
Abstract
Introduction
Psychological and psychosocial impacts of major trauma, defined as any injury that has the potential to be life-threatening and/or life changing, are common, far-reaching and often enduring. There is evidence that these aspects of major trauma care are often underserved. The aim of this research was to gain insight into the current provision and operationalisation of psychological and psychosocial aspects of major trauma care across the UK and Ireland.
Methods
A cross-sectional online survey, open to health professionals working in major trauma network hospitals was undertaken. The survey had 69 questions across six sections: Participant Demographics, Psychological First Aid, Psychosocial Assessment and Care, Assessing and Responding to Distress, Clinical Psychology Services, and Major Trauma Keyworker (Coordinator) Role.
Results
There were 102 respondents from across the regions and from a range of professional groups. Survey findings indicate a lack of formalised systems to assess, respond and evaluate psychological and psychosocial aspects of major trauma care, most notably for patients with lower-level distress and psychosocial support needs, and for trauma populations that don't reach threshold for serious injury or complex health need. The findings highlight the role of major trauma keyworkers (coordinators) in psychosocial aspects of care and that although major trauma clinical psychology services are increasingly embedded, many lack the capacity to meet demand.
Conclusion
Neglecting psychological and psychosocial aspects of major trauma care may extend peritraumatic distress, result in preventable Years Lived with Disability and widen post-trauma health inequalities. A stepped psychological and psychosocial care pathway for major trauma patients and their families from the point of injury and continuing as they move through services towards recovery is needed. Research to fulfil knowledge gaps to develop and implement such a model for major trauma populations should be prioritised along with the development of corresponding service specifications for providers.
Introduction
Each year in the UK, injury from trauma causes an estimated 1.5 million Years Lived with Disability (YLDs) 1 and only a third of trauma survivors fully recover within a year of their injury. 2 Psychological and psychosocial impacts of major trauma, defined as any injury that has the potential to be life-threatening and/or life changing, are common, far-reaching and often enduring. Major trauma survivors report experiencing psychological3–5 and psychosocial distress 6 in prehospital and acute care periods. Post-traumatic distress in the peri-traumatic period is an important risk factor for the later development of post-traumatic stress disorder (PTSD).7–9 Approximately a third of survivors will develop depression, and more than a quarter, PTSD. 10 Psychosocial impacts are felt in social and family life,5,11,12 work13–15 and school life, 11 as well as economically. 16
Since 2010, major trauma care in the UK and Ireland has been increasingly operationalised through regional, hub and spoke major trauma care networks, with the most seriously injured cared for in specialised major trauma centres (MTCs).17–22 Although major trauma policy documents across the UK and Ireland17–22 incorporate psychological and psychosocial aspects of care, the level of detail across them varies. There is evidence that these aspects of major trauma care are often underserved in the UK. 23 Although major trauma networks may operate differently, the aim of this research was to gain insight into the current provision and operationalisation of psychological and psychosocial aspects of major trauma care for survivors and their families across the UK and Ireland.
Methods
A cross-sectional, online survey of psychological and psychosocial aspects of major trauma care was conducted to identify and describe current practices, including assessment, intervention and evaluation, and education and training. Survey design drew on policy documents and practice knowledge and was designed and tested by a multidisciplinary research team that included public and patient advisors. Ethical approval was granted from the University of Central Lancashire Ethics Review Panel (Reference ID: HEALTH 0144).
Hosted on Qualtrics® Survey Software (Provo, UT, USA), the survey (Online Supplementary Material 1) had 69 questions grouped into six sections: Participant Demographics, Psychological First Aid (PFA), Psychosocial Assessment and Care, Assessing and Responding to Distress, Clinical Psychology Services and Major Trauma Keyworker (Coordinator) Role. Psychological First Aid was defined as ‘psychosocial care to recognise mental health impacts, promote well-being, and help people in the immediate aftermath of an emergency event’. The survey was open from 25 February 2021 to 31 March 2021 and hospital-based professionals working in major trauma were invited to participate via opt-in invitation distributed by email and social media to major trauma research groups, professional networks, and stakeholder organisations. The invitation contained a link to an information sheet from which participants could access the survey after completing a digital consent form. Survey responses were monitored and recruitment was targeted to groups and regions with low or no response.
Analysis
Survey data were exported from Qualtrics® into Microsoft Excel (Version 2108, Microsoft Corporation, Redmond, WA, USA) and Statistical Package for the Social Sciences (SPSS, Version 27, IBM Corporation, Armonk, NY, USA) for analysis. Descriptive statistics were used to summarise the data. The survey had filter questions; therefore, the number of responses varies across questions. Percentages are reported according to the number of responses for each question and were rounded. Work areas with similar characteristics were grouped into five units of analysis:
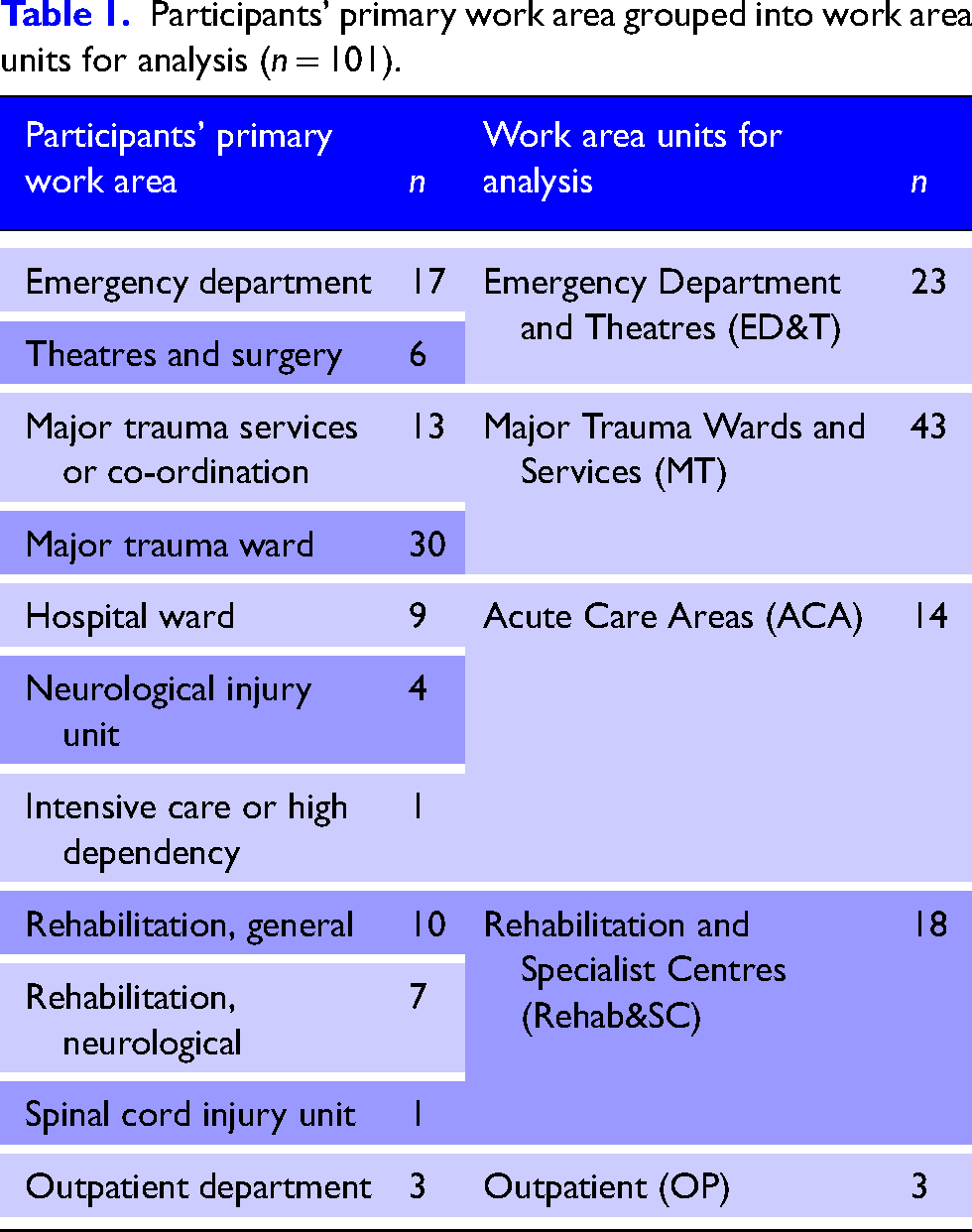
Emergency Department and Theatres (ED&T): clinical areas providing initial reception and / or stabilisation for short periods of time Major Trauma Wards and Services (MT): specialist major trauma clinical areas and services Acute Care Areas (ACA): clinical areas in which major trauma forms only part of the caseload (e.g. surgical, high dependency or intensive care units) Rehabilitation and Specialist Centres (Rehab&SC): specialist trauma care services likely to have longer term care relationships with patients and families Outpatient (OP): clinical areas providing follow-up care after discharge
Results
Respondent demographics are described first followed by a presentation of the results for PFA, Psychosocial Assessment and Care, Assessing and Responding to Distress, Clinical Psychology Services and Major Trauma Keyworker Role.
Survey respondents
There were 102 respondents, though one response was removed from the dataset because their responses were not about hospital-based major trauma care (n = 101). Responses covered England, Ireland, Northern Ireland, Scotland and Wales; however, response across them varied and some regions are over-represented (Online Supplementary Material 2). Most respondents worked in designated MTCs (n = 84), 46 in adult MTCs, 9 in children's MTCs and 29 in combined MTCs. Fourteen worked in hospitals designated as Trauma Unit (TU) and three worked in non-trauma designated Emergency Departments. Respondents were from a range of professional groups including doctors (n = 23), nursing (n = 20), physiotherapy (n = 17), major trauma practitioners (n = 15), clinical psychology (n = 13), occupational therapy (n = 7) and speech and language therapy (n = 2) (missing data n = 4). Three-quarters were from in-patient settings, and those working in Major Trauma Wards and Services formed the largest respondent group, followed by Emergency Department and Theatres, Rehabilitation and Specialist Centres, Acute Care Areas and Outpatients (Table 1).
Participants’ primary work area grouped into work area units for analysis (n = 101).
Psychological First Aid
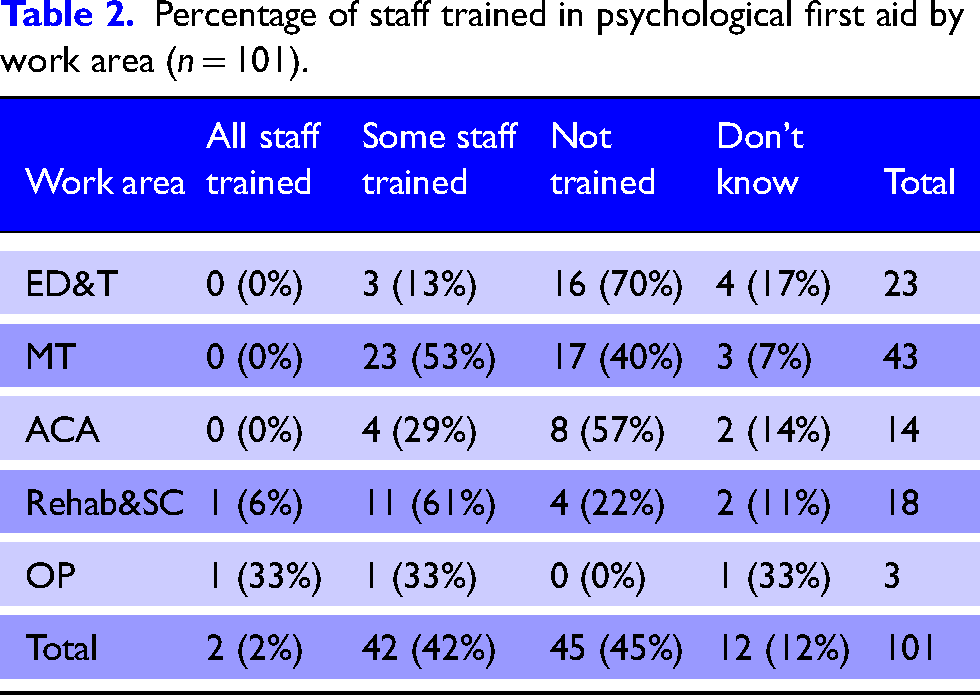
Less than half of respondents (n = 44/101, 44%) reported staff in their work area were trained in PFA (Table 2). Respondents working in rehabilitation and specialist centres and outpatients reported highest rates of PFA training (67%) followed by major trauma areas (53%), acute care areas (29%) and emergency department and theatres (13%).
Percentage of staff trained in psychological first aid by work area (n = 101).
Psychosocial assessment and care
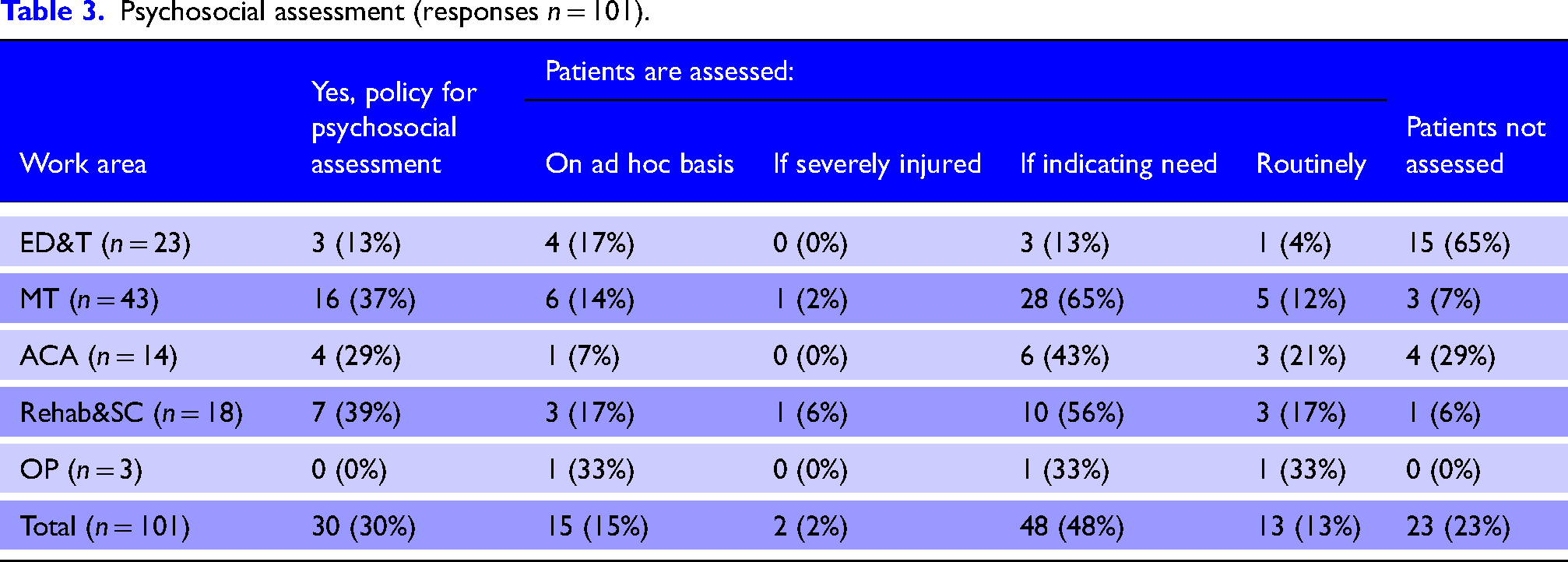
Less than a third of respondents reported there was a policy in their unit for assessing major trauma patients’ psychosocial needs (Table 3). However, most reported some degree of psychosocial assessment (77%), whether this was for all patients (13%) or only some (64%).
Psychosocial assessment (responses n = 101).
Timing of psychosocial assessment varied from being done within 24 h (n = 9/76, 12%) to within 72 h of admission (n = 29/76, 38%) or on an ad hoc basis (n = 38/76, 50%). Participants (n = 78) reported psychosocial assessment was most frequently undertaken by clinical psychologists (n = 48, 62%), followed by nurses (n = 33, 42%), occupational therapists (n = 28, 36%), physiotherapists (n = 27, 35%) and psychological well-being practitioners (n = 4, 5%). Few reported staff had training in psychosocial assessment (n = 14/78, 18%). Participants were asked to select the types of psychosocial care interventions available where they worked (Table 4).
Psychosocial interventions available* in frequency order.
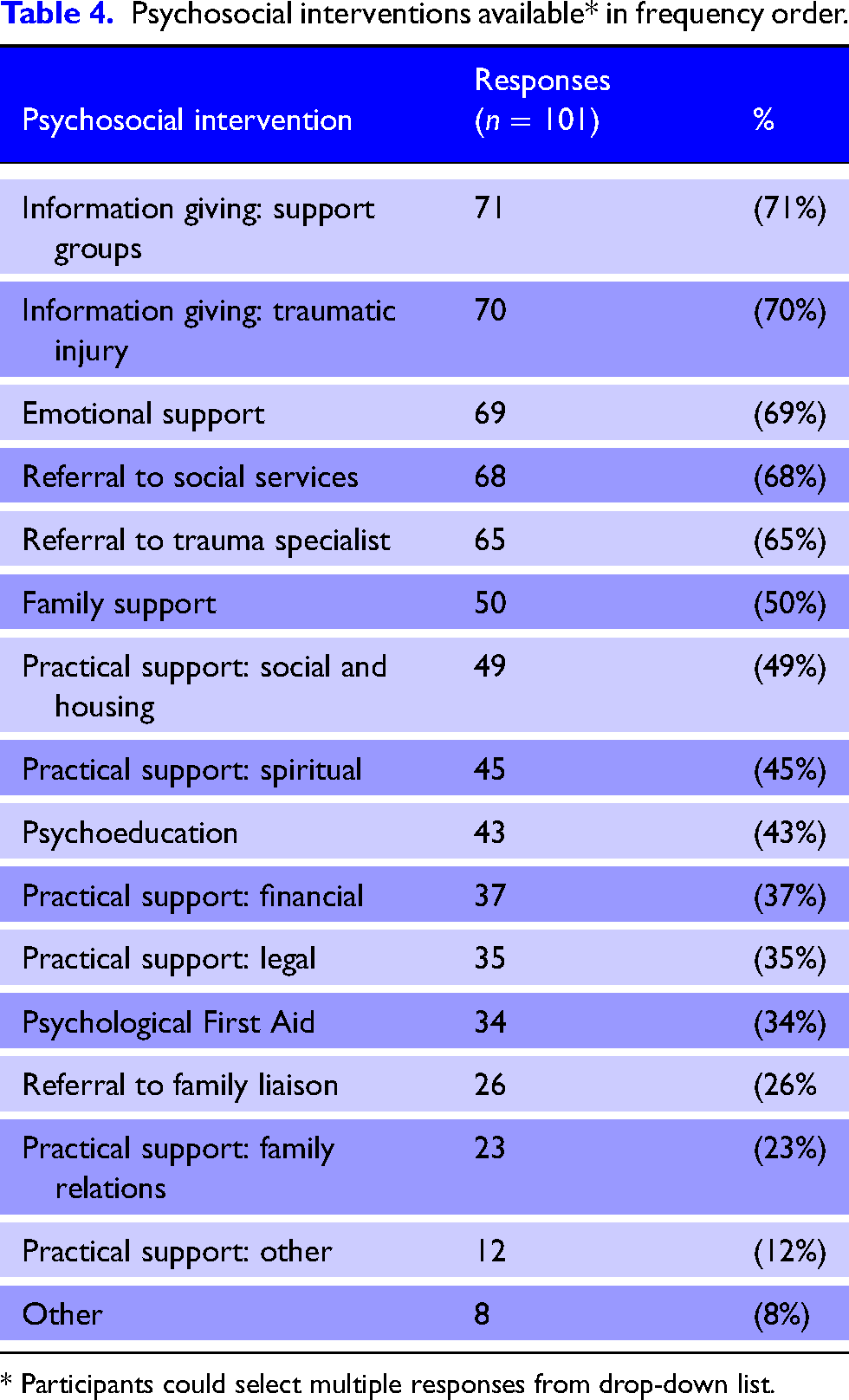
* Participants could select multiple responses from drop-down list.
The most frequently reported interventions were information given about support groups and about the injury, provision of emotional support, referrals to social services and trauma specialists, and family support. Lower frequency interventions were financial and legal support and PFA. Free-text ‘other’ responses included psychological therapy and vocational rehabilitation.
Assessing and responding to distress
Similarly, few reported having a policy for assessing major trauma patients’ distress (n = 21/101, 21%) (Table 5), though many respondents (61%) reported distress was assessed in practice, most commonly on an as-needed basis. Routine distress assessment for major trauma patients was reported by 15% (n = 9/61) of respondents, and assessment was reported as most frequently undertaken by clinical psychology (n = 42/61), and followed by, trauma specialist staff from nursing (n = 26/61), physiotherapy (n = 24/61), medical and occupational therapy (n = 21/64).
Distress assessment by work area.
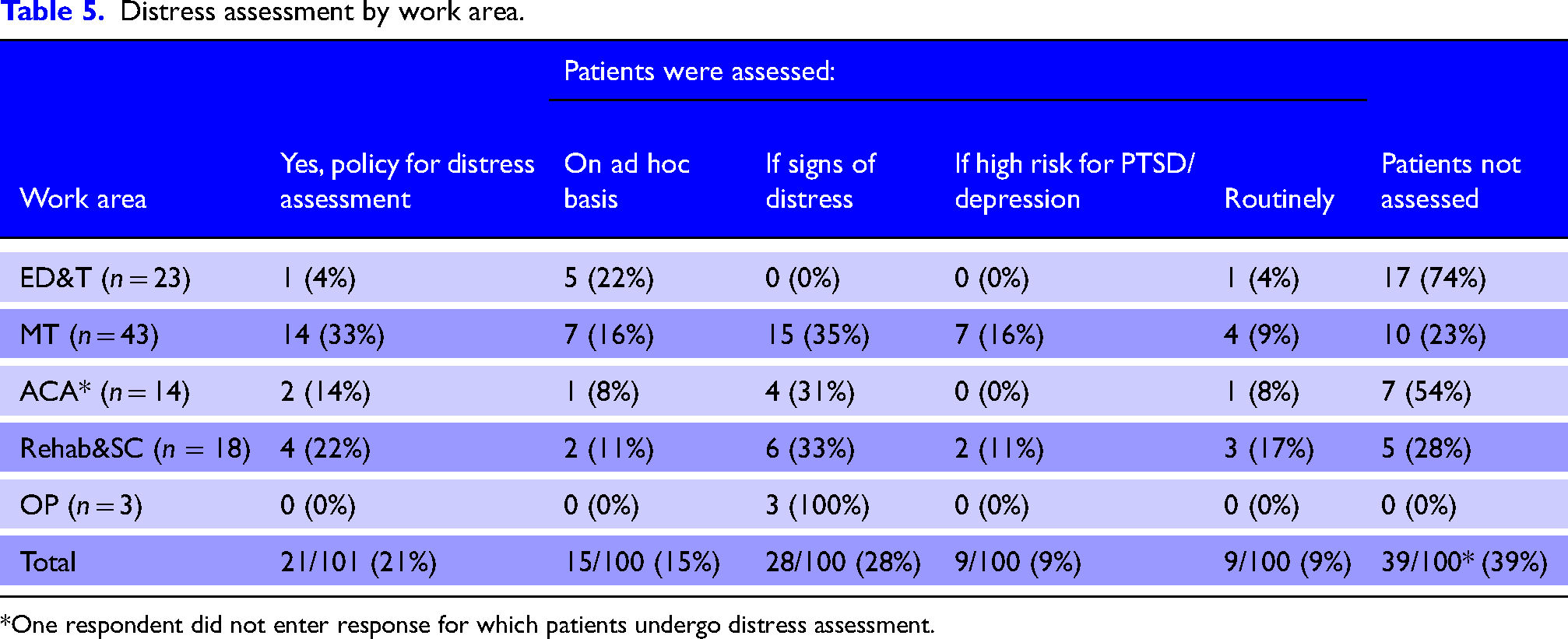
*One respondent did not enter response for which patients undergo distress assessment.
Participants were asked to select interventions available for responding to distress from a multi-option list. Higher frequency interventions included a referral to mental health (n = 40/61) and clinical psychology services (n = 38/61), emotional support (n = 39/61), information giving about the injury (n = 39/61) and support groups (n = 37/61). Lower frequency interventions were PFA (n = 30/61), practical support including social and housing (n = 29/61), financial (n = 27/61), spiritual (n = 22/61), legal (n = 19/61) and family support (n = 28/61). Nearly one-third reported there was a clinical pathway that followed distress assessment (n = 19/61, 31%), one-third didn't know (n = 20/61, 33%) and just over a third reported there wasn't a pathway (n = 22/61 36%).
Psychological and psychosocial assessment tools
Participants were asked about psychological and psychosocial assessment tools used in their work area on three occasions in the survey: the psychosocial section, the distress assessment section and the major trauma clinical psychology services section. Respondents could select from a multi-option list as well as entering names of tools used. Table 6 is an amalgamation of these results, produced to identify the type and range of tools used across different regions. Responses indicate a variety of tools in use both within and across regions with the IES-r, PAS, Distress Thermometer, PHQ9 and GAD7 most widespread. Single entry ‘Other’ measures were appearance-related concerns scale; health locus of control scale; communication tool; observations; clinical judgement; and child appropriate. Some regions had more respondents than others, and this may explain differences in the range of tools reported.
Tools in use by region.
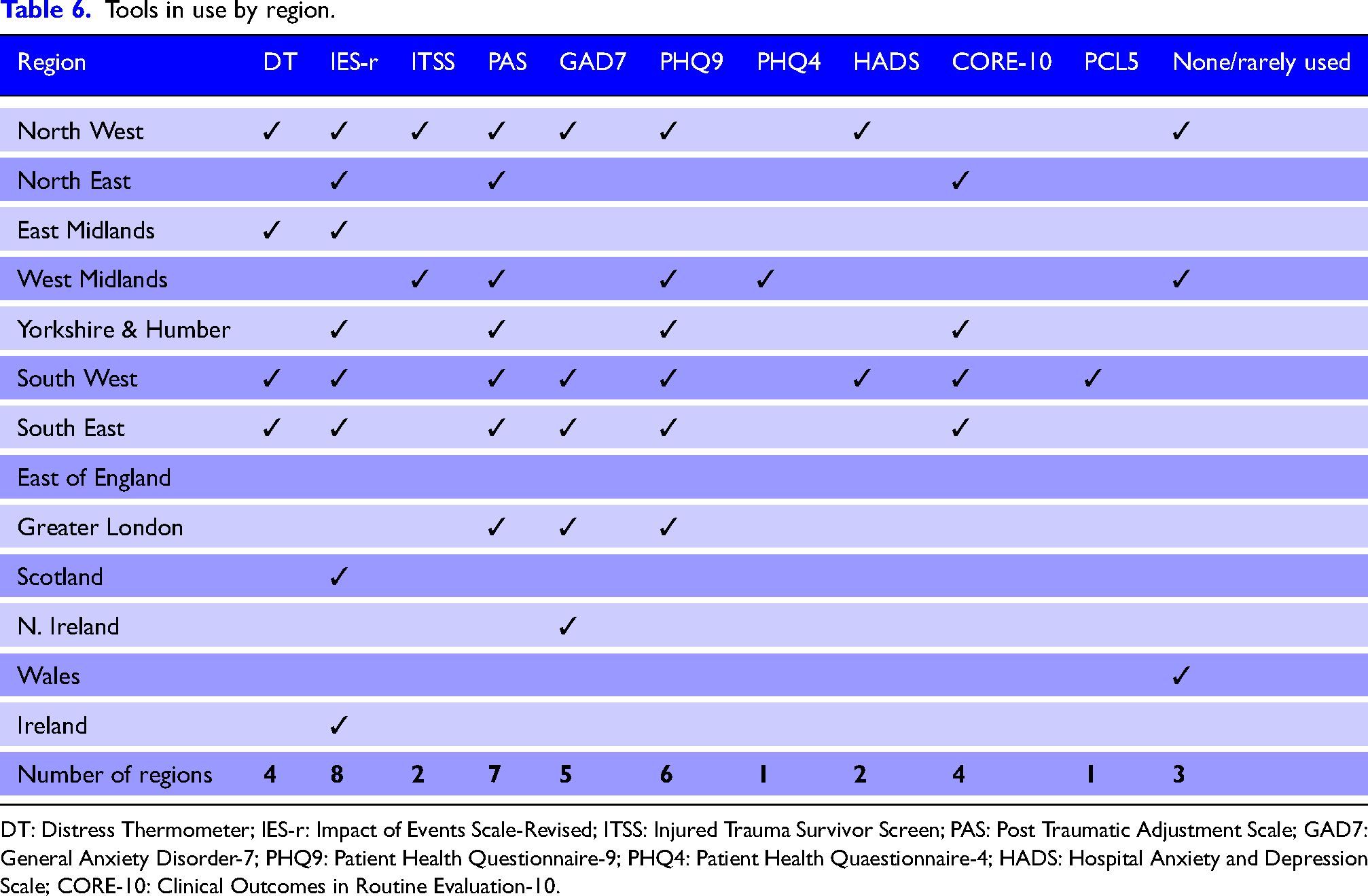
DT: Distress Thermometer; IES-r: Impact of Events Scale-Revised; ITSS: Injured Trauma Survivor Screen; PAS: Post Traumatic Adjustment Scale; GAD7: General Anxiety Disorder-7; PHQ9: Patient Health Questionnaire-9; PHQ4: Patient Health Quaestionnaire-4; HADS: Hospital Anxiety and Depression Scale; CORE-10: Clinical Outcomes in Routine Evaluation-10.
Major trauma clinical psychology services: Accessibility
Approximately 60% of participants (n = 60/101) reported there was a Major Trauma Clinical Psychology Service in the hospital where they worked, 35% reported there wasn't (n = 35/101) and 7% (n = 7/101) didn't know. Of those reporting a Major Trauma Clinical Psychology Service (n = 60), most reported the service was open to all major trauma patients (n = 45, 75%), there was access to both clinical psychology and neuropsychology (n = 46, 77%), and information about the service was available to patients and families (n = 39, 65%). Most had a referral process for the service (n = 53/60, 88%), and nurses (n = 49/60, 82%), physiotherapists (n = 46/60, 77%), occupational therapists (n = 45/60, 75%) and medical staff (n = 48/60, 80%) could refer to it. Pre-referral psychological screening was most often not required (n = 47/60, 78%) and more than half reported no eligibility threshold (n = 33/60, 55%, though many didn't know (n = 23/60, 38%). Those reporting eligibility thresholds (n = 4/60, 7%) identified these as: admission to the major trauma ward (n = 1); injury pattern and complexity (n = 1); distress related to the major trauma (n = 1); and not being able to accept patients who were suicidal (n = 1).
Respondents also indicated there may be groups of patients that may not know about or be able to access clinical psychology services (n = 12/60, 20%), the reasons for which were: patients admitted to non-major trauma areas (n = 3) or discharged directly from the emergency department (n = 1), and the service only funded for traumatic brain injury or spinal cord injury (n = 3). Over half of respondents (n = 33/60, 55%) felt a major trauma clinical psychology service lacked resources to meet demand, and this was explained in terms of understaffing (n = 19), underfunding (n = 4), lack of major trauma neuropsychologist (n = 1) and no clinical psychologist in the post (n = 2).
Major trauma clinical psychology services: Scope of role
Participants were asked about the role and responsibilities of the Major Trauma Clinical Psychology Service (Online Supplementary Material 3). Higher frequency responses (>60%) were that clinical psychologists were part of major trauma patients’ multidisciplinary team, undertook psychological assessments, provided psychological therapies, contributed to rehabilitation prescriptions, provided out-patient follow-up and provided psychological support for families, and were a source of clinical advice for staff. Fewer (≤50%) reported the service provided staff training in psychosocial and psychological aspects of care, though more than a third didn't know.
Named major trauma keyworker (coordinator) role
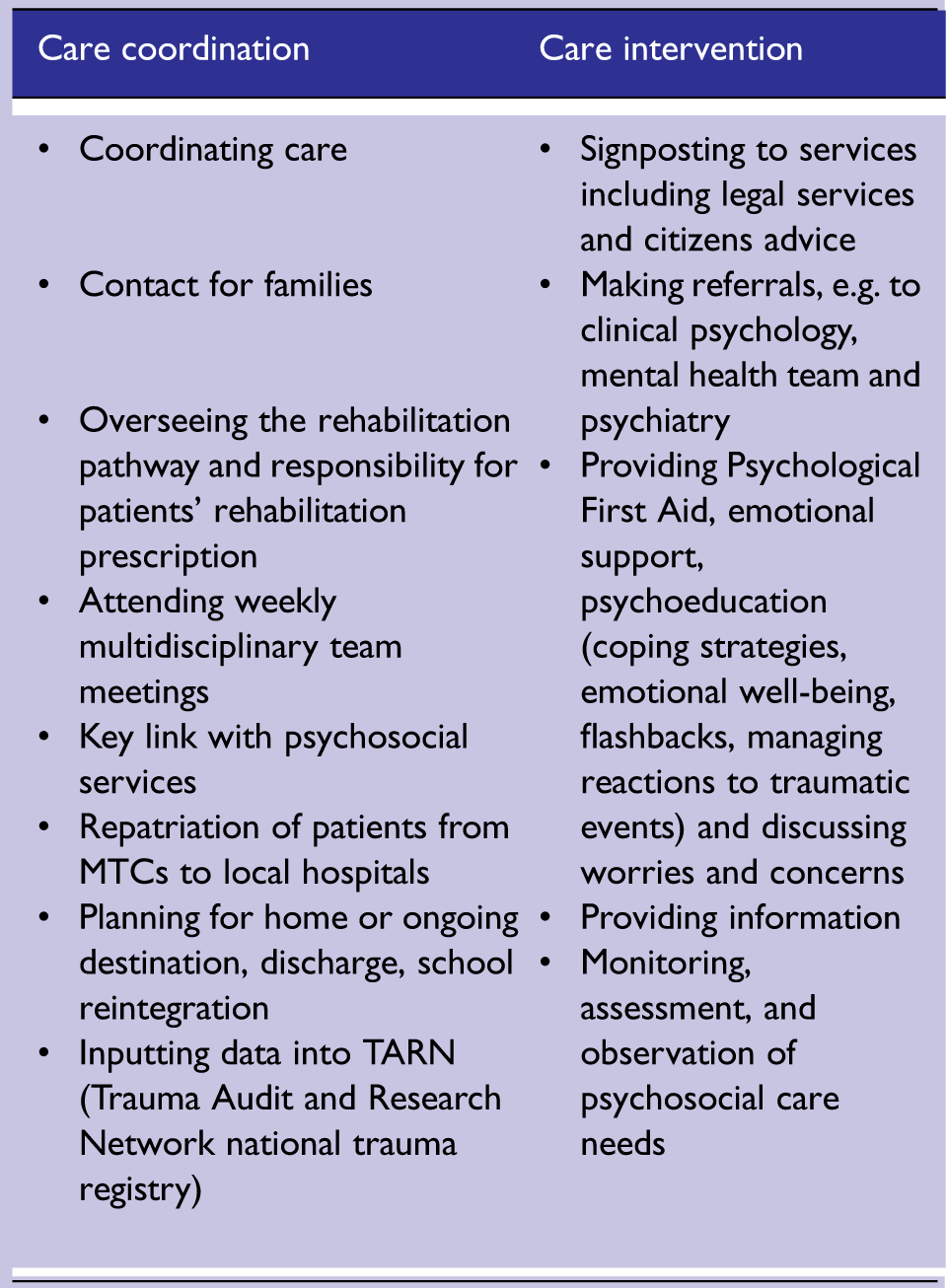
Two-thirds of respondents reported major trauma patients had a named major trauma keyworker (n = 65/95, 68%). Participants were asked to enter examples of the role in relation to patients’ psychosocial care into a free text box. Responses from 56 respondents were collated into Care Coordination activities and Care Intervention activities (Box 1).
Psychosocial aspects of major trauma keyworker (coordinator) roles.
Just over half of respondents stated major trauma keyworkers (coordinators) followed up with patients after the patient was discharged (n = 36/64, 56%), though nearly a quarter didn't know (n = 14/64, 22%). Timings of major trauma key worker follow-up were reported as occurring initially at two (n = 16) or four weeks (n = 3) post-discharge, and second follow-up varying from 6 weeks, 3 months, to 6 months, or on an as-needed basis. One respondent reported follow-up may continue for two years and another reported possible continuation for up to three years.
Discussion
In this section, results are contextualised with reference to policy documents, practice guidelines and previous research. A discussion of models of psychological and psychosocial care follows, bringing together survey findings, highlighting gaps in provision and concluding with priorities for future development.
Psychological First Aid
Psychological first aid has gained traction as a term describing psychosocial care in the immediate and early periods following a traumatic event. 24 PFA bridges the intervention gap between a traumatic event and specialised psychosocial and psychological assessment and intervention. 17 The principles of PFA aim to promote feelings of safety, calm, self-efficacy, connectedness and hope. 25 Trauma survivors have reported feeling safe and cared for when staff were empathetic, kept them informed and gave reassurance,3,6 thus illustrating the relevance of PFA for major trauma populations. Although PFA was advocated in the Major Trauma Clinical Advisory Group Report, 17 the findings of this survey indicate it has not been widely embedded. There are numerous models of PFA, having been adapted for different settings, although evidence of the effectiveness of PFA in reducing distress and enabling adaptive strategies after traumatic events is limited. 24
Distress and psychosocial assessments and response pathways
The survey results illustrate processes for distress and psychosocial assessment and response were not formalised in practice and largely undertaken ‘as needed’. Ad hoc approaches may introduce cognitive bias that neglects less obvious risk factors for distress such as being treated outside one's area 26 and pre-incident risk factors. 27 The survey also found that distress and psychosocial assessments were undertaken by many professional groups, though which group had overall responsibility is not clear. Low levels of training in PFA and psychosocial assessment introduce uncertainty about the quality of assessments, emotional support given, and information provided. The findings identify gaps in current provision, which may lead to detrimental variation in practice, 28 as early predictors and intervention for the causes of distress could be missed.
Major trauma clinical psychology services
The findings indicate major trauma clinical psychology services are growing and that where they do exist formalised systems (e.g. referral processes) are embedded. Major trauma service specifications for patients with serious injury (Injury Severity Score >8) in England 18 and Wales 22 list clinical psychology services as a MTC co-located specialty. Importantly, 22% of respondents who did not know (n = 4) or answered no (n = 18) about having a major trauma clinical psychology service worked in TUs (n = 14) or non-trauma designated emergency departments (n = 3), and/or regions (n = 6) not covered by these service specifications. Still, even in areas covered by the service specification, provision is not yet universal. Respondents also reported insufficient capacity to meet demand, limited population eligibility and long waiting lists for post-discharge services. The scope of clinical psychology services likely reflects capacity with patient and family facing services and clinical advice for staff widely reported but education and training activities less so.
Psychological screening tools
Several validated tools for identifying the risk of development of PTSD and depression,29,30 posttraumatic stress, 31 generalised anxiety disorder 32 and depression33,34 and that would form part of clinical psychology assessments were in use. The Posttraumatic Adjustment Screen has demonstrated reasonable accuracy in a UK population for early identification of patients at risk of later posttraumatic stress and depression following major trauma. 26 The Distress Thermometer, a single-item tool favourably validated to assess distress and psychosocial needs of cancer patients, 35 was in use in some regions. The appeal of the distress thermometer is its rapidity and ease of administration by trained, but non-specialist staff. Although likely transferable to non-cancer populations, the distress thermometer has not been validated for major trauma populations. Overall, the findings indicate there may be variation in the tools being used. A consensus and common language around assessment and screening tools so it is clear which tools are most useful, for which patients, for what purpose, and what they may lead to would help underpin a joined up psychological and psychosocial care pathway for trauma patients as they move through services.
Named major trauma keyworker (coordinator) role
The widespread introduction of the major trauma keyworker (coordinator) role identified in this survey is likely a consequence of their inclusion in service specifications across all countries.18–22 In England, this role is described as ‘a named member of clinical staff (a key worker, often a senior nurse) assigned at each stage of the care pathway who coordinates the patient's care’. 36 A previous study of trauma nurse coordinator activity in 2013 37 revealed the role involved clinical work, trauma registry data collection, quality improvement, administrative tasks, and education, research and outreach work. This survey has unpacked clinical aspects of the role in relation to psychological and psychosocial major trauma care and echoing international research 38 found they are often central in major trauma survivor (and family member) care experiences and outcomes.
Models of psychological and psychosocial care
A personalised Rehabilitation Prescription (or Rehabilitation Plan) for patients with serious injury is a key performance indicator for major trauma service providers across UK and Ireland.18–22 Rehabilitation Prescriptions follow a biopsychosocial model in which information about psychological (mental capacity, emotional state) and psychosocial (activities of daily living, housing, social support, vocational activities) situations can be recorded. 39 They incorporate higher level specialist psychological and psychosocial care (e.g. formal family support, psychology and psychiatry). Recognising that the rehabilitation pathway for people with less severe injury was less well defined, the recent ‘Rehabilitation after Traumatic Injury’ guideline, 40 published after this survey was undertaken, targets a broader population of people admitted to hospital after the trauma but who nonetheless have complex rehabilitation needs (defined as involving coordinated multidisciplinary input from at least two allied health professional disciplines). This new guidance calls attention to acute stress responses, psychological and emotional support as well as psychological and psychosocial risk factors; however, there is little detail for operationalising these in practice. The survey findings reflect current policy and practice guidance, in that higher level care provision, such as those embedded in the Rehabilitation Prescription or specialist clinical psychology services are more likely to be formalised in practice, whereas systems to guide lower level psychological and psychosocial care were less so.
The 2010 NHS Clinical Advisory Group Report for Regional Networks for Major Trauma 17 proposed a stepped model of psychosocial and mental health care commencing at the point of injury. In this model, responding to distress through social support, PFA, and welfare (financial, legal, social) aid were universal components delivered by staff in pre-hospital and immediate care periods, and progressing as needed to specialist care. It is not clear why this model was not incorporated into subsequent major trauma policy documents and guidance. However, there is increasing evidence of the effectiveness of stepped psychological and psychosocial approaches in major trauma care in terms of improving longer term outcomes, 41 reducing posttraumatic psychological distress symptoms and identifying those at risk of developing PTSD, anxiety and/or depression.41,42 Recent NHS guidance 27 describes a graduated psychological and psychosocial response and intervention pathway for people affected by incidents and emergencies. This guidance, focussed on major incident and community health threat events, provides operational considerations about planning, resources and training for service planners and commissioners, although operational detail for assessment and response within the pathway is less well defined.
Limitations
The survey was conducted during a period of Covid-19 lockdown and immense health service pressures which likely affected the response rate. Responses in some demographic variables were low and responses may not be representative. Some regions were over-represented in the overall survey response, and it is possible that some hospitals may also be over-represented within regions. An alternative would have been to ask one person from each major trauma network hospital to complete the survey. However, we decided against this approach because major trauma care is a pathway rather than a discrete discipline, not all MTCs have designated major trauma wards major trauma patients may be admitted to other speciality units (e.g. plastic and reconstructive surgery, neurosurgery etc.), and some may have a general ward placement for all or part of their admission. We aimed to reach respondents from across this spectrum and which may have been missed if one person from an organisation had been asked to complete. It is also not possible to report a response rate because the number of people that could have responded is indeterminate. Survey responses regarding capacity shortages may also have been affected by the ongoing Covid-19 pandemic, which alongside the enormous personal and professional strain staff were experiencing 43 also led to increased demands on clinical psychology services. 44
A strength of the survey was that responses were received from all regions and from a range of professionals. However, this is also problematic because of differences across major trauma networks and service specifications. However, in recognition of the advancing specialisation of major trauma care and the operational interconnectedness across the five countries, the goal of this survey was to generate exploratory insights about psychological and psychosocial aspects of major trauma care across the UK and Ireland.
Conclusion
This survey of practice has generated a first insight into psychological and psychosocial aspects of major trauma care in the UK and Ireland. Survey findings indicate a lack of formalised systems to assess, respond and evaluate psychological and psychosocial aspects of major trauma care, most notably for patients with lower-level distress and psychosocial support needs, and for trauma populations that don't reach the threshold for serious injury or complex health need. The findings highlight the role of major trauma keyworkers (coordinators) in psychosocial aspects of care and that although major trauma clinical psychology services are increasingly embedded, many lack the capacity to meet demand. The strengths and limitations of current practice reflect existing service specifications, drawing attention to their importance as levers of change and quality improvement.
Neglecting psychological and psychosocial aspects of major trauma care may extend peritraumatic distress, result in preventable YLDs and widen post-trauma health inequalities. A stepped psychological and psychosocial care pathway for major trauma patients and their families from the point of injury and continuing as they move through services towards recovery is needed. Building on psychological and psychosocial care pathways from parallel fields, research to fulfil knowledge gaps to develop and implement such a model for major trauma populations across the UK and Ireland should be prioritised along with the development of corresponding service specifications for providers. This would pave the way for more efficient service planning, improve outcomes and reduce health inequalities after trauma.
Supplemental Material
sj-docx-1-tra-10.1177_14604086221145529 - Supplemental material for Psychological and psychosocial aspects of major trauma care: A survey of current practice across UK and Ireland
Supplemental material, sj-docx-1-tra-10.1177_14604086221145529 for Psychological and psychosocial aspects of major trauma care: A survey of current practice across UK and Ireland by P Olive, L Hives, A Ashton, MC O’Brien, A Taylor, G Mercer, C Horsfield, R Carey, R Jassat, J Spencer and N Wilson in Trauma
Supplemental Material
sj-docx-2-tra-10.1177_14604086221145529 - Supplemental material for Psychological and psychosocial aspects of major trauma care: A survey of current practice across UK and Ireland
Supplemental material, sj-docx-2-tra-10.1177_14604086221145529 for Psychological and psychosocial aspects of major trauma care: A survey of current practice across UK and Ireland by P Olive, L Hives, A Ashton, MC O’Brien, A Taylor, G Mercer, C Horsfield, R Carey, R Jassat, J Spencer and N Wilson in Trauma
Supplemental Material
sj-docx-3-tra-10.1177_14604086221145529 - Supplemental material for Psychological and psychosocial aspects of major trauma care: A survey of current practice across UK and Ireland
Supplemental material, sj-docx-3-tra-10.1177_14604086221145529 for Psychological and psychosocial aspects of major trauma care: A survey of current practice across UK and Ireland by P Olive, L Hives, A Ashton, MC O’Brien, A Taylor, G Mercer, C Horsfield, R Carey, R Jassat, J Spencer and N Wilson in Trauma
Footnotes
Declarations
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the UCLan Institute for Global Health and Wellbeing (LIFE) Research Grant.
Ethical Approval
The research received ethical approval from the University of Central Lancashire Health Ethics Review Panel (HEALTH 0144).
Informed Consent
The invitation to potential participants contained a link to a participant information form from which participants could access the survey after completing a digital consent form.
Trial Registration
Not applicable.
Contributorship
PO, LH, AA, MCOB, GM, AT and CH contributed to conception of the study. All authors contributed to design of the research. LH, RJ and PO contributed to the acquisition of data. PO, LH, JS and RC contributed to analysis of data. PO, LH, AA, MCOB, AT, CH, GM and NW contributed to interpretation and contextualisation of data. All authors contributed to drafting the paper, have approved the final version and agree to be accountable for the work.
Acknowledgements
The authors would like to thank the wider professional and public members of the RePEAT (Research and innovation to address Psychological, Emotional, and psychosocial well-being After major Trauma) project group who advised on the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.