
Abstract
Introduction
Motorcyclists are over-represented in collision statistics in Ireland. There is a lack of descriptive studies assessing the impact and injury pattern of this trauma cohort. This study examines this trauma subset using data collected by the Major Trauma Audit (MTA) by the National Office of Clinical Audit (NOCA) to identify patient demographics, injury mechanism and type, treatments received, and outcomes.
Methods
All motorcycle-related trauma cases recorded on the MTA, NOCA in Ireland for the period 2014 to 2019 were gathered and analysed.
Results
There were 704 cases identified; 94% of cases were male. The median (interquartile range (IQR)) age was 38.2 (26.7–49.7). There were 6.4% (n = 45) aged 0–18 years, 88.2% (n = 621) aged 18–64 and 5.4% (n = 38) greater than 65 years. The median injury severity score (ISS) overall of this trauma cohort was 13 (IQR 9–24) but 306 patients (43.5%) had an ISS
Conclusion
Motorcycle trauma predominantly affects a young male population with moderate severity injury characteristics. A significant proportion of patients present at weekends during the summer months, likely the result of recreational riding. A large cohort of patients requires transfer for definitive care, which has significant implications for trauma care pathways. National policies to enforce safety measures and public awareness for recreational motorcycle use may improve traffic safety and ultimately population health.
Introduction
Trauma and injury are a global public health issue, accounting for the deaths of an estimated 4.4 million people globally each year; this constitutes nearly 8% of all deaths. 1 These injuries place a massive burden on national economies, as well as patients and their families. This complex patient cohort often requires specialised care with prolonged periods in hospital, equating to 87,768 acute hospital bed days in Ireland in 2018. 2 Traumatic injury can be classified as low, moderate, or severe using the injury severity score (ISS). 3 This is an established scoring system first published in 1971 assessing trauma severity and correlates with morbidity, mortality, and other measures of severity. For each trauma death, there will be two survivors with their quality of life impacted by disability. 4
Road traffic trauma comprises a significant proportion of trauma cases and is the eighth-leading cause of deaths globally. 5 Motorcyclists constitute vulnerable road users, and are disproportionality impacted, with 28% of road fatalities attributed to this group internationally. 5 Motorcycles constituted 1.6% of all registered vehicles in Ireland in 2020, and the number registered increased from 42,492 in 2019 to 44,819 in 2020, an increase of 5.5%. 6 They are proportionately over-represented in collision statistics in Ireland. Data from the Road Safety Authority (RSA), which functions as the statutory body for road safety in Ireland, has shown that motorcyclists are disproportionately impacted by road trauma. In 2018, 6% of road traffic casualties (defined as persons killed or injured in a road collision) in Ireland were the result of motorcycle accidents. 7 The Major Trauma Audit (MTA), published by the National Office of Clinical Audit (NOCA), has similarly shown an increase in motorcycle-related trauma cases. In 2018, 16% of trauma captured by NOCA in Ireland was the result of road trauma (n = 875) with 17% of those (n = 146) involving motorcyclists, compared to 12% (n = 102) in 2017. 2 The safety of this vulnerable group is an increasing concern globally.8–10
Despite the prevalence and risk of serious injury with motorcycle trauma, there is limited research looking at the types of injuries sustained by motorcyclists. Published literature is focused predominantly on fatalities. 11 The existing literature has examined various aspects of motorcycle trauma, including a systematic review looking at the use of motorcycle helmets on morbidity and mortality in collisions.12–18 Published literature reveals a mainly young male cohort. A similar study conducted in a level 1 trauma centre in Saudi Arabia revealed significant injury characteristics with extremities and head injuries the two most common types. 15 However, the lack of specific injury and collision statistics in Ireland makes it more difficult to implement effective prevention strategies and trauma pathways. Conducting a national multiyear study of motorcycle trauma in Ireland may provide a greater understanding of the burden and trends associated with this cohort. The establishment of the MTA in 2013 provides an invaluable resource to access these data.2,19–21
This study examines this trauma subset using hospital-based statistics to identify patient demographics, injury mechanism and type, as well as treatments received and outcomes. By collating hospital data, we hope to provide a clearer picture of injury patterns to guide future health and safety policies.
Methods
This is an observational retrospective study, using national registry data, of motorcycle-related trauma in Ireland over a six-year period from 2014 to 2019. Patients were identified from the NOCA MTA database. Since 2013, the MTA has used the internationally recognised Trauma Audit and Research Network (TARN) methodology, which has been in operation in the UK since the 1980s. 2 The 26 hospitals that receive trauma patients in Ireland submit data to TARN. Eligible cases are identified using the TARN inclusion criteria by running a Hospital Inpatient Enquiry (HIPE) report, or by reviewing Emergency Department (ED) activity log books. The principal function of HIPE is the collection and correlation of data on discharged patients from the acute hospital service. 22 Data is inputted by audit coordinators in the respective hospitals after a retrospective review of patients’ medical records and information technology systems. Data entries are then analysed by TARN's coders and analytical team to create key variables. Injuries are scored between 1 and 6 based on the Abbreviated Injury Scale (AIS) to calculate the ISS.23,24 The ISS is calculated based on the highest AIS score in the three most affected body regions (head and neck, face, chest, abdomen, spine, limbs and others). ISS range from 1 to 75. A score of 1 to 8 is classified as low severity, for example, fractured wrist or ankle; a score of 9 to 15 as moderate severity, for example, fractured femur; and a score >15 as severe injury, for example, large subdural haematoma. The body area with highest AIS severity injury is classified as the most severely injured body region. If there is an equal AIS score in two or more body regions, the most severely injured body region is classified as ‘multiple’.
The Charlson comorbidity index (CCI) is used for statistical adjustment for comorbidities in TARN and has been validated for predicting the outcome and mortality risk for many comorbid diseases. 25
TARN captures the care of traumatically injured patients whose hospital lengths of stay are >72 h, require intensive care or high dependency admission, die in hospital within 30 days, or require transfer to a tertiary/specialist centre for trauma care (Supplementary Online Material: Appendix A). Patients who suffer the following are excluded: isolated single pubic ramus fractures in patients >65 years; isolated femoral neck fractures in patients >65 years; and simple uncomplicated isolated injuries, for example, uncomplicated ulnar fracture. TARN does not capture deaths that occur pre-hospital.
MTA data from 2014 to 2019 was investigated to identify all motorcycle-related trauma cases recorded in Ireland. Information including patient demographics, location of injury, mechanism of injury, body regions injured, ISS, injury type, surgery, treatments received, and outcomes were extracted. Medians with interquartile ranges (IQRs) are reported for continuous variables with a skewed distribution and compared by using Mann–Whitney U-test. Chi-square tests were used for comparisons between categorical variables. For data analysis, we used IBM SPSS Statistics software Version 26. A p-value <0.05 was considered statistically significant. There were no adjustments made for multiple comparisons.
Results
There were 704 motorcycle-related trauma cases that met study criteria, constituting 2.8% of all TARN cases in Ireland during this period. The baseline demographic characteristics of this patient cohort are displayed in Table 1. The majority (94%) of these cases were male (664 of 704), compared to 57.8% (14,757 of 25,532) of the overall trauma cohort (p < 0.001); there were 41 (5.8%) pillion passengers with the remaining 663 classified as motorcyclists. The median age of our patient cohort was 38.2 years (IQR 26.7–49.7), with 45 (6.4%) aged 0 to 18 years and 38 (5.4%) older than 65 years (Figure 1). A detailed mechanism of injury is not available. However, the circumstances of the collisions are shown in Table 1.
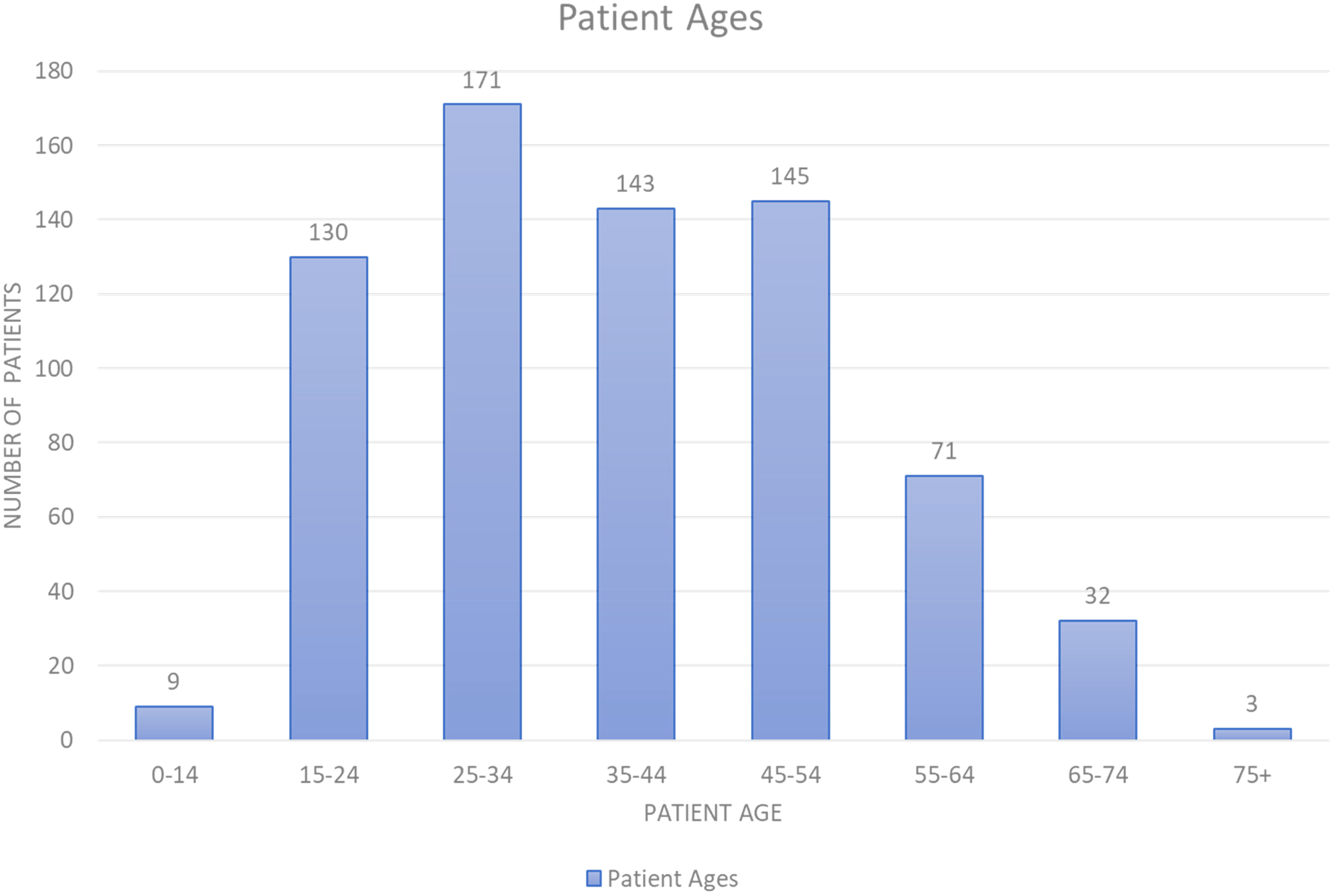
Patient ages breakdown.
Patient demographics presented as numbers (%) or medians (interquartile ranges).
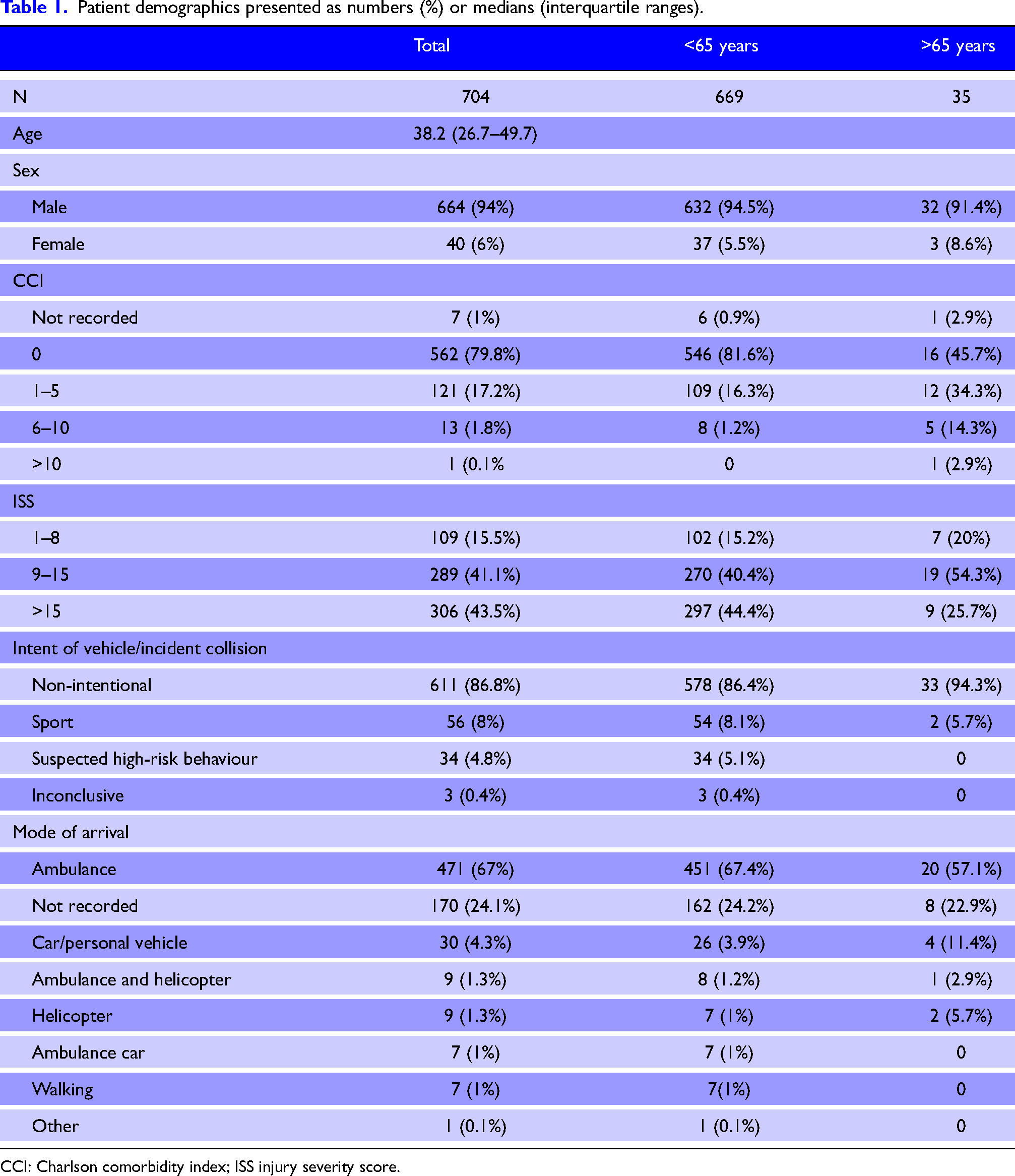
CCI: Charlson comorbidity index; ISS injury severity score.
Patients predominantly arrived to hospital by ambulance (67.3%, n = 471). According to the TARN database, only 17.5% (n = 123) of patients were met by a “trauma team” on arrival to hospital.
Sunday was the most common day of presentation (n = 181, 25.7%) with the fewest cases arriving on Wednesday (n = 70, 9.9%) (Figure 2). The months with the highest attendance were May to August (n = 366, 52%), while January had the fewest presentations (n = 26, 3.7%) (Figure 3). Arrival times to ED are displayed in Figure 4. Patients predominantly arrived ‘out-of-hours’ with 63.1% (n = 444) presenting between the hours of 16:00 and 08:00. There were 15.8% of cases (n = 111) who arrived during ‘rush-hour traffic’ between the hours of 07:00–09:00 and 16:00–19:00 on Monday to Friday.
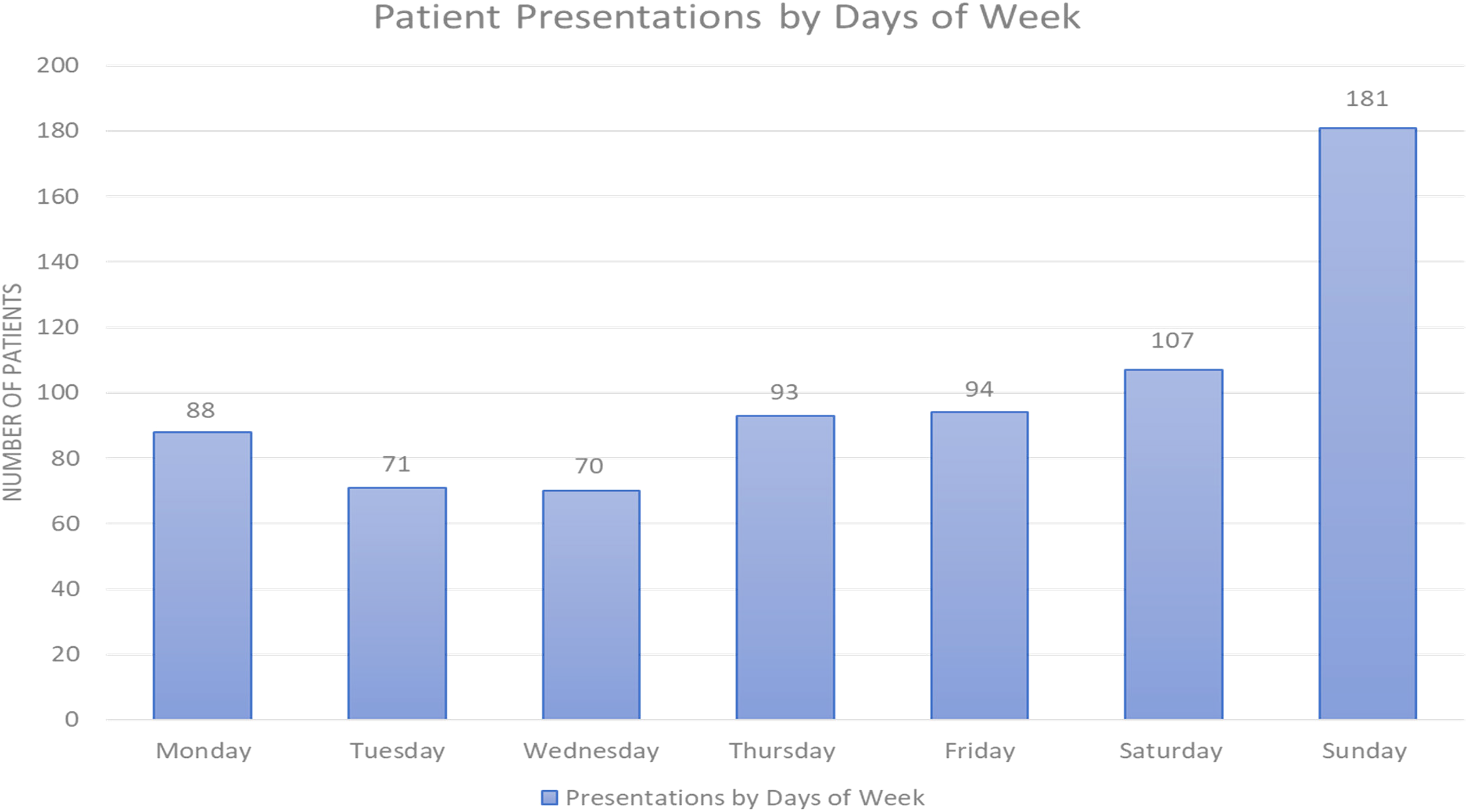
Patient presentations by days of week.
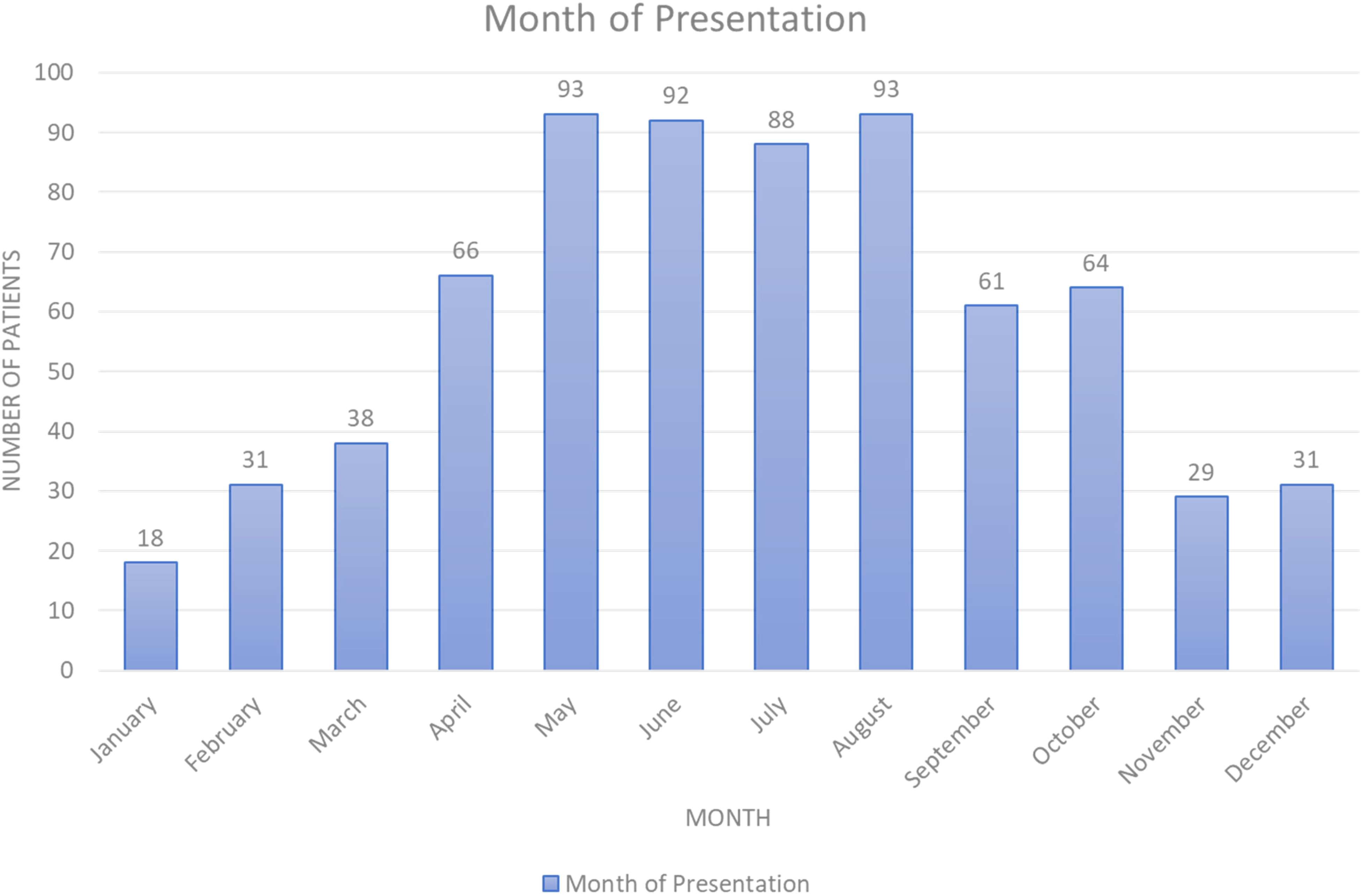
Patient presentations by month.
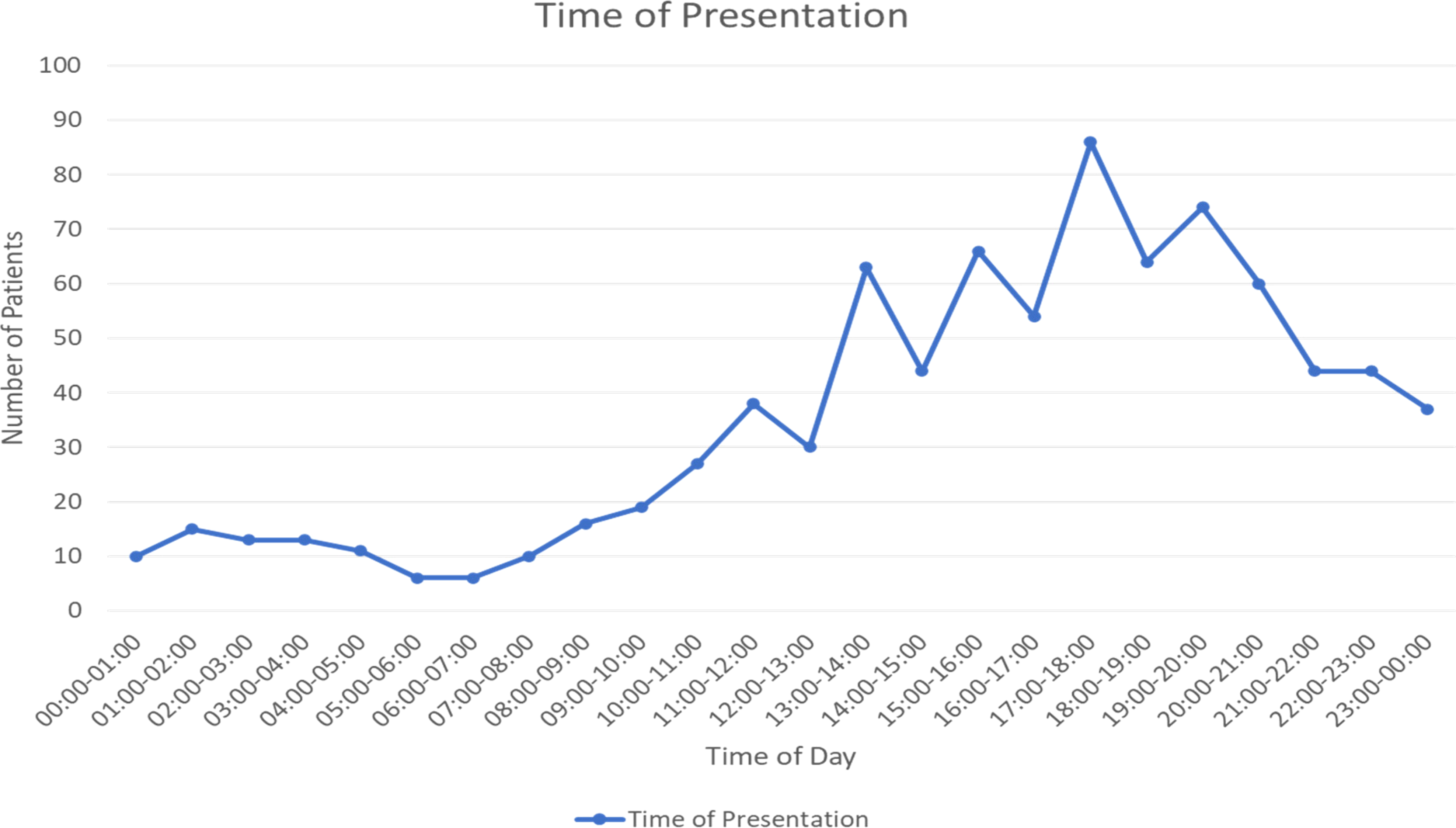
Patient presentations by time of day.
The median ISS of this trauma cohort was 13 (IQR 9–24). The most severe injury body region was the limbs (35.4% of cases, n = 249); followed by the chest (21.3%, n = 150), ‘multiple’ (19.3%, n = 136), head (10.2%, n = 72), spine (9.1%, n = 64), abdomen (3.6%, n = 25) and face (1.1%, n = 8). Almost all cases (99.9%, n = 703) were the result of blunt trauma with just one case resulting from penetrating trauma.
Table 1 reveals the CCI breakdown of our patient group. In total, 79.8% of patients had a CCI of 0. Predictably, patients aged >65 years had higher CCI scores than those under 65 years.
There were 19 (2.7%) patients who did not survive to hospital discharge. The median age of those who died was 36 years (IQR 26–43.5; range 21–53.2) and the median ISS was 34 (IQR 30–45). Head injury was the most seriously injured body area of 42.1% (n = 8) of patients who died.
There was no helmet use recorded in 46 cases (6.5%) and 152 cases where helmet use was not known (21.6%). Of this group who did not wear a helmet, three of 46 (6.5%) patients died compared with 10 of 507 (2%) for those documented as wearing a helmet; this was not statistically significant (p = 0.051). The median ISS for those not wearing a helmet was 14 (IQR 9–28.3).
The median length of hospital stay was seven days (IQR 6–14). There were 174 patients (24.7%) admitted to an intensive care unit (ICU). The median length of ICU stay was four days (IQR 1.3–8). Over half (58%, n = 408) of patients underwent operative intervention. Notably, 43.8% (n = 308) of patients were transferred to at least one other hospital for further care. This compares to 23.6% (n = 6026) of the overall trauma MTA cohort (p < 0.001). A further breakdown is shown of patient outcomes in Table 2.
Patient treatments and outcomes are reported as number (%) or as median (interquartile range).
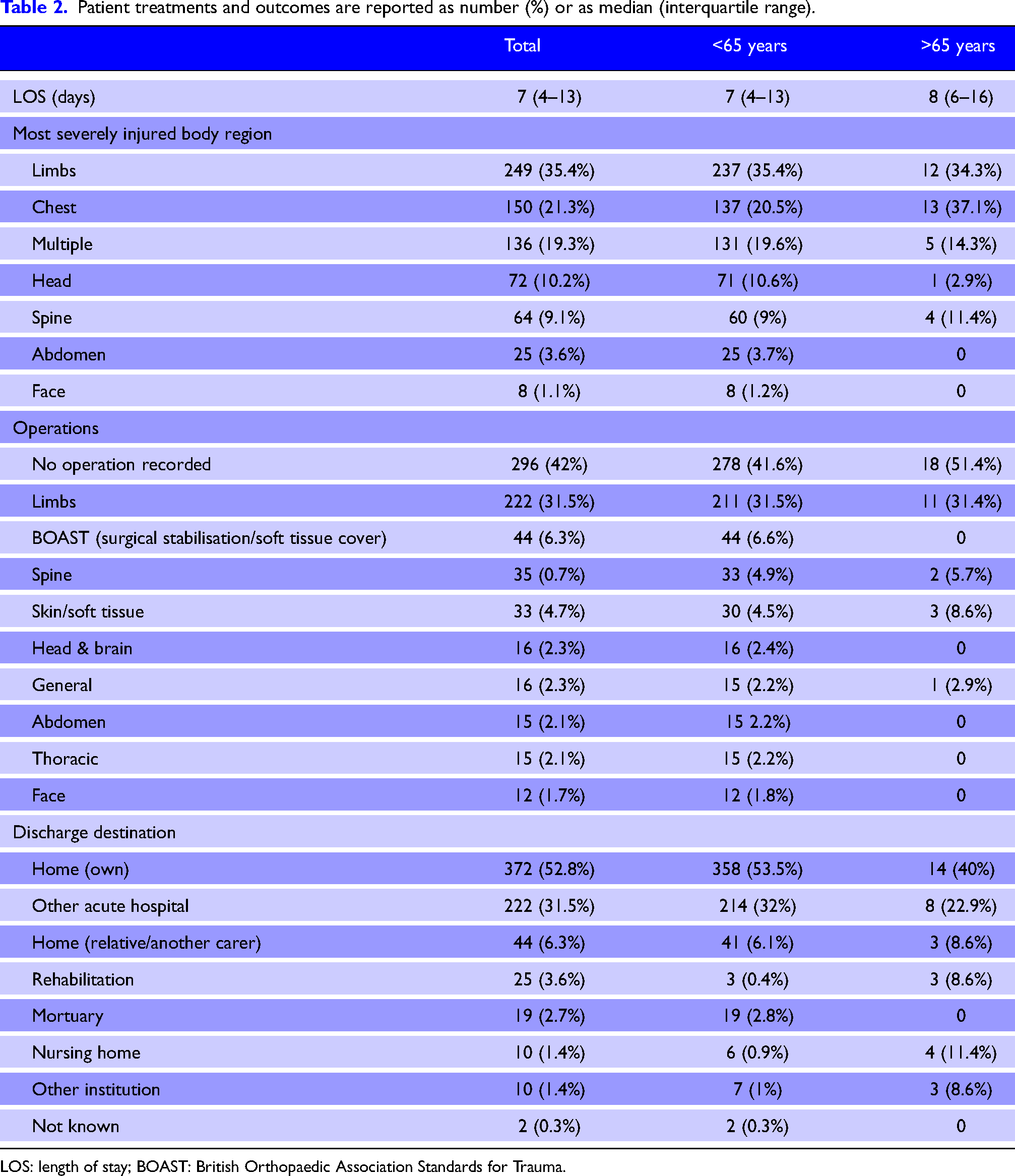
LOS: length of stay; BOAST: British Orthopaedic Association Standards for Trauma.
There were 47 patients aged >65 years. The median ISS for patients under 65 years was 13 (IQR 9–24) and 9 (IQR 9–14.5) for those aged >65 years (p < 0.005). The median length of stay was seven days (IQR 4–13) for those under 65 years and eight (IQR 6–16) for those older than 65 years (p = 0.005).
Discussion
This is the first study of motorcycle-related trauma in Ireland. Road trauma internationally is an enormous public health problem, and global trends would suggest this will continue.26,27 The implementation of effective road safety strategies, legislation to mitigate high-risk behaviours, as well as timely access to emergency services and definitive care is required. It is necessary, therefore, to have reliable and comprehensive data on the burden, injuries, and deaths associated with motorcycle trauma to target interventions and monitor progress. We have shown that motorcycle trauma carries with it significant injury characteristics and extended hospital stays. Motorcycle engine size dictates the legal age to obtain a driving licence in Ireland with 16 being the youngest age to obtain one. Our study revealed that young healthy males were predominantly affected, as was demonstrated by this study and similar ones internationally. 15 This is an important background and context-specific information for the implementation of road safety measures for motorcyclists. With a better understanding of the age-cohort affected, and the activities during which accidents occur, national safety policies, such as media campaigns, can be effectively introduced.
Motorcycle-related trauma predominantly presented in the warm weather of late spring and summer months with 41% of cases arriving on the weekends. This is consistent with the motorcycle riding habits demonstrated by the Road Safety Authority Motorcyclist Rider Behaviour Study in 2017. 28 Most patient attendances were ‘out-of-hours’. This has important implications for provision of unscheduled care and the configuration of the new trauma system for Ireland – access to senior doctors, diagnostics, and operating theatre availability must match these demands.
The lack of specific data surrounding the mechanism of injury makes it difficult to identify precipitating factors. Only 8% of our cases were the result of sporting accidents, with 4.8% associated with suspected high-risk behaviour. There is no further information available for 86.9% of collisions which are classified as ‘non-intentional’. Most motorcycle crashes are likely from recreational use, as most presentations were seen on weekends during the summer. The RSA Pre-Crash Report 2008–2012 on motorcycle fatalities found that speed was a contributory factor in 49% of fatal collisions and 54% occurred in an 80 km/h (50 m/h) speed zone. 11 Similarly, 15% of cases presented during rush-hour traffic, highlighting the importance of motorcycle safety awareness campaigns for other road users.
The median ISS of our trauma cohort was in the moderate severity bracket; nevertheless, 356 patients (41.8%) had an ISS
Ireland has an ageing population, and this is reflected by the burden of trauma in our hospitals with 46% of all TARN patients aged older than 65 years in 2018. 2 While those patients aged >65 years in our study had a lower median ISS, they had longer hospital stays. Older motorcyclists have more age-related comorbidities; these are associated with poorer outcomes. 35 As the population of western countries ages, there is likely to be a higher percentage of older riders presenting. This is an important consideration for planning trauma services going forward.
A key principle in the delivery of trauma care is that every patient is treated at the most appropriate healthcare facility in a timely manner to manage their complex medical needs. Almost half of patients in this study required transfer to at least one other healthcare facility for definitive care of their injuries with (43.8%, n = 308), compared to 23.6% (n = 6026) of the overall MTA cohort during the same period (p < 0.001). Data from the MTA aids decision making in the areas of trauma prevention, rehabilitation, and bypass protocols to ensure that all patients receive the right care in the right place at the right time. 2 Two Trauma Networks are being developed in Ireland to improve trauma care across the service. MTA data enables the National Office for Trauma Services to monitor the impact of the two Trauma Networks to ensure that the advantages of an inclusive trauma system are demonstrably realised. Data from studies such as this allows detailed subgroup analyses in granular detail, revealing further insights. With the development of an integrated trauma system in Ireland, comprising Major Trauma Centres and trauma units arranged into networks, it is hoped that patients will arrive at the most appropriate facility initially, reducing the need for hospital transfers. 3 Similar changes were implemented in the United Kingdom in 2012, which resulted in significant improvements in care processes as well as patient outcomes. 36 Trauma team activation criteria vary by trust and site; typically trauma teams will be activated in the case of significantly abnormal vital signs, suspected life-threatening traumatic injury, a likelihood of necessity for life-saving procedures or operations, or senior clinician concern. 37 Further resources and training for pre-hospital personnel and pre-hospital triage systems could also be considered; the aim is to ensure that the ‘right’ patient is delivered to the ‘right’ hospital initially.
This study has several limitations including its retrospective design and missing data surrounding the circumstances of the mechanism of injury. Lack of data regarding the type of motorcycle or speed involved in collisions and use of protective equipment such as knee braces prevented analysis of the impact on injury characteristics and outcomes. Alcohol and drug use were also not identified and analysed, which may be a confounding factor. This study only assesses trauma cases reported by the MTA (Supplementary Online Material: Appendix A), which will underestimate the true burden of motorcycle crashes on health services. Despite its limitations, this is the first major national study in Ireland analysing motorcycle trauma. This study provides valuable information to inform preventative public health campaigns, help in planning trauma networks, and pave the way for future research in the field.
Conclusion
Motorcycle trauma predominantly affects a young male population with moderate severity injury characteristics. A significant proportion of patients present at weekends during the summer months, likely the result of leisure riding. A large cohort of patients requires transfer for definitive care, which has significant implications for trauma care pathways. More prospective studies are needed to capture injury mechanism. This could be used to facilitate prevention strategies. National policies to enforce safety measures and public awareness for recreational motorcycle use may improve traffic safety and ultimately population health.
Declaration
Supplemental Material
sj-docx-1-tra-10.1177_14604086221130544 - Supplemental material for Motorcycle-related trauma in Ireland
Supplemental material, sj-docx-1-tra-10.1177_14604086221130544 for Motorcycle-related trauma in Ireland by Enda Hession, Micheal Sheehan, Louise Brent, and John Cronin in Trauma
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect of the research, authorship, and/or publication of this article. Provenance and peer review not commissioned, externally peer-reviewed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study received ethical approval from the Research Ethics Committee in St. Vincent's University Hospital, Dublin 4, Ireland.
Informed consent
Not applicable.
Trial registration
Not applicable.
Guarantor
EH
Contributorship
EH and JC were involved in study conception. EH, MS and JC were involved in literature review as well as seeking ethical approval. LB was involved in data acquisition and data analysis with EH. EH wrote the first draft of manuscript. All authors reviewed and edited the manuscript and approved the final version.
Acknowledgements
None.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.