
Abstract
Introduction
Children, given anatomical variations, are at increased risk of renal injury following trauma. The management of paediatric renal injuries has, similar to other solid organ injuries, largely shifted towards conservative management; however, hemodynamically unstable patients may still warrant surgical exploration or interventional techniques. The aim of this study is to describe the local incidence, demographics, morbidity and outcomes associated with high- and low-grade renal injury in a paediatric major trauma population.
Method
This was a 5-year retrospective review of trauma registry data and chart analysis of all paediatric renal injuries from major trauma at a North American level 1 paediatric trauma centre between January 2016–31 December 2020. Data was analysed using SPSS v27 with p < 0.05 considered significant.
Results
Of 1334 major trauma patients, 45 suffered a kidney injury (20 high-grade and 25 low-grade injuries), of which 93.3% underwent conservative management with no difference in outcomes between groups. 80% of patients had concurrent injuries (a quarter requiring surgery for these), with a trend towards higher rates of chest injuries in high-grade renal injury patients (p = 0.08). Bicycle injuries were statistically more likely to cause high-grade renal injury (p = 0.02). Angiography was utilized infrequently (3/45 patients, 6.6%), and no patients underwent embolization in our study population. Overall mortality (4.4%) and length of stay were unaffected by grade of injury.
Conclusion
Paediatric renal injury is an uncommon injury in major trauma patients (3.4%). Most cases can be managed conservatively regardless of the grade of injury. Renal injury patients are likely to have concurrent injuries, often requiring surgery. Further studies are needed to measure the success and utilization of interventional radiology techniques for management in children.
Introduction
Injury remains the leading cause of death and disability in Canadian children and youth, and abdominal trauma is an important contributor to morbidity, and sometimes mortality.
Children are more vulnerable to sustaining significant abdominal trauma given their unique anatomic characteristics. Relatively compact torsos with smaller anterior-posterior diameters reduce the area over which the force of the injury can be dissipated. Larger viscera, including their liver, spleen and kidneys, extend below the costal margin and the bladder sits intra-abdominally instead of protected within the pelvis, making these organs vulnerable. 1 Additionally, children often have less overlying fat to cushion intra-abdominal structures from blunt force. Physiologic differences in children that allow for robust vasoconstriction and natural haemorrhage control 2 also allow for the majority of abdominal trauma in children (as now also in adults) to be safely managed conservatively and rarely requiring operative intervention.2–10 Furthermore, the World Society of Emergency Surgery and the American Association for the Surgery of Trauma (AAST) guidelines state that non-operative management (NOM) should be the treatment of choice for all hemodynamically stable or stabilized minor-moderate (AAST I-II and III) and severe (AAST IV-V) lesions.11,36 In their study outcomes, no specific recommendations exist for NOM in blunt and penetrating kidney injuries in children that are different than those used for adults. 12
The literature currently lacks definitive data on the management and outcomes specifically of paediatric renal trauma patients, and controversy still exists about the role of conservative management in high-grade injuries in this cohort.13–15 In adults’ angiography and embolization use is increasing for kidney injuries, yet there is little in the literature for the paediatric population. Current indications for angiography and embolization in children are not universally recognized, but include moderate and severe injuries, active bleeding with contrast blush on CT-scan and ongoing haemodynamic instability. 12
The purpose of this study was to determine the incidence, demographics, morbidity and outcomes associated with high- and low-grade kidney injuries resulting from major trauma in a paediatric population within a single level 1 paediatric trauma centre in North America. 16
Method
A retrospective chart and trauma registry review of paediatric (< 17 years old) trauma admissions from 1 January 2016 to 31 December 2020 was performed. Approval for the study was granted by the Hospital for Sick Children, Research Ethics Board Review Board. The Hospital for Sick Children is a major trauma centre providing care to children across Ontario, Canada.
Trauma patients were identified as those meeting requirements for level 1 or level 2 trauma team activation in the emergency department (ED) or patients whom did not receive a level 1/2 call but had injury severity scores (ISS) ≥ 12 (i.e. trauma transfers with significant injuries or walk-ins found to have severe injuries on imaging).
The patient demographics, injury type, associated injuries, ISS, length of stay (LOS), management (surgical, embolization, conservative and use of haemostatic resuscitation) and the kidney injury grading were reviewed. The AAST renal injury grade was determined by chart review using EPIC/Kidcare, as well as review of computed tomography (CT) reports and operation notes. Renal injury grades were divided into low- (I–III) and high-grade (IV–V) injuries for comparison using the AAST classification.
Categorical variables were compared using Pearson chi-squared and Fisher’s exact test, with p ≤ 0.05 considered as a significant result. Statistical analysis was conducted using SPSS V27.
The primary outcome was mortality; secondary outcomes included operative management, blood products, hospital LOS, intensive care unit (ICU) LOS and concurrent injuries sustained between the two groups.
Results
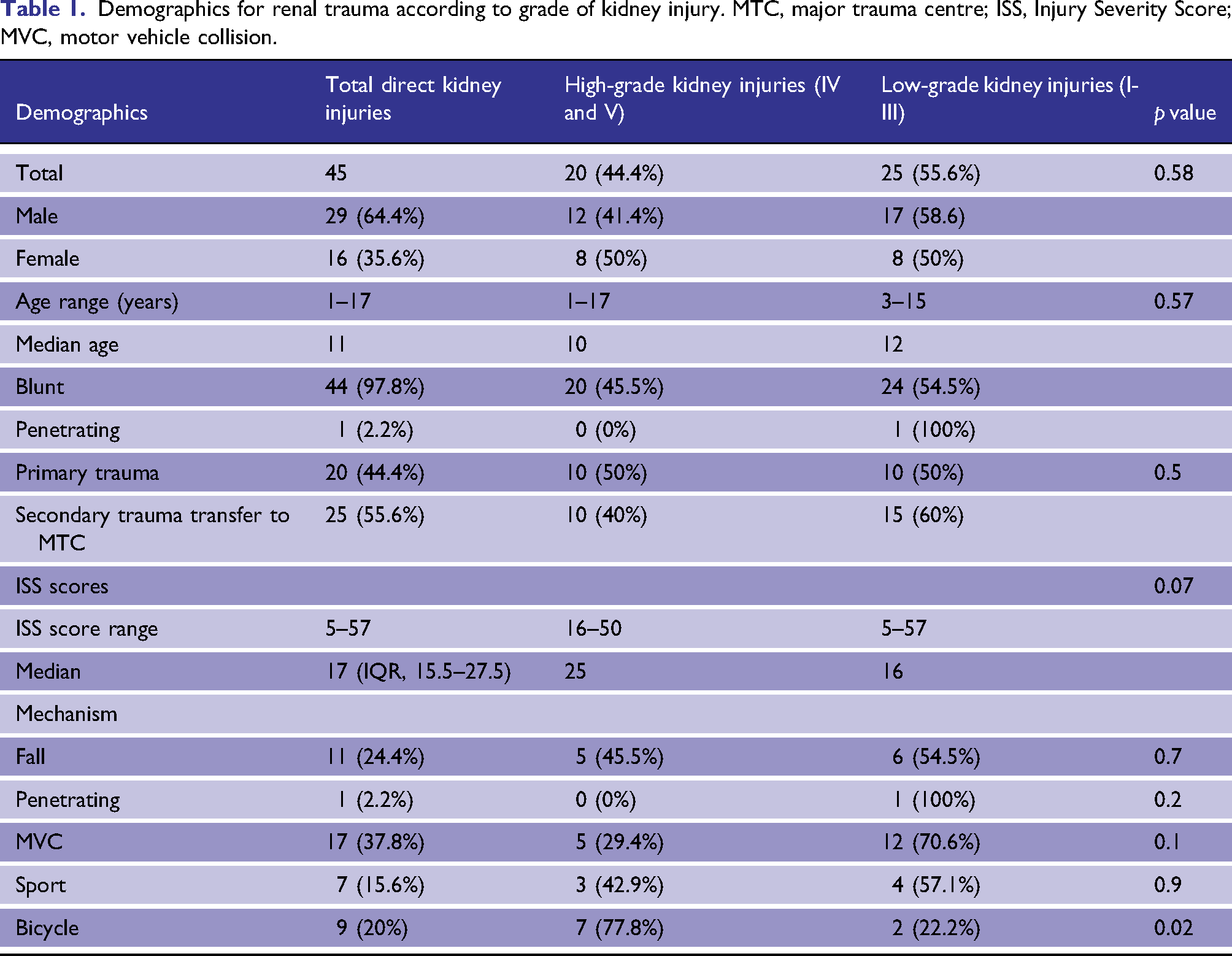
Demographics for renal trauma according to grade of kidney injury. MTC, major trauma centre; ISS, Injury Severity Score; MVC, motor vehicle collision.
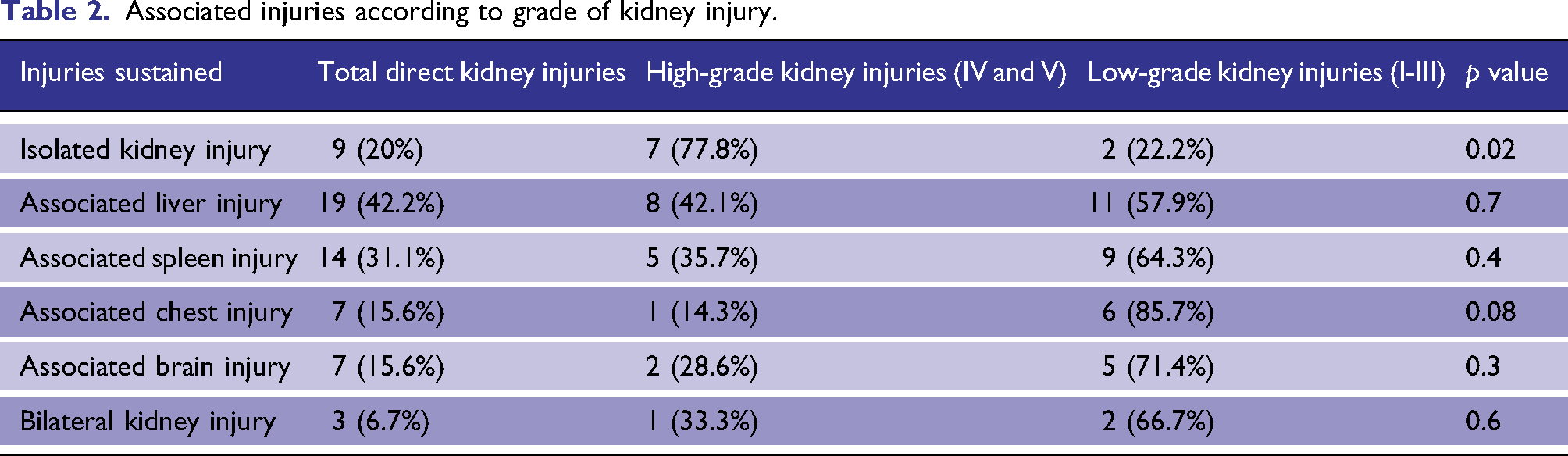
Associated injuries according to grade of kidney injury.
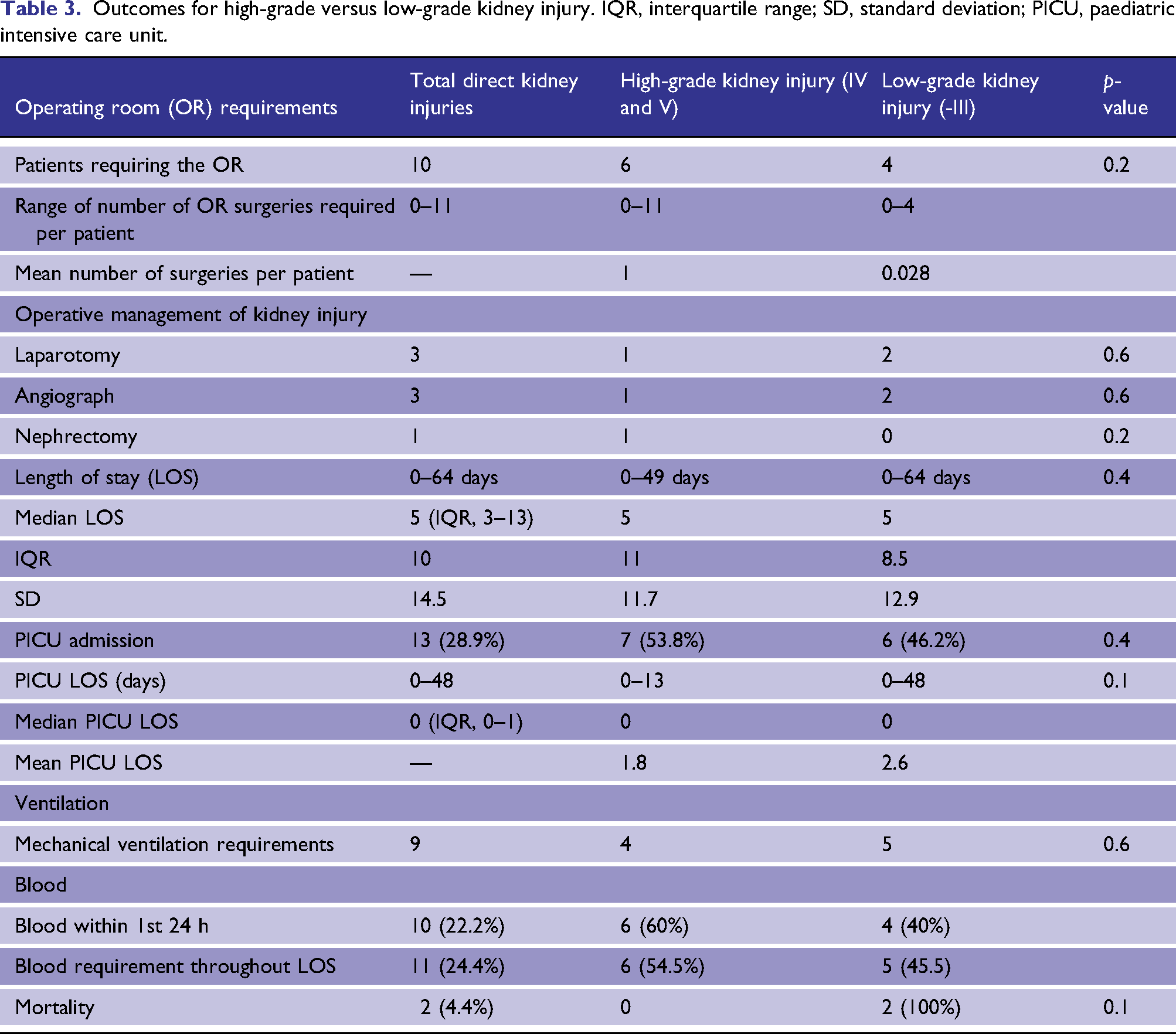
Overall, 22% of patients with a direct kidney injury required operative management for their traumatic injuries, though only 6.7% of patients required operative management specifically for their renal injury; three patients underwent laparotomy, two for low-grade and one for high-grade injuries with one nephrectomy for high-grade injury. Three patients required angiography (6.7%) (two low-grade and one high-grade); no patients received embolization.
Outcomes for high-grade versus low-grade kidney injury. IQR, interquartile range; SD, standard deviation; PICU, paediatric intensive care unit.
Discussion
At a high-volume tertiary paediatric trauma centre in Canada, the incidence of kidney injury was rare (3.4%). Of those that did have a kidney injury, the split between high-grade and low-grade was 44.4% and 55.6%, respectively, with conservative management being achieved in 93.3%. Despite conservative management for the direct renal injuries in our study population, most children with renal injury had concurrent injuries (80%), with just under a quarter requiring operative management for these other injuries and a quarter requiring blood/blood products. Of the 6.7% of patients requiring surgery for a direct kidney injury (laparotomy), two patients went straight to the operating room (OR) from the ED, and one to the paediatric ICU prior to OR. The mechanisms of injury for these patients were MVCs in two and one penetrating gunshot wound injury.
In our study, the majority of renal injuries were managed conservatively, even when high-grade, which is similar to the current literature that demonstrates nephrectomy rates in these patients (2.2%) are rare.16–19 These rates are lower than those in the adult population where the incidence is approximately 6%,20–22 despite the anatomical vulnerability of these organs in children.20–22 The grade of renal injury should therefore not be the only parameter used to decide on surgical management or nephrectomy for traumatic injury to the kidney, particularly in children. Haemodynamic status, concurrent injuries and requirement for haemostatic resuscitation acutely should be taken into account in decisions regarding operative management. Angiography was rarely utilized (3/45 patients, 6.6%), and no patients underwent embolization in our study. Similarly, Graziano et al. showed embolization rates of 1.4% and Ishida et al., 1.5%. We may be limited in our study to capture these rare events given the infrequent occurrence of this important intervention.16,22 Furthermore, the only nephrectomy in our patient cohort occurred in the acute period where the patient went from the trauma bay to the OR immediately.
This nephrectomy was for an avulsion to the upper pole of the left kidney (Grade 5 injury) with urinary extravasation. The remaining two surgical laparotomy patients underwent renal repairs, further details of which were not highlighted in the initial data. These interventions were all ‘early’, and it is important to note that no ‘late’ interventions (ureteric stent or nephrostomy) were required for ongoing urinary leak or late nephrectomy.
Hospital and ICU LOS did not differ between groups. This is consistent with previous studies that demonstrate hospital LOS did not increase with worsening severity of renal injury, and instead was determined by the severity of the non-renal-associated injuries.16,23,24 This suggests that renal trauma in isolation has a consistent prognosis between groups and other associated injuries are the factors that prolong LOS. However, associated injuries in these patients are significant with a high overall mortality rate of patients with renal injury (4.4%) compared to all mortality rates for our institution (3.1%) for major trauma. Across the world, in-hospital mortality of paediatric trauma patients is reported to vary from 0.3% to 8.5%.25–32 Mortality in all cases from this cohort was related to concurrent severe brain injury.
Although there is no difference in ICU stay or hospital LOS between our two groups, it is important to note that there is also no significant difference in important associated injuries. For example, multiorgan injury, specifically neuro trauma, is related to a higher degree of mortality. Our results demonstrate that these important contributors of morbidity were similar between the two groups. Injuries such as intra-abdominal (liver and spleen), head injury and chest trauma that typically cause ICU admission were present in both cohorts.
Although most renal patients did not require surgery for their injuries, it is possible that acute kidney injury (AKI) from their injuries contributed to their ICU requirement/organ support needs. However, the overall LOS was likely related closely to other concurrent injuries. We do not have information on creatinine/urine output in order to characterize AKI in this patient cohort.
The trend towards chest injury and high-grade kidney injury can be explained by the fact that the kidney’s position is relatively high in the abdominal cavity. The thorax needs to be evaluated thoroughly, particularly for patients with bicycle injuries, who tended to have a higher incidence of high-grade renal injury. The positioning of the handlebars may account for this with direct impact taking most of the force on the upper abdomen/lower chest.17,19,23,34 Isolated injuries were more likely to be high-grade injuries, perhaps due to more force being applied through a smaller area.
A strength of this study was the comprehensive and meticulous recording of registry data by a single trauma registry analyst, which reduced bias secondary to inaccurate or incomplete data. Limitations included the small number of patients in the cohort, retrospective design for assessing data and insufficient details for certain data elements such as biochemical derangement, urinary output or the presence of acute kidney injury in relation to direct injury. Future research would benefit from multi-centre involvement to more accurately assess the utilization of embolization for this injury type and to further delineate important rare events.
Conclusion
Renal injury in children is uncommon, and management is primarily conservative with low operative rates and distinctly uncommon use of interventional modalities. Mortality rates are high, secondary to concomitant injuries, and high- versus low-grade renal injury did not impact mortality. More data is needed to determine the utility of interventional radiology in paediatric renal trauma.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was obtained from Research Ethics Board at the Hospital for Sick Children Toronto (RE approval number 100,074,627)
Informed consent
Informed consent was not sought for the present study because 5-year data already collected as part of the trauma database and de-identified.