
Abstract
Potential unintended consequences of health information technology include fragmentation of workflow and redundant work. We could not identify any prior direct observation studies that quantified redundant work related to health information technology in the clinical setting. Our objective was to quantify redundant work during admission and discharge to our general internal medicine service at an academic medical center. We performed a time and motion study at Sunnybrook Health Sciences Centre in Toronto, Canada. We observed 13 clinicians performing an admission or a discharge, and the type and length of each task was recorded using an Apple iPad tablet. We identified redundant tasks related to health information technology and calculated the time spent completing these tasks. We found that 22 percent of clinician time was spent on redundant tasks. Our finding highlights the importance of workflow and software integration when implementing health information technology.
Background and significance
Clinician time is a precious non-renewable resource. Efficient use of clinician time is important from a health systems perspective since physician remuneration accounts for a substantial proportion of health-care costs. 1 Clinician efficiency contributes to the overall efficiency of a process, such as the flow of patients through an emergency department. 2
Many claim health information technology reduces errors, increases patient safety, and improves efficiency, but it may have unintended consequences. 3 Fragmented workflow due to health information technology attenuates improvements in physician efficiency.4–6 Independent information technology systems are often developed for specific tasks without considering the entire clinical workflow or integration with other clinical applications. When independent systems require similar information inputs, such as a list of medications, health-care providers must perform redundant work by finding and opening another clinical application (or the paper chart), finding the same patient in the second application, and manually searching for the same information in the second application. An efficient integrated system would allow a clinician to complete work within a single application, with a single password/log on, within a single patient chart, by bringing information to the user’s attention when and where the information was needed, and allowing the user full control to select and modify relevant information.
Studies of redundant clinical documentation report up to 30 percent information redundancy between admission and discharge notes.7–9 Implementing an electronic signout tool caused a subjective reduction in redundant work, according to a small survey of physicians. 9 We could not identify any prior direct observation studies quantifying redundant work in the clinical setting.
Materials and methods
We performed a time and motion study in December 2011 on the general internal medicine inpatient service at Sunnybrook Health Sciences Centre, a teaching hospital in Toronto, Canada. We directly observed a convenience sample of 13 participants performing hospital admission and discharges in the emergency department or in the general internal medicine wards. We included residents, medical students, and nurse practitioners, since all perform similar tasks using the same paper documents and electronic clinical applications on our service. We collected time and motion data using an Apple iPad tablet and InMotion Pro Time Study software (InnovateLabs, version 3.1). We developed the study according to the guidelines for time and motion studies established by Zheng et al. 10 Institutional Research Ethics Board approved the study.
Clinical workflow for admissions and discharges to our general internal medicine service involves paper documents and three electronic applications: Electronic Patient Record (EPR), eSignout, and eDischarge. EPR is a commercial software developed by Oacis (version 7.0, DINMAR 2003) that contains laboratory investigations, imaging and other test reports, and transcribed reports including clinic letters and discharge summaries. eSignout is an in-house-developed application that allows clinicians to build and maintain patient lists and requires manual entry of data. eDischarge is an in-house-developed application that creates standardized discharge summaries by manual entry of all necessary data such as past medical history, history of presenting illness, course in hospital, and follow-up plan. We developed the applications as standalone solutions for specific tasks, and they lack integration and require separate sign-on.
We generated a list of tasks by consensus. Task lists from previous time and motion studies did not provide adequate detail on admission and discharge tasks. We performed minor modifications to the task list during the study, primarily clarifications on categorizing some activities. In cases where multitasking occurred, we judged what represented the primary task and categorized the activity accordingly.
We obtained informed consent and administered a survey prior to study commencement. We instructed participants to proceed with the admission or discharge as they usually would. We minimized interruptions by the observer, although participants were asked for clarification when necessary. We recorded data continuously resulting in no “transition time” between tasks. The period of observation lasted until the task was completed to the participant’s satisfaction or the participant was unable to proceed for any reason.
We defined redundant work as any of the following:
Re-typing or re-copying information from one electronic application to another;
Copying information from an electronic application to paper;
Re-typing or re-copying the same information a second time;
Locating or filling out paper requisition forms.
For example, for work involving two electronic clinical applications, redundant work would require a clinician to (1) open a second application, (2) enter a second password, (3) re-select the current patient in the second application, (4) search for the relevant information, and (5) re-type or re-copy information.
We reviewed each observation and assigned one of two descriptive labels: “redundant” or “not redundant” based on a pre-specified classification scheme (see Table 1). Figure 1 illustrates our classification scheme with examples. Although activities classified as “redundant” were felt to have a significant component of redundant work, it is possible that some non-redundant work was captured in this category.
Classification scheme for redundant activities.
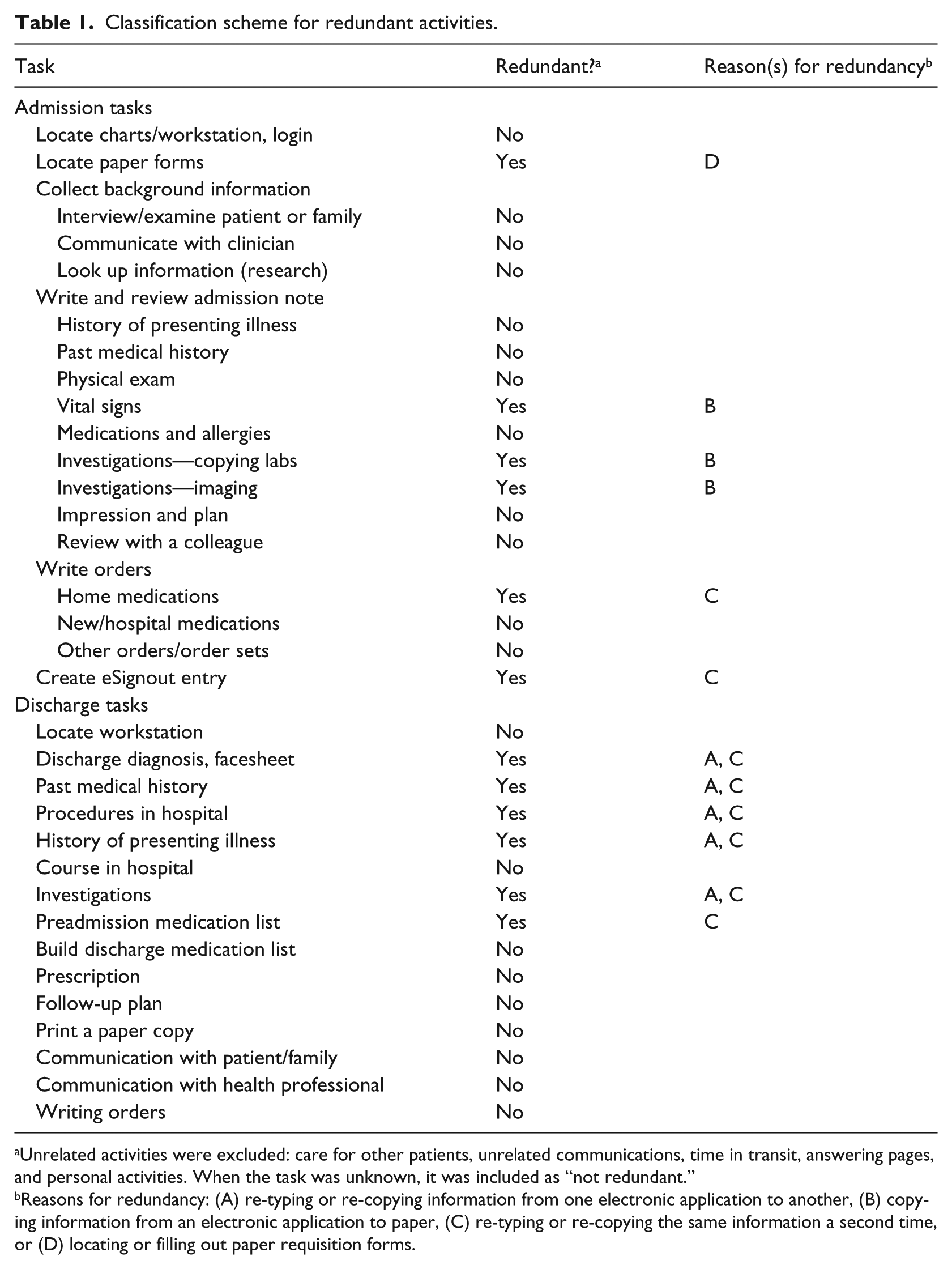
Unrelated activities were excluded: care for other patients, unrelated communications, time in transit, answering pages, and personal activities. When the task was unknown, it was included as “not redundant.”
Reasons for redundancy: (A) re-typing or re-copying information from one electronic application to another, (B) copying information from an electronic application to paper, (C) re-typing or re-copying the same information a second time, or (D) locating or filling out paper requisition forms.
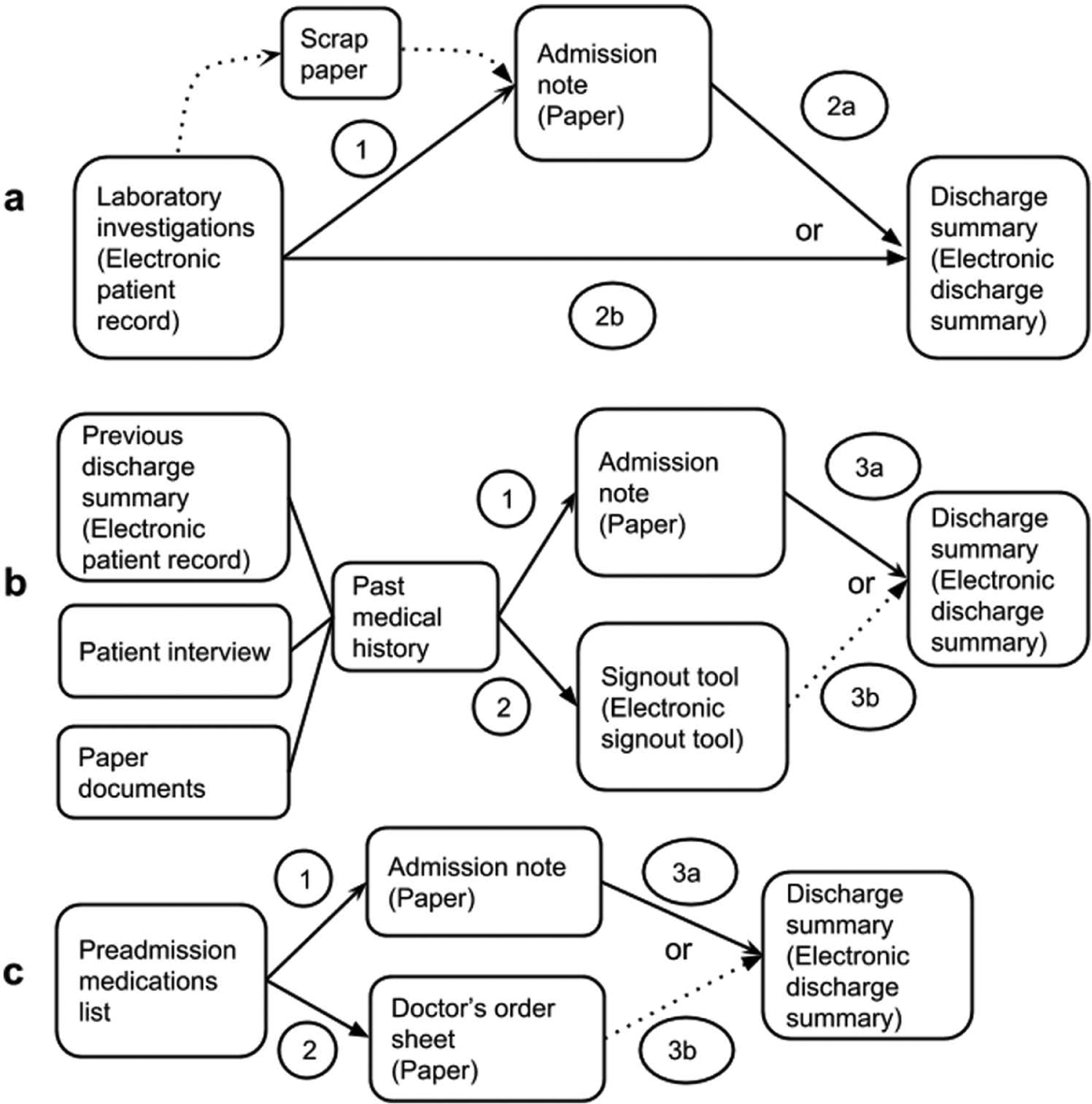
Flow diagrams illustrating redundant processes during admission and discharge on general internal medicine at Sunnybrook Health Sciences Centre. (a) In step 1, laboratory investigations are copied from the Electronic Patient Record to a paper admission note, which is considered redundant due to copying from an electronic system to paper. Steps 2a and 2b require copying the same information from step 1 and are therefore redundant. Step 2b requires copying information from one electronic system to another electronic system. Some participants added an extra redundant step by using scrap paper. (b) Step 1 is not considered redundant because this is the first time past medical history is recorded/transcribed. Steps 2, 3a, and 3b are redundant because they require re-copying the same information from step 1 into the electronic signout tool and discharge summary. (c) Step 1 is not considered redundant because this is the first time preadmission medications are recorded/transcribed. Steps 2, 3a, and 3b are redundant because they require re-copying the same information from step 1 onto the paper order sheet and into the electronic discharge summary, respectively.
To maintain a conservative analysis, when the nature of the primary task was unclear, we classified the observations as “not redundant.” We performed the analysis both with and without tasks that we considered unrelated to the admission and discharge process, such as socializing or eating, in order to obtain the most conservative possible estimate.
Results
We observed 13 participants completing 16 admissions or discharge summaries, including 10 residents, 2 medical students, and 1 nurse practitioner. Most of the residents (70%) were internal medicine residents, and the majority (60%) were first-year residents. There were similar numbers of male and female participants. Participants had completed a median of 1.5 months on the general internal medicine service at our hospital at the time of observation (range: 0.5–29 months). All participants rated themselves at least “Somewhat Comfortable” using computers and the hospital clinical information systems. The average duration of each observation was 88.6 min for admissions and 30.4 min for discharges.
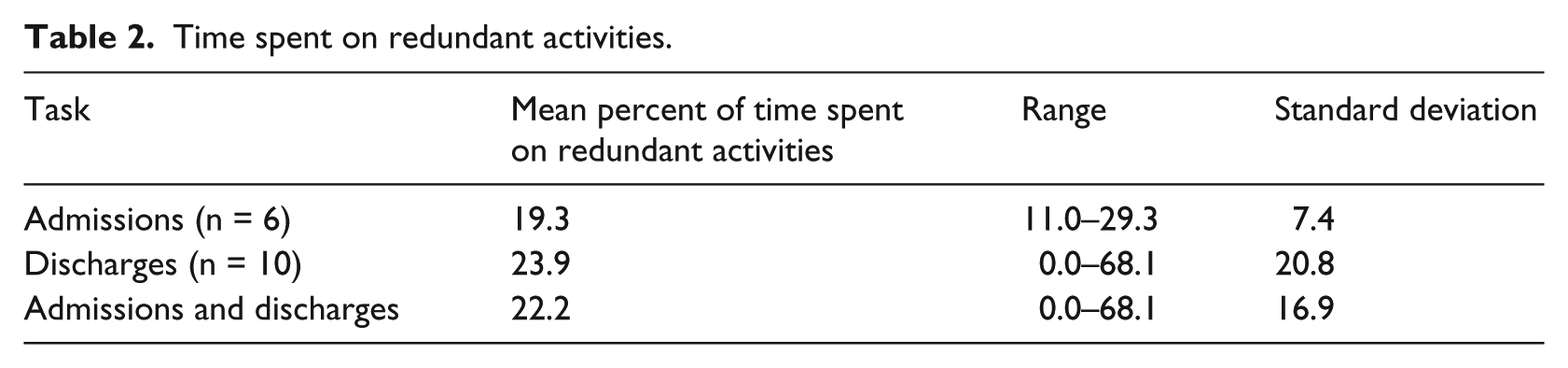
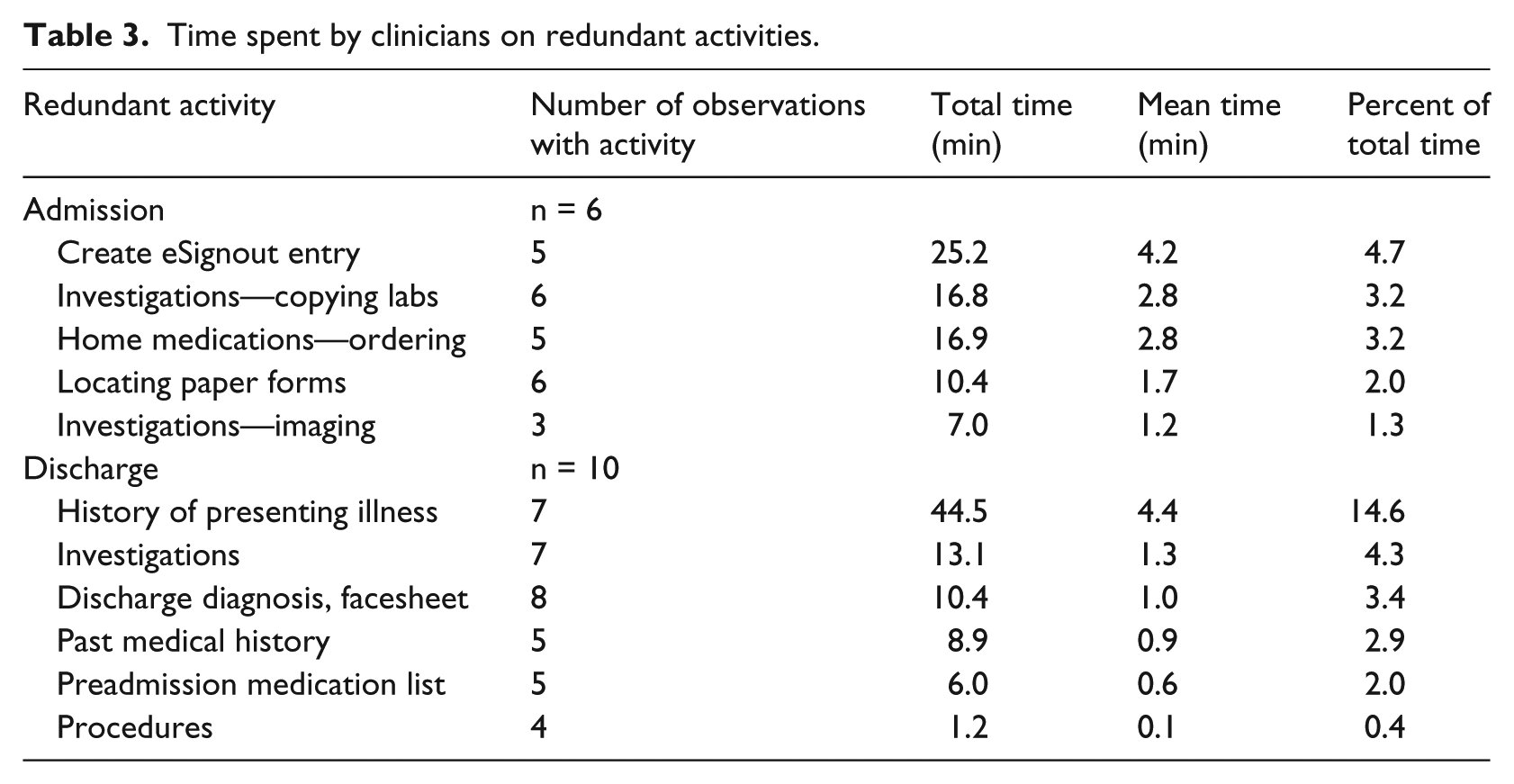
Our main findings are as follows: 22 percent of work on an admission or discharge is redundant (Table 2). Practitioners spent an average of 13 min per admission and 8.4 min per discharge on redundant work. During admissions, common redundant tasks were completing the signout entry, copying laboratory investigations, and writing home medications on paper order sheets (Table 3). Participants spent 2 percent of their time locating and stamping paper forms. During discharges, the most common redundant task was completing the history of presenting illness (14.6% or 4.4 min on average). We found similar results when the analysis included the tasks unrelated to the admission or discharge process such as socializing or eating.
Time spent on redundant activities.
Time spent by clinicians on redundant activities.
Most (92%) participants agreed that there is information redundancy in the admission and discharge process at our hospital. Participants identified numerous examples of redundant work, such as copying information from the paper admission note to multiple places including the paper order sheet, the electronic signout list, and the electronic discharge summary. Participants commonly identified copying information from one electronic database to another as redundant work, such as manually copying medical imaging reports from the EPR to the electronic discharge summary.
Discussion
We found that clinicians spend 22 percent of their time performing redundant work during hospital admission and discharge on our general internal medicine service. On average, clinicians spent 13 min on redundant work during an admission and 8.4 min for a discharge. Our study is the first to quantify time spent on redundant work using time and motion methods. We developed a data collection method that can be adapted and used by others performing similar research. Our result is consistent with a retrospective chart review that found 30 percent information redundancy between admission note, discharge summary, and signout note. 8
The main implications of our study are as follows: design health information technology based on clinical workflow to minimize redundant work; pay attention to potential and actual unintended consequences of health information technology implementation, especially workflow; ensuring integration and easy data flow between electronic applications could reduce redundant work. In fact, we have used our findings to design a better-integrated application that facilitates the admission, signout, and discharge process. We estimate that the new design will eliminate a significant proportion of redundant work.
Our study has important limitations. First, we studied a small sample at a single site. We do not generalize our results to other settings with different health information technology systems; rather, others may wish to use our methods to quantify and characterize redundant work in their own settings. Second, the reliability and validity of classifying work as redundant are not known. We used only one observer and did not evaluate intra- or inter-rater reliability. However, our rater was experienced and familiar with clinical workflow and all clinical applications, so our data have high face validity. We intentionally used a conservative design and analysis which may underestimate the true level of redundant work during these tasks.
Direct observation studies are susceptible to observer-effect which might have impacted our participants’ behavior. To mitigate this, we did not inform participants of the study hypothesis in advance and informed participants that the study did not assess speed of completion or quality of task completion.
We acknowledge that some redundancy may be beneficial by creating an opportunity for errors to be discovered and corrected. We cannot rule out the possibility that reducing redundancy in clinical workflow will reduce detection of errors, and we urge further study in this area. Redundancy is sometimes used beneficially in education, where repetition can improve information retention. However, we believe that the redundant activities in our study have little didactic value, such as launching second applications, re-entering passwords, re-selecting the same patient in a second application, searching for information in second applications, and re-copying and re-typing information multiple times. An efficient integrated system would eliminate these low-value activities and bring the relevant information to the clinician for didactically useful activities such as review, revision, and analysis.
Conclusion
In summary, clinicians spent 22 percent of time on redundant work during admission and discharge on our general medicine service, which highlights the importance of workflow and software integration. We have used our findings to design a better-integrated application that facilitates the admission, signout, and discharge processes. We estimate that the new design will eliminate a significant proportion of redundant work. We urge others to quantify redundant work in their own settings to improve efficiency.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.