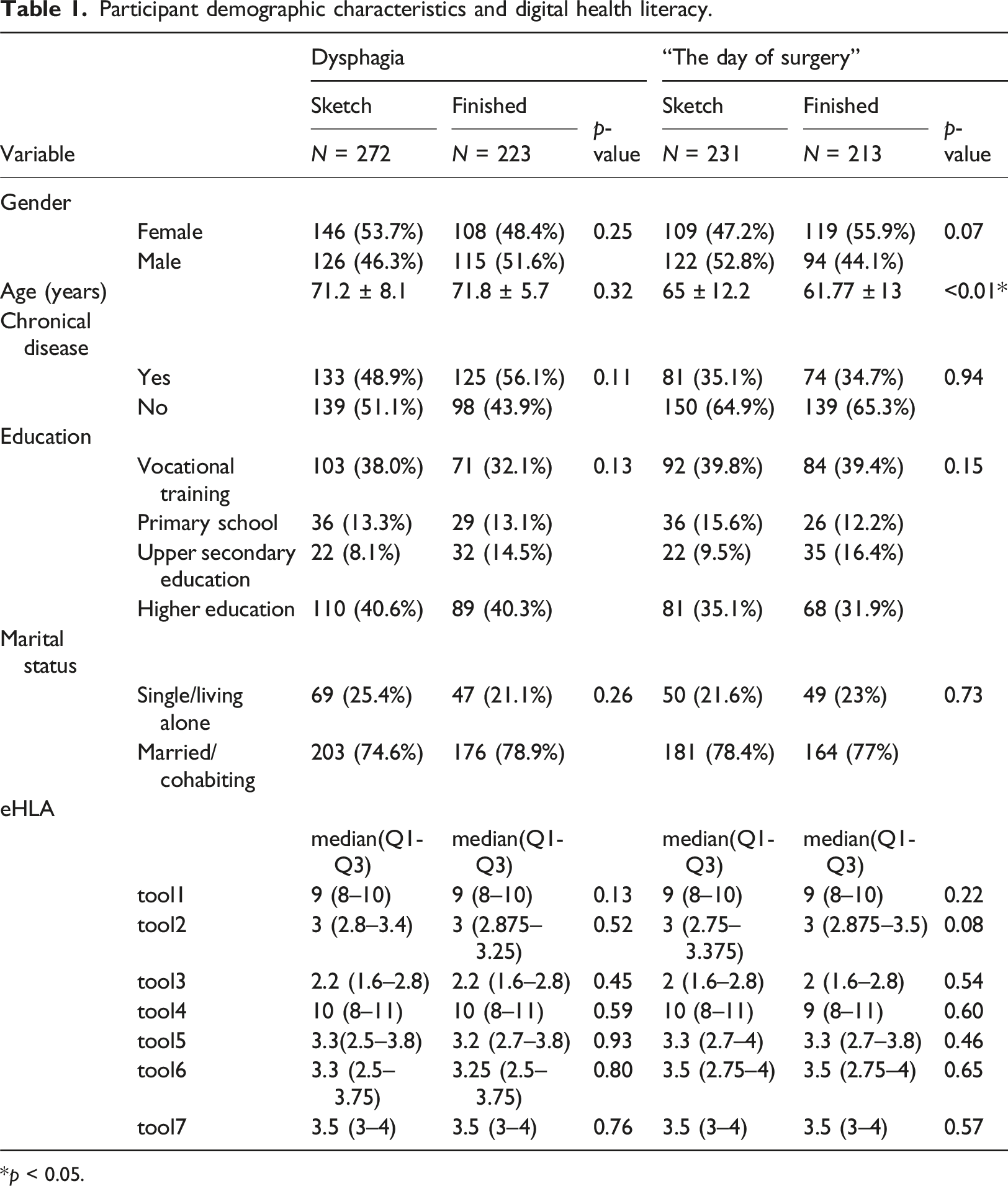
*p < 0.05.
Association between level of details and information recall stratified by digital health literacy.

Adjusted for gender, age and education.
Changing the cut-off point for information recall to ≤6 (10% lowest) and 10 (20% highest) did not alter the results. Also, using the 7 separate tools in the eHLA instead of dichotomizing into low or medium/high digital health literacy did not show any significant associations between the level of details and information recall (data not shown).
Discussion
This study sought to investigate the association between the level of detail in health animations and patients’ ability to recall information and whether this association was influenced by digital health literacy. The results indicate that the level of detail in animations is not associated with patients’ information recall and that there is no indication that the results are different for patients with low digital health literacy.
Interpretation
Previous studies have found that animations, compared to other information sources, can improve patients’ ability to recall information.8–12 To our knowledge, no studies have investigated how this improvement in patients’ ability to recall information is affected by the level of detail in the animation. Since producing animations can be expensive and time-consuming, exploring ways to optimize the process by making the animations simpler is relevant.
Studies have found that the level of detail can impact the viewers’ attention and experience with animations.15,18 Patients’ attention towards the animation may affect their ability to recall information as they may miss some information. However, this study shows that patients could recall information effectively even when presented with a sketch version of the animation. Our interpretation of these results suggests that this high recall ability may be due to the limited duration of the animations used in this study, which were only 2 min long. This limited duration also limits the patient’s amount of information to process. It is generally acknowledged that animations should be as short as possible to ensure a better user experience and increased engagement.
Furthermore, the patients who had seen the animations about the day of surgery got the highest scores in information recall, and few patients scored below 7. This could indicate that the subject of the animation impacts patients’ ability to recall information. Hence, the consequence of not following instructions on the day of surgery could be a canceled surgery. Therefore, we believe that participants who saw the animations about the day of surgery were more motivated than patients’ who saw the animations about dysphagia. We assume that the patients’ who had seen the animations about dysphagia did not have the same motivation since the information disseminated in this animation had a more informative and preventive purpose. Also, the information from the animations about the day of surgery was disseminated to the participants through other sources, possibly affecting their ability to recall information. Future studies could investigate whether different types of information affect the association between the level of detail and information recall. Additionally, it would be beneficial to gather information about the participants’ knowledge of the topic before they were included in the study.
Previous studies have found that animations especially benefit patients with low health literacy.9,10 This study found no association between the level of detail and information recall among patients with low digital health literacy, which indicates that animations could be simpler in the future and still support the patients in most need of alternative sources of information than text and illustrations. Simple animations have shorter work processes and are more affordable and sustainable. These results contribute knowledge about the potential of simple animations and how to make animations more economically available for the healthcare system in the future.
Limitations
In what follows, we will discuss some methodological limitations and what practical implications there may have been. A limitation of this study was the recruitment method, which decidedly took place through digital platforms (Danish digital mailbox, website, and Facebook). Only 8% of Danish adults are excluded from e-Boks, but studies have shown that the percentage of Danish adults uncomfortable with digital solutions is higher (17%). 27 Thus, there is a risk that the recruitment strategy coursed selection problems because our included groups of participants have better digital health competencies than the general population. Since higher digital competencies are associated with a better understanding of disease and condition, the recruited participants were probably better at comprehending and recalling health information regardless of the source of information.16,17 This could have led to an overestimation of the patients’ information recall. However, it may also have led to underestimating the association between information recall and detail level in animations. Participants with higher digital health competencies would have had greater odds of possessing knowledge about surgery or dysphagia independent of which animation they saw. Future research should aim for a more controlled and clear recruitment of participants, allowing comparison of non-responders and responders. Also, it would be beneficial to include additional recruitment strategies to target patients with lower digital competencies to minimize the risk of selection problems.
Another limitation is potential information problems on the outcome (information recall) collected through questionnaires. This also includes developing the scoring system of 0–10 points in information recall. The questionnaire was not tested for content validity in the target group before distribution, which raises concerns that the instrument may not effectively measure information recall as initially intended. Also, the scoring system of 0–10 may not reflect actual information recall, as we did not test the participants’ level of knowledge before the animations. Therefore, we do not know to which degree the animations impacted the participant’s level of knowledge on the specific subject. This non-differentiated information problem could have weakened the possibility of finding any association between information recall and level of detail. However, the questionnaire was pilot-tested for content validity in a group of researchers. As the questions are single-item and factual, we believe the ability to recall information could be measured using the defined questions. Future studies should focus more on developing valid and reliable measures of information recall. They could also include a control group to examine the “baseline” knowledge level among the animation’s target group. Participants could also find information from other resources, like the internet or relatives, to fill in the questionnaire. This potential limitation is always present in the choice of a questionnaire method, and other qualitative study designs, like an interview study examining the same research question, could be an alternative in the future.
Furthermore, we also have a potential information problem with the exposure (level of details) because even the finished animations in this study were very simple, and there were perhaps insufficient differences between the sketch and finished versions. This could have led to non-differential misclassification of the exposure. Thus, there is a risk that this study underestimates the association between the level of detail in health animations and patients’ ability to recall information. Future research could advantageously compare information recall from more complex animations to simpler animations to better understand the relationship between the level of details and information recall.
The use of the validated toolkit eHLA is an advantage of this study. Nevertheless, as described, there is an irregularity in the method due to one question in tool 2 from eHLA being left out of the questionnaire. The exclusion of a single question could potentially impact some participants’ overall classification of digital health literacy. However, it was possible to calculate all scores for tool 2 despite the missing question due to the terms of the tool. 21 Therefore, we presume that this error did not play any significant role in the classification of digital health literacy. The eHealth literacy assessment toolkit has no cut-off points or classifications and should be interpreted as seven individual scores. However, in this study, we decided to dichotomize the participants into medium/high and low digital health literacy to simplify the data and make the results easier to interpret. Dichotomizing digital health literacy could have reduced the complexity of the results, as the eHealth literacy assessment toolkit was designed to be multifaceted and to encompass different aspects of digital health literacy, including elements from all six literacies of the Lily model. 21 However, a sensitivity analysis was conducted to evaluate whether the dichotomization had restricted the possibility of investigating whether the association between the level of detail and information recall was affected by the participant’s digital health literacy. This sensitivity analysis assessed whether the results would differ if the seven tools from the eHLA were handled separately instead of as a dichotomized variable. The sensitivity analysis indicated that the dichotomization did not affect the conclusions drawn in this study.
Generalizability
The study focused on only two animations, one about surgery and one about dysphagia, which means that the generalizability of the results is limited to populations similar to the target groups of these animations. Furthermore, the results are limited to populations in Denmark or similar countries with comparable cultures, social structures, and other factors that may impact the results. Therefore, it is important to consider the context before applying the findings to other populations or contexts.
Conclusion
This study contributes insights into the use of health animations and the consequences of making the animations simpler with a low level of detail. The results indicate that the level of detail does not impact the patients’ information recall, and this was also the case for patients with low digital health literacy. The results support the potential of making health animations with fewer details. However, our conclusions should be interpreted cautiously, given the significant risk of bias in the present study. Further research could advantageously investigate the same research question with more significant differences in the level of detail and focus on which type of health information is the most suitable for animations.
Supplemental Material
Supplemental Material - Do we need a high level of detail in health information animations? An experimental study investigating the association between level of detail and information recall
Supplemental Material for Do we need a high level of detail in health information animations? An experimental study investigating the association between level of detail and information recall by Pernille Blom Pedersen, Mette T Høybye, Line Borreskov Dahl and Cecilie Rud Budtz in Health Informatics Journal.
Footnotes
Acknowledgements
The authors would like to thank Regional Hospital Central Jutland, Viborg Municipality, Capio Private Hospital, and WonWon.
Author contributions
L.B.D. and M.T.H. planned and designed the study. P.B.P. and C.R.B. performed the statistical analyses, and P.B.P. drafted the manuscript. All authors contributed to interpretation of the results and substantial and critical revision of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by Regional Hospital Central Jutland, Viborg Municipality, and Central Denmark Region.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.