
Abstract
Background
Delivering adequate quality care remains a challenge in many low-and middle-income countries (LMICs), especially for people living with type 1 diabetes (T1D), requiring a complex treatment regimen. Digital health solutions, including electronic medical record (EMR) systems, have shown potential to improve delivery and quality of care but still require a successful implementation.
Objective
To analyze the adoption of a newly implemented EMR system in Rwanda from the perspectives of individuals with T1D, health care providers, and experts.
Study design
A qualitative study was conducted using the Diffusion of Innovation (DoI) theory to guide the focus of the analysis. A data triangulation strategy was used to gain multi-dimensional insights, involving in-depth interviews and participant observations with T1D individuals, EMR system users, and experts (with varying levels of acquaintance with the EMR system). Experiences of early adoption of the EMR system were explored through thematic analysis guided by the DoI theory.
Results
In general, all the participant groups had a positive attitude towards the EMR system, believed to increase the likelihood of a successful implementation. The system was described as user-friendly and improved workflows, data quality, and patient care. The main concerns to successful adoption were related to the maintenance and long-term sustainability of the system.
Conclusion
The EMR system showed great potential, was valued by users, and was positively believed to have potential to improve care and outcomes for patients. However, sustainability aspects must not be overlooked when assessing the adoption and use of an EMR system.
Keywords
Introduction
Importance of type 1 diabetes and its management in Africa
Type 1 diabetes (T1D) is one of the most prevalent endocrine and metabolic conditions in childhood and requires strict management.1,2 According to the IDF Diabetes Atlas 2021, the number of individuals with T1D under 20 in sub-Saharan Africa (SSA) has more than doubled since 2019, reaching 51,000, with an annual incidence of around 19,000.3,4 However, due to a lack of accurate and high-quality data, T1D incidence and prevalence rates, as well as the burden of complications, remain largely unknown in much of the region.2,5,6 Without continuous follow-up and effective disease management, individuals with T1D are at increased risk of diabetes-related complications and premature mortality.5,7,8 Implementing a systematic approach to data collection and patient monitoring could significantly improve the management and outcomes of T1D.
Current care processes and roles
Rwanda Diabetes Association (RDA) has been the main health care provider for people living with T1D in Rwanda since 2009. 9 Individuals are typically diagnosed with T1D at the local health facility, the district hospitals, at a private clinic, or the RDA clinic upon presentation with symptoms. RDA is responsible for the continuous follow-up of individuals with T1D for treatment and control purposes and operates according to national diagnosis and treatment guidelines. RDA has one clinic in Kigali and collaborates with the non-communicable disease (NCD) clinics at the district hospitals throughout the country. For individuals living outside Kigali, a team of diabetes nurses and educators from RDA conduct quarterly and annual visits to the district hospitals, providing treatment and care. 10
Despite these efforts, the management of T1D in Rwanda faces numerous challenges. Limited resources, lack of education and awareness about the signs and symptoms of T1D, impede regular monitoring and effective disease management. The health infrastructure, particularly in rural areas, is inadequate, leading to unreliable access to healthcare facilities, diagnostic tests, and a consistent supply of necessary medications and monitoring supplies. 11 Additionally, access to specialized diabetes care is limited, and the lack of accurate data on T1D complicates understanding the true burden of the disease and its complications. This data deficiency underscores the need for more comprehensive research and data collection efforts to address treatment gaps and inform policy and intervention strategies. 12
Technological solutions and EMR systems
Electronic medical records (EMRs) play a crucial role in health service delivery by collecting, storing, and displaying client information. Access to and use of this collected health data is essential for sustaining and providing high-quality healthcare. 13 EMRs serve as a decision support tool, guiding the health care professionals (HCPs) in making better-informed decisions for patients. This is achieved by providing comprehensive patient information, including medical history, previous treatment regimens, test results, and other critical data.14,15 The use of EMRs is believed to improve data quality, workflow efficiency, and treatment compliance, leading to better care and outcomes. 16 However, the success of these systems largely depends on their proper implementation, user training, and acceptance by healthcare professionals. 17 Studies evaluating the implementation and use of EMR systems have shown significant improvements in healthcare delivery, patient safety, care coordination, and informed decision-making. 6
Despite the increasing use of EMRs for disease management and health systems strengthening, their use is still limited in most of sub-Saharan Africa (SSA).18,19 Existing EMRs have primarily focused on infectious diseases, such as HIV/AIDS, with very few targeting chronic diseases. 20 Widespread adoption of EMRs in SSA faces challenges including limited digital infrastructure, low digital literacy, technology cost considerations, and cultural barriers. Further research into the factors that facilitates or hinder the adoption and use of EMRs is needed—beyond disease verticals that are historically well-funded and which have well-established health infrastructure. 19
Contextual background and study purpose
Between February 2021 and February 2022 local stakeholders and software developers designed and developed an EMR, Electronic Diabetes Medical Records System (EDMRS), system for the clinical management of T1D. This work was funded by WDF (WDF20-1740) and the extensive stakeholder engagement, iterative design phases, and contextual understanding that guided the platform development have been described in a previous publication. 21 The platform serves as a vital tool for RDA HCPs during routine clinical encounters at the Kigali clinic. Additionally, it is employed for mobile consultations during quarterly and annual visits, facilitating the treatment of T1D patients at the 42 district hospitals located outside of Kigali. The early launch phase between February 2022 and May 2023 included training of HCP users and the establishment of ongoing support mechanisms including a hotline for immediate concerns and routine bi-monthly meetings to discuss potential system updates. Currently, the platform is only used by HCPs employed by RDA and the module has not yet been integrated into national health information platforms for wider use by national health system HCPs. Discussions about system integration are ongoing and will be informed by research into the experiences of early adopters and insights into the outcomes of patients enrolled in the T1D EMR.
In this study, we investigate user experiences adopting and incorporating the EDMRS into routine clinical care for people with T1D. The study also identifies potential barriers and enablers to its implementation from a diverse range of stakeholders.
The electronic diabetes medical records system
The EDMRS is an innovative web-based SQL system. Currently, the system is only developed for the use of RDA; however, an Application Programming Interface (API) has been developed to eventually connect it to the national health management information system. The system was developed using open-source software including Ruby on Rails, Java, Java Script, and Angular, which are all used to build web applications and websites. The system is maintained by the platform development team following standard maintenance practices. Some of the key features of the system are; user authentication and account management, patient registration and clinical data collection, patient appointment management, Short Message Service (SMS) notifications and reminders, and the generation of summary reports on aggregated and individual levels.
Theoretical framework
In this research, we focus on understanding factors that encourage or limit the adoption of the EDRMS for T1D management in Rwanda using Rogers Diffusion of Innovation (DoI) Theory.
22
The adoption of the EMR system by HCPs is a critical “first factor” in its successful implementation. In this article “Adoption” meaning the extent to which users support, accept, perceive, and utilize the EMR system. A key element in bridging the implementation of the new technology with user acceptance is to engage frontline users and those impacted by the intervention. In this study, the users of the EDRMS are HCPs and individuals with T1D. The adoption of technology into healthcare systems relies on human factors, making the DoI theory a useful assessment tool given its acknowledgment of the individual's response to the intervention. The theory was used to identify meaningful themes related to the adoption of the EDMRS, including potential barriers and enablers to its implementation. The analysis will focus on the following dimensions inspired by the DoI theory and an additional two* dimensions considered important for a successful adaption to the EDRMS system in an LMIC context:
The extent to which the EMR can be tested and modified.
Methods (study design and setting)
Study design
Multiple data sources (interviews, participant observations) were used to get a more comprehensive and reliable understanding of user experiences. The research was undertaken in five health facilities in three regions from 19 April 2023 to 17 May 2023. Sites were conveniently selected to maximize the participation of HCPs and people living with T1D.
Participants and recruitment
Participants were selected using purposive and convenience sampling approaches. This strategy was adopted both to source data from specific people with relevant knowledge and experience, and to collect data from an easily accessible and available group of people where purposive sampling was not possible. The study participants are defined in the following three target groups:
Individuals with T1D; whose personal and clinical data are being captured and stored in the EDRMS and used by HCPs for caregiving purposes. The participants were purposively selected from the RDA clinic and at four district Hospitals (Remera-Rukoma, Nemba, Kinihira, and Byumba) located throughout the country, representing both sexes and a variety of ages. Individuals diagnosed after the implementation of the EDMRS were excluded from the study as they did not have any experience with old procedures before the initiation of the system. HCPs using the EDRMS; the RDA staff either working as nurses, doctors, or project managers. Participants were recruited by convenience sampling as the users were limited to those working at RDA. Experts; were purposively recruited based on their knowledge and expertise related to T1D, technology, and the political landscape of health system strengthening. We included an endocrinologist, who, despite working at a referral hospital not utilizing the EDMRS, provided valuable perspectives on its potential impact on T1D management. Software developers offered an understanding of the system's functionalities that could support positive attitudes and adoption, while MOH officers contributed insights into organizational support and policy issues.
Data collection
In-depth interviews and clinical observations were conducted 9–10 months post-system deployment, allowing users sufficient time to interact with the system across clinical contexts and to fully explore its features. The interview guide was developed based on the dimensions mentioned under the theoretical framework and included open-ended questions designed to explore key themes related to the implementation EMR system. This approach allowed for flexibility in probing deeper into specific areas of interest while ensuring that all relevant topics were covered.
All interviews with T1D individuals were recruited face-to-face and participant observations were conducted at health facilities during routine care visits. This provided an opportunity to investigate the interaction between the two participant groups—T1D individuals and HCPs—as well as their interaction with the EDMRS. All users and experts were invited by e-mail or WhatsApp message, and interviews took place at the location of the participants’ choice. Data were captured either using audio records and by taking notes during the interviews or the participant observations. All user and expert interviews were conducted in English by the primary investigator NB (Female, MSc, Public Health and Epidemiology, Research Associate and PhD Student, World Diabetes Foundation and University of Copenhagen) and for all interviews the relationship was established prior to the study. Interviews with T1D individuals were conducted by a native investigator (CG) in the local language [Kinyarwanda] using simultaneous translation into English captured by principal investigator NB. The relationship was established during the interview. A summary of the research activities and research participants is described in Table 1.
Summarized research approach.
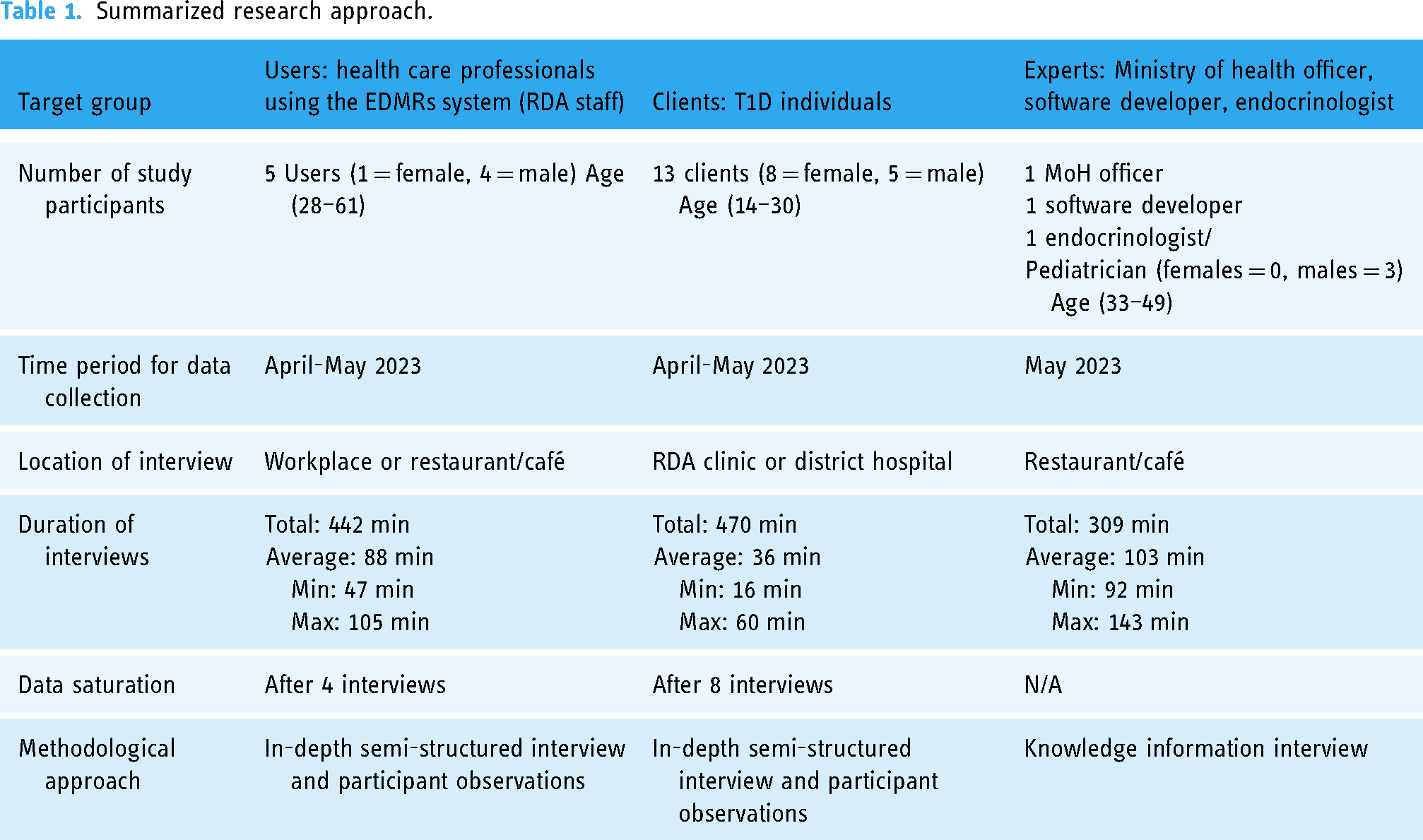
HCP user and T1D experience interviews were conducted with HCPs (n = 5) and T1D patients (n = 13). Interviews were conducted until thematic saturation was reached—which was estimated to be between 5 and 10 interviews given the narrow scope of the topics. Semi-structured interviews explored interviewees’ perceptions of adopting, using, and interacting with the EDMRs. Interview guides were developed to conduct interviews with both practitioners and diabetes patients. The interview guide included queries about the perceived benefits, challenges, changes, concerns, and unclarities related to the EDRMS.
Participant observations provided insight into the HCPs use of the system while conducting clinical consultation, including retrieving patient's clinical history and collecting their data into the EDMRS. The primary investigator NB shadowed participating practitioners for 25 h, including at least 65 clinical consultations with T1D patients. The researcher observed practitioners’ clinical consultations, environment, duties, relationships, and interactions with the EDMRs. Field notes were recorded using a structured observation guide.
Expert experience interviews were conducted with an MoH official (n = 1), a software developer (n = 1), and a pediatric endocrinologist (n = 1). Semi-structured interviews explored interviewees’ views on the factors contributing to a successful implementation, as well as their perceptions of HCP's attitude towards the EDRMS. The interview guide contained questions related to; potential facilitators and barriers, risks and concerns for failure, advantages, differences in care, uncertainties, and any experiences or insights that could be beneficial for enhancing the EDRMS going forward.
Data analysis
All data were coded by NB into themes using thematic analysis guided by the DoI theory. A deductive approach was employed, as the themes were pre-determined based on the theoretical framework. Data from each user group were initially coded separately. Themes were identified by analyzing similarities and differences across responses, and the frequency of agreed-upon similarities and differences was used to create hierarchies of identified themes. Although a structured approach to data saturation was not explicitly employed, we observed that no new insights were emerging after four HCP interviews and eight T1D individual interviews, as the themes identified were consistently repeated across participants without additional unique information being uncovered. However, it should be noted that the limited number of interviews with experts was not enough to achieve saturation in that group. Participants did not give any feedback on the findings.
Results
Findings were structured into three themes as guided by the DoI thematic framework: (1) acceptability/compatibility, (2) relative advantage, (3) complexity and reinvention, and a fourth theme that emerged from the thematic analysis (4) fidelity and sustainability. Within each theme, sub-themes were identified, and the experiences and perspectives of different user groups were explored. The results are summarized in Figure 1.

Summary of the themes, sub-themes, and key insights from the three participant groups.
Acceptability/compatibility
User satisfaction
Most participants had a positive view of the EDMRS system. HCPs found the system aligned with their needs and workflows, and their involvement in development increased system ownership. HCPs expressed a high level of satisfaction with the EDMRS, highlighting its ease of use and the efficiency it brings to their daily tasks: Quote HCP A: I prefer using the system over writing everything on paper forms and then transferring the data into Excel sheets. Now we also don’t have to print forms, bring them to the consultations and log it in cabinets afterwards
This sentiment was echoed by several other HCPs, who appreciated the streamlined data entry process and the reduction in manual paperwork. From participant observation, it was noted that no paper forms were used during the data collection process, indicating a successful transition to the digital system and supporting the feedback from HCPs. Experts agreed the system met user needs, and noted high acceptance and early adoption among RDA staff: Quote Expert A: Early adopters… fans - the open-minded people. They see the potential benefits, have positive attitude and are more positive towards change. From RDA it seems all have been early adopters. They really wanted the system.
Another Expert suggested that some might belong to the “early majority,” a group that initially exhibits slight resistance to new technology but quickly adapts following the lead of early adopters. Quote Expert C: From the beginning, I had a feeling that [Nurse] was not ready to take the chance, but now she seems very happy. In general, people have been curious about the system, and they believe it improves the situation.
Data protection
Users appreciated the EDMRS system's secure data storage, access controls, and audit trails, which ensured data access only to authorized users. This was seen as an improvement over Excel sheets and paper registries, which were more vulnerable to security breaches and data loss. Experts concurred, noted that the EDMRS, with its role- and responsibility-based access offered better data protection. However, they also highlighted the need to safeguard large amounts of sensitive patient data from unauthorized access, misuse, and potential discrimination: Quote Expert A: One of the concerns we need to consider… data security… because health care information can be misused for malicious intends. Quote Expert C: Denying people services or opportunities based on their health information would be a potential risk. Data can also get hijacked, and patients can be blackmailed to give money to preserve their data for not being used against them.
Despite acknowledging potential risks of the EDRMS, the consensus was that its benefits for patient care outweighed these risks. Clients also expressed confidence in the system and trusted their data would be used for beneficial purposes. This trust and acceptance was linked to RDA's long-standing responsibly and care for T1D individuals, which was mentioned by several clients: Quote T1 Individual A: We trust what they [RDA] do for us, why wouldn’t we also trust how they keep and use our information. We know they are there for us. Quote T1 Individual B: I only doubt for the data that were kept on the papers – it can disappear, but in the system, they can keep the data safe. I now trust the care more because RDA has recorded and kept my results from last time.
SMS functionality
The SMS functionality, designed to improve clinical attendance and patient follow-up, was widely valued by individuals with T1D. All recipients found the messages comprehensible and helpful in remembering appointments and test results. Many clients felt that this feature made them feel acknowledged and significant. All who received the message reported it was easy to understand and helped them remember their appointments and test results. Several clients expressed that it made them feel considered and important: Quote T1 Individual C: When I received the message from RDA, I understood it was special treatment and the right time to go to the clinical visit – e.g., I knew they were going to take my blood sugar test.
The long travel distances to the hospital were costly, often requiring clients to take a full day off from school or work. Some clients mentioned that receiving an SMS reminder had helped them convince their parents or teachers to prioritize the appointment: Quote T1 Individual B: I showed my parents that I need to go to the hospital – I use it a as a proof, so they believe me that I have to go.
However, one client expressed concern about potentially losing or breaking their phone, preventing them from receiving or reading the message. They suggested that a phone call would better ensure that the message was delivered and understood—while an SMS would serve as a valuable supplement.
Relative advantage
Informed decision making
The relative advantage of the EDMRS was most evident from a User's perspective. However, all participant groups agreed that the system's primary benefit was its ability to inform patients about their condition and provide personalized recommendations based on their individual data. One expert highlighted the value of accessing patients’ clinical history for comparative analysis across visits: Quote Expert C: I saw in the system, the left side, the measures of last time, this is very good for the people who provide care. They can use it for comparative purposes.
Clients also reported positive changes in care, including better access to medical data and increased self-involvement. The T1D individuals appreciated the convenience of having their information securely stored and easily accessible to healthcare providers as needed: Quote T1 Individual D: Now I can just ask RDA about my data at any time. Before I had to carry around a notebook or paper – which can be lost or I can forget it. Today they [RDA] can always find it and give it to me. The idea is to keep the data in a secure way and be able to look at the information when it is needed.
The data provided by the system improved communication with HCPs and helped Clients to better understand their disease and to make informed decisions about care management. They could monitor their progress and make adjustments based on data-driven recommendations from the HCPs. Quote T1 Individual A. We have a better treatment, because they [RDA] tell the exact information from previous visits and it is used in the care. The information from last time was kept and compared to this time. Last time my HbA1c was 8%, today it's 9.7%. Why? I will monitor my blood sugar levels more closely and not assume that I know. I will think about what has changed in my lifestyle so I can get it back down.
Aligned with the Client's perspective, Users also reported a shift in care provision approach and data usage. The system facilitated easy access to patient data, including medical history and test result, enabling comparisons with previous visits. This data-driven approach bolstered the confidence of HCPs: Quote HCP A: It makes me confident when I communicate and discuss the results with the patient. The data help teaching the patient how to better manage the disease.
Tracking and patient follow-up
Users also noted that the EDMRS implementation facilitated the tracking of patients. The system allowed the RDA to monitor attendance, identify irregularities, and track patients who missed appointments using the registered contact information (such as personal, relatives, and community health worker's phone numbers, address, and primary points of care). Quote HCP B: You can locate the patient, see where the patient lives and for how long the patient has been missing the treatment. It is a problem we have had for a long time… The system is the best solution to follow the patients.
Overall, the EDMRS was believed to improve patient follow-up procedures by providing an overview of which patients were missing and for how long—a feature that was lacking in the old procedures.
Efficiency and optimized workflow
Users reported that the system enabled more accurate and efficient data entry, as HCPs could enter data directly into the system. Excel sheets and paper-based registries required more manual effort and were more prone to errors. The EDMRS ensured that critical data were collected and introduced data validation on certain indicators. Quote HCP A: Errors are easier to identify with the system. We have mandatory cells to fill out and the system give us alerts if you forgot to fill out critical information. We also gain time - I spent a lot of time filling out papers and afterwards transfer the data to excel. Now we can spend more time talking to the patients.
Users also reported that the EDMRS saved them time on data transfer and repetitive data registration. The system stores all client information, and therefore, information that never or rarely changes were only collected when relevant. This contrasted with paper forms that required some information (e.g. name, gender, phone number) filled out every time for each clinic visit. The new data collection procedures were believed to streamline workflows and increase convenience for the HCPs and clients. Quote HCP B: Digital solution as the EMR system, its quick, easy to use, it captures everything, and you don’t have to repeat data collection on some variables. Before, the patient even asked why the same questions were repeated. They don’t understand why we kept asking the same questions.
However, one User mentioned that the EDMRS required more information than the paper forms, consequently taking more time. However, it was still believed that the improved data quality offered by the system justified the additional time investment. Quote HCP C: We are collecting more information now in the system. Maybe writing and using the paper form would take less time, but the data quality is much better, so I see it's worth it.
Diabetes monitoring and research
Both Users and Experts mentioned that the system-generated data could be used to create cohort reports, providing insights into T1D epidemiology, including prevalence, incidence, and treatment quality. It could also enhance understanding of disease progression, optimal treatment, and potential risk factors. Additionally, the data could help prioritize resources and develop targeted interventions. Quote Expert A: If we want to know if less than 10% do not have the care they need – the system can easily provide that information, and we can target the care better.
This perspective was shared by Users, who expressed that the system could help monitor disease management over time and if targeted efforts are needed.
Complexity and reinvention
The interaction between the RDA staff, T1 individuals, and the system was smooth and effective, indicating its feasibility and practicality for daily operations.
Participant observation: The system appeared intuitive to use, with the setup of bringing a computer, logging in, and consulting patients seamlessly integrated into the workflow - whether it was at the clinic of RDA or at the district hospital.
The NCD nurses at the district hospitals were well aware of the RDA visits and the use of the EMR system, and the collaboration and communication seemed to work well, despite the system not being used by the NCD nurses. However, the integration of the EDMRS into the district hospitals might add to its complexity and adaption to the daily district hospital workflows.
Data registration/capture
Users widely agreed that the EDMRS only required basic computer skills, was user-friendly, and served as a valuable tool in their daily tasks. HCPs expressed great confidence in data capture, facilitated by mandatory cells and clinical validations. However, they also indicated a need for more skills and training in data analysis and evaluation. Quote HCP A: The system guides you through the data collection step by step. It's very intuitive and easy to use… But I would also like to know more about how I can better use the data for improvements.
Despite this, most Users reported that the system was easy to use, it was observed that some clinical information was not consistently measured, and the system could potentially ease and streamline this process: Quote Expert B: I observed one person, who was 151 cm during the first visit, 145 cm the second visit, and now again 151 cm. When being measured, patients sometimes wear shoes, sometimes they don’t, therefore the height can vary, but not by 6 cm. Maybe the system can help identifying this error.
While the EDMRS already introduced mandatory cells and data validation features, this underscores the importance of ongoing evaluation and the need for continuous improvements.
Modification of the system
Users emphasized the need for continuous testing and modification of the system as issues emerge and potential areas for improvement are identified: Quote HCP C: When we keep using it [the EDRMS] we will find more things that can be improved, but for now this is not my concern because it works well. We can always add more information. Quote HCP D: We have regular meetings with the software developer, and we have planned for a phase two of the project where we will upgrade the system and do some minor changes.
Other Users already identified additional features to enhance the platform. It was suggested to include more lab tests, socio-economic parameters, and the functionalities for determining loss to follow-up could be further advanced. None of the suggestions were believed to be critical to the use of the system or a limitation to providing the necessary care.
Fidelity
The majority of system features functioned as expected and Users reported no issues navigating the platform, registering new patients, accessing historical medical records, entering and saving data, and interacting with data validation features. While system interruptions were not widely reported during the evaluation period, some concerns were raised about potential internet failure. In the absence of an internet connection, HCPs might be unable to access patient data or enter new data into the system, potentially disrupting workflows and causing delays in patient care. Quote HCP D: When the internet fails, sometimes we have to register the data more than one time… and other times it turns out that the data have been registered and uploaded anyway, which means there can be a double registration.
However, it was also reported by Experts that Rwanda generally has good connectivity and Users expressed that the EDMRS system can be used without any major problems related to internet failure.
Clients’ interaction with the platform features was more limited and was largely experienced through the automatic appointment reminders. While clients generally appreciated these SMS reminders, there was inconsistency in the delivery. Some clients received a single message, others received multiple reminders, and some did not receive any at all. This inconsistency suggests that the implementation of the SMS reminder feature could be improved for better reliability.
Sustainability
While sustainability was not part of the original DoI framework guiding the thematic analysis, it emerged as a crucial theme within Rwanda's resource-constrained health system. The EDMRS platform was developed with the Ministry of Health's approval—acknowledging it as a stand-alone, disease-specific platform that does not currently integrate with existing national health information architecture. Experts also mentioned that it might take years for a fully realized national EMR platform to launch. Quote Expert C: In the ideal world an overarching fully integrated system would be preferable, whereas in reality it is overly complicated.
However, the EDRMS could be vulnerable to replacement as the digital health transformation in Rwanda matures towards an integrated national EMR system encompassing all relevant disease areas. Experts suggested that EDMRS sustainability could be improved by ensuring its data interoperability with the national system currently under development. System- and data integration are extensively used within healthcare systems to allow software applications and services to function cohesively as a unified system. Additionally, the issue of continuous financial support was raised as a potential risk to the system's maintenance and ongoing sustainability. Although a definite maintenance plan was not yet established, several potential funding sources were proposed, such as ongoing core funding and project-based initiatives: Quote Expert A: The RDA clinic could allocate a monthly amount for EMR support. In addition, the project manager can work on individual fundraising projects. Also, since the database could eventually attract researchers, we could implement a Fee for Access, which would help to cover the maintenance costs.
Having an estimated overview of running costs and resources needed for continuous upgrade platform upgrades was highlighted as central elements for the long-term sustainability of the EDMRS.
Discussion
Summary of findings
The DoI framework guided our understanding of how the new EDMRS was adopted among users and helped us identify factors promoting its adoption and use. Our findings, analyzed through the lens of acceptability, advantage, and complexity, indicated that the system aligned well with existing work procedures and effectively met user needs. Users collectively preferred the EDMRS over paper forms and Excel sheets, citing its benefits in improving patient care and its effectiveness in monitoring and tracking patient data over time. While the system was generally found to be user-friendly, there was a highlighted need for additional training, particularly in data analysis and use. Concerns were also raised about the system's long-term sustainability, indicating areas for future focus and improvement.
Comparison with previous studies
In this study, the EDMRS was found widely acceptable among the Users. The Users reported that they liked using the system and it was easy to use (complexity). Similar results were found in a review assessing the implementation and usability of EMRs for infectious disease management in the SSA region. 14 The review included 19 studies and determined that “ease of learning” was the factor contributing most positively to the implementation. “Effectiveness,” including enhanced data quality and patient care, also seemed to positively influence usability, whereas “user satisfaction” was found important but contributed least to the adoption. In this study, user satisfaction (acceptability), including reliability in the system and perceived benefits, were found to be high and contributed positively to the adoption of the EDMRS. In general, there was a belief that the system saved time, improved care for patients, and contributed to improved workflows and less paperwork (relative advantage). This was aligned with a study from Nigeria, that also found usefulness and relative advantages to significantly increase clinician's intention to adopt an EMR system. 18 Other studies highlighted, that apart from improving the quality of care, the system should fit with existing workflows, 23 users need to see some personal benefits and have a sense of involvement and ownership of the system. 16 If users do not have clear incentives for using the EMR, they will be more likely to stick to usual work routines and the system less likely to be adopted. Therefore, successful implementation and adoption of the EMR system are closely tied to how well it is perceived by users, including ease of use (including technical skills), benefits over the previous system, resistance from users, and the level of support provided during the transition period.24,25
In this study, Users had a perception of being involved in the development process and the EDMRS was designed to match the needs of the Users. 21 Participation and engagement throughout the design and deployment phase of the system seemed to increase platform acceptance. In addition to the User's adoption of the EMR system, we found that the T1D individuals appreciated the improved access to data and greater involvement in their own care. This aligns with other studies, finding that patient engagement and involvement in personal care improve satisfaction (acceptability) and treatment outcomes (relative advantage)26,27. The findings further align with the DoI theory, which posits that acceptability, perceived benefits and user-friendliness increase the likelihood of successful adoption of a new intervention like an EMR system.
Data protection and legal factors, including privacy and security concerns, have been frequently reported as significant concerns related to the implementation and use of EMR systems. 16 In this study, data protection was less of a concern from the perspective of users and individuals with T1D, likely due to a long-standing trust in the RDA. However, some Experts highlighted data protection as a risk that needed to be considered. A study from Iran identified data security and confidentiality as the key elements when developing and using a web-based system for diabetes management, even in a clinical trial environment. 28 Another study, identified regulatory barriers and data rights as major obstacles in this domain and highlighted the importance of legal frameworks and data-sharing agreements to secure data security and privacy. 15
It has also been argued that changes in culture required to accompany a switch from the use of paper to an EMR system is an overlooked aspect that can lead to a slow adoption of the EMR system, 29 as technology alone is not sufficient to achieve a widespread use. 30 The EDRMS was quickly institutionalized, becoming a core component of the care process, leading to the retirement of the paper-based system. This swift institutionalization was likely attributed to a pre-existing demand for more efficient work processes at RDA. Furthermore, the active involvement of users in the design of the EDRMS likely facilitated a smooth transition, serving as an effective change management process. Rapid staff turnover, especially of champions in the early implementation, might affect the continued level of commitment to the EMR system. 31 However, in this context, this is considered unlikely given that RDA has a long history of high job tenure. Moreover, the system relies on external or internal support, and a shift in systemic or political priorities towards more integrated care could necessitate a transition from siloed systems, such as the EDMRS for T1D, to more comprehensive integrated solutions. 32
In this study, complexity did not emerge as a significant theme—possibly due to the implementation of the “stand-alone” platform with a focused clinical scope. However, as system integration was highlighted by experts in relation to sustainability, complexity could become a more significant theme in the future, contributing to the overall intricacy of the platform. These concerns were highlighted in another study, which pointed out technical challenges such as system integration and data interoperability, to ensure that systems speak the same language. 15 The major challenges include the lack of standardized data formats, differences in healthcare terminologies, as well as infrastructure disparities. Moreover, compliance with international standards adds another layer of complexity to integrating EMR systems. Adhering to multiple, independently developed standards like HL7, FHIR, and ICD can lead to inconsistencies in data formats and coding. Efforts towards harmonization are ongoing but face significant hurdles, requiring consensus among diverse stakeholders and substantial resources for implementation. This can be a challenge in countries, like Rwanda, with limited healthcare budgets and technological capabilities.15,33
Limitations and barriers
Designing and implementing a functioning digital intervention in a real-world setting is a challenging task, and it is unlikely that everything can be considered, delivered, and worked fully as intended.34,35 Especially in an LMIC context, such as Rwanda, where higher uncertainty, instability, and unpredictability could be expected due to limitations in digital infrastructure and resources. The DoI theory does not consider external contextual factors that might influence the implementation of a new intervention. The theory has been criticized for oversimplifying the diffusion process by focusing only on the characteristics of the innovation and the adapters, while overlooking the influence and interaction of social, economic, legal, political, and cultural factors.16,36,37
The complexity and reinvention dimension were included as an evaluation theme, but not deeply reflected in the analysis. This omission could be because the users were involved in the development process and the EMR system was continuously updated as issues emerged. However, it could be a limitation of the theory that not all adoption factors were equally accounted for in the analysis.
In this study, we evaluated the implementation after 9–10 months and explored the adoption of the system through the perspective of different relevant participant groups through data triangulation. However, it was clear that HCPs had more insights related to the EDRMS system than the T1D individuals and experts, having more limited acquaintance with the EDRMS. Recruitment was purposive rather than random, and it is possible that different or additional insights might have been identified by involving other stakeholder groups and participants from other regions. However, the purposive sample included various dimensions of diversity with some level of knowledge related to T1D or EMR systems. In qualitative research, achieving data saturation is prioritized over sample size calculation. By including a diverse range of participants, we observed that saturation was reached for HCPs and T1D individual interviews. However, new themes continued to emerge from the expert group, likely due to the diversity within this group, and the limited number of expert interviews was not sufficient to achieve data saturation in that group. Consequently, the sample size and recruitment strategy may affect the generalizability of the findings.
Conclusion
This study concludes a high level of adoption and successful implementation of the EDMRS for T1D management in Rwanda. The EDMRS was believed to have a relative advantage in tracking and follow-up of patients compared to old procedures. The T1D individuals appreciated receiving SMS reminders and trusted the system to collect and store their data securely. HCPs expressed satisfaction with the system, as it allowed for more efficient and accurate data entry, reduced errors, and saved time for more patient-related tasks. The system also enabled better communication with patients. The EDMRS was perceived as user-friendly, but some clinical guidelines and training materials related to data usage were still needed. Considering the dimensions of the DoI theory, it appears that T1D individuals, HCPS, and Experts successfully adopted to the use of the EDMRS system. However, concerns were raised about the fidelity of the SMS reminder functionality and the consistency of clinical information measurement. Experts highlight the importance of sustainability and maintenance of the EDMRS, including local ownership, continuous financial support and commitment from policy makers. The effect of the EDMRS on quality of care and clinical outcomes will be further investigated in a separate study.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241311057 - Supplemental material for A qualitative exploration of the early adoption of an electronic medical record system for type 1 diabetes management in Rwanda
Supplemental material, sj-docx-1-dhj-10.1177_20552076241311057 for A qualitative exploration of the early adoption of an electronic medical record system for type 1 diabetes management in Rwanda by Nathalie Bille, Dirk Lund Christensen, Stine Byberg, Crispin Gishoma, Sarah Fredsted Villadsen and Michael Calopietro in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241311057 - Supplemental material for A qualitative exploration of the early adoption of an electronic medical record system for type 1 diabetes management in Rwanda
Supplemental material, sj-docx-2-dhj-10.1177_20552076241311057 for A qualitative exploration of the early adoption of an electronic medical record system for type 1 diabetes management in Rwanda by Nathalie Bille, Dirk Lund Christensen, Stine Byberg, Crispin Gishoma, Sarah Fredsted Villadsen and Michael Calopietro in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to express their profound appreciation to the RDA staff, including Etienne Uwingabire, Paul Mbonyi, and Alvera Mukamazimpaka, for their invaluable contributions to this study and their support for T1D in Rwanda. Our immense gratitude extends to Angelo Igitego, Director of Karisimbi Technology Solutions, for his exceptional contribution and technical support in the development of the EMR system.
Contributorship
MHJC contributed to the theoretical framework and how to apply it to the empirical data. DLC contributed to the structure, academic writing as well as physiological and medical knowledge. SB contributed critically revising and commenting on the paper. CG contributed to the contextual aspects, knowledge about the study population, clinical procedures, and the project implementation. SVF contributed with the qualitatively methodological approach regarding the process evaluation and thematic analysis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This project was approved by the Institutional Review Board, College of Medicine and Health Sciences, University of Rwanda (FWA assurance No. 0001971, IRB 00001497 of IORG 0001100). The study purposes and the role of the primary investigator (NB) were thoroughly explained to participants before conducting the interviews. All participants provided their signed informed consent. Participation was completely voluntary, and all data were handled anonymously. Participants could opt out of the study at any point. No compensations were provided for participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the World Diabetes Foundation (WDF20–1740).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.