
Abstract
Background and objective:
Non-obstetric surgery is fairly common in pregnant women. We performed a systematic review to update data on non-obstetric surgery in pregnant women. The aim of this review was to evaluate the effects of non-obstetric surgery during pregnancy on pregnancy, fetal and maternal outcomes.
Methods:
A systematic literature search of MEDLINE and Scopus was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The search span was from January 2000 to November 2022. Thirty-six studies matched the inclusion criteria, and 24 publications were identified through reference mining; 60 studies were included in this review. Outcome measures were miscarriage, stillbirth, preterm birth, low birth weight, low Apgar score, and infant and maternal morbidity and mortality rates.
Results:
We obtained data for 80,205 women who underwent non-obstetric surgery and data for 16,655,486 women who did not undergo surgery during pregnancy. Prevalence of non-obstetric surgery was between 0.23% and 0.74% (median 0.37%). Appendectomy was the most common procedure with median prevalence of 0.10%. Near half (43%) of the procedures were performed during the second trimester, 32% during the first trimester, and 25% during the third trimester. Half of surgeries were scheduled, and half were emergent. Laparoscopic and open techniques were used equally for abdominal cavity. Women who underwent non-obstetric surgery during pregnancy had increased rate of stillbirth (odds ratio (OR) 2.0) and preterm birth (OR 2.1) compared to women without surgery. Surgery during pregnancy did not increase rate of miscarriage (OR 1.1), low 5 min Apgar scores (OR 1.1), the fetus being small for gestational age (OR 1.1) or congenital anomalies (OR 1.0).
Conclusions:
The prevalence of non-obstetric surgery has decreased during last decades, but still two out of 1000 pregnant women have scheduled surgery during pregnancy. Surgery during pregnancy increases the risk of stillbirth, and preterm birth. For abdominal cavity surgery, both laparoscopic and open approaches are feasible.
Keywords
Context and Relevance
Previous studies demonstrate that non-obstetric surgery is common in pregnant women with the prevalence of 0.5%–2%. Emergent situations may require urgent surgical treatment, but pregnant women undergo elective surgeries also. Surgery is associated to increased risk of adverse birth outcomes, such as miscarriage, stillbirth, preterm birth, low birth weight, and a low Apgar score.
Our study indicates that the prevalence of non-obstetric surgery has decreased in recent years, but elective surgery is still common in pregnant women. Surgery during pregnancy increases the risk of stillbirth, preterm birth, and congenital anomalies. Fetal and maternal safety of non-obstetric surgery has, however, increased during the last two decades and surgical intervention should not be postponed in emergent conditions requiring surgery.
Introduction
Older data indicate that non-obstetric surgery is performed in 0.5%-2% of all pregnancies and that the most common conditions requiring surgical intervention during pregnancy are appendicitis, cholecystitis, gynecological disorders, and traumas. 1 It has been proposed that scheduled surgery should be postponed until after pregnancy,2,3 but both scheduled and emergent surgeries are fairly commonly performed in pregnant women. Emergent situations, such as acute appendicitis and ovarian torsion, often require urgent intervention, whereas the timing of scheduled surgery in pregnant patients must be carefully evaluated.2 If scheduled surgery is required during pregnancy, the second trimester after organogenesis is considered the most appropriate time.1,3
Non-obstetric surgery during pregnancy increases the risk of adverse birth outcomes, such as miscarriage, stillbirth, preterm birth, low birth weight, and a low Apgar score.1,4,5 Surgical disease and surgery predispose both pregnant woman and fetuses to several risks, such as surgical and oxidative stress, anesthetics, analgesics, and postoperative pain, which may also affect the course of pregnancy. Longer anesthesia duration in pregnancy may induce fetal neuronal injury and increase the risk of impaired learning and memory during childhood and adolescence.6 The timing of the surgery may affect the risk of adverse birth outcomes, as surgical procedures performed in the first and third trimesters are associated with a higher risk of preterm birth, birth weight under 1750 g, and low Apgar scores.3,7 However, the surgical condition itself can be a risk for the pregnant woman, the pregnancy outcome, and the fetus if left untreated. Therefore, surgical intervention should not be postponed if symptoms do not improve with conservative measures or if conservative measures are not available.1–4
In this study, our aim was to update data on non-obstetric surgery in pregnant women. During the last two decades, the diagnostic accuracy of surgical conditions has improved, mini-invasive surgical techniques have become more common, perioperative fetal monitoring and maternal–fetal care have improved, and updated guidelines on non-obstetric surgery during pregnancy have been published.2,3 Our hypothesis was that the prevalence of non-obstetric surgery has decreased, and the safety of surgery has increased during the last two decades compared to previously. In this updated systematic review, we evaluated the effects of non-obstetric surgery during pregnancy on pregnancy and fetal and maternal outcomes. In addition, the prevalence of non-obstetric surgery, the proportions of emergent and scheduled surgery, and the proportions of laparoscopic and open approaches in non-obstetric surgery in pregnant women were quantified.
Methods
This systematic review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.8
Search strategy
A systematic literature search of MEDLINE (PubMed) and Scopus was conducted in January 2020 and updated in November 2022. The search strategy combined Medical Subject Heading (MeSH) terms and keywords. The following terms were used in combination to search for relevant studies: pregnancy outcome, preterm delivery, birth outcome, spontaneous abortion, miscarriage, live birth, stillbirth, non-obstetric, laparoscopic, surgical, surgery, and surgical procedures. The initial search was restricted to English-language articles published between January 1989 and November 2022 and produced 185 relevant results. The literature search was performed under the guidance of an information retrieval and information management professional. The search strategy is demonstrated in Appendix 1.
Study selection
Two independent reviewers (AH and HK) participated in the study selection and data extraction, and any disagreements were resolved through dialogue. In the first phase, article titles were screened for relevance, and the resulting set was reduced from 185 articles to 97. In the second phase, the abstracts were reviewed, and 51 articles were selected for further evaluation. After excluding double publications, overlapping studies, and irrelevant publications, and restricting selection to articles published between January 2000 and November 2022 to have the most up-to-date data, a total of 36 studies matched the inclusion criteria. An additional 24 citations were identified through reference mining. Ultimately, 60 studies were included in the review (Figure 1).
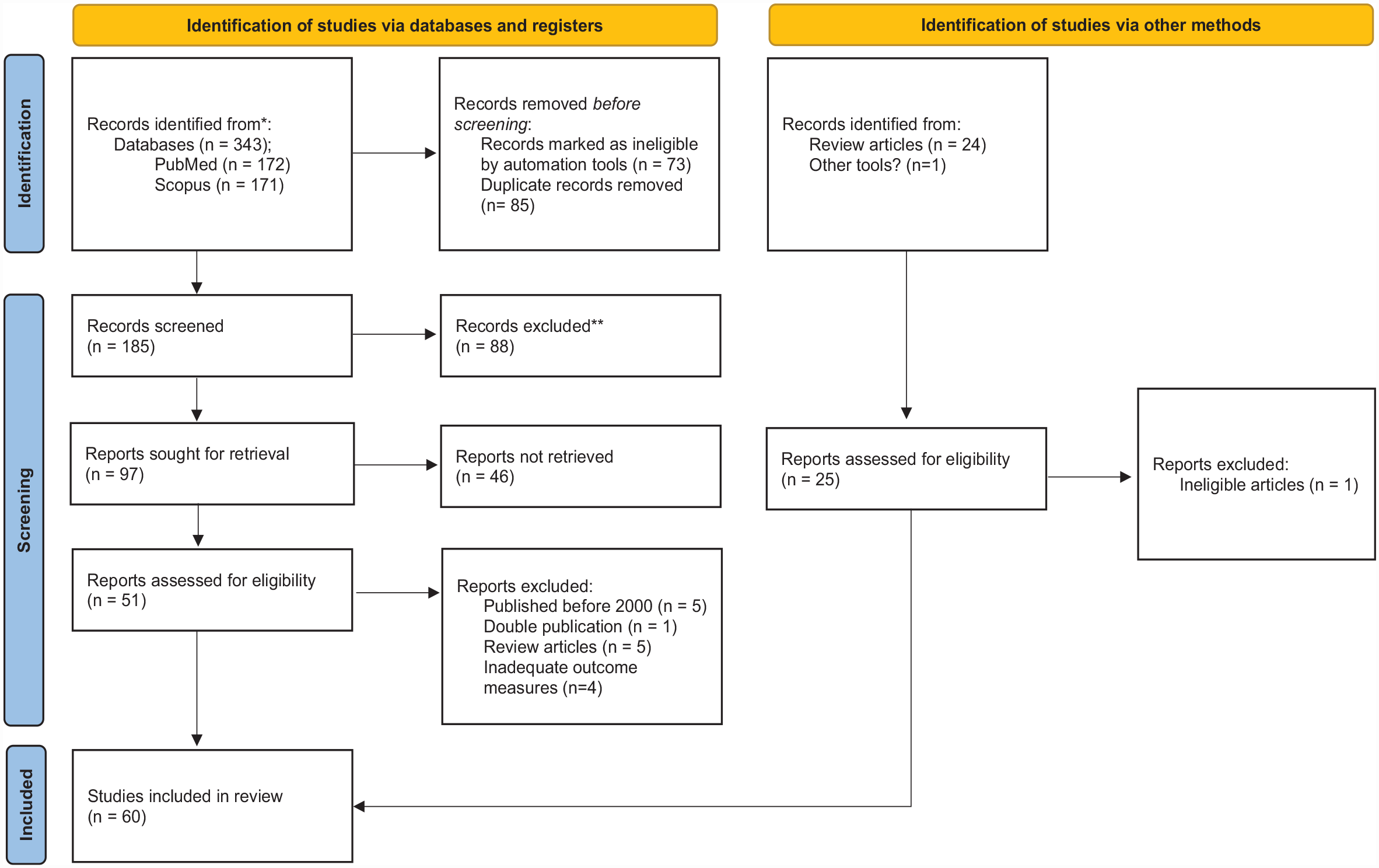
PRISMA flow sheet describing the study selection process.
Eligibility criteria
Studies concerning non-obstetric surgery during pregnancy and its effects on the course of pregnancy with primary outcome measures of miscarriage, stillbirth, preterm birth, low birth weight, and an Apgar score less than 7 at 5 min were included in the review. The included studies were retrospective cohort studies, cross-sectional studies, and case series studies. We excluded studies published before 2000.
Data extraction and analysis
The extracted information is shown in Table 2 and includes author(s), year of publication, study design, participant information, study period, surgical intervention, outcome measures (miscarriage, stillbirth, preterm birth, low birth weight, Apgar score < 7, and infant and maternal morbidity and mortality), and the prevalence of non-obstetric surgery.
Odds ratios (ORs) with a 95% confidence interval (CI) were calculated to determine whether non-obstetric surgery was a risk for an adverse outcome of pregnancy and to estimate the magnitude of risk. Associations between categorical variables were tested using a chi-square test, and the Pearson correlation coefficient was calculated to measure the degree of association between the time of publication, sample size, and the proportion of laparoscopic procedures. A p < 0.05 was considered statistically significant.
Quality appraisal
A quality assessment was independently performed by two researchers (AH and HK). In case of disagreement, consensus was reached through dialogue. The quality of the reports was assessed according to the method described by Murad et al. 9 in 2018, which included examining patient selection, adequate exposure and outcome ascertainment, causality, sufficient follow-up, adequate reporting, and hence the possibility of replicating the study.
Results
We gathered the data of 80,205 women who underwent non-obstetric surgery during pregnancy from 60 studies and of 16,655,486 women who had no surgery during pregnancy from 23 studies. The studies included are listed in Table 1.
The Quality assessment of the included studies according to Murad et al.9 Green color indicates sufficient quality and red color insufficient quality.
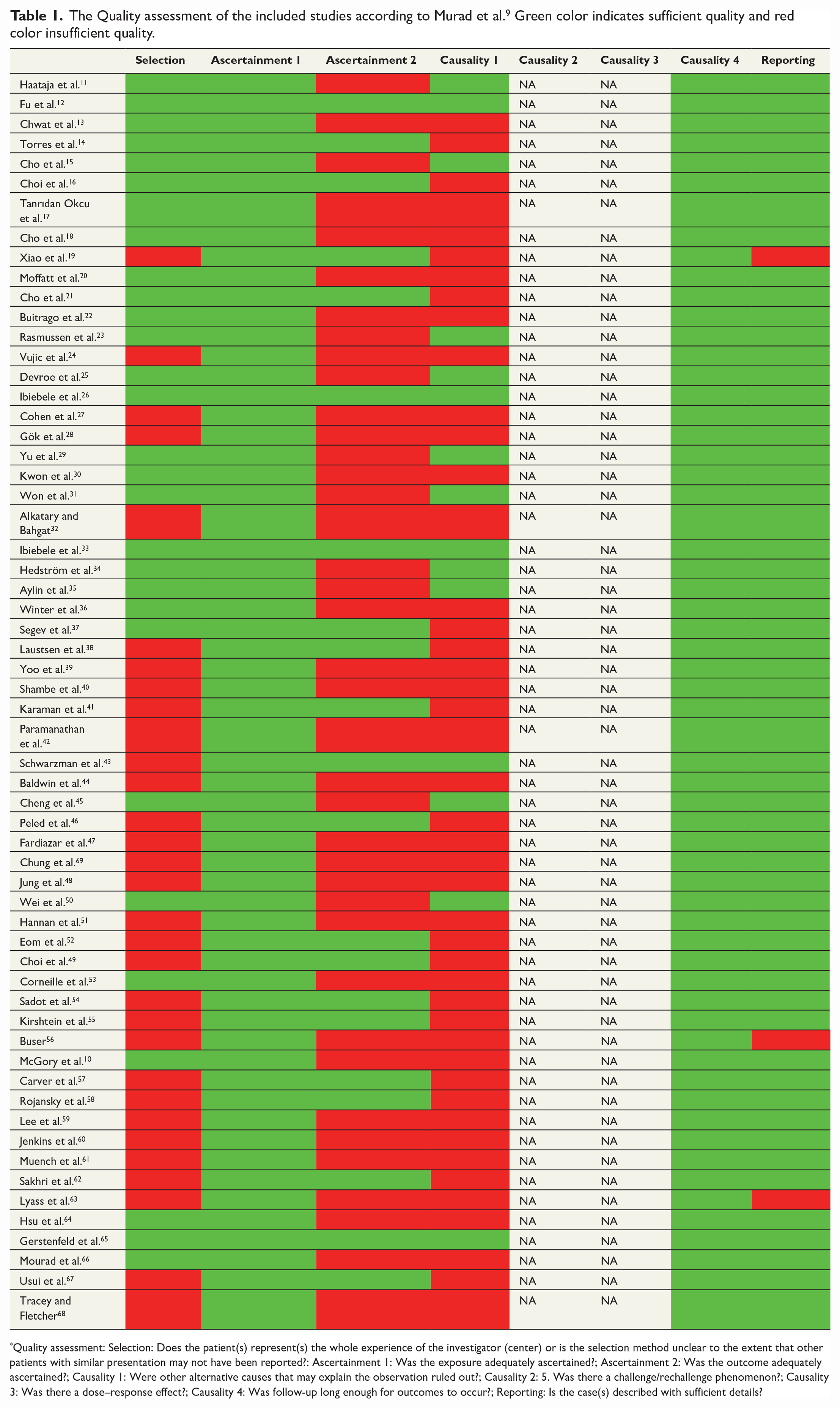
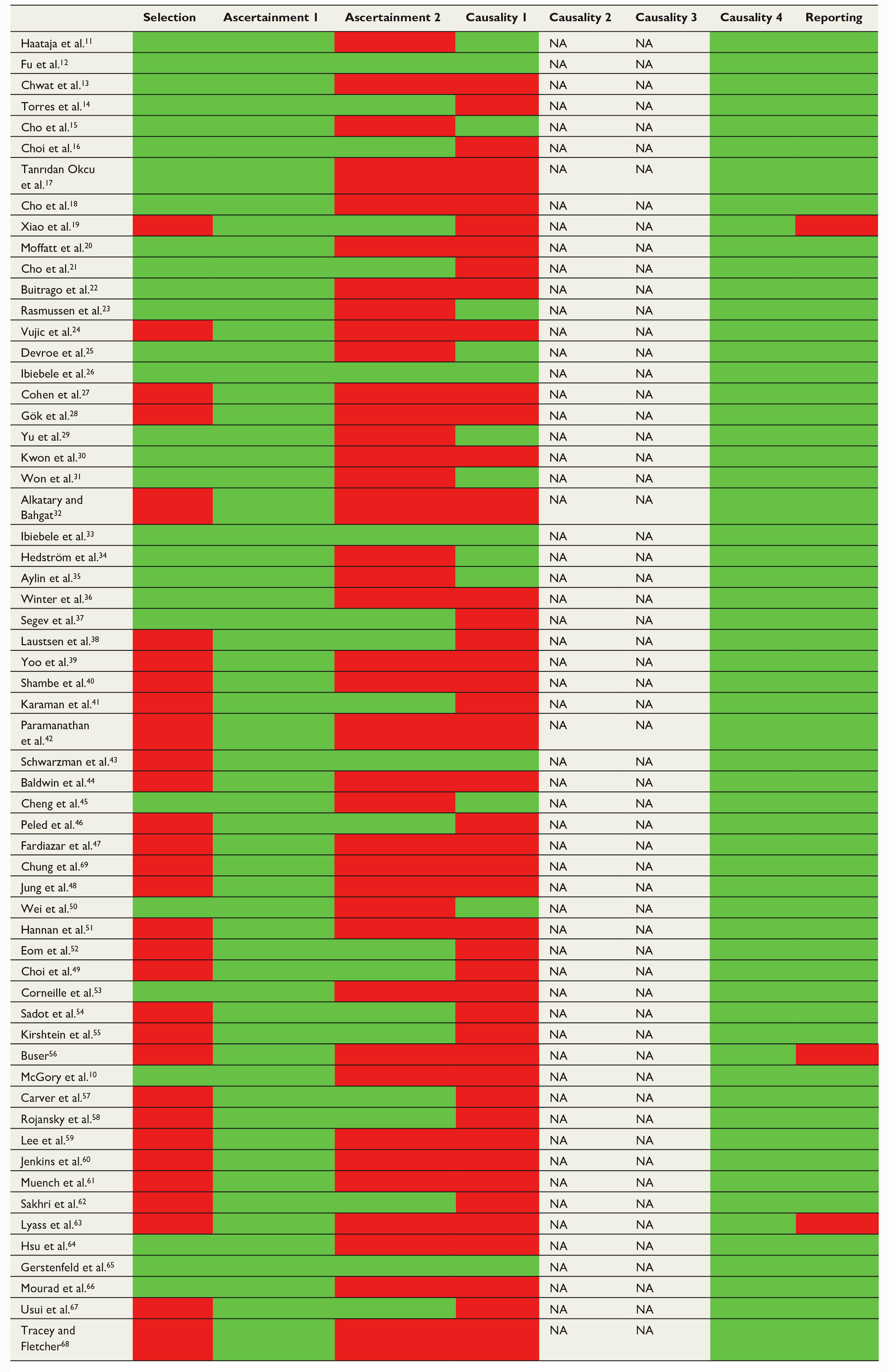
Quality assessment: Selection: Does the patient(s) represent(s) the whole experience of the investigator (center) or is the selection method unclear to the extent that other patients with similar presentation may not have been reported?: Ascertainment 1: Was the exposure adequately ascertained?; Ascertainment 2: Was the outcome adequately ascertained?; Causality 1: Were other alternative causes that may explain the observation ruled out?; Causality 2: 5. Was there a challenge/rechallenge phenomenon?; Causality 3: Was there a dose–response effect?; Causality 4: Was follow-up long enough for outcomes to occur?; Reporting: Is the case(s) described with sufficient details?
Fourteen studies reported population-based data,10–12,15,22,23,26,29,31,33,35,42,45,50 three studies reported multicenter data36,39,60 and 43 studies reported single-center data,13,14,16–21,24,25,27,28,30,32,34,37,38,40,41,43,44,46–49,51–59,61–69 and all, expect one small prospective single-center study on 22 women,63 were retrospective.
The prevalence of non-obstetric surgery was between 0.31% and 0.73% (median 0.39%).11,12,22,23,25,29,35,60
There was broad variation in the quality of the studies, since the selection method was unclear in many studies and some publications lacked precise outcome data and control group for the study population (Table 2).
Description of included studies.

aRR: adjusted risk ratio; ARDS: adult respiratory distress syndrome; BW: birth weight; CI: confidence interval; CNS: central nervous system; EENT: eye, ear, nose and throat; ERCP: endoscopic retrograde cholangiopancreatography; FESS: functional endoscopic sinus surgery; GA: gestational age; GW: gestational week; HR: hazard ratio; LS: laparoscopic surgery; LBW: low birth weight; MC: miscarriage; OR: odds ratio; PB: premature birth; RR: risk ratio; SGA: small for gestational age.
Description of the studies according to the type of surgery
Appendectomy
Appendectomy is one of the most common surgeries during pregnancy, and 31 studies evaluated pregnancy outcomes in women who underwent this procedure.10, 13, 17, 18 22, 26, 28, 31,32,36-39, 41, 45, 46,48-55, 57, 62–66, 68, 69
There were data on 22,987 pregnant women who had an appendectomy during pregnancy. The median prevalence of appendectomies was 0.10%, but there was over a 10-fold difference, 0.03%-0.42%, between the studies (n = 15,430,217). Based on data on 5754 women, 40% of appendectomies were performed in the first, 42% in the second, and 18% in the third trimester (p < 0.001, chi-square test). When the surgical approach was described (n = 14,373), the laparoscopic technique was used in 39% of the procedures. Laparoscopy was used more commonly in the first (64% of cases) and the second trimester (47% of cases) but less frequently in the third trimester (16% of cases) (p < 0.001). The conversion rate in laparoscopic procedures (n = 332) was 6%.
Cholecystectomy
Cholecystectomy is a common gastrointestinal surgery during pregnancy. Pregnancy outcomes were evaluated in four retrospective studies11,21,33,34 and in three laparoscopic feasibility studies.42,53,61 The median prevalence of cholecystectomy in 1891 women was 0.02% (range between 0.01% and 0.03%, (n = 8,988,320). There was one outlier; in the study by Buser, 56 the prevalence of cholecystectomy during pregnancy was 50 times higher at 0.97%. Based on data on 255 women, 41% of cholecystectomies were performed in the first, 49% in the second, and 10% in the third trimester (p = 0.005). When the surgical approach was described (n = 83), the laparoscopic technique was used in 89% of the procedures. Laparoscopy was used in the majority (86%-87%) of the cases in the first and the second trimesters, and in 60% of the cases in the third trimester (p = 0.142). The conversion rate in the laparoscopic procedures (n = 59) was relatively high, 14%.
Abdominal surgery in general
There were data for 8,934,684 pregnant women with 15,084 non-obstetric abdominal surgeries in general in 13 retrospective studies (prevalence 0.28%; range 0.19%-1.3%).11,16,23,24,27,30,35,40,47,53,56,58,65 The most common procedures were appendectomies, laparotomies, cholecystectomies, and anal and perianal surgeries. When it was described (n = 285), 80% of procedures were emergent, and the laparoscopic technique was used in 66% of procedures. Based on data for 7020 women, 37% procedures were performed in the first, 40% in the second, and 23% in the third trimester (p < 0.001).
Non-obstetric gynecological surgery
Five studies evaluated pregnancy outcomes after non-obstetric gynecological surgery.11,15,21,59,67 There were data for 4,452,453 pregnant women with 4,281 non-obstetric gynecologic surgery (prevalence 0.08%). In a study by Cho et al., 15 laparoscopy was used in 44% of cases. In a study by Haataja et al., 11 32% of surgeries were performed in the first, 40% trimester, 40% in the second, and 28% in the third trimester (p < 0.001).
Trauma and orthopedic surgery
Ten studies reported data on trauma and orthopedic surgery.11,16,20,21,25,29,35,40,44,60 Based on data for 7,792,335 pregnant women, the prevalence of trauma surgery was 0.07%. Of note, the proportion of scheduled procedures was high; in the Haataja et al. 11 study 47% of the procedures were elective. Contrary to other types of surgeries that are commonly performed under general anesthesia, regional anesthesia was commonly used in trauma and orthopedic surgery cases. For example, in the Devroe et al. 25 study two-thirds of the cases were performed under regional anesthesia.
Non-obstetric surgery in general
Pregnancy outcomes after surgeries falling under different specialties were evaluated in 10 retrospective studies,11,12,16,21,25,29,35,43,44,60 There were data on 57,949 pregnancies where non-obstetric surgery was performed (prevalence 0.4%). Half of the procedures (52%) were scheduled, and half were emergency procedures (48%). In the first trimester, two-thirds (62%) of the procedures were scheduled, in the second trimester 42%, and in the third trimester one third (33%) were scheduled procedures (p < 0.001). The most common types of surgical procedures were gastrointestinal (42%) and gynecological (20%), followed by trauma/orthopedic (12%), urological (7%), plastic surgery (4%), and neurosurgery (2%). The laparoscopic technique was used in 65% of intra-abdominal procedures, in 83% cases in the first, 38% in the second trimester, and 29% in the third trimester (p < 0.001).
Laparoscopic versus open surgery
We were also interested in studies comparing laparoscopic and open surgeries in abdominal cavity surgeries, and data were available from 32 studies for 36,120 pregnant women.10,17,21,22,24–26,28,30–32,34–39,41,45,46,48,49,52–55,57,58,63,65,68,69 In these studies, the use of these two approaches was similar; 47% of patients had laparoscopic and 53% open surgery. However, there was wide distribution between the studies, the lowest proportion of laparoscopic approach 5% 22 and the highest 89%. 34 There was no correlation between the proportion of laparoscopy and time of the study (r = −0.042) or the sample size (r = 0.092), but between trimesters there was a significant difference; laparoscopy was used in 82% of procedures in the first, in 41% in the second, and in 27% of procedures in the third trimester (p < 0.001).
Comparison of trimesters
Data regarding the trimester when surgery was performed were available in the majority of the studies.11–14,16,17,19,21–25,28–30,32,35–39,41,42,47–51,53,54,56,59–63,66,68,69 There were data for 47,153 pregnant women; 43% of procedures were carried out during the first, 32% during the second, and 25% during the third trimester.
Description of the studies according to the fetal and maternal outcomes
Miscarriage
Data for miscarriage (fetal loss before 20 weeks of pregnancy) were reported in 25 studies.13,16–18,21,23–25,29,34–37,40,41,46,48,51–53,55,57,58,65,67 In the majority of these studies gestational age at surgery was reported, and the timing of the intervention being in the early pregnancy was verified. The prevalence of miscarriage was 3.9% in pregnancies where the mother had non-obstetric surgery (n = 54,223). Most of the studies provided data on time from surgery to the event of miscarriage, which was most commonly within the first two weeks after surgery. In four studies comparing outcomes after non-obstetric surgery (n = 52,615) with no surgery/conservative treatment (n = 7,773,465), the prevalence of miscarriage was similar at 5.1% and 4.6%, with an OR of 1.1 [95% CI 1.1-1.2].23,29,34,35 Based on data from nine studies (n = 693) comparing outcomes after laparoscopic and open non-obstetric surgery, the prevalence of miscarriage was 4.7% and 2.6%, with an OR of 1.9 [0.81-4.3], respectively.36,37,41,46,52,53,55,57,58
Stillbirth
Stillbirth (fetal loss at or after 20 weeks of pregnancy) is another concern associated with non-obstetric surgery during pregnancy. Data for stillbirth were reported in 35 studies.10–12,16,20,21,25,26,28,31,32,35,36,38–42,44,45,47,49,52–54,56–58,60,62–64,67–69 The prevalence of stillbirth in pregnancies where the mother had non-obstetric surgery (n = 67,649) was 1.1%. In 6 studies comparing outcomes after non-obstetric surgery (n = 58,642) with no surgery/conservative treatment (n = 8,791,416), the prevalence of stillbirth was higher in pregnancies with surgery at 1.3% than in pregnancies with no surgery at 0.5%, with an OR of 2.0 [1.9-2.2].11,12,26,30,31,42 Based on data from 16 studies comparing outcomes after laparoscopic (n = 979) and open (n = 3781) non-obstetric surgery, the prevalence of stillbirth was slightly higher at 4.5% after laparoscopic surgery than after open surgery at 3.5%, with an OR of 1.3 [0.9-1.8].10,28,32,36,38,39,41,45,52–54,57,58,63,68,69
Preterm birth
Preterm birth (birth before 37 weeks of pregnancy) was the most commonly reported outcome, reported in 54 studies.10-17, 19-39, 41-46, 48, 50-54, 56-63, 65-69 There were 8265 (9.7%) preterm births in 67,367 pregnancies in women with non-obstetric surgery. Fourteen studies compared data on preterm births in women with non-obstetric surgery (n = 73,110) and with no surgery during pregnancy (n = 14,833,865). The prevalence of preterm birth was higher in women with non-obstetric surgery, 9.8% versus 4.9%, with an OR of 2.1 [2.0-2.1].11,12,15,23,25,26,29,33–35,43,45,50,65 Based on data from 22 studies comparing outcomes after laparoscopic (n = 4730) and open (n = 9477) non-obstetric surgery, the prevalence of preterm birth was lower at 4.8% after laparoscopic surgery than after open surgery at 7.0%, with an OR of 0.68 [0.58-0.79].10,15,21,26,28,30,32,36–39,41,45,46,48,52–54,57,58,63,69
Low birth weight
Data on low birth weight and on fetuses being small for gestational age were reported in 19 studies.12–16,19,22,23,25–27,33–35,50,53,58,62,65 The prevalence of low birth weight was 7.8% in 64,329 pregnancies and that of fetuses being small for gestational age was 6.5% in 6980 pregnancies in which non-obstetric surgery was performed. Seven studies compared low birth weight between deliveries in women who had undergone non-obstetric surgery during pregnancy (n = 61,762) and women with no surgery (n = 9,822,477). The prevalence of low birth weight was higher after pregnancies in which surgery was performed at 8.0% versus 4.7%, with an OR of 1.8 [1.7-1.8].12,15,25,34,35,50,65 On the contrary, non-obstetric surgery did not have an impact on the prevalence of fetuses being small for gestational age. In four studies comparing that aspect, the prevalence was 6.6% (n = 6661) in pregnancies in which non-obstetric surgery was performed and 6.0% (n = 2,328,110) in pregnancies with no surgery, OR 1.1 [1.0-1.2], respectively.23,26,33,50 In Cho et al. 15 study, the prevalence of low birth weight was 5,6% after laparoscopic and 5,8% after open surgery. The prevalence of small for gestational age was 7.0% after laparoscopic surgery (n = 640) and 9.2% after open surgery (n = 521), with an OR of 0.7 [0.5-1.1].26,53,58
Low 5 min Apgar score
Data on a low Apgar score of < 7 at 5 min were reported in 16 studies.12,14,17,19,22,26,27,33,37,43,50,58,61,62,65 The prevalence of a low Apgar score was 1.7% in 9822 pregnancies in which non-obstetric surgery was performed. Six studies compared low Apgar scores between deliveries in women who had undergone surgery during pregnancy (n = 7,085) with women with no surgery (n = 1,205,005), and the prevalence was similar at 2.1% versus 1.9%, with an OR of 1.1 [0.9-1.3].12,26,33,43,50,65
Six studies reported the prevalence of low Apgar scores after laparoscopic (n = 655) and open surgery (n = 610), and the prevalence was 1.2 % and 2.6%, respectively, with an OR of 0.50 [0.2-1.1].26,27,37,58,61,65
Developmental delays or congenital anomalies
Data on developmental delays were reported in three studies,49,57,63 and data on congenital anomalies were reported in eight studies.11,14,17,18,32,50,51,58 There were no cases of developmental delays. Non-obstetric surgery (n = 5453) did not affect the prevalence of congenital anomalies, the prevalence was 4.1% in both groups.
Maternal morbidity or mortality
Data on maternal morbidity or mortality were available in 36 studies.11,16,17,20,21,24,26–33,35,37–42,46,48,49,52,54–58,60–64,68,69 The maternal mortality rate reported in eleven studies was 0.029% in pregnancies in which non-obstetric surgery was performed (n = 52,255) and 0.0043% in women with no surgery during pregnancy (n = 7,728,427), with an OR of 6.6 [4.0-11.1].11,16,17,20,21,24,29,35,40,48,56,61 Data on postoperative maternal morbidity were inconsistent. A detailed listing of complications was provided in four studies.42,46,62,68 There were no data on the type of morbidity in four studies.24,26,31,33 Surgical site infection/fever (n = 43) was reported in 17 studies,17,18,27,28,30,32,37–39,41,48,49,52,54,60,64,69 and postoperative hemorrhage/hemoperitoneum was reported in two studies.54,58 There was no maternal morbidity related to non-obstetric surgery in four studies.55,57,61,63
Discussion
This systematic review identified 60 studies published between January 2000 and November 2022 that provided eligible data concerning pregnancy, fetal and maternal outcomes after non-obstetric surgery during pregnancy. Most of the data in these publications were from the last two decades, and some older data from the 1980s were reported in three publications.60–67 The review included data for 80,205 women who underwent non-obstetric surgery during pregnancy and data for 16,655,486 pregnancies in women who had no surgery during pregnancy.
The prevalence of non-obstetric surgery was between 0.23% and 0.74% (median 0.37%), which is substantially less than the commonly quoted 2% based on data from the 1960s70 and the 1.6% recently reported in Denmark.71 The median proportions for the trimesters of non-obstetric surgeries were 43% for the first, 32% for the second, and 25% for the third trimester. In this review, the proportion was higher in the first trimester and lower in the second trimester than those at 30% and 50% reported by Cohen-Kerem et al.72 in the earlier review. Regarding emergent surgery, the distribution between the trimesters was more equal.
In our review, pregnant women who underwent non-obstetric surgery during pregnancy had an increased rate of stillbirth (OR 2.0), preterm birth (OR 2.1), and low birth weight (OR 1.8) compared to pregnant women with no non-obstetric surgery during pregnancy. However, surgery during pregnancy did not increase the rate of miscarriage (OR 1.1), low 5 min Apgar scores (OR 1.1), congenital anomalies (OR 1.0) or fetuses being small for gestational age (OR 1.1). The latter indicates that non-obstetric surgery during pregnancy was not associated with intrauterine growth retardation and that the higher prevalence of preterm births is the likely reason for the higher prevalence of low birth weight for women who underwent surgery.
Our data are consistent with that of older studies showing that non-obstetric surgery may increase the risk of adverse pregnancy outcomes.1,70,72 The prevalence of miscarriage (3.9% vs 5.8%), fetal loss (1.1% vs 2.0%) and maternal mortality rate in women (0.029% vs 0.053%) in our data were substantially less than, birth defects (4.1% vs 2.0%) higher, and prematurity similar (9.7% vs 8.2%) to that earlier review by Cohen-Kerem et al., 72 Of note, the prevalence of birth defects in the present review was similar in neonates after pregnancy with non-obstetric surgery and after pregnancy with no surgery. Recently, Moore et al. 73 showed that the 30-day mortality rates are similar in pregnant women and non-pregnant women undergoing general surgery. However, in that study, 73 the mortality rate was 10-fold higher at 0.3%-0.4% compared to the studies in this review. Taken together, our systematic review indicates that the maternal and fetal safety of non-obstetric surgery during pregnancy have increased during the last two decades, but that it is still associated increased rates of stillbirth and preterm birth. It remains an open question whether these risks are related to surgical procedures per se, the surgical disease treated, or a combination of both.
Abdominal surgery was the most common emergent surgery in the present review, and appendectomy was the most common single procedure with a median rate of 98/100,000 pregnant women. In this review, there were no studies comparing surgical approach with non-surgical treatment to treat acute appendicitis during pregnancy. In the non-pregnant population, antibiotic treatment is increasingly used as an alternative to surgery for uncomplicated acute appendicitis. 74 Recently, Yang et al. 75 showed that antibiotic treatment could be a feasible treatment for acute appendicitis in pregnant women also.
Cholecystectomy was also a common procedure with a median surgery rate of 21/100,000 pregnant women. This is consistent with data indicating that pregnant women are at higher risk of gallstones and associated diseases, such as cholecystitis, cholangitis, and pancreatitis. In this review, two studies compared operative and non-operative treatment and showed rather similar outcomes for these two approaches, but the surgical cases had a higher prevalence of low Apgar scores (4.2% vs 1.8%) compared to women who received non-operative treatment.33,34 Regarding cholecystectomy, the laparoscopic approach was used in most of the surgical cases, but the conversion rate was relatively high (14%), 3-fold higher than reported in non-pregnant population. 76 Minilaparotomy is another mini-invasive surgical cholecystectomy technique, 76 but no data on pregnant women were available.
Contrary to what was expected, our review shows no increase in the proportion of the laparoscopic approach over time for abdominal cavity surgery. Thirty-two studies including 36,000 pregnant women showed equal proportions regarding the use of the two techniques; 47% of patients had laparoscopic surgery and 53% had open surgery. The even prevalence of the laparoscopic approach was not expected, as the popularity of laparoscopic surgeries has increased over the last decades in surgical populations in general. 77 In 2011, the Board of Governors of the Society of American Gastrointestinal and Endoscopic Surgeons stated that laparoscopic treatment of acute abdominal disease has the same indications in pregnant and nonpregnant patients, and that laparoscopy can be safely performed during all trimesters of pregnancy.78 In the present review, the laparoscopic approach was used in four out of five cases in the first trimester, but only in one out of four abdominal procedures in the third trimester. Pregnant patients undergoing laparoscopic surgery had a two-fold higher rate of miscarriage and a one-third-fold higher rate of stillbirth, but a substantially lower rate of preterm birth, the fetus being small for gestational age, and low 5 min Apgar scores compared to open surgery. This is consistent with previous systematic reviews reporting that laparoscopy is associated with a higher rate of fetal loss, but a lower risk of preterm birth compared to open surgery.79,80
Not only surgical disease and surgery but also anesthetic agents are a concern in non-obstetric surgery during pregnancy. In clinical situations, it is difficult to separate the effects of anesthesia from those of surgery. Concerns about anesthetics effects were raised again two decades ago when experimental data showed that exposure to anesthetic agents may cause widespread neurodegeneration in the developing brain, as well as persistent memory and learning impairments.81 However, in animal studies, a number of confounding variables make these conclusions difficult to interpret for a human population. Human data have not shown these kinds of harmful effects on the developing fetal brain, and currently used anesthetics have not been shown to be teratogenic in clinical concentrations.2
The surgical condition itself can be a potential risk for pregnant women, pregnancy outcomes, and fetuses if left untreated. Therefore, the need for surgery and the timing of the intervention must be carefully evaluated. However, half of the procedures in the present studies were scheduled, indicating that non-emergent surgery is still common in pregnant women.24,29,35,59,65 One study comparing pregnancy outcomes after emergent and scheduled surgery found that emergency surgery was associated with a higher risk of preterm birth.59 Moreover, studies in which the majority of the surgeries were emergent the rate of adverse birth outcomes were similar compared to pregnant women with no surgery.24,65
Our study provides an updated systematic review that evaluates the effects of non-obstetric surgery during pregnancy on pregnancy, fetal and maternal outcomes, and on adherence to recent guidelines.2,3,13 The main limitation of this systematic review is that all the data, expect one small study,63 were based on retrospective studies. Furthermore, less than half of the studies had a control group consisting of pregnant women with no non-obstetric surgery during pregnancy. One of the main limitations is the heterogeneity of the types of non-obstetric surgery included in the publications. We assume that the risks for the pregnancy, fetal and maternal outcomes are not the same for example elective dental procedures and emergent abdominal cavity surgery. 35 This heterogenicity should be taken into account when interpreting the data of the present review. It appeared that only a few publications11,24,29,35,59,65 provide data on whether the procedures were elective or emergent, and even less data was available for the distribution on surgical diagnoses on benign or malignant conditions. Thus, we feel unable to give any evidence-based recommendations for performing elective surgical procedures during pregnancy and to conclude whether any specific trimester is safe from this point of view.
Further investigation is also needed concerning the comparison of conservative and operative approaches in managing different diseases in pregnant women. For example, many studies have shown the safety of surgical treatment for acute appendicitis,24,27,30 but no data are available comparing surgery and conservative treatment for pregnant women with this condition.
In conclusion, non-obstetric surgery during pregnancy increases the risk of stillbirth, preterm birth, and congenital anomalies. Surgical disease itself, however, can be a potential risk for pregnancy, fetus, and pregnant woman, and therefore surgical intervention should not be postponed in emergent conditions requiring surgery. Furthermore, our study demonstrates that the fetal and maternal safety of non-obstetric surgery have increased during the last two decades, and that both the laparoscopic and open techniques are feasible for pregnant women.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969231175569 – Supplemental material for Non-obstetric surgery during pregnancy and the effects on maternal and fetal outcomes: A systematic review
Supplemental material, sj-docx-1-sjs-10.1177_14574969231175569 for Non-obstetric surgery during pregnancy and the effects on maternal and fetal outcomes: A systematic review by Anna Haataja, Hannu Kokki, Outi Uimari and Merja Kokki in Scandinavian Journal of Surgery
Footnotes
Author contributions
The concept or design of the work: AH, HK, OU, MK; Acquisition and analysis of data: AH, HK; Interpretation of data: AH, HK, OU, MK; Drafted the article: AH; Revised it critically for important intellectual content: HK, OU, MK; Approved the version to be published: AH, HK, OU, MK.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.