
Abstract
Introduction
More people are surviving major trauma, often with life changing injuries. Alongside physical injury, many survivors of major trauma experience psychological and psychosocial impacts. Presently, there is little guidance at the UK national level for psychological and psychosocial aspects of major trauma care. Set in the context of the regional model of major trauma care implemented in the UK in 2012, the purpose of this review was to identify and bring together primary research about psychological and psychosocial aspects of major trauma care in the UK to produce an overview of the field to date, identify knowledge gaps and set research priorities.
Methods
A scoping review was undertaken. Seven electronic databases (MEDLINE, Cochrane Library, CINAHL, Embase, PsycINFO, SocINDEX with Full Text and PROSPERO) were searched alongside a targeted grey literature search. Data from included studies were extracted using a predefined extraction form and underwent bibliometric analysis. Included studies were then grouped by type of research, summarised, and synthesised to produce a descriptive summary and overview of the field.
Results
The searches identified 5,975 articles. Following screening, 43 primary research studies were included in the scoping review. The scoping review, along with previous research, illustrates that psychological and psychosocial impacts are to be expected following major trauma. However, it also found that these aspects of care are commonly underserved and that there are inherent inequities across major trauma care pathways in the UK.
Conclusion
Though the scoping review identified a growing body of research investigating psychological and psychosocial aspects of major trauma care pathways in the UK, significant gaps in the evidence base remain. Research is needed to establish clinically effective psychological and psychosocial assessment tools, corresponding interventions, and patient-centred outcome measures so that survivors of major trauma (and family members or carers) receive the most appropriate care and intervention.
Introduction
The term ‘major trauma’ is used to describe a serious injury, or combination of injuries, that has the potential to be life-threatening and/or life-changing. 1 The UK operates a regional model of major trauma care designed to deliver best care in the most optimal time frame and which is made up of i) Major Trauma Centres providing specialist trauma services for the most seriously injured (analogous to US Level 1 trauma centers), ii) Trauma Units providing specialist care for patients who do not have multiple injuries and iii) Local emergency departments that do not provide trauma services but have systems in place to transfer patients for specialist care if needed. 2 This model of care was implemented in response to recommendations from the National Confidential Enquiry into Trauma Patient Outcome and Death which found that major trauma care and outcomes in the UK were much worse than similar, high income, countries. 3 Following its London pilot in 2010, and subsequent roll out across the UK in 2012, this model of care has proved successful. In the first 5 years following implementation the odds of survival after major trauma increased by 19%. 4
Increased survivorship also means that more people are living with serious injury and disability. In 1 year alone, injuries accounted for 57 million years lived with disability worldwide 5 and 1.5 million in the UK. 6 Alongside physical injury, psychological impact is common. Survivors of major trauma report experiencing acute stress reactions in the prehospital, 7 emergency 8 and hospital 9 care periods and a significant number will develop acute stress disorder, 10 post-traumatic stress disorder (PTSD) 11 and/or depression 12 and which can impact recovery. 13 Post-traumatic stress in peri and post-traumatic periods are important risk factors for the development of PTSD.14,15 Psychosocial impacts of major trauma are also far-reaching, affecting people’s sense of self, their social relationships and family life, 16 their occupation and work life,17,18 and their economic wellbeing. 19 Family members are impacted too, they may have witnessed the trauma itself, been a first responder, and/or have significant and enduring life-changes as they support their family member’s care and recovery. 20 Clearly, early intervention for identifying and addressing psychological and psychosocial impacts of major trauma is an important aspect of care.
Indeed, the National Health Service (NHS) standard contract for major trauma service providers in England requires that clinical psychology and rehabilitation services be co-located in major trauma centres. 21 The requirements for rehabilitation services are expressly stated, in terms that all major trauma patients with an Injury Severity Score of >8, should receive a rehabilitation assessment by a rehabilitation medicine consultant within 3 days and an initial rehabilitation prescription by day 4. 21 Conversely however, there is little detail about the form that major trauma clinical psychology services should take, 21 there is only a requirement for 24/7 psychiatry on call and a recommendation that staff on major trauma wards be provided with training to recognise mental health impacts of major trauma. Less detail for clinical psychology services may have reflected limitations in the evidence-base when the national major trauma guideline 22 was developed. Set in the context of the establishment of a national system for major trauma care in 2012 and the corresponding requirements for rehabilitation and clinical psychology major trauma service provision, the purpose of this study was to undertake a scoping review 23 to identify and bring together any primary research about psychological or psychosocial aspects of major trauma care in the UK since the introduction of the UK’s first major trauma care pathway.
Methods
A scoping review following JBI Methodology for Scoping Reviews24,25 and the Extended Arksey and O’Malley Framework 26 was undertaken and is reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist 27 and PRISMA 2020 Statement. 28 The objectives of the scoping review were to identify, chart and summarise primary research about psychological or psychosocial aspects of major trauma care in the UK and produce an overview of the field to date, identify knowledge gaps and set research priorities.
Search Strategy
We conducted a search of 7 major electronic databases (MEDLINE (Ovid), Cochrane Database of Systematic Reviews and Cochrane Central Register of Controlled Trials (Cochrane Library), CINAHL (EBSCO), Embase (Ovid), PsycINFO (EBSCO), SocINDEX with Full Text (EBSCO) and PROSPERO), for peer-reviewed research publications from January 2010 (the year that major trauma centres were first piloted in the UK), to 20th November 2020, and this was updated on 14th September 2021. The search strategy included keywords and Subject Headings for “major trauma” and UK-specific search filters29,30 were used to limit the retrieved studies to those conducted in the United Kingdom. Searches were adapted for use in each database and the full search strategy for each database and search time-point is reported in online Supplementary 1. A targeted grey literature search was undertaken between 28th January 2021 to 22nd March 2021 and involved searches of the OpenGrey database, UK-based trauma care research centres, Non-Government Organisations, Government Departments and related organisations, Professional Organisations, Health Think Tanks, and key researcher webpages. The full list of grey literature sources is reported in online Supplementary 2.
Eligibility Criteria
Primary research about psychological or psychosocial aspects of major trauma care, set in Major Trauma Centres or clearly connected to the post-2012 Major Trauma Care Pathway in the United Kingdom was included. ‘Care’ was broadly defined to include research about assessment, interventions, outcome measures, service delivery, and experiences of trauma and trauma care. Relevant conference abstracts were excluded following a search to find any associated published articles or reports. Studies focused on physical measures of function or recovery following medical or surgical interventions, e.g. degrees of movement in a limb or moderate recovery on the short, 5-point Glasgow Outcome Scale, were excluded if they did not also include psychological or psychosocial aspects of care. Similarly, epidemiological studies solely reporting psychological or psychosocial outcomes after major trauma were also excluded. The full inclusion and exclusion eligibility criteria are reported in online Supplementary 3.
Study selection
A database of all identified studies was created and managed in EndNote v.X9 (Clarivate Analytics, PA, USA). Duplicate references were deleted, firstly using the EndNote ‘‘find duplicates’’ function and then manually. Using the inclusion/exclusion criteria, the titles and abstracts of all papers were screened independently by two reviewers (PO, LH, RJ) and adjudicated by a third reviewer if needed. The full texts of articles deemed relevant at this stage were also screened independently by two reviewers (PO, LH, RJ) with the third reviewer available as needed to reach consensus for the final set of included papers.
Data extraction and charting
Information from each included study was extracted using a predefined data extraction form on Microsoft Excel (online Supplementary 4). Data extraction for each paper was carried out by one reviewer (LH) and checked by a second reviewer (NW or PO). The information extracted and charted included first author, year of publication, country, study aim, psychological/psychosocial focus, focus of research, type of research, methods, participant population, number of participants, year of data collection and key findings. In line with scoping review methodology to produce an overview of a field rather than a synthesis, 25 methodological quality appraisal was not undertaken.
Collating, summarising and reporting the results
Bibliometric data were analysed to produce a trend of publications over time and journal publication frequencies. To collate and summarise the included research, studies were grouped according to the focus of the research as follows: • Major Trauma Care Pathways • Major Trauma Care and Experiences • Major Trauma Care Innovations • Major Trauma Assessment Tools and Outcome Measures • Major Trauma Research Prioritisation Studies
A descriptive analytical method 26 was undertaken by two team members (NW and PO) to produce a descriptive summary of each group. This was an iterative process of analysis of included papers in each group, individually and in relation to each other, and involved familiarisation, note taking, summarising and synthesis. The results are reported and then discussed in relation to current policy, strengths and limitations, and areas for further research. Methodological learning from undertaking database searches for major trauma care research is also reported.
Results
Study selection
The searches identified 5975 articles from databases, registers, and grey literature sources. Following screening, 43 primary research studies were included in the scoping review. The study identification and selection process is illustrated in Figure 1. PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi:10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/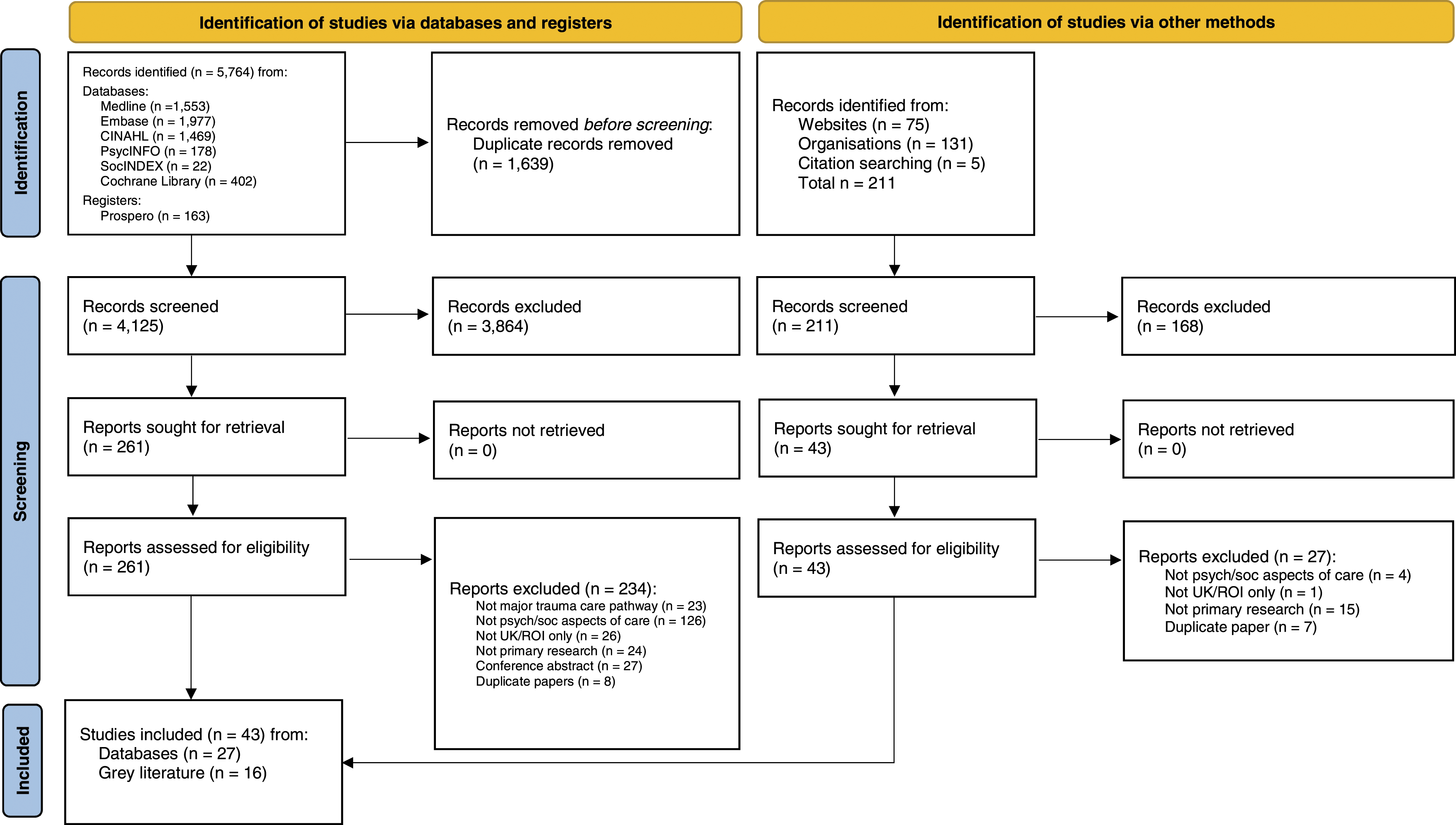
Trend over time
There has been an upward trend in publication of research articles over time (Figure 2). There were few publications per year between 2010 and 2015 with growth noticeable in 2016 and again in 2021. The dip in 2020 is likely an effect of the COVID-19 pandemic which may have delayed article submissions and journal peer review processes. In 2021, 10 articles had been published up to the most recent database search (September) evidencing increased interest and growth. Frequencies of publications over time.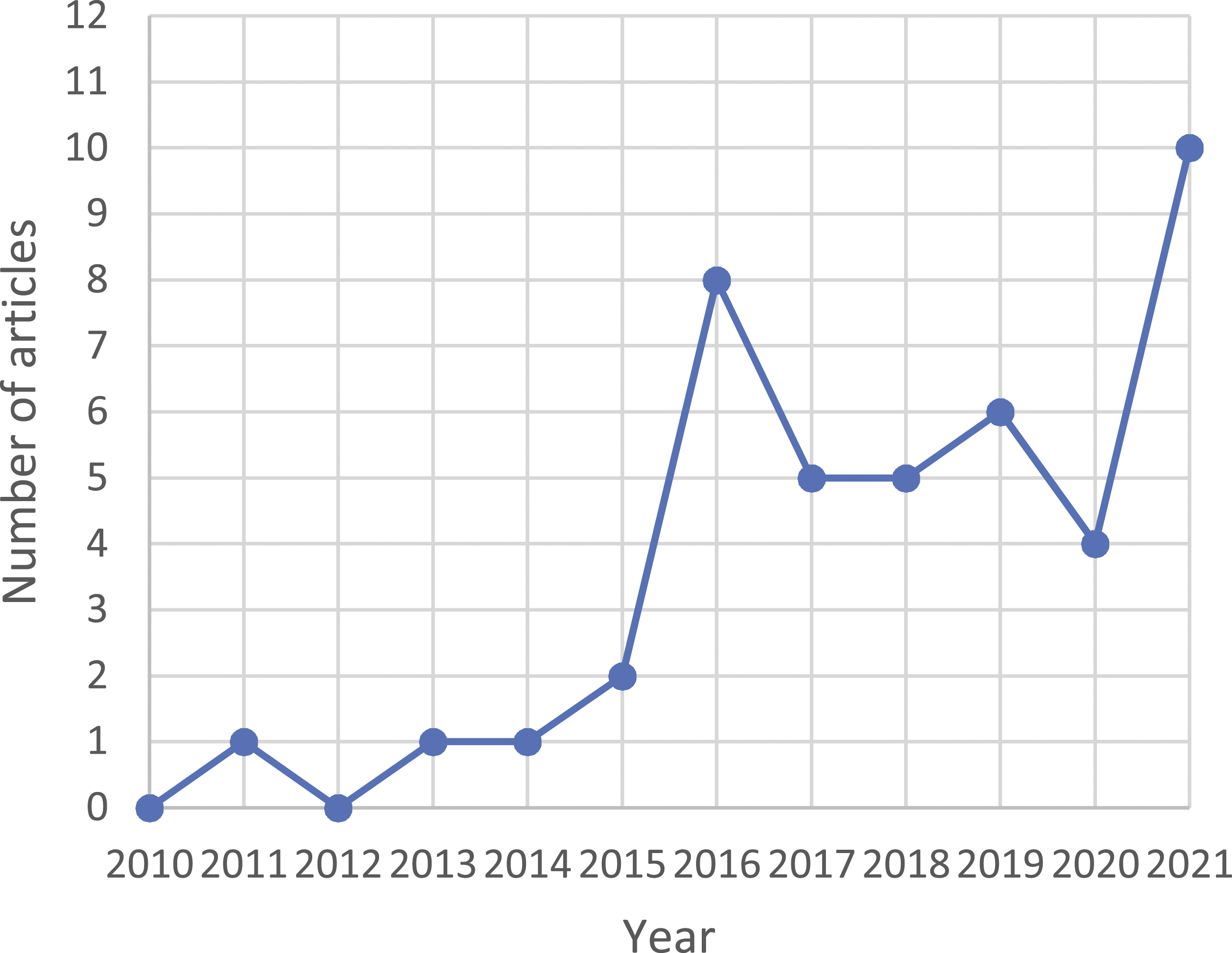
Journals
The included studies were published in a total of 25 journals, the most common being Injury (n = 5), Trauma (n = 4) and Clinical Rehabilitation (n = 3).
Summaries of research evidence
Major Trauma Care Pathways
Eight studies looked at Major Trauma Care Pathways and were concerned with understanding care journeys of patients from admission to discharge and community rehabilitation. They sought to identify gaps in care, examples of good practice, and opportunities for improvement. Three focused on early pre-hospital 31 or acute care32,33 stages of the pathway, whilst another five investigated continuation of care pathways to post-acute care services, including psychological, 34 vocational, 35 rehabilitation36,37 and neurorehabilitation. 38 Three studies focussed on children under 18 years of age31,36,38 and three looked at pathways for patients with specific causes of injury; suspected child abuse 31 and suicide attempt.32,33 Most studies in this category involved analysis and audit of routinely collected, local or national, quantitative trauma data. Three studies were mixed method, incorporating interviews or surveys to gather patient and professional stakeholder perspectives.
Key findings in this group related to gaps in major trauma care. Rehabilitation pathways overall were reported as fragmented and regionally inconsistent, lacking in vocational and psychological support with poor communication and co-ordination between acute and community services.35,37 Some types of major trauma injuries were found to have more established and integrated pathways (e.g. traumatic brain injury, spinal cord injury) than others (musculoskeletal injury).35,37 Gaps were also noted in children’s rehabilitation services 36 and in neurorehabilitation services for children under 4 years. 38 In addition, it was found that children presenting with injuries caused by suspected child abuse were less likely to trigger a major trauma alert, be taken to a major trauma centre and receive timely intervention despite having more serious injuries. 31 Recommendations for practice involved addressing identified gaps in service provision, better recognition of the role of mental health in recovery journeys and incorporation of psychological and vocational support into major trauma care pathways.
Major trauma and care experiences
There were 12 studies in the major trauma and care experiences group. Four explored adult patient experiences in relation to: being a patient in an emergency department following trauma, 39 the trauma experience itself, 40 and a specific injury (multiple rib fractures).41,42 Three studied patient and family experiences; one was adult-patient and family focused 43 and two were about children’s and parents’ experiences of major trauma care.44,45 Two further studies explored family members’ experiences alone; one about parents’ experiences 46 and the second about impacts for family members who lived far from the intensive care unit where their adult relative was admitted. 47 Two studies incorporated service provider as well as patients’ perspectives about trauma care48,49 whilst another focused solely on service provider views. 50 Most studies in this category employed qualitative methods for data collection, 10 used semi-structured interviews, one study applied an ethnographic approach that incorporated observations as well as interviews, and one study used a postal survey.
The desire for a ‘return to normality’ and resumption of pre-trauma routines and activities was a key finding across several studies.41,42,44,46 Parents talked about additional responsibilities they faced in supporting their child’s recovery and impacts for family and work life. 45 Similarly, family members supporting adults after major trauma described additional caring responsibilities, 48 and psychological, physical (exhaustion), and financial impacts. 47 Post-traumatic stress type symptoms were common experiences for patients and family members.39,41,45–47 One study found that the way patients spoke about their major trauma experience could identify psychological distress cues to aid early detection by clinical staff of mental health needs. 40 Patients and family members had unmet information needs about the injury, the impact of injury (daily activities, occupational, emotional) and about management and recovery which caused anxiety and made transitions home difficult.43–49 Service providers from across the trauma care pathway were very much aware that sometimes trauma care was below best-practice standards because of capacity pressures and lack of psychological and vocational services. 50 In addition, patients did not always know about or were unable to access relevant services after discharge,48,49 and sometimes when they did request services such as counselling their needs were dismissed. 49 Across the studies, participants did report positive experiences too, and these were in relation to timely and person/family-centred care and communication of information,43,44,48,49 and a contact 45 or case manager48,49 to answer questions after discharge. Recommendations for practice included fulfilling patient and family information needs, attending to distress, provision of psychological support for patient and family members, access to the right care at the right time, better communication between services, and a contact for questions after discharge from hospital.
Major trauma care innovations
Eleven studies were evaluations of major trauma care innovations. These studies were about better integration of rehabilitation into major trauma care,51,52,53 improving transition from hospital to community,54–56 addressing psychosocial impacts of major trauma,53,57 integrating psychological support,58,59 improving communication between patients and surgeons 60 and designing trauma care education for intensive care nurses. 61 A variety of methodological approaches were used in this category, including several mixed methods approaches.
Key findings from the major trauma innovations group of studies related to improvements in rehabilitation, self-management, psychosocial, and psychological aspects of care. Educational intervention aimed at health professionals proved positive in facilitating patients’ self-management,55,56 though sustainability was difficult with challenges related to upskilling and adoption across diverse multi-disciplinary teams,55,56 staff turnover, 56 and bed occupancy pressures. 55 Elsewhere, a quality trauma discharge package of pharmacy counselling and tailored aftercare facilitated patients to manage their own self-care needs and improved patient satisfaction. 54 Other successful innovations included a model of paediatric neurorehabilitation, 52 an integrated rehabilitation service, 51 vocational rehabilitation training for occupational therapists, 53 a free legal service for trauma patients providing advice about welfare, insurance, employment, care, and housing, 57 an embedded psychology service providing support and tools to manage distress, 58 and a community peer support programme for people following spinal cord injury. 59 These evaluations of major trauma care innovations are important in illustrating locally successful practices that could be used to advance psychological and psychosocial aspects of major trauma care nationally.
Major trauma assessment tools and outcome measures
There were nine studies investigating major trauma assessment tools or outcome measures. These investigated tools to predict psychological outcome following major trauma62,63 and effectiveness of cognitive screening tools for patients with traumatic brain injury.64,65 Feasibility of assessment of frailty by emergency department nurses was the focus of one study. 66 Four studies investigated outcome measures, in terms of identifying the most important rehabilitation and health outcome measures, 67 a patient-centred method for pre and post trauma measures of function, 68 and outcomes relating to return to work.69,70 Most studies in this category used quantitative methods.
In terms of key findings, patients whose injuries were a result of violence had greater post-traumatic stress and depressive symptoms than those whose injury was accidental. 63 Posttraumatic Adjustment Screen (PAS) scores during admission were found to be significant predictors of post-traumatic stress symptoms and psychological distress following discharge. 62 An online survey of 14 clinical psychologists in neuropsychology found that the Addenbrooke’s Cognitive Examination-III and the Montreal Cognitive Assessment were the most frequently used cognitive screening tools for patients with traumatic brain injury. 64 And in related work, a shortened cognitive assessment tool (Neuropsychological Assessment Battery Screening Module, NAB-SM) was found to be promising for identifying cognitive impairment following traumatic brain injury, though the authors advise caution of interpretation of findings at this early stage of testing. 65 Similarly, feasibility studies produced promising results for frailty assessment by emergency department nurses 66 and for patient-centred assessment of pre-trauma functionality. 68 One study found that even though two-thirds of major trauma survivors had a complete return to work, they continued to have poor quality of life outcomes and ongoing mental health issues. 69 This led the authors to conclude that major trauma survivors have long term, often unmet health needs for several years and that return to work alone was an insufficient outcome measure. 69 Across the studies there were calls for improved psychological screening and support62,63,69 and for further research to develop patient-centred assessment tools and outcome measures.65,66,68,70
Major trauma research prioritisation studies
There were three research prioritisation studies. Two involved research priority setting in relation to specific injuries, burns 71 and complex fractures 72 whilst the third study was broader relating to all major trauma populations. 73 Studies in this group employed a variety of prioritisation consensus methods. Research questions of effectiveness of psychological and psychosocial needs assessments and interventions featured across all the research prioritisation exercises.
Discussion
The findings from this scoping review indicate that major trauma care pathways in England are inherently complex (involving myriad services), partial and fragmented, and lack effective communication and co-ordination between services.35,37,43,48,49 The hub and spoke configuration of regional major trauma care in the UK also means that patients’ care journeys may pass through different units and services that may be geographically dispersed and which may be difficult for patients, families, and clinicians to navigate. The scoping review also identified that some types of major trauma injury had more established and integrated pathways whilst others were underserved.31–38,49,50 In summary, there is inherent inequity across major trauma care pathways that likely result in health inequality following major trauma, and which may be amplified by existing health and social inequalities. The NHS standard contract for major trauma care providers advocates for holistic trauma care that includes co-ordination of immediate and ongoing care, provision of information about major trauma care pathways, signposting to voluntary and/or non-government support services that can assist with psychological and social impacts of major trauma as well as supporting family members and carers during and after admission. 21 The findings of this scoping review indicate that this standard is frequently not achieved. Congruent with previous research,7–12,14,15 the scoping review also found that psychological (e.g. post-traumatic stress symptoms, sense of self)39–41,45–47 and psychosocial (e.g. family, social, work or school life) impacts were commonly reported by patients and family members, though needs relating to these aspects of care were often not met.41,43,45–50 In the wider literature, collaborative care, described as a multidisciplinary team approach to evaluate patient needs and provide individualised care, was identified as a promising practice for reducing post-traumatic stress symptoms and preventing PTSD following traumatic injury though warranting further research. 74
The scoping review identified several studies evaluating innovations to improve care pathways in hospital51–53 and in transition to home or community care.54–56 Innovations for integrating hospital-based services for psychosocial aspects (legal advice service, 57 vocational support service, 53 peer support programme 59 ) and psychological support 58 evaluated well. Reports of these locally successful innovations raise important questions about strengthening the position of psychological and psychosocial aspects of major trauma care in national policy documents, establishing clinical effectiveness of innovations, feasibility testing to inform wider adoption and methods for sharing promising practices across regional major trauma networks.
The NHS major trauma standard contract
21
has two aims relating to psychological and psychosocial aspects of major trauma care: • To deliver a system based on a pathway of care from the pre-hospital phase including rehabilitation [general and specialist] and a return to socio-economic functioning (pp4). • To improve the functionality, health and psychological wellbeing, in those patients who survive their traumatic injuries; increasing their quality of life (pp4).
To demonstrate achievement of these aims effective assessment tools and outcome measures are required. Research investigating tools for types of psychological,62–65 functional, 68 and frailty 66 assessments were important foci of research. The Posttraumatic Adjustment Screen was found to have potential for identifying those at risk of developing PTSD and/or depression after major trauma and who may benefit from early clinical psychology intervention. 62 We did not find any research about tools for assessing distress and concerns relating to psychosocial impacts of major trauma. Overall, there was no clear indication about which assessment tools were best for which situation nor what they should lead to. The scoping review also identified that current outcome measures may not be sufficiently nuanced to capture patient and/or family centred outcomes. For example, ‘return to work’ was found to be an insufficient outcome measure and indicator of recovery because many trauma survivors, though having returned to work, reported enduring and often unmet health needs that may not be captured by existing major trauma outcome measures. 69 Many studies made recommendations for development of patient-centred assessment tools and outcome measures.65–70
Strengths and limitations
Scoping reviews have their own challenges because their research questions are intentionally broad to identify and summarise the range and extent of literature in a field yet require clarity in terms of population and area of interest. 26 We balanced comprehensiveness conceptually (psychological and psychosocial aspects of care) and methodologically (seven databases and grey literature search) with focus (primary research across the newly adopted UK major trauma care pathway). Inclusion and exclusion criteria were developed to ensure breadth and comprehensiveness yet retain focus and feasibility. 26 The review is limited by its focus on the major trauma care pathway which may have missed studies undertaken in the UK’s Trauma Units, either as a primary place of major trauma care or as a secondary place of care for patients repatriated from major trauma centres. It is also limited by its UK focus, there is likely relevant and potentially transferable research from outside the UK (e.g., validation of mental health assessment tools with major trauma populations). Nonetheless, this scoping review has identified gaps in the UK evidence base and provides a foundation to inform further research to develop psychological and psychosocial aspects of major trauma care in the UK. A further strength of this study was the involvement of public and professional stakeholders in shaping the scope and focus of the review.
Methodological learning: Major trauma research
Through undertaking this scoping review, we found that research about major trauma care was not readily identifiable from papers’ titles and abstracts, or indeed from full texts. We also found that many studies were flagged as taking place in a major trauma centre, but the research was not in fact about major trauma patients or the major trauma care pathway. In the absence of an agreed database indexing system, we recommend authors identify the focus of major trauma research by expressly stating, for example that it is about major trauma, major trauma care, major trauma care pathway etc., in the title and/or abstract.
Conclusion
Psychological and psychosocial aspects of major trauma care is gathering momentum as an important yet underserved field of major trauma care practice and research. The aim of this scoping review was to identify and bring together primary research in the field, undertaken in the UK since the introduction of the UK’s first major trauma care pathway, to identify what has been done and where further research is needed. Survivors of major trauma often live with lifechanging injuries and this scoping review along with previous research illustrates that psychological and psychosocial impacts are common following major trauma in both the immediate period and longer term. However, it also identified that these aspects of care are commonly underserved in current care pathways in the UK. The review found that some major trauma care pathways are better served than others, concluding there are inherent inequities across major trauma care pathways that likely result in health inequality following major trauma, and which may be amplified by existing health and social inequalities. Therefore, it is important that regional major trauma operating delivery networks map their provision of care across all major trauma populations to identity and address service gaps and inequities.
Though the scoping review identified a growing body of research investigating psychological and psychosocial aspects of major trauma care pathways in the UK, significant gaps in the evidence base remain. Presently, there are no published evidence-based standards or best practice consensus at the national level in the UK for psychological and psychosocial aspects of major trauma care. A qualitative evidence synthesis of the 12 studies exploring patient and/or family member experiences of UK major trauma care pathways would be useful to answer questions about care pathway complexities and inform future development of national practice guidelines. Further primary research is also needed to establish clinically effective psychological and psychosocial assessment tools (e.g., which tools are best for which purpose and population at which timepoints), corresponding psychological and psychosocial interventions, and patient-centred outcome measures so that in the future survivors of major trauma and their family members and/or carers receive the most appropriate care and intervention.
Supplemental Material
sj-pdf-1-tra-10.1177_14604086221104934 – Supplemental Material for Psychological and psychosocial aspects of major trauma care in the United Kingdom: A scoping review of primary research
Supplemental Material, sj-pdf-1-tra-10.1177_14604086221104934 for Psychological and psychosocial aspects of major trauma care in the United Kingdom: A scoping review of primary research by Philippa Olive, Lucy Hives, Neil Wilson, Amy Ashton, Marie Claire O’Brien, Gemma Mercer, Raeesa Jassat and Catherine Harris in Trauma
Footnotes
Acknowledgements
The authors would like to thank the wider professional and public members of the RePEAT (Research and innovation to address Psychological, Emotional, and psychosocial wellbeing After major Trauma) project group who served as advisors for the study.
Author contributions
PO, LH, AA, MCOB, GM, NW and RJ contributed to conception and design of the work. CH contributed to design of the search strategy. LH, RJ and PO contributed to the acquisition of data. LH, NW and PO contributed to the extraction and analysis of data. PO, LH, NW, AA, MCOB and GM contributed to contextualisation and interpretation of data. PO, LH, NW, AA, MCOB, GM, RJ and CH contributed to drafting and revision. All authors have approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the UCLan Institute for Global health and wellbeing (LIFE) Research Writing Group Grant.
Guarantor
PO acts as guarantor for this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.