
Abstract
The response of health professionals to the use of health information technology (HIT) is an important research topic that can partly explain the success or failure of any HIT application. The present study applied a modified version of the revised technology acceptance model (TAM) to assess the relevant beliefs and acceptance of HIT systems in a sample of health professionals (n = 133). Structured anonymous questionnaires were used and a cross-sectional design was employed. The main outcome measure was the intention to use HIT systems. ANOVA was employed to examine differences in TAM-related variables between nurses and medical doctors, and no significant differences were found. Multiple linear regression analysis was used to assess the predictors of HIT usage intentions. The findings showed that perceived ease of use, but not usefulness, relevance and subjective norms directly predicted HIT usage intentions. The present findings suggest that a modification of the original TAM approach is needed to better understand health professionals’ support and endorsement of HIT. Perceived ease of use, relevance of HIT to the medical and nursing professions, as well as social influences, should be tapped by information campaigns aiming to enhance support for HIT in healthcare settings.
Keywords
Introduction
Understanding the way in which people react to the emergence of new technologies is of great relevance to the field of health informatics. One reason is that low acceptance of health information technology (HIT) applications would result in delays in, or even failure of, successful implementation HIT systems, and the achievement of relevant organizational goals, such as effective patient data-management and storage.1,2 Furthermore, resistance to the use of HIT applications would require specific policy actions to increase acceptance and perhaps familiarize potential users with the benefits of the debated IT applications. So far, research in the acceptance of various forms of IT applications, such as Web 2.0, the internet, mobile phone use applications and different kinds of software, has identified a number of key psychological variables that predict usage intentions. Specifically, perceived utility (PU), perceived ease of use (PEOU) and the attitudes towards the IT applications in question have been found to be the strongest predictors of usage intentions. The tripartite of PU, PEOU and attitudes has been well summarized in the technology acceptance model (TAM), which was originally developed by Davis 3 to assess IBM employees’ acceptance of new software. Over the last 20 years, research on the TAM has expanded considerably, and TAM figures prominently among the key theoretical approaches used to understand people’s intentions to accept various forms of information technology. 4 Furthermore, reformulations of the original TAM, and even alternative models, have been developed to account for technology acceptance in a variety of settings, ranging from e-commerce to health informatics.2–6 The development of the TAM and related theoretical approaches, their application in the field of HIT, as well as the rationale, methodology and findings of the present study, are discussed in more detail in the sections that follow.
Understanding technology acceptance
As Davis 3 mentioned in his seminal work on technology acceptance ‘information technology offers the potential for substantially improving white collar performance’ (p. 319). This is even more so almost 20 years after that statement was initially made, mainly because the applications of IT are relevant to virtually all domains of work, social interaction and entertainment. Davis’ initial work provided the cornerstone for a thriving stream of research on technology acceptance by professionals and lay people, and initiated a psychological/behavioural approach to technology acceptance issues.7–9 The legacy of Davis’ TAM3,10 is illustrated in more updated version of the TAM and alternative behavioural models to understand technology acceptance. What is important before discussing the theoretical underpinnings of TAM and its application in the healthcare setting is that technology acceptance and use is conceptualized as an expression of human behaviour. As such, the laws and mechanisms that govern other aspects of human behaviour, such as learning, acceptance of policies, attitudes and reasoned action, could potentially be extended to understand issues of technology acceptance better. This has been the main position of the majority of theoretical approaches developed to understand acceptance of technology better.
TAM: Theoretical underpinnings
The TAM was originally developed on the grounds of the theory of reasoned action (TRA). 11 The TRA posits that people are rational decision-makers, consciously choosing their course of action based on an analysis of potential costs and benefits attached to each of various behaviour alternatives.11–14 In this process, the role of attitudes, social norms and intentions are important. Attitudes represent the combination of outcome expectancies (i.e. a behaviour will lead to specific outcomes) and the valences attached to these outcomes, whereas social norms represent perceived pressure to conform to other people’s expectations or behavioural choices.14,15 Finally, behavioural intentions represent the goal intention to perform the behaviour in question and are assumed to be the most immediate precursors of action initiation.12,16
Following the rationale of the TRA, the TAM assumed that what drives people’s intentions to use IT applications is their attitude towards those applications. Davis 3 further argued that attitudes are formed by beliefs about the perceived utility and ease of use of the IT applications in question (Figure 1).
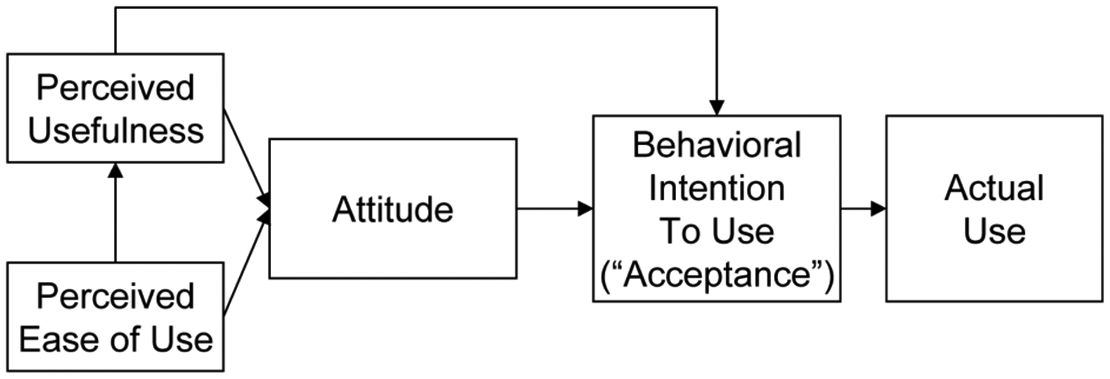
The original version of the Technology Acceptance Model. Figure taken by Holden & Karsh [3].
Numerous studies have supported the theoretical postulates of TAM, and several meta-Analyses17,18 and review articles8,19 have noted the importance of the model in understanding the process of acceptance and use of IT.
In 2000, Venkatesh and Davis 4 reconsidered the structure of the original TAM and used empirical findings to judge the importance of the models’ traditional constructs. In their revised model, known as TAM2, they excluded attitudes, but retained perceived usefulness and ease of use, as these two variables were consistently found to be strong drivers of intentions to use technology. Furthermore, the TAM2 approach added measures of subjective norms to capture social influences (Figure 2). Based on the TRA, 14 subjective norms in the TAM2 were conceptualized as indicators of social influences and, more specifically, the opinions of important others (colleagues, friends, supervisors) about an individual’s use of IT applications. 2 A recent meta-analysis showed that subjective norms, indeed, exert a significant strong influence on TAM variables and on intentions to use technology. 20 Venkatesh and Davis 4 also argued that job relevance is another important variable to be included in the TAM2. This construct reflects people’s beliefs about the applicability of the target IT applications to one’s job or daily routines at work. Other constructs related to output quality and results demonstrability of IT applications were also added in TAM2 based on the idea that those influences, along with social norms and job relevance, would predict perceived usefulness and ease of use. Therefore, compared with the original TAM approach, the TAM2 expanded considerably the range of indirect effects of distal predictors (e.g. social norms, relevance) on usage intentions, while emphasizing the central role of perceived usefulness and ease of use.
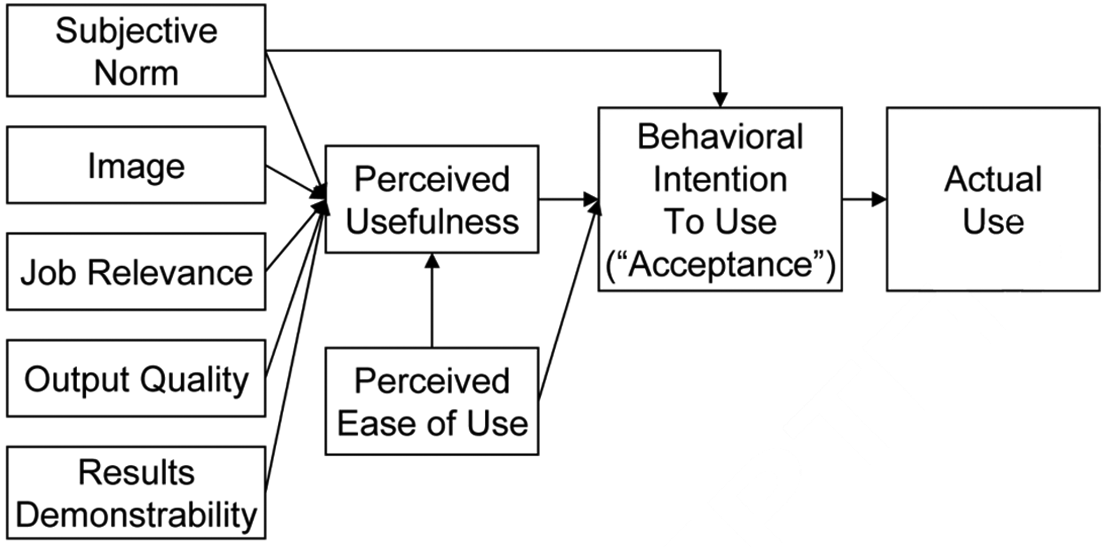
The revised Technology Acceptance Model. Figure taken by Holden & Karsh [3].
Over the last 10 years there have been numerous studies using either the TAM or TAM2 to predict intentions and the actual use of technology in several domains. A common feature of most of these studies, however, is that they do not use exactly the same measures of TAM or TAM2 variables and, in some cases, the predictors of technology acceptance are different from the ones originally proposed in the respective models.2,8 Thus, the TAM approach provides the general framework wherein new variables can be added as long as they are theoretically relevant and their addition reflects an evidence-based decision and not a haphazard choice. In more recent years, the legacy of technology acceptance literature included alternative models for technology acceptance, such as the unified theory of acceptance and use of technology (UTAUT 21 ), which has many similarities with the initial TAM approach, but differs in the content and number of predictors of intentions and actual use of technology. 2
Technology acceptance in healthcare settings
The implementation of comprehensive information systems in health care practices has proved to be a path ridden with risks and dangers. It has become evident that there are many more failure stories to tell than there are success stories—and the more comprehensive the technology, or the wider the span of the implementation, the more difficult it appears to achieve success [. . .] whether an information system is ‘successful’ or not is decided on the workfloor (Berg, 2001, pp. 143–144)
1
This statement illustrates the need and importance of stepping outside the laboratory setting to try to understand why, and how, health professionals endorse and successfully implement HIT systems in their daily work routines. Unless a system is accepted and effectively used, it is doomed to failure. 22 The points raised by Berg 1 have been addressed by researchers working in technology acceptance. As Holden and Karsh 2 noted, the TAM approach (and related ones) have already been applied in several studies in the healthcare setting.
Studies of technology acceptance in healthcare
Van Schaik et al. 23 applied the original TAM to assess physiotherapists’ endorsement of a prototype system for postural assessment. They found that the TAM core variables, namely perceived usefulness and ease of use, significantly predicted acceptance of the new device and used their findings to provide specific policy recommendations that would make the prototype device more appealing to physiotherapists (e.g. improve ease of use of the system in order to increase usefulness and, in turn, readiness to use the system). In another study, Chau and Hu 24 compared the utility of the TAM with the theory of planned behaviour 16 in predicting physicians’ acceptance of telemedicine technology. They found that the TAM was a more appropriate model than planned behaviour theory to understand physicians’ acceptance of technology and further suggested that the initial TAM structure should be modified to accommodate issues specific to the healthcare setting. These suggestions were echoed by Yi et al. 25 who used an integrated approach with key elements from TAM and other theories to assess healthcare professionals’ acceptance of a personal digital assistance (PDA). They found that a core TAM variable (perceived usefulness), along with subjective norms and self-efficacy beliefs significantly predicted usage intentions. These findings suggest that traditional TAM variables can be effectively integrated with variables derived from other theoretical approaches to better understand healthcare professionals’ acceptance of new information technologies.
The road ahead: How to improve research in HIT acceptance
Holden and Karsh 2 provided a comprehensive review of the literature on applications of the TAM and related models on healthcare professionals’ acceptance of IT, and more specifically, health informatics systems. They argued that research on healthcare professionals’ acceptance of technology would benefit from the integration of theoretical approaches with widely researched TAM variables, such as perceived usefulness. This approach follows the ‘adding variables’ principle, which is has been proposed as an effective one in deepening and broadening existing theoretical frameworks of human behaviour. 26 Nevertheless, Holden and Karsh 2 noted that the addition or integration of novel constructs within the TAM or related models should be theory-driven and evidence-based. Otherwise, the resulting behavioural models of technology acceptance might risk their parsimony and focus. Overall, healthcare provides a totally different setting for the study of technology acceptance, with obvious differences to other professional settings, such as companies and information technology organizations. As such, a model of technology acceptance for healthcare professionals should take into account, and be sensitive towards, the peculiarities of the specific professions.
The present study
Following the recommendations by Holden and Karsh 2 and the evidence in applications of TAM-related approaches to healthcare settings, 25 the present study set out to assess the predictors of HIT among nurses and medical doctors. The theoretical underpinnings of the study derive from Venkatesh and Davis’ revised TAM 4 and from related studies in healthcare. Specifically, we tested empirically a model including TAM2 variables, such as perceived usefulness and ease of use, job relevance and subjective norms. We also included computer anxiety, which has theoretical relevance to technology acceptance and has been assessed in studies of TAM2. 9 Also, in further extending the views by Venkatesh and Davis 4 and Yi et al. 25 regarding the importance of social influences in technology acceptance, we expanded the measures of social norms to include the concept of descriptive norms. Unlike subjective norms that reflect perceived approval of an individual’s course of action (e.g. technology acceptance) by others, descriptive norms reflect the perceived prevalence of a target behaviour in other people. 27 Thus, descriptive norms in the field of technology acceptance would resemble measures of perceived use (or potential use) of technological innovations by other people, usually individuals with similarities to the person (e.g. colleagues, or friends).
Based on previous research,2,4,9,25 the following hypotheses were formed.
PU and PEOU will significantly predict healthcare professionals’ intentions to use HIT systems.
Subjective and descriptive norms, relevance and computer anxiety will predict usage intentions over and above the effects of PU and PEOU.
Methodology
Sampling
A two-stage cluster sampling method was used. In the first stage, three clinics in the city of Skopje were randomly selected. In the second stage, all health professionals (nurses and medical doctors) employed in the selected clinics, were eligible to participate. Overall, 200 questionnaires were administered, 169 were returned, yielding a high response rate (84.5%), and 133 questionnaires were eligible for further analysis. Those excluded from the analysis were either partially completed (major parts of key variables were missing), left blank or completed by non-health professionals. Of the 133 respondents, 51.1% were medical doctors (females = 80.9%, mean age = 44.3 years, SD = 10.7) and 48.9% were nurses (females = 96.9%, mean age = 40.1 years, SD = 9.83). In compliance with international standards for ethics in research involving human subjects, all participants were informed about the aims and purposes of the study, their anonymity and confidentiality of responses, as well as their right to withdraw their data from the study at any point without negative consequences.
Measures
A structured questionnaire was used, including measures of demographic characteristics (age, gender), variables of the standard TAM (perceived usefulness, perceived ease of use and usage intentions), and variables derived from related studies on the extension of the TAM (computer anxiety, relevance, self-efficacy, subjective and descriptive norms, and familiarity/use of computers). All the measures were initially developed in English and the translation-back translation method was used. 28 At the top of the questionnaire, a brief definition of HIT systems was used (‘Generally, by Health Information Technology (or Health IT) we mean the application of information processing involving both computer hardware and software that deals with the storage, retrieval, sharing, and use of health care information, data, and knowledge for communication and decision-making’) and participants were asked to provide their answers by imagining that they were required to use HIT systems in the future. Prior to data collection, the questionnaire were given to a small sample (n = 5) medical doctors and nurses to assess the comprehensiveness of language, as well as the understanding of the items and completion instructions. Response options in the measures described below were coded on a seven-point Likert scale (1 = strongly disagree, 7 = strongly agree), unless otherwise stated.
PU was assessed as the mean score of four items describing several aspects of perceived usefulness from using the HIT applications (e.g. ‘using the Health IT applications will increase my performance’). The measure was derived from Venkatesh and Balla 9 and higher mean scores indicated higher perceived utility of HIT.
PEOU was also measured with the mean of seven items reflecting several aspects of ease of using HIT (e.g. ‘I would find Health IT applications easy to use’). The measure included technology-specific ease of use and more general beliefs of self-efficacy in using successfully the HIT systems, and was derived by Venkatesh and Balla, 9 Venkatesh and Davis, 4 and Yi et al. 25 Higher scores denoted higher perceived ease of using HIT systems.
Usage intentions were assessed with the mean score of three items reflecting the behavioural tendency and willingness to use HIT systems (e.g. ‘I intend to use Health IT systems if they are implemented’). The items were derived from Venkatesh and Davis 4 and Yi et al., 25 and higher scores reflected stronger intentions to use HIT.
Computer anxiety was measured with the mean of four items derived from Venkatesh and Balla, 9 describing different feelings of anxiety and nervousness related to computer use (e.g. ‘working with a computer makes me nervous’). Higher scores reflected greater anxiety towards interaction with computers.
The relevance of HIT to the job was measured with two items taken by Venkatesh and Davis (e.g. ‘In my job, usage of Health IT systems would be relevant’). 4 Higher scores reflected greater perceived relevance of HIT to the job tasks of medical doctors and nurses respectively.
Subjective norms were assessed with the mean of three items derived from Venkatesh and Balla 9 and Yi et al., 25 and reflected the perceived acceptability and endorsement of HIT systems by colleagues and important others. Higher scores reflected greater perceived social approval and endorsement of HIT.
Descriptive norms were assessed with a single item adapted by related research on normative influences on behaviour 27 and required participants to estimate how many of their colleagues would use HIT systems if they were implemented. Response options were coded on a five-point continuous scale (1 = none of them, 5 = all of them), and higher scores reflected greater perceived potential use of HIT systems by colleagues.
Computer use was assessed with a couple of items derived from Teo et al. 29 One question asked participants whether they had access to a personal computer at home or at work (with yes/no response options). Two open-ended items asked participants to report the average years and the average time per day they use a computer.
Procedure
The questionnaires were distributed to medical doctors and nurses by the administration staff or clinical directors of the participating clinics. No time limits were imposed and survey completion lasted approximately seven minutes. The completed questionnaires were returned into a sealed envelope to one of the co-authors.
Results
Reliability and construct validity of the measures used
Cronbach’s alpha (α) was estimated for the TAM-related multi-item measures used in the study. All measures had high internal consistency reliability (α > 0.70). Furthermore, construct validity was assessed by the intercorrelations between the TAM-related variables. All correlations were statistically significant and in the expected direction according to the TAM theoretical approach. The findings and the mean scores and standard deviations of the measures used are presented in Table 1.
Intercorrelations, mean (M) and standard deviation (SD) scores, and reliability coefficients of the measures used
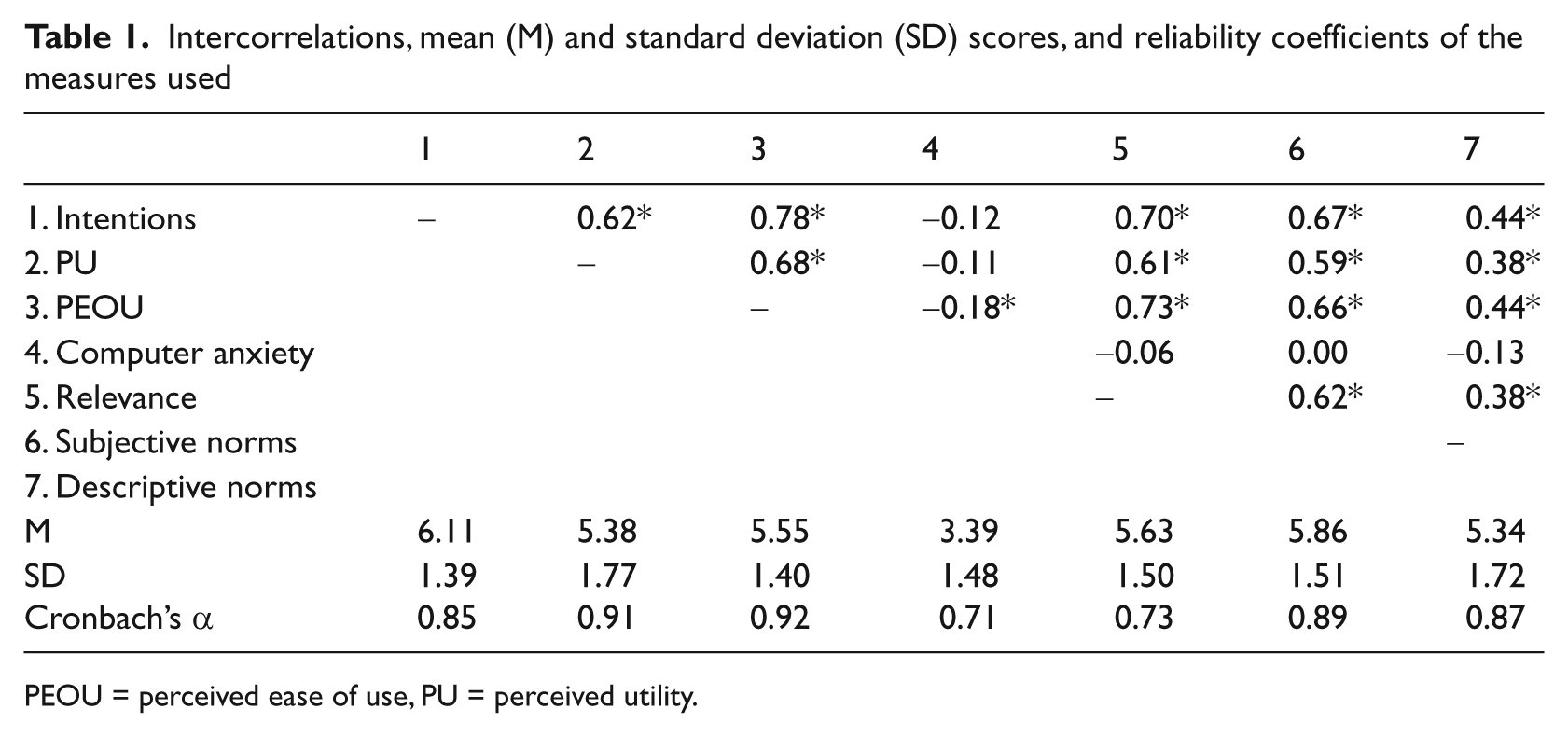
PEOU = perceived ease of use, PU = perceived utility.
Differences between nurses and medical doctors in HIT acceptance
One-way ANOVA was used to assess differences between nurses and medical doctors in mean scores of TAM-related variables. The analysis showed that there were no statistically significant differences (p > 0.05) between the two groups, except for average years using computers [F (1,122) = 21.43, p < 0.001] and average time per day spend on using a computer [F (1,114) = 6.58, p < 0.05], where doctors reported higher scores than nurses.
Predictors of HIT acceptance
A multiple linear regression analysis was used to assess the psychosocial predictors of HIT acceptance. The criterion variable was usage intentions and the predictor variables included perceived usefulness (PU) and ease of use (PEOU), computer anxiety, relevance and social norms (descriptive and subjective). The stepwise method was used and an overall significant model [F (3,124) = 88.2, p < 0.001] emerged in three steps, explaining 67.9% (Adjusted R2) of the variance in intentions to use HIT systems—a large multivariate effect size (f2 > .4) according to Cohen. 30 The findings showed that the significant predictors of intentions to use HIT at the final step of the analysis were PEOU, relevance and subjective norms. The results of the regression analysis are summarized in Table 2.
Psychosocial predictors of health information technology (HIT) acceptance
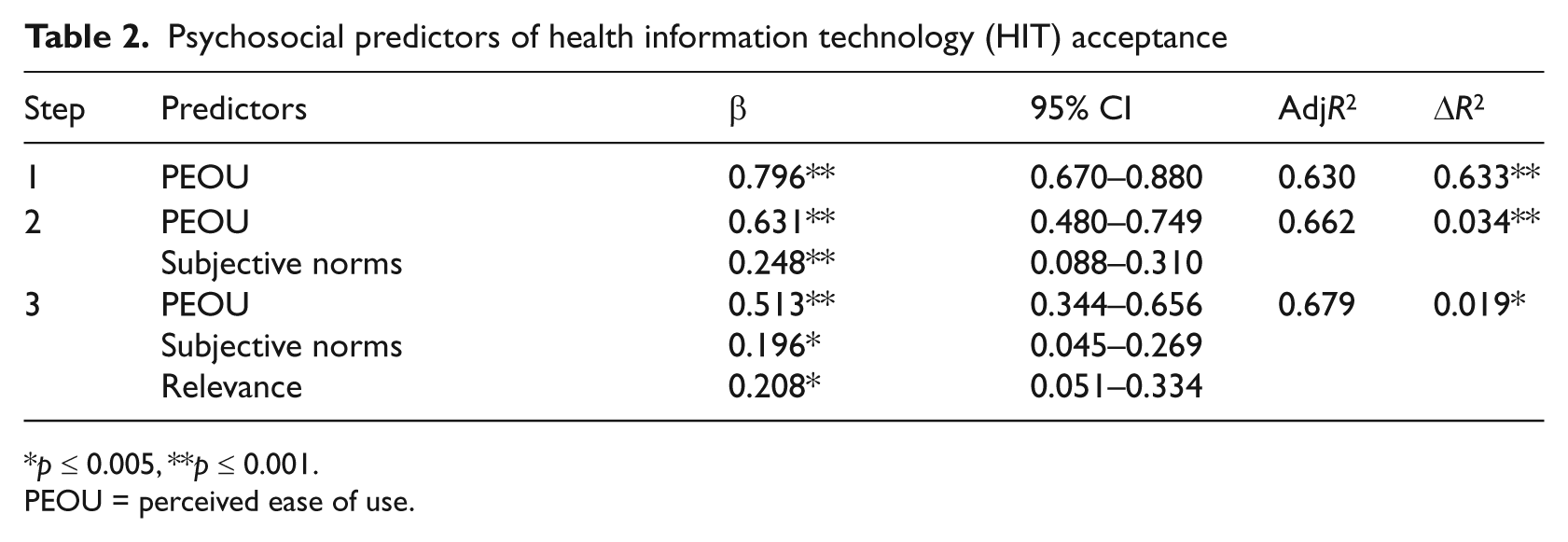
p ≤ 0.005, **p ≤ 0.001.
PEOU = perceived ease of use.
Discussion
The present study set out to assess a modified version of TAM2 4 among healthcare professionals. It was hypothesized that healthcare professionals’ intentions to use HIT systems would be predicted by core TAM2 variables, such as PU and PEOU. The findings from the regression analysis, however, partially supported this hypothesis, as only perceived ease of use, and not usefulness, significantly predicted HIT usage intentions. This is an interesting, and rather novel, finding as perceived usefulness has been found to be among the strongest predictors in numerous studies of TAM or TAM2.2,17,19,25 Perhaps the sample used in the present study placed higher value on issues of competence and skills needed to use HIT systems effectively and attached lesser importance to the actual utility and usefulness of HIT in their daily job routines. This finding has interesting implications for policy-makers and HIT system designers, because it shows that information about the effective use of HIT systems, the development of user-friendly applications and the provision of hands-on workshops to enhance familiarity and competence skills among potential users of HIT systems could potentially bring changes to perceived ease of use and, in turn, lead to higher acceptance.
The effect of job relevance was also significant, showing that the more healthcare professionals know about the applicability of HIT systems on their daily work routines, the more likely they are to accept those systems. This finding shows that prior to the implementation of HIT systems in the healthcare setting, it is advisable to educate potential end-users about the applicability of the systems to their work. This may include information about how the tasks can become easier, for example, by automating processes; how the workload can be reduced, for example, by reducing duplication of data entry; or become more manageable, for example, by improving patient booking systems; and how IT can improve safety and outcomes, for example, by reducing medication errors.
Furthermore, we extended the notion of social norms of the TAM2 approach by considering the influence of descriptive norms (i.e. perceived prevalence of HIT acceptance by others), alongside subjective norms (i.e. perceived acceptance and approval of HIT by others). The results showed that subjective, but not descriptive norms, predicted usage intentions. Thus, our initiative to expand the notion of social influences originally found in TAM2 applications was not supported by the data. This contrasts with previous research on the broader social psychological and behavioural science literature, in which descriptive norms have profound effects on a range of behaviours, including pro-environmental action, substance use and exercise participation.27,31,32 A potential explanation of the non-significant effect of descriptive norms on intentions in the present study could be that the behaviour in question (i.e. use of HIT systems) was not established in referent others. Thus, unlike the psychological literature mentioned above where descriptive norms are assessed in pragmatic terms (i.e. a proportion of referent others performs or is assumed to perform a target action), in our study the referent others did not actually use HIT systems. Rather, the question we used to assess descriptive norms was more hypothetical in nature, asking respondents to estimate the prevalence of their colleagues who would potentially use HIT systems. Therefore, we should not rule out the effects of descriptive norms on HIT acceptance by health professionals. Rather we should re-examine the effects of descriptive norms in a context where HIT systems are actually implemented, so that estimates of acceptance among others is more realistic and less bound by purely subjective hypothetical assumptions.
Finally, based on Venkatesh and Balla, 9 we assumed that HIT acceptance could be influenced by computer anxiety – that is the extent to which end-users have difficutly interacting with computers and new technologies. Nevertheless, the findings showed that computer anxiety did not predict HIT use intentions. In fact, as shown in Table 1, the mean score of computer anxiety was rather low (3.39 in a scale ranging from 1 to 7), thus suggesting that computer use is not seen as a particularly stressful task. Of course, the present findings apply to the specific sample used and further research is needed to verify our results.
Conclusions
In line with previous studies of technology acceptance in healthcare settings,3,25 we concur that a modified version of existing TAM approaches is needed in order to better understand healthcare professionals’ acceptance of HIT systems. The roles of perceived ease of use, job relevance and social norms seem important, thus showing that TAM2 is perhaps more appropriate for use in healthcare settings than the original TAM. Furthermore, the present findings point out that specific action should be taken to educate healthcare professionals about the potential applicability of HIT in their daily work routines, as well as to enhance their efficacy/competence skills in relation to computer interaction. Finally, creating an organizational culture that promotes and endorses the use of novel IT application could positively impact social norm beliefs thus producing greater usage intentions. These conclusions are relevant to the specific national sample used in the present study, but further research will show whether these arguments are valid in other cultures and ethnic samples.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.