
Abstract
Patient care handoffs are cognitively intense activities, especially on medical and surgical units where nurses synthesize information across an average of four to five patients every shift. The objective of this study was to examine handoffs and nurses’ use of computerized patient summary reports in an electronic health record after computerized provider order entry (CPOE) was installed. We observed and audio taped 93 patient handoffs on 25 occasions on 5 acute care units in 2 different facilities sharing a vendor’s electronic health record. We found that the computerized patient summary report and the electronic health record were minimally used during the handoff and that the existing patient summary reports did not provide adequate cognitive support for nurses. The patient summary reports were incomplete, rigid and did not offer “at a glance” information, or help nurses encode information. We make recommendations about a redesign of patient summary reports and technology to support the cognitive needs of nurses during handoffs at the change of shift.
Introduction
Patient care handoffs are cognitively intense activities. Before each shift in every acute care facility worldwide, medical and surgical nurses seek, filter and synthesize patient information across an average of four to five patients, and use a variety of paper-based and electronic tools to support the handoff process. Most electronic health records (EHRs) offer a patient summary report specifically designed for nursing handoffs. Because they integrate information across typical electronic health record modules, these reports should help reduce cognitive burden for acute care nurses.
Previous research showed that nurses relied on informal, hand-written, personalized paper forms they call their “brains”, even in a facility with an electronic health record having a full range of functions, including computerized provider order entry and decision support capabilities. 1 No research other than two reports of nurses’ perceptions is available about actual use of electronic handoff forms during nursing handoffs. In this study, we explored whether nurses in two additional hospitals used the electronic patient summary report for handoffs after computerized provider order entry (CPOE) and its associated summary report were deployed. Based on our findings, we provide insights about why the current design of the electronic patient summary report does not provide the required cognitive support for medical and surgical nurses in acute care settings. We make recommendations about potential solutions for the future design of technology-enabled handoffs.
Background
Accurate and pertinent information exchange during patient care handoffs is crucial for safe patient care, 2 especially with the increasing complexity for patients on medical and surgical units in acute care institutions.3,4 Yet, patient care handoffs are typically informal, inconsistent and unstructured.1,5 These informal handoffs can lead to gaps and errors in care. 6 For example, communication break-downs led to patient harm in 60 out of 444 medical malpractice claims. Of the 60 cases, 43% had communication breakdowns during handoffs. 7 Inadequate handoffs were related to sentinel events, 8 critical incidences, 9 errors and near misses in novice nurses, 3 and information omissions that did not allow nurses to immediately begin patient care after handoffs were completed. 10 Nagpal et al. noted information loss at every handoff point in a surgical patient care continuum 11 until only 43.9% of essential information reached the inpatient unit. Likewise, Richard 12 , found incongruence in all 57 handoffs for 584 patients when comparing handoff information to patients’ actual conditions.
In the past, nurses have published numerous opinion pieces and perceptions concerning handoffs. Nurses in Europe expressed dissatisfaction with handoffs. 13 Computerized handoffs were seen as one solution to reducing dissatisfaction and minimizing errors during complex cognitive activities, such as handoffs, 14 but others claimed that replacing face-to-face handoffs with asynchronous electronic records would hinder nursing handoffs. 15 Authors have described various handoff methods available including: written/printed, 16 phoned including S-BAR [Situation, Background, Assessment and Recommendation], 17 taped, 18 care-plan based, 19 bedside;20–25 and reading the patient’s chart at the bedside. 26 Nurses had positive perceptions about these various types of handoffs on effectiveness and efficiencies for these measures: accuracy, 23 quality, 18 relevancy, 18 conciseness, 18 completeness;23,26 improved documentation, 19 satisfaction with the method;19,20,27 perceived effectiveness; 25 perceived safety, 22 teamwork; 22 confidentiality; 25 ability to care for patients; 28 quality 18 and access to information. 25 Authors reported decreased overtime with bedside report,20,23 taped report, 18 phone report 17 and increased efficiency and teamwork. 22
At least eight reviews on handoffs are now available, although purposes and conclusions largely differ.29–36 All but Arora et al. and Cohen and Hilligoss center completely on nursing handoffs. Cohen and Hilligoss described the lack of standardization on handoffs, or even the availability of a common definition for the activity. For this paper, we adopt the definition offered by them: “the exchange between health professionals of information about a patient accompanying either a transfer of control over, or of responsibility for the patient”. 30 Both Matic 33 and Riesenberg et al. 37 concluded that evidence is not yet substantial enough to support any particular method or mode of nursing handoff delivery, even though Strople and Ottani previously recommended the use of computer technology and wireless communication to improve handoff processes. 36 Hays 38 offered handoff suggestions for staff development educators, and Messam and Pettifer 35 found that studies of bedside handoff methods had mixed results and were not suitable for palliative care: their area of interest.
Formal research, both qualitative and quantitative, has been completed on nursing handoffs for medical and surgical units. Handoffs were complex39,40 and cryptic, given at high speed and included jargon.41,42 Recently, informatics researchers examined patient-centered, multi- professional handoffs using network analysis. 40 Networks ranged from 11 to 20, were non-linear, unpredictable, and shaped by providers’ information needs. Across studies, structured formats improved information completeness using seven different formats26,43–47 and a change to bedside handoffs improved information completeness in one study. 48 However, bedside handoffs were difficult on palliative care units because of sensitive information. 27 Taped handoffs had more information omissions than verbal reports but were more congruent with the patient’s actual condition. 12 O’Connell and Penney 49 concluded that no one type of handoff was most effective because of differences in contexts, patients and nurses.
Pothier et al. discovered that nurses in a laboratory experiment had only 31% accuracy on traditional written notes after handing off information five times while a combination of verbal report with a typed sheet resulted in minimal information decrements. 46 Dowding found low average information recall rates of 27% and only a 45.2% average accuracy rate during a laboratory study comparing two handoffs with different information structures. 50 However, Dowding also found that information recall and accuracy were improved with consistent formats. 50 Randell et al. found two functions for handoff forms, one public, with relevance to an entire patient care unit, and one private – a personal workspace. 51 They argue that any computerization needs to perform these two functions to be effective. Tang et al. expanded upon the themes of public and personal space to indicate information content and how information interacts across these two spaces. 52 Handoff observations indicated that information was obtained from sources including paper, verbal, and digital.
Riesenberg et al. reported a review of interdisciplinary mnemonics, finding only four research-based articles, none of which was computerized. 31 Other authors found positive results for standardized, electronic tools for physician handoffs.53–55 However, only two authors completed evaluations of computerized handoffs for nurses. Nelson et al. created a positively received template for electronic handoffs; 56 unfortunately, it was not integrated with the local electronic health record which would impede its long-term use. Kalish et al. evaluated nurses’ perceptions about a computerized handoff template. 57
To date, no research has examined nurses’ actual use of computerized handoff forms. Thus, we conducted this exploratory, descriptive study to understand how acute care nurses used an electronic patient summary reports or EHRs during nursing handoffs.
Methods
A qualitative, interpretive descriptive approach was used.58,59 This approach is centered on an interpretative orientation acknowledging the contextual and constructed nature of health. Researchers use foundational knowledge on the topic to allow linkages to prior work, data analysis is inductive and the technique sustains methodological rigor. This study was part of a larger ethnography on nurses’ information management during handoffs on medical and surgical units. Appropriate approvals were obtained from the institutional review board, hospital chief nurses and nurse managers before data were collected.
Setting
The study was conducted in two institutions in the western USA: an academic medical institution and an oncology specialty hospital. The academic center is a 425-bed tertiary care facility with two surgical and one medical units, and the oncology hospital is a 50-bed cancer hospital with one surgical and one medical unit. These institutions employ over 1700 registered nurses, all of whom are required to use the installed electronic health record. The institutions shared a global vendor’s electronic health record; the implementation was at Stage 4 of 7 according to the Health Information Management Systems Society Electronic Medical Record Adoption Model 60 with computerized provider order entry, an electronic medication administration record, nursing documentation, results review and a picture archiving and communication system in place. Order entry and the existing electronic summary report were in use for nine months before data were collected. Appropriate approvals were obtained from the institutional review board as well as the chief nursing officers.
Sample
Nurses were selected using purposive sampling across nurse expertise, type of nurse (regular staff members or intermittent such as per diem or travel nurses), shifts and experience on the unit. Nurses were excluded from participating unless they had more than six months of nursing experience. Nurses in both facilities all used face-to-face, verbal handoffs, typically between two nurses (the nurse giving and the nurse receiving report). We sampled equally across units, shift times and durations, nursing expertise and experience.
Data collection
Data were collected on 25 different occasions from October to November 2009. A total of 93 patient handoffs were observed, involving 26 nurses giving reports on an average of 4 patients. Nurses worked 8- or 12-hour shifts, with handoffs scheduled for 0700, 1500, 1900 and 2300. The observation and interviews took place in the units at the end of the 8- or 12-hour shifts. Nursing handoffs were observed, audio taped and field notes of the unit environment were recorded 30 min before the end of shift and during the handoff. One observer captured the context of report, such as interruptions, and another recorded specific EHR screens nurses used. The observations were limited to nurses giving the report because they synthesize information from various sources to prepare for report. Nurses receiving report have different cognitive tasks. The average length of an observation was 40 minutes per nurse.
The nurses giving report were also interviewed immediately after completing handoffs using semi-structured questions. The interviews lasted approximately 30 minutes per nurse. Sample questions included: 1) Tell us how you prepare to give report, 2) What tools do you use to give report?; and, 3) Tell us about the piece of paper that you use to give report. If nurses did not use the available electronic summary report we asked them to discuss why not. The interviews also explored other aspects of current practice that were observed, such as why nurses did or did not use the computer (EHR) while giving report. Although we observed nurses before and during handoffs and saw how they prepared for report and the tools they used, we included questions about tools and handoff preparation to assure that we were observing common practices. This proved to be useful because we discovered additional information we did not observe with each nurse - writing pertinent information on alcohol pads or a scrap of paper, use of a cell phone for medication information, and we found nurses who indicated that they prepared for report throughout their shifts versus at a particular time period.
Data analyses
Audio files were transcribed verbatim, checked by for accuracy by the investigators, and blinded to protect the identities of nurses, patients, and others named in the interviews and reports. Observations were recorded by the research team as field notes during the handoff and summarized across investigators within hours after each data collection occasion. The field notes and observations were combined with the interview data and analyzed as a set. Interviews were analyzed to understand nurses’ use of the computerized nursing summary form during the handoff processes using conventional content analysis techniques 61 and Atlas ti version 6.0.
The investigators worked jointly and separately with the analysis moving back and forth among them. The investigators analyzed 8 of the 25 transcripts jointly. The first six were analyzed by all authors to develop the coding manual, category definitions and calibrate the granularity of the analyses. The remaining manuscripts were then analyzed independently by three of the authors (NS, JB and SK) using the jointly developed coding manual consisting of 33 categories. Example categories were: brains-personalized, brains-encoding, information access-at a glance, application design limitations and futuristic designs for report. Two of the transcripts were compared across raters for reliability and validity of coding. The analysis revealed similar category coding and meaning across the three researchers.
Results
Sample
The sample of 3 male and 23 female nurses had an average age of 37. The modal educational level was a Bachelor’s degree. Nurses’ experience on their specific units ranged from 1 week to 9 years, with an average of 3 years. Total nursing experience ranged from 6 months to 20 years with an average of 5.6 years. The institutions no longer employed intermittent nurses so the sample consisted of regular staff nurses.
Handoff processes
We observed similar processes on the five acute care units. Nurses looked up their assigned patients and the associated nurse who cared for these patients during the previous shift on a paper report or on a unit whiteboard. Nurses then “found” their handoff partner by actively searching the nurses’ station for the other nurse or by sitting at a computer terminal working and waiting until the other nurse approached them. All dyads of nurses conducted handoffs while seated in front of computer terminals as was the institutional policy initiated when CPOE went live. Nurses had an average of 2-3 handoff partners, with a range from 1 to 4.
We observed that nurses either printed the nursing summary report available through the electronic health record (Figure 1) or crafted a personalized paper form to use during handoffs (Figure 2). Seventeen nurses used personal forms and nine used the printed nurse summary reports. As may be seen in Figures 1 and 2, nurses wrote additional information on their forms during the handoff, highlighting material and creating customized grids of information such as important laboratory results, activities to complete or a list of medications due. From interviews, nurses indicated that they used the forms throughout their shifts by adding pertinent information as it occurred. Nurses called these tailored forms their “brains.” Despite being mandated to sit in front of computer terminals during the handoffs, we observed nurses giving the handoff relying on their personalized paper and printed electronic forms instead of the updated patient summary report in the EHR. Nurses used the EHR only to double-check information such as intake and output volumes, vital signs, physician orders or a recent pain medication. The tailored forms were then their “gold standard” of information to convey to the oncoming shift.

Example of a nurse’s computerized patient summary report
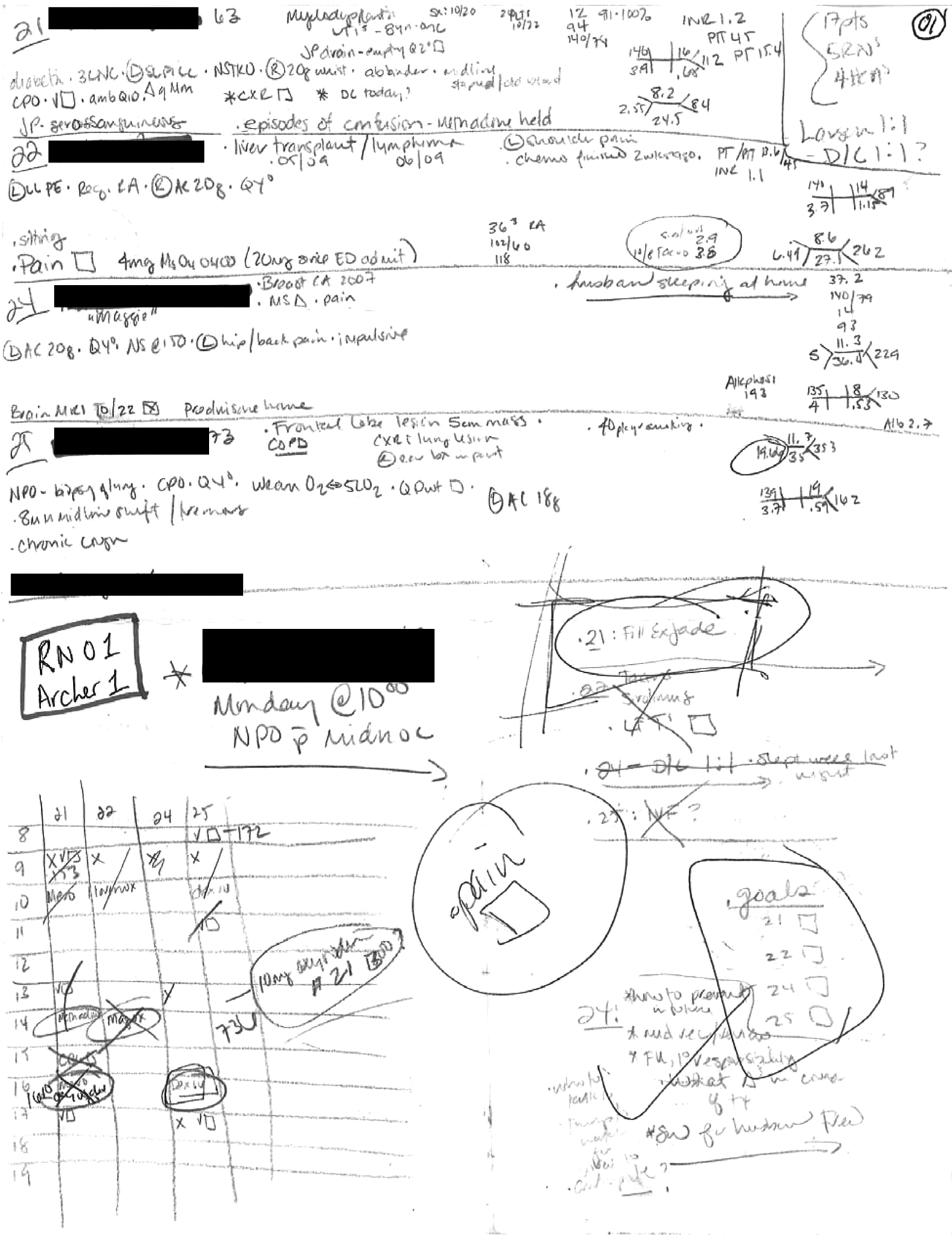
Example of a personalized paper handoff form
Incomplete electronic summary reports
The electronic health record had two generic designs for nursing summary reports: one for medical/surgical and one for intensive care units. Hospital leaders strongly encouraged nurses to use the summary report during handoffs. However, the researchers observed that the printed summary report was not widely used and found that its use had eroded over the months since installation. A nurse explained why she preferred creating her own form: “If we can’t get most of the information that we need on that piece of paper [the Nursing Summary Report], we actually miss enough that it doesn’t make it worth it.”
Nurses conveyed numerous complaints about the summary report to the researchers, particularly that it was incomplete. As one nurse noted: “The nursing summary report has only about 50% of the information that I need.” For example, the nursing summary report did not include the patients’ history; instead, the physician summary report included that information. Substituting the physician summary during the handoff would not work because it, in turn, did not include information nurses needed, such as orders and intake and output. Nurses wanted to read the patient’s history to get the full picture of the patient and understand how current medications and treatments related to their history.
The nursing summary report included a list of orders as may be seen in Figure 1; however, the orders were truncated to fit on one printed page per patient. After adverse events and feedback from clinicians, a warning was printed in small font on the report stating: “SEE CHART, INCOMPLETE CLINICAL INFORMATION”, as can be seen in Figure 1. Nurses told the researchers that they initially learned by trial and error that the orders were not complete, after they missed a medication or treatment. Also, standard order sets such as those from the pain service could consume nearly the entire space allocated for orders, leaving nurses to uncover other pertinent orders elsewhere.
Nurses spoke about other issues with the summary report. The appearance of the printed summary report was different than its on-screen display; it was also different than the way nurses were used to finding information. One nurse who used the Nursing Summary Report for two weeks reported that she had abandoned the form because its organization was inconsistent with her style of information processing:
I felt like the information - sometimes it doesn’t always make it on the same page. Sometimes it carries over to the next and it’s never really organized in a certain pattern where I can - where if I’m looking for something specific where I can just go to into this one area and there it is. I have to search for the information that I’m looking for.
If the patient had more than a few orders, little space was left for the nurse to take notes during the handoff as can be seen in Figure 1. The ability to tailor the report form and take notes during the handoff was deemed critical by nurses. As one nurse indicated:
Sometimes they don’t have all of it on there, so I just have to fill it in, but it’s just because there’s so many orders. On some patients, there are so many orders it doesn’t catch it all on the first page, so you just have to write in what’s missing.”
Last, nurses’ tasks include the ability to organize and sort activities both within and across their assigned patients. For example, in Figure 1, readers can see that a nurse wrote times medications were due as cues for tasks across the four patients.
Limited personalized information
Nurses complained that the current system did not match the way they worked. As one nurse indicated: “I really don’t like our computer system. I don’t think it works…[it’s not] a program that was designed by a nurse or someone in the medical field. It just seemed like it was somebody on the outside who didn’t understand.” Therefore, nurses created personalized paper forms that better matched the way they do work and the way they think about patient care. One nurse told the researchers: “Plus with the computer, it’s always what somebody else thinks is important, whereas with your own paper it’s what’s important to you.”
The generic nursing summary reports in the electronic health record lacked necessary tailoring. For example, if nurses cared for the patient in the past, they do not need general information about the patient, such as age, diagnosis or history. Instead, they only need to know the changes since the last time they cared for the patient. Unfortunately, the generic electronic health record summary reports are rigid and provide the same information each time they are displayed or printed.
Nurses indicated their need for information beyond the typical information pulled from EHR modules into the summary report. Rather than seeing only the last set of vital signs in the summary report, for instance, nurses wanted trended data across the last 24 hours. As one nurse noted:
I want a 12-hour overview of their vital signs, I want a 12-hour overview of what they had for I’s and O’s [intake and output] so ….we can see if anything is trending up or trending down…I’s and O’s are big on this [surgical] floor.
Data also needed to be integrated across typical electronic health record modules, certain medications (Digoxin) with vital signs (apical pulse), certain laboratory results (INR) with medications (warfarin), for example. Abnormal values need to be consistently highlighted across all data – results, vital signs, intake and output. Only the results data currently had highlighting for abnormal values while nurses had to scan existing vital sign data for abnormal values. Other pertinent information should appear – if the patient is deaf, for example.
Portability and information “at a glance.”
One of the reasons nurses are wedded to their current paper brains is because of the easy portability of paper and because they provide information “at a glance.” Nurses tucked the paper brains in their pockets and carried them throughout the shift. Nurses commented about how they always had information readily available, especially as they entered patients’ rooms:
And after you get report…you have four or five patients. You can’t remember everything. So right before I go in the room, I look at the paper. Okay, what do they have again? What wounds am I going to be looking at?…So it’s just a quick reference for me. I would never keep going to the computer and looking it up. It’s faster to have a piece of paper in front of you.
Nurses could easily consult their paper brains if patients asked questions about their care, particularly about medications. Logging on to computer terminals, even if they were in the room, was deemed too time-consuming according to these nurses. Besides, the electronic health record had too much information to wade through, making the use of in-room or computers on wheels too arduous.
Most importantly, the paper brains provided information “at a glance.” One nurse said: “But it [the Nursing Summary Report] is just too busy. It’s just too much for me. I just like the basics on my brain.” Nurses had already highlighted crucial information such as an abnormal vital sign or surgical site drainage, so they could quickly scan their paper forms to find that information as well as any other cues about patient care. If they answered a patient’s call light they could scan their forms to find that the patient was nil per os (NPO) and not allowed to eat or drink despite the patient’s ardent request. Similarly, nurses would glance at their paper brains quickly to remind themselves of the next time a patient should have a glucose level checked.
Encoding Information
A subset of nurses wanted to be able to write on a paper form. One nurse remarked:
I learn better and think better when I can write it down. And it makes it more real, in my mind, and it’s just kinda like glue that holds it in there, instead of just looking at the computer.
Nurses are afraid if they do not write down information, they will forget something important. Writing helped nurses encode that important information in their own brains: “Writing information helps you remember what you need to do.” Another nurse stated, “I’m gonna have my own sheet that I start because when you write it down, you incorporate it. On the computer, it’s a fantastic system, but it’s limited by the fact that you’re not engaged.” Writing also helped nurses organize information and assisted with setting priorities, including tasks they need to get done before going home or starting work, once they complete the handoff.
Findings across nurses and units
The findings were similar on each of the units, except for two issues. First, nurses on one of the surgical units, specializing on the care of transplant patients, used the computerized form more than the other surgical and medical units did. Their preference, they said, was based upon the fact that they did not have to copy general information such as patient demographics, the attending physician, do not resuscitate orders and the standard transplant orders. The medical units in particular found the summary report less useful because of the complexity of patients and the scarce room to write specifics about their patients. Existing orders consumed the allocated space, yet pertinent orders remained in the electronic chart.
The second difference was based upon the experience of nurses. Although the sample included fewer expert nurses than those newer to the profession, as could be ascertained by the average years of experience at five years, the nurses with higher levels of experience had developed their preferred structures over many years. They found the change to the rigid handoff form more difficult and retained their honed structures.
Discussion
This study is the first to examine nurses’ actual use of computerized handoff forms. Although some findings from this study are consistent with concepts known in human factors literature, such as the need for “at a glance” information, other findings are new. Stead and Lin described the difficulties physicians have in obtaining the “big picture of the patient” and the difficulty of finding pertinent information across modules in current electronic health records. 62 The findings here are consistent with Stead and Lin and extend to nurses. Nursing handoffs are cognitive activities that require nurses to perform information synthesis across EHR modules and multiple information sources, but nurses search for different information - obtaining the “big picture” of patients from a nursing perspective and locating pertinent information across various tools and modules typical of electronic health records. Nurses avoided these difficulties by continuing to rely on their paper forms as the “gold standard” for information to convey during a handoff despite the more timely and accurate data in an EHR.
The findings also extend beyond those of Hardey et al. 63 They documented nurses’ reliance on paper forms for handoffs and care delivery; however, their data were collected before computerized handoff forms were available. The fact that nurses continue to rely primarily on paper-based forms is a new and important finding. As mentioned earlier, current literature describes the link between handoffs and patient safety, making the attention to computerized designs a contemporary and imperative finding. The reliance on paper forms will not contribute to improvements in patient safety. Further, handoffs forms are not just another form to quickly design and disseminate. These forms are crucial to care and deserve more attention than has been devoted to their computerization to date.
This particular vendor, with installations worldwide, did not perform usability evaluations on applications nor did the facility complete usability testing despite its sophistication about informatics. This finding may not be surprising given a May 2010 report across vendors in the USA from the Agency for Health Research and Quality, 64 but adds to the evidence of the impact applications can have when they are not subjected to user-centered design principles and processes.
The findings are a call-to-action for facilities and vendors to focus attention on the design of handoff forms and to provide cognitive support for nurses in particular. Our findings indicate that the current computerized nursing summary report did not support the cognitive work of nurses during patient care handoffs in the acute care institutions studied here. Current computerized summary reports are incomplete, text-dense and do not provide the kind of “at a glance” information cues that nurses need. More importantly, these reports do not support nurses’ workflow. The information from the initial handoff is used throughout the rest of the shift, making the initial design of the report form even more critical for effective cognitive support.
Computerized summary reports need to be redesigned to match the way nurses work and think. The following section builds on the results and discusses specific recommendations for improving the design of patient summary reports for nurses on medical and surgical units, acknowledging that designing computerized support for cognitively-intense activities, such as handoffs, is a complex endeavor.
Precise tailoring of summary reports
Vendor-generated reports must be tailored beyond the typical generic reports for two types of units: acute care and intensive care. The first tailoring is to unit context with separate forms for surgical and medical patients. Beyond that, different diagnoses will require specific information. For example, generic information about surgical patients includes data about pain, last pain medication, intake and output status, ambulation, etc. However, an orthopedic surgery should trigger trends on the patient’s neurovascular checks. These capabilities are available now.
In the future, more complex functions could be available. Even nurses on the same unit do not necessarily synthesize data in the same way. One nurse on a unit may need a complete patient history, while another nurse in that same unit may forego the complete history for a brief highlight because of the patient’s current diagnosis, or because the patient is known to the nurse. Another nurse may want a complete medication profile because of the complex medications for a patient. Thus, future summary reports should be adaptive and tailored both to the patient’s diagnosis and condition, as well as individual nurses’ preferences.
Match to workflow
The technology supporting handoffs needs to match nurses’ workflow. Nurses use their paper forms throughout their shifts, rather than just while giving, or receiving, a handoff. Thus, any technology used during shift report will need to move with nurses as they travel from room to room. Computer terminals in patients’ rooms are not sufficient to fulfill this requirement because nurses in this study deemed them to take too long to access, navigate and retrieve information. Likewise, laptops and workstations on wheels were deemed too bulky by nurses in this study. Mobile devices may meet this requirement only if they fit easily in nurses’ pockets, if they are wearable devices or if they involve ubiquitous computing.
Simply providing different technology will not be sufficient. A critical component of “at a glance” information was the quickness of information retrieval that paper-based forms provided. Any technology used during and after shift report must be exceptionally quick to respond to log-ins. For example, a portable device may require only a four digit code or a proximity chip tied to the nurse’s identification badge could allow nurses to be logged-in when they have the devices with them. Suitable mobile device technology can be explored now.
Highlighting pertinent information
Any interface designed for computerized nursing handoffs needs to have the ability to highlight information that an individual nurse deems critical. This finding is consistent with those reported at a human-computer interaction conference by Tang et al. 52 The interface needs to have the ability to display trends in data with highlighted abnormal values. These also need to be tailored to the specific patient. For instance, what initially seems like an abnormal vital sign or laboratory value may actually be in range once a 12-hour trend is available. Showing trends and allowing highlighting are also capabilities currently available.
Enabling information encoding
As noted earlier, a subset of nurses in this study commented that writing on their paper forms helped them to remember information. “It helps cement it more up here [gestures to head] if you can write it down”, as one nurse commented. Nurses were particularly worried that if they did not write information down, they would forget a crucial aspect of care. They used highlighting and underlining to emphasize priorities. This finding is unique to this study and is supported by work in psychology—that information experienced in more than one mode is better encoded in the human brain. 65 The physical act of writing then helps nurses retain the information they hear. Also, the researchers observed that nurses receiving report used the act of writing to help plan tasks, indicate priorities and sift through data for pertinent information.
How encoding would be mirrored in technology could be more of a challenge. Nurses in this study reported anecdotally that they remembered less when they typed the information. This finding is consistent with the pilot study by Pothier et al. who found that verbal reports resulted in more information loss than a combination of verbal and written (printed). 46 However, future research may be needed to test this notion on nurses. Also, encoding abilities between writing and typing may be a generational issue. It is possible that younger nurses who have had computers and smart phones ubiquitously in their lives may have greater abilities to encode information through typing.
Study limitations
This study involved two institutions sharing one vendor-supported electronic health record. However, in the investigators’ experience, the existing patient summary report in these facilities is typical of vendors’ current solutions for summary reports. More importantly, this particular vendor has a world-wide presence. Improved summary reports could exist elsewhere with other vendors’ products.
Conclusions
This study explored nurses’ use of electronic health records and computerized patient summary reports during nursing handoffs on medical and surgical units in two hospitals. The results indicate that it is imperative to redesign the electronic summary reports and that different technology is needed to match the way nurses think and work. To the authors’ knowledge, this study is the first to examine nurses’ use of electronic summary reports after installation. Redesign is a critical need given the correlation between handoffs and patient safety. The areas of redesign are described: precise tailoring, match to workflow, highlighting pertinent information and enabling information encoding.