
Abstract
Objectives:
This study aimed to identify the clusters of patients with different developmental trajectories of pain and disability after anterior cervical decompression and fusion (ACDF).
Methods:
Group-based trajectory analysis among 318 patients undergoing the ACDF.
Results:
Three developmental trajectories of disability were identified: “Steadily good functioning,” “Improved functioning,” and “Steadily poor functioning.” Three developmental trajectories of neck pain were identified: “Worsened pain,” “Pain relief,” and “Steadily severe pain.” Two developmental trajectories of arm pain were identified: “Decreased arm pain” and “Severe arm pain with only short-term relief.” No associations were found between sex, preoperative pain duration, or body weight and probability to be classified into a particular disability trajectory group. Female sex (relative risk ratio (RRR) 1.78) and longer history of preoperative pain (RRR 2.31–2.68) increased the probability to be classified into a group with steadily severe neck pain. Longer history of preoperative pain increased the probability to be classified into group with severe arm pain with only short-term pain relief (RRR 2.68).
Conclusion:
After the ACDF, dissimilar developmental trajectories of pain and disability were identified between the patient clusters. While sex, preoperative pain duration, and body weight were not associated with differences in improvement in disability level, female sex and longer duration of preoperative pain were correlated with more severe neck and arm pain after surgery.
Keywords
Introduction
When evaluating the results of anterior cervical decompression and fusion (ACDF), research mostly focuses on an average change in outcome, leaving unrevealed a potential variation between dissimilar patient groups. 1 Group-based trajectory analysis (GBTA) has only been applied by a few studies among patients undergoing cervical spine surgery.2,3 Previous studies have observed pain relief and improved functioning after ACDF in most of the patients. 4 At the same time, smaller groups did not show improvement, or they displayed even worse pain, disability, and quality of life after surgery. 4 One study, employing latent class analysis, has mentioned some social factors, such as ethnicity, poor insurance, lower socioeconomic status, and poor employment, as risks of worse surgery outcome. 5 While there is inconsistency in the literature regarding the impact of obesity on the outcome of ACDF, obese patients may have a higher likelihood of developing perioperative complication. 6 Longer preoperative pain duration more than 2 years has been considered a predictor of worse ACDF outcome.7–9
With certain reservations, some relevant inferences could be made from previous GBTA analyses among patients undergoing different lumbar spinal surgical procedures. While most of the patients have shown pain relief and improved functioning, smaller groups showed worse outcomes.10–14 Among factors associated with worse outcome, younger age, female sex, worse pain before and immediately after surgery, 12 and pain catastrophizing have been reported. 13 In turn, psychological flexibility and postoperative pain acceptance have been suggested as factors predicting better outcome. 13
In general, variability in the trajectories of changes in pain and disability after ACDF across different patient groups is poorly studied. Also, there is only limited evidence concerning factors, which may be associated with worse or better ACDF outcome in different patient groups. Based on previous evidence, it can be hypothesized that differences related to sex, obesity, and preoperative pain duration may affect the trajectories of changes in pain and disability after ACDF. Using these factors as explanatory variables, the GBTA may be able to identify groups of patients, who may benefit the most from surgery, and those, who will probably not improve.4,10,15,16 Identifying groups with dissimilar recovery trajectories may support clinical decision-making by detecting patients with higher risk of developing chronic pain and prolonged disability.17,18 The objective was to identify the clusters of patients with different developmental trajectories of pain and disability after the ACDF, and to detect potential associations between sex, preoperative pain, and obesity and probability to be classified into a group with either better or worse recovering.
Methods
The data were a subset of the FinSpine register limited to patients undergoing cervical surgery of any kind between 21 June 2018 and 17 August 2021 in a university hospital. 19 All patients who had participated in an online survey before the surgery were included. A patient was included if the procedure code was one of the following: NAG40, NAG41, or ABC21 according to the Nordic Classification of Surgical Procedures (NCSP), version 1.15. Re-operations were excluded. The ACDF without fixation (NAG40) was a standard procedure. The ACDF with fixation (NAG41) was essentially the same procedure, except for using a fixating plate. Also, the ACDF with the insertion of interbody fixating implant (ABC21) is technically identical to the ACDF without fixation. The use of anonymous data extracted from the register did not require a formal approval or informed consent as determined by the hospital ethical board.
The patients responded to repeated surveys within 2 months before the surgery (Timepoint 0), 2–4 months after the surgery (Timepoint 1), 11–13 months after the surgery (Timepoint 2); and 23–25 months after the surgery (Timepoint 3). The survey contained questions on demographics, pain, and disability.
Age was defined in full years at the time of surgery. Body mass index (BMI) was self-reported and defined as a body weight divided by a squared height and expressed in kg/m2. The BMI was categorized as < 25 “normal weight,” 25–30 “overweight,” or > 30 kg/m2 “obesity.” The preoperative duration of pain was dichotomized as ⩽ 3 versus > 3 months. Pain intensity was assessed using a visual analogue scale (VAS) from 0 to 100 with 0 indicating no pain and 100 indicating the worst possible pain.
The Neck Disability Index (NDI) is a questionnaire containing 10 items covering disability caused by neck pain. Each item is assessed on a six-level ordinal scale with “0” describing “no limitation” and “5” describing “extreme limitation or an inability to function.” The total score is a percentage calculated as a sum of all item scores divided by 50 (the maximum possible number of points) and multiplied by 100 as follows: “Total score = (∑item scores/50) × 100.” The equation is adjusted when the responses to one or more items were missing. A score of 0% represents the highest possible level of functioning and independence, while a score of 100% represents the lowest level of functioning with total dependency. The NDI score was interpreted as follows: ⩽ 8% “no disability”; 10%–28% “mild disability”; 30%–45% “moderate disability”; 50%–68% “severe disability,” and > 68% “complete disability.” 20
Statistical analysis
The logic behind the present statistical analysis is shown in Fig. 1. The number of clusters and the order of regression were determined by running all available combinations from one to four clusters and from first-order (linear) to third-order (cubic) regression models. The highest possible order (first, second, or third) with a significant p-value less than 0.05 was retained. The goodness-of-fit of a retaining model was confirmed by calculating the Bayesian information criterion (BIC) and the Akaike information criterion (AIC), preferring estimates closest to zero. In addition, the cut-off for the average posterior probability (APP) was set at 0.7 and the cut-off for the smallest possible cluster was set to 10%. Trajectory analysis was repeated separately for the NDI and the severity of neck and arm pain. The goodness-of-fit of retaining models is presented in Table 1. The analyzes were run separately for the NDI, neck pain VAS, and arm pain VAS.
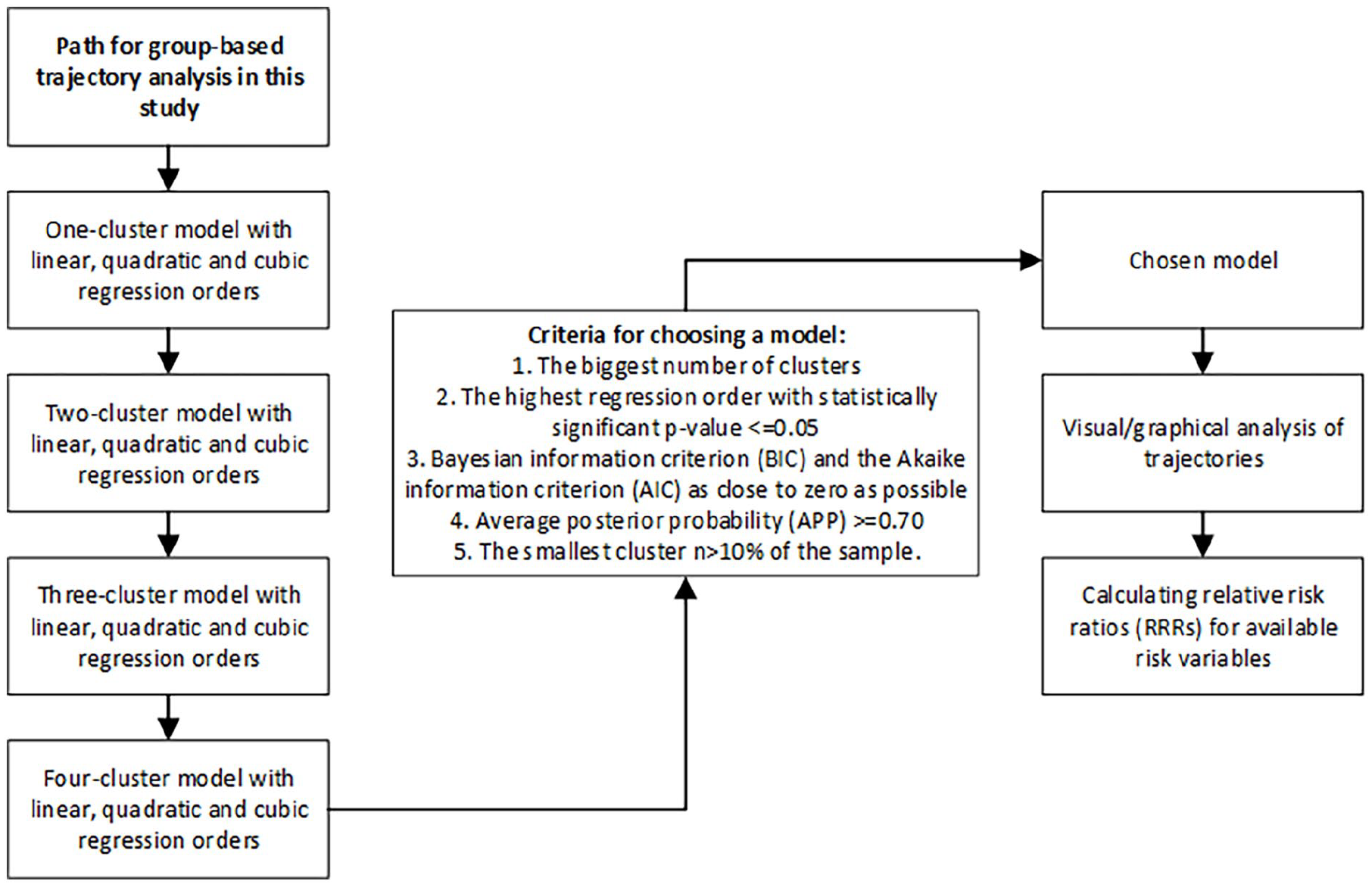
Path for GBTA.
Goodness-of-fit of GBTA models. The chosen models are shown underlined.
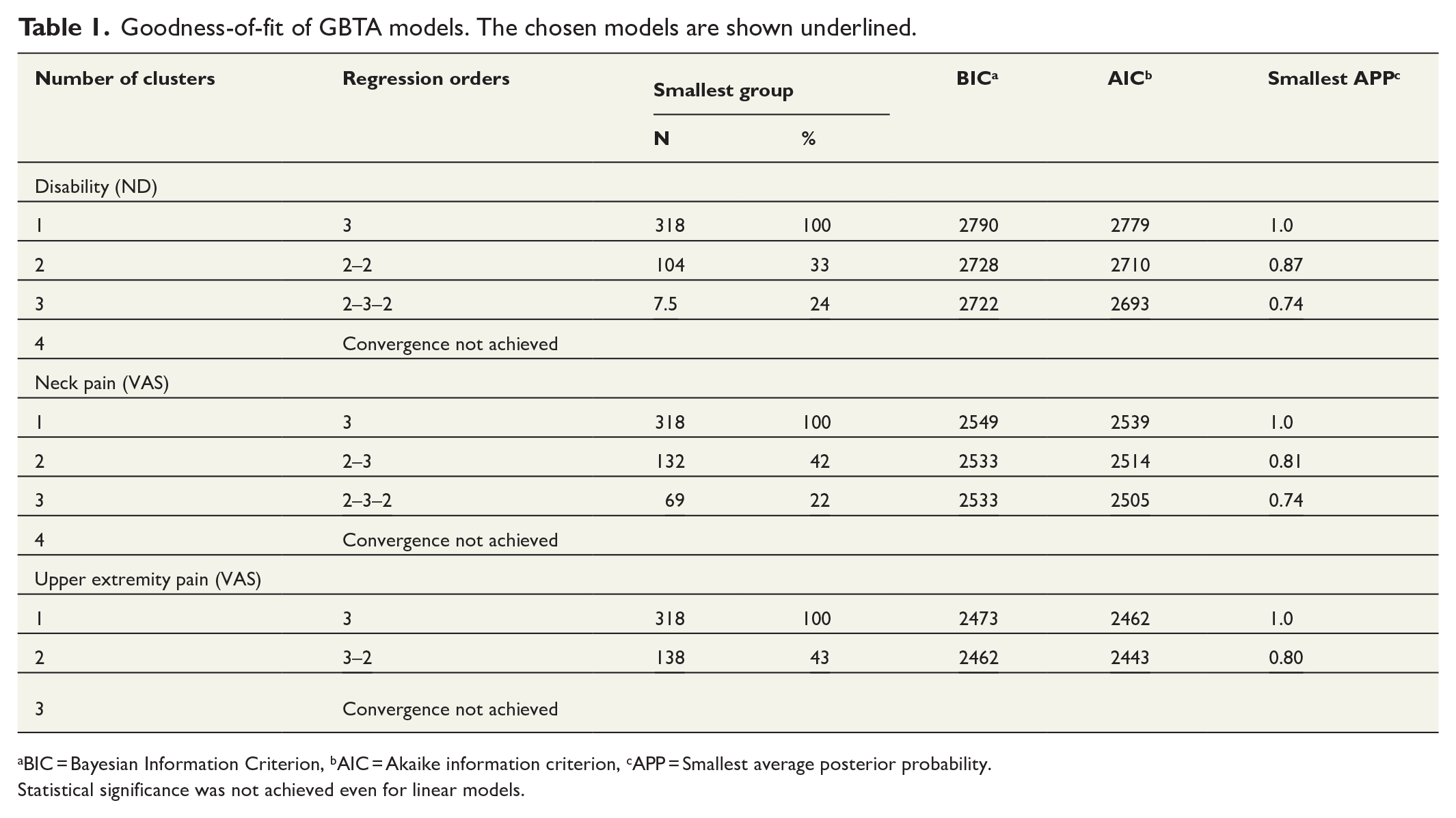
BIC = Bayesian Information Criterion, bAIC = Akaike information criterion, cAPP = Smallest average posterior probability.
Statistical significance was not achieved even for linear models.
For the changes in NDI score and neck pain, three trajectory models were chosen, as the four trajectory models had resulted in the smallest group below a pre-agreed threshold of 10% of the sample size. Respectively, a two-trajectory model has been retained for the changes in arm pain.
After identifying clusters, the probability of group membership was calculated based on sex, the duration of pain before surgery, and BMI. These probabilities were expressed as relative risk ratios (RRRs) along with 95% confidence intervals (95% CI). All the analyses were conducted using Stata/IC Statistical Software: Release 17, College Station (StataCorp LP, TX, USA).
Results
A total of 318 patients completed preoperative surveys. The descriptive characteristics of the sample are shown in Table 2. The mean age was 52.8 (10.3) years, while the BMI was 28.3 (5.7) kg/m2. Of the patients, 253 (84%) had experienced neck pain for more than 3 months. The average NDI score was 44.9% (16.9%) preoperatively. The ACDF without fixation was the most used technique (86%). The most frequent reasons for surgery were “M50 Cervical disc disorders” (43%) and “M47 Spondylosis” (35%), according to the International Classification of Diseases, 10th Edition (ICD-10). NDI scores and pain severity at different timepoints are shown in Supplement 1.
Baseline characteristics of the study population.
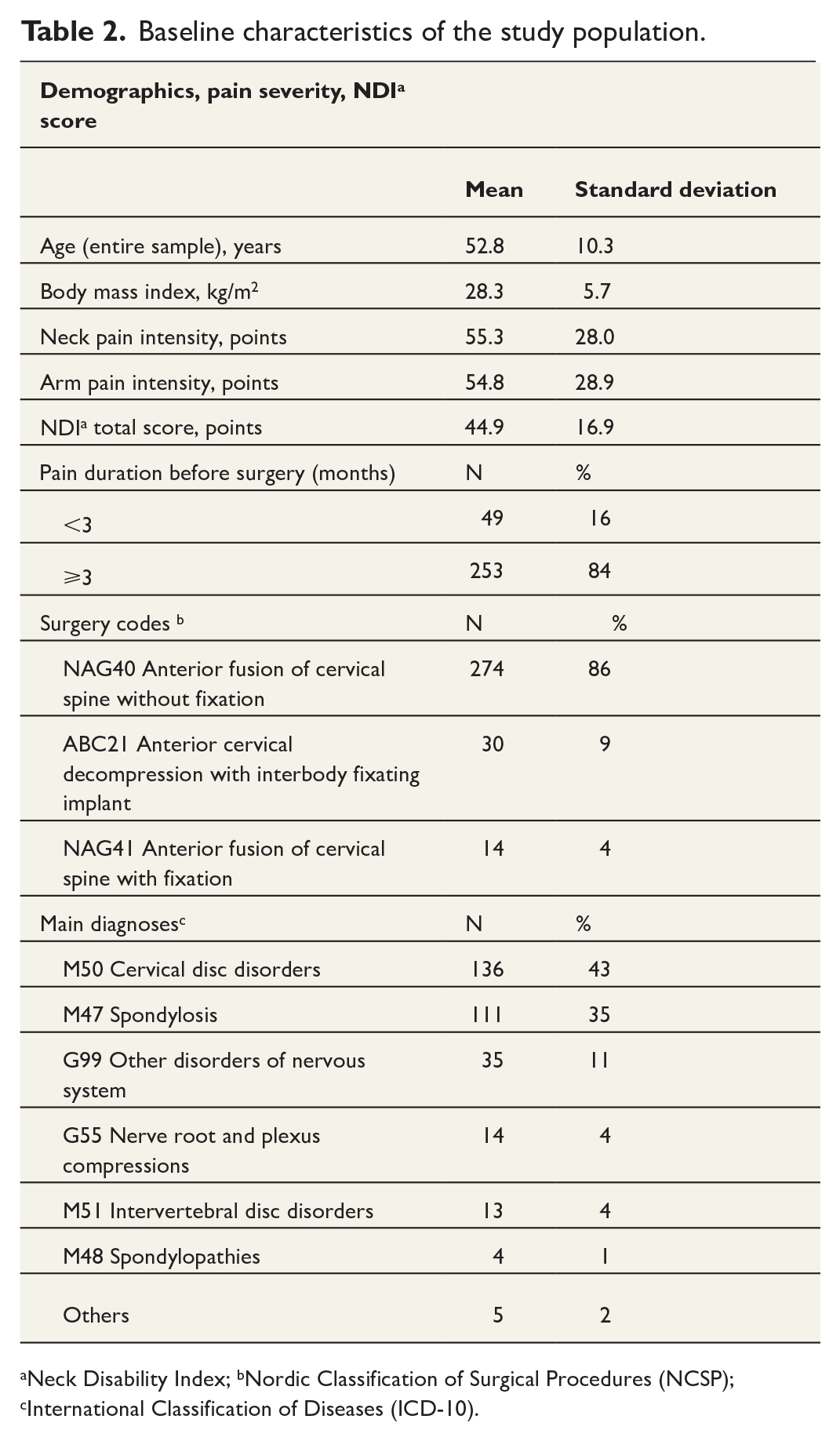
Neck Disability Index; bNordic Classification of Surgical Procedures (NCSP); cInternational Classification of Diseases (ICD-10).
Trajectory groups based on changes in functioning (Fig. 2)
“Steadily good functioning” (24% of sample) In this group, the baseline NDI score of 26.5% decreased to 8.1% during the first year after surgery. At the end of 2-year follow-up, the NDI score slightly grew to 13.2%, still remaining below the baseline level.
2. “Improved functioning” (49% of sample) During the first year after surgery, the high baseline NDI score of 48.0% decreased to 20.5%. At the end of 2-year follow-up, the NDI score raised a little up to 24.2% remaining, however, two-time lower than the baseline level.
3. “Steadily poor functioning” (27% of sample)
The NDI score remained nearly unchanged through the entire 2-year follow-up: from 56.3% at baseline to 49.3% after 1 year, and 53.2% after 2 years.
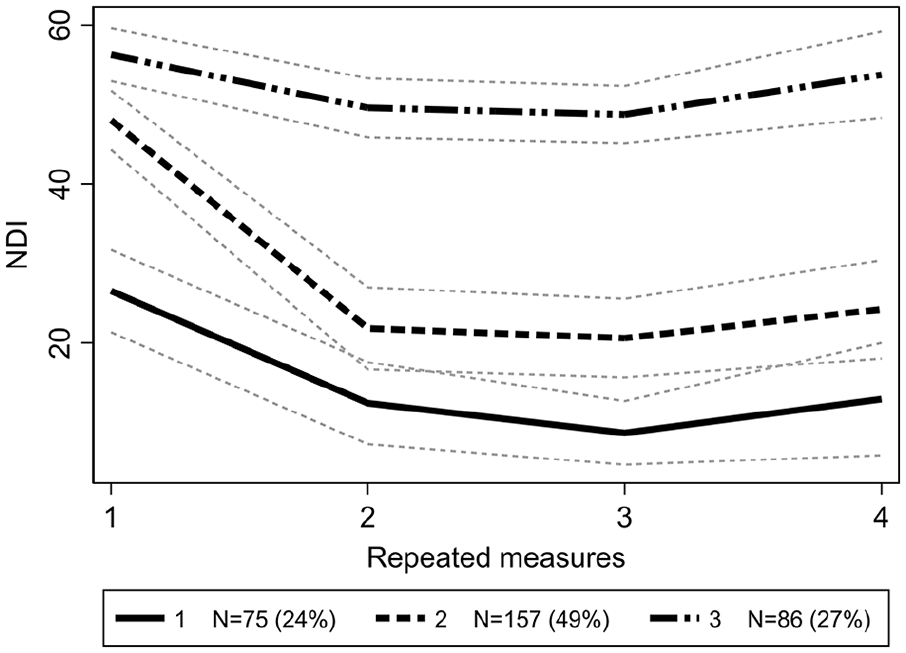
Trajectories of changes in the NDI score.
Trajectory groups based on changes in neck pain severity (Fig. 3)
“Worsened neck pain” (22% of sample) During the first year, no substantial change in pain level was seen—pain was mild before and after the surgery, 21.5 and 19.5 points, respectively. However, at the end of a 2-year follow-up, the baseline level was more than doubled showing a significant increase in pain level up to 49.7 points.
2. “Relieved neck pain” (32% of sample) Neck pain severity declined from severe 64.8 down to 12.1 points after 1 year. This improvement endured through the second year as well, resulting in mild 12.6 points at the end of 2-year follow-up.
3. “Steadily severe neck pain” (46% of sample) Through the entire 2-year follow-up, neck pain level varied only slightly around severe 60–70 points.
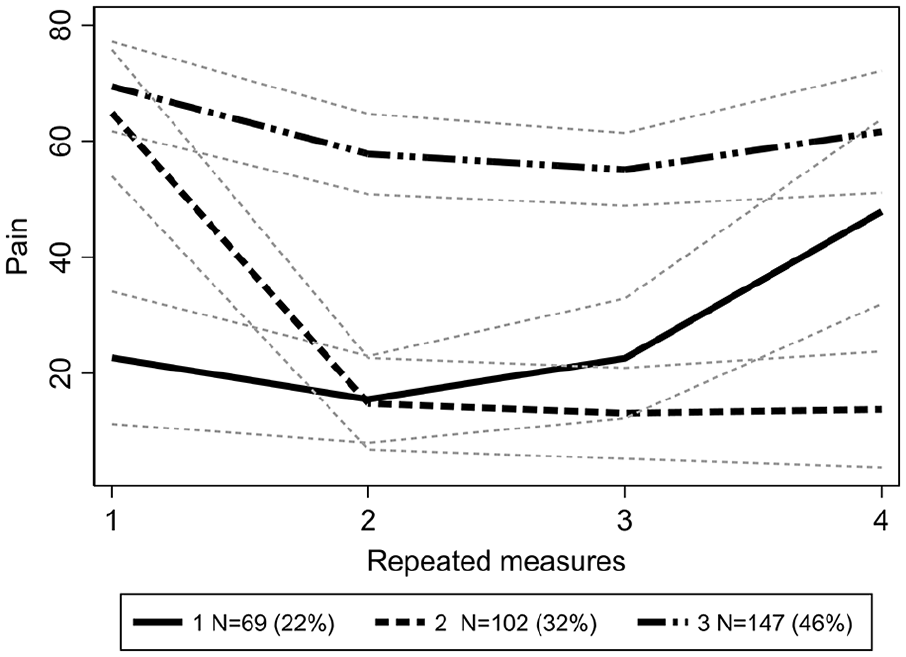
Trajectories of changes in neck pain.
Changes in arm pain severity (Fig. 4)
“Decreased arm pain” (57% of sample) Moderate pain of 40.4 points at the baseline declined down to 15.4 points 1 year after surgery, slightly increasing up to 19.6 points at the end of 2-year follow-up.
2. “Severe arm pain with only short-term relief” (43% of sample) At the baseline, arm pain severity was 70.6 points. After 1 year, pain decreased down to 47.9 points, but increased again up to 61.0 points after 2 years.
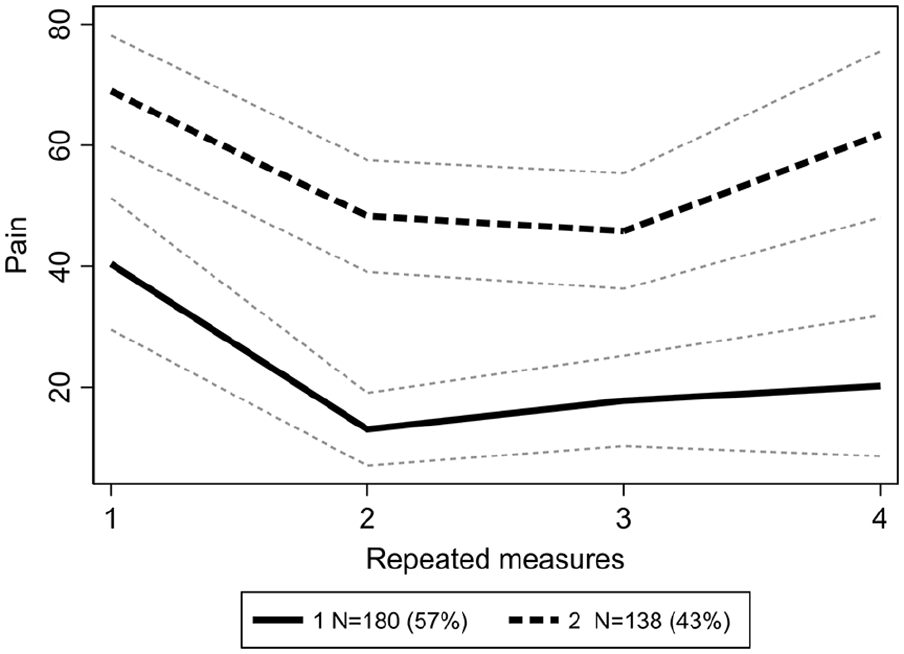
Trajectories of changes in arm pain.
Association between demographic factors and trajectory groups
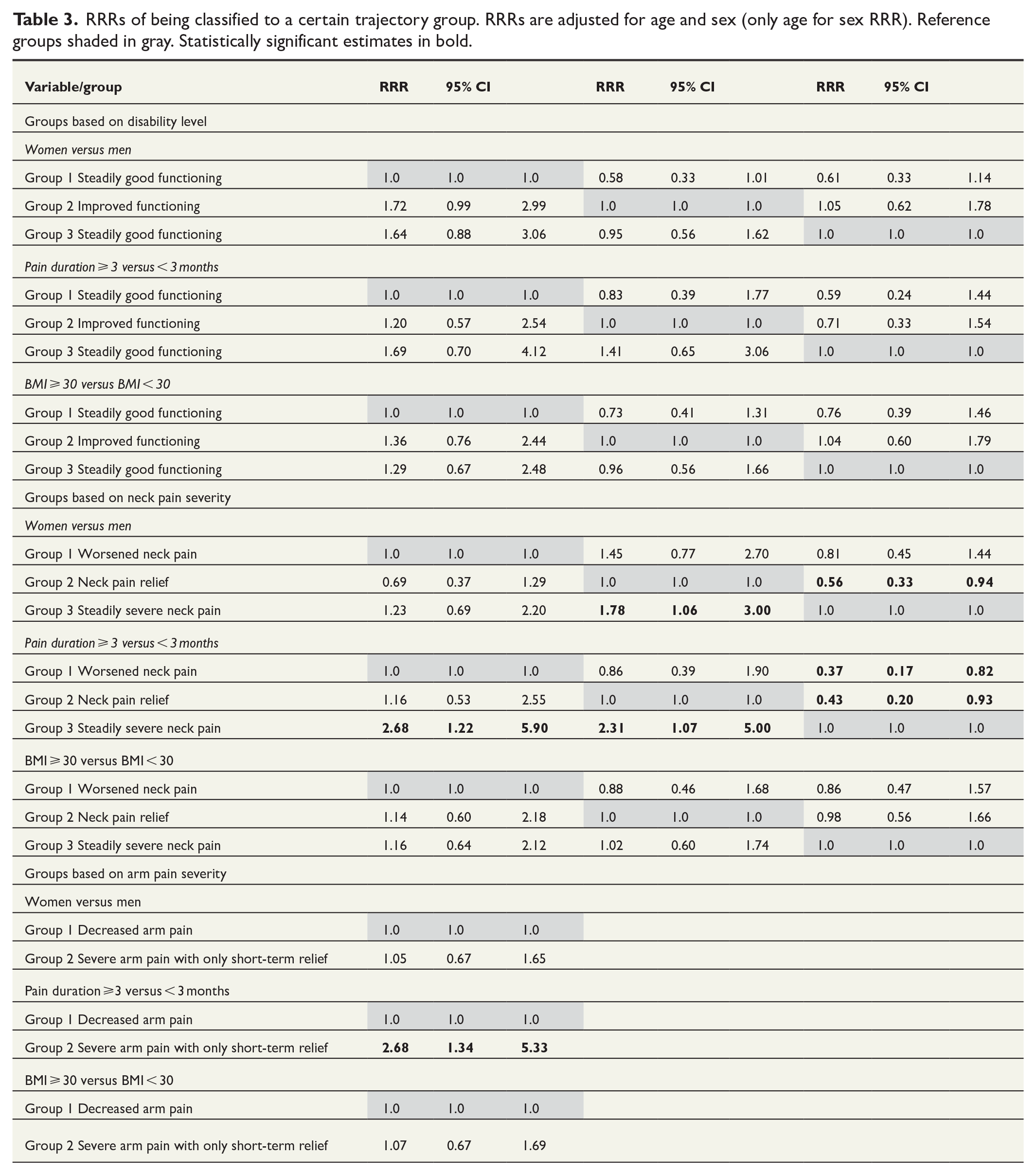
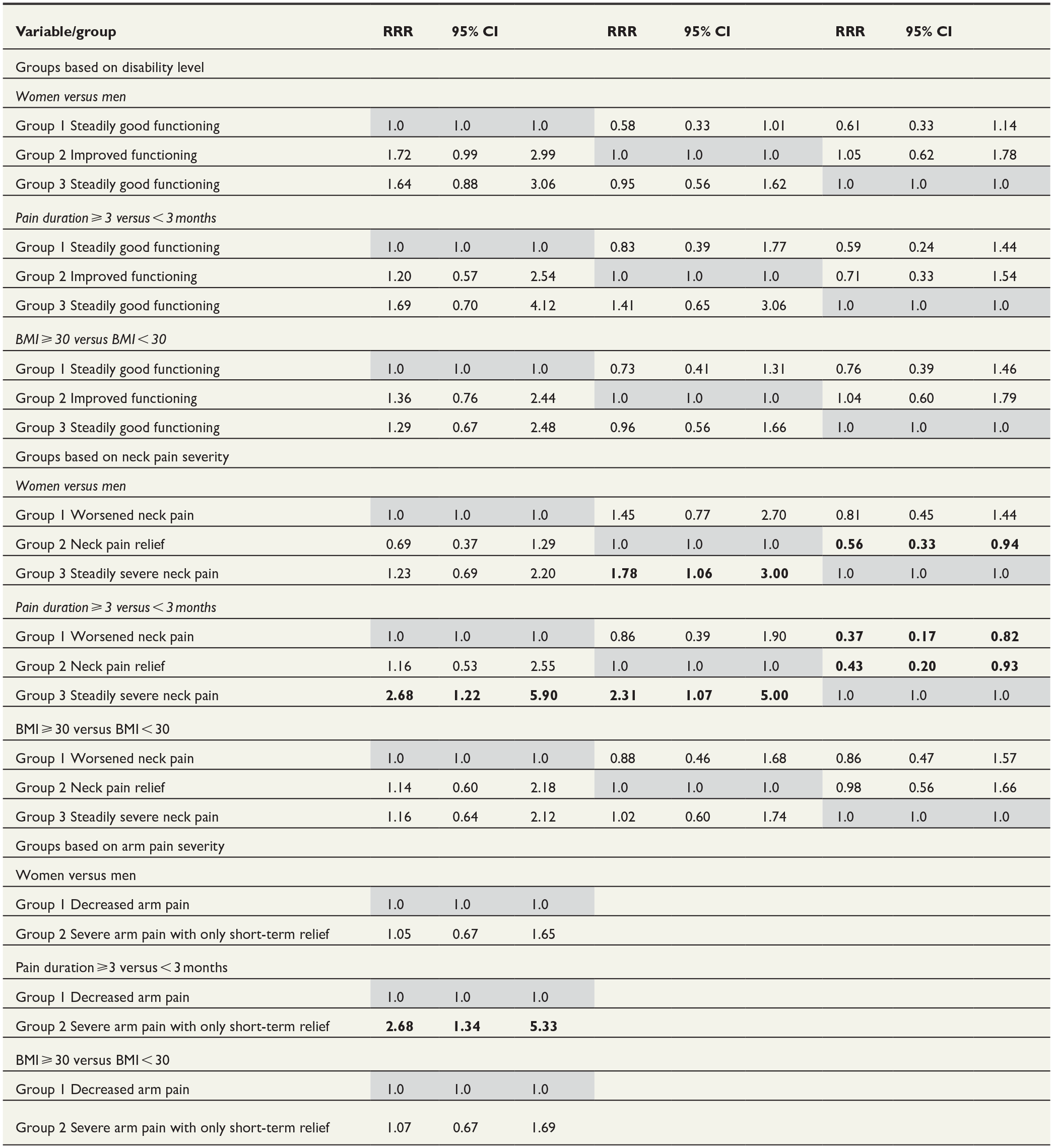
Concerning disability level, no statistically significant associations were found between sex, preoperative pain duration, or BMI and probability to be classified into a particular trajectory group (Table 3). Regarding neck pain, female sex increased the probability to be classified into group “Steadily severe pain” compared to group “Neck pain relief,” which included patients who have experienced pain relief (RRR 1.78 (95% CI 1.06 to 3.00)). Longer history of preoperative pain was associated with higher probability to be classified into group “Steadily severe pain” than in any other two groups, RRR 2.68 (95% CI 1.22 to 5.90) and RRR 2.31 (95% CI 1.07 to 5.0), respectively. In the case of clusters formed based on arm pain severity, longer preoperative pain increased the probability to be classified into group “Severe arm pain with only short-term relief,” RRR 2.68 (95% CI 1.34 to 5.33). The BMI did not significantly affect any of probabilities. Supplements 2 and 3 provide a closer look on disability and neck and arm pain at baseline by sex and by preoperative neck pain duration in different trajectory groups.
RRRs of being classified to a certain trajectory group. RRRs are adjusted for age and sex (only age for sex RRR). Reference groups shaded in gray. Statistically significant estimates in bold.
Discussion
This register-based retrospective study among 318 patients treated with the ACDF investigated the trajectories of changes in severity of disability and pain after surgery. Three trajectory groups were identified based on the changes in disability level: “Steadily good functioning,” “Improved functioning,” and “Steadily poor functioning.” Three groups were identified based on the changes in neck pain severity: “Worsened pain,” “Decreased neck pain,” and “Steadily severe pain.” Two trajectory groups were identified based on the changes in arm pain severity: “Decreased arm pain” and “Severe arm pain with only short-term relief.” Regarding the changes in disability severity, no associations were found between sex, preoperative pain duration, or body weight and probability to be classified into a particular trajectory group. Female sex and longer history of preoperative pain increased the probability to be classified into a group with steadily severe neck pain. Longer history of preoperative pain also increased the probability to be classified into group with severe arm pain with only short-term pain relief.
The generalizability of the results might be affected by several issues. This study was conducted in a single university clinic with a small number of surgeons. While to the best of our knowledge most of the patients responded to a preoperative survey, the exact data on missing responses were unavailable. The sample size might not be big enough to reveal all the existing trends employing the GBTA. There were heterogeneous reasons for a surgery, which might emphasize the negative effect of small sample size. Only a few potential explanatory variables were available. Thus, it is possible, and even probable, that some important factors (e.g. educational level, occupation, depression, etc.) affecting the developmental curves have remained unrecognized. For example, Phan et al. 21 have suggested an inverse relationship between preoperative depression and the functional outcome of the ACDF. Regarding the choice of a 3-month cut-off for preoperative pain duration, given that most patients (84%) were operated on later, there could be a bias toward operating on those with worse symptoms within 3 months.
Men might have significantly higher probability to be referred for surgery than women. 22 However, previous evidence suggests that even though women may suffer worse postoperative pain and experience greater disability than men do, satisfaction with outcome is the same for both sexes.23–25 Also, among patients with back pain, Lim et al. 26 have found that while women might have worse preoperative disability, both sexes improved postoperatively during a 5-year follow-up. Overall, previous knowledge on the impact of sex on postsurgical outcomes of the ACDF may be compromised by a recognized publication bias—insignificant findings are often remained unpublished. 23 In our study, no sex-related differences were found in postoperative change in the severity of disability. In turn, female sex was associated with steadily severe postoperative neck pain.
In a 6-year follow-up, Peolsson and Peolsson have found that male sex, milder disability, and especially preoperative pain intensity have been predictive for the outcome of ACDF measured using the NDI. 27 This study observed the same connection between milder preoperative and milder postoperative disability (group “Steadily good functioning”).
Peolsson and Peolsson have stated that the duration of symptoms has seemed to have minor importance for the clinical outcome, maybe due to the inclusion criteria of at least 6-month duration of symptoms before ACDF. Tarazona et al. 7 have reported that the preoperative duration of symptoms greater than 2 years might result in significantly worse postoperative functioning and pain. It has to be taken into account that the duration of preoperative pain may often be determined by other motives than clinical reasons, for example, by waiting for radiological examinations or surgery. 25 This might partially explain why the duration of preoperative pain has not been consistently found to have a negative effect on the outcome. In this study, longer history of preoperative neck and arm pain increased the probability to be classified into trajectory groups of “Steadily severe neck pain” and “Severe arm pain with only short-term relief.”
In this study, BMI was not predictive for probability to be classified in any of the identified trajectory clusters. Previous research has suggested that obesity might not limit the benefits of surgical intervention, but instead increase the risk of postoperative complications.6,24
Further research may confirm the present results using larger samples, longer follow-ups and including other potentially relevant explanatory variables into trajectory analysis models. Also, respective trajectory analysis may focus on samples with more specifically defined clinical reasons for the ACDF.
After the ACDF, several groups demonstrated dissimilar developmental trajectories of pain and disability. While sex, preoperative pain duration, and body weight were not associated with differences in improvement in disability level, female sex and longer duration of preoperative pain were correlated with more severe neck and arm pain after surgery.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969241241969 – Supplemental material for Disability and pain after anterior cervical decompression and fusion: A group-based trajectory analysis
Supplemental material, sj-docx-1-sjs-10.1177_14574969241241969 for Disability and pain after anterior cervical decompression and fusion: A group-based trajectory analysis by Sara S. Widbom-Kolhanen, Katri I. Pernaa, Roosa E. Lintuaho, Anna Kotkansalo and Mikhail Saltychev in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-2-sjs-10.1177_14574969241241969 – Supplemental material for Disability and pain after anterior cervical decompression and fusion: A group-based trajectory analysis
Supplemental material, sj-docx-2-sjs-10.1177_14574969241241969 for Disability and pain after anterior cervical decompression and fusion: A group-based trajectory analysis by Sara S. Widbom-Kolhanen, Katri I. Pernaa, Roosa E. Lintuaho, Anna Kotkansalo and Mikhail Saltychev in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-3-sjs-10.1177_14574969241241969 – Supplemental material for Disability and pain after anterior cervical decompression and fusion: A group-based trajectory analysis
Supplemental material, sj-docx-3-sjs-10.1177_14574969241241969 for Disability and pain after anterior cervical decompression and fusion: A group-based trajectory analysis by Sara S. Widbom-Kolhanen, Katri I. Pernaa, Roosa E. Lintuaho, Anna Kotkansalo and Mikhail Saltychev in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
None declared.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.