
Abstract
Purpose:
Management of nephrolithiasis is unique in pregnancy and requires multidisciplinary care. To identify the effectiveness or safety of temporary drainage or definitive treatment methods to manage urolithiasis in pregnancy.
Methods:
The search strategy aimed to find both published and unpublished studies was conducted in August 2021. Studies published in any language on any date were considered for inclusion.
Results:
Of a total of 3349 publications, 36 studies were included in our qualitative evaluation and 32 studies in the quantitative synthesis. The commonly reported method was stent insertion (n = 29 studies), pneumatic (n = 12), laser (n = 9) lithotripsy, and stone removal using any devices (basket, grasper, or forceps) (n = 11). In seven studies, the authors reported the outcomes of conservative management, and the results showed that the stone-free rate is 54%, and symptom relief occurred in 62% of women. Seven eligible studies reported that 79.9% of urolithiasis were expulsed through stent insertion, while this rate was 94.6% among percutaneous nephrostomy use in two included studies, 88.5% for pneumatic lithotripsy (n = 7 studies), and 76.4% for laser lithotripsy (n = 4 studies), or 95.4% for stone removal method. In addition, adverse events were reported in less than 10% of pregnant women.
Conclusions:
The results showed that stent, pneumatic or laser lithotripsy, and ureteroscopic stone removal were the commonest used methods in the included studies. They can be effective and safe treatment approaches without major maternal or neonatal complications, and could be introduced as an effective and safe therapeutic method for urolithiasis during pregnancy. However, most of the included studies had moderate quality according to critical appraisal checklists. Further prospective studies are needed to reach a conclusion.
Brief summary
The stone-free rate and symptom relief following different urolithiasis management methods was 78% in pregnancy. Seven eligible studies reported that 79.9% of urolithiasis were expulsed through stent insertion, while this rate was 88.5%, for pneumatic lithotripsy, 76.4% for laser lithotripsy, or 95.4% for the stone removal method. In addition, adverse events were reported in less than 10% of pregnant women.
Introduction
During pregnancy, urolithiasis constitutes a significant health concern and a common cause of non-obstetric pain and hospitalization. The incidence of urinary stones during pregnancy varies from 1/200 to 1/2000, not different from non-pregnant women.1,2 Urolithiasis is more common in the second or third trimester of pregnancy and is more common in multiparous women. 3 Predisposing factors for stone formation in pregnancy include dilatation of the urinary tract due to ureteral obstruction by the uterus, the relaxing effect of progesterone smooth muscle, and infection. 4 In addition, physiological hydronephrosis, up to 90% on the right and 67% on the left in the pregnancy lead to stasis, stone formation, and misdiagnosis. 5
An accurate diagnosis of ureteral stones is essential for all possible complications. During pregnancy, clinical manifestations of ureteral stones include colic or vague pain. Other symptoms include hematuria and fever. An initial diagnosis can be made based on these symptoms, but in about 28% of pregnant patients, the diagnosis can be inaccurate and misdiagnosed as diverticulitis, appendicitis, and placental abruption. 6 Causes of misdiagnosis include limited use of X-rays, intravenous urography (IVU), and computed tomography (CT) during pregnancy due to teratogenicity.7,8 Ultrasound (US) is mainly used as the preferred diagnostic test in pregnant women suspected of having ureteral colic due to lack of ionizing radiation, low cost, and availability. However, it is challenging to manage ureteral stones during pregnancy due to its low sensitivity. In comparison to renal US, transvaginal US in the identification of distal ureteral stones, and differentiation between obstruction and physiologic hydronephrosis has higher sensitivity. The other diagnostic methods, that is, noncontrast CT as the gold standard in general populations, has over 98% sensitivity and specificity. However, this modality is avoided due to concerns about fetal radiation exposure in pregnancy especially in the first trimester. Magnetic resonance imaging (MRI) utilizes nonionizing radiation, and is considered as a useful alternative to CT in the pregnant patients. In addition, it has similar or greater sensitivity and specificity than CT. Magnetic resonance urography (MRU) is another modality that is useful in distinguishing physiologic from obstructive hydronephrosis in pregnancy. IVU, or pyelography (IVP), which uses iodinated contrast to visualize the collecting system by providing serial plain film imaging, more commonly used in the past. However, its utility in pregnancy due to the radiation dose exposure as well as in the general population is called into question, and alternative imaging modalities, including US, CT, and MRI, are superior for the diagnosis of urolithiasis. 9
Management of urolithiasis during pregnancy is crucial because of the potential risks to the mother and fetus. 10 The main threats are preterm delivery and premature rupture of membranes. Other pregnancy complications include obstructive uropathy, hypertension, increased incidence of cesarean section, gestational diabetes, recurrent miscarriages, and preeclampsia. 11 In conservatively resistant patients, the management of stones in pregnancy varies from conservative treatments to a double J (DJ) stent (DJ) or percutaneous nephrostomy (PCN) tube.12,13 Although ureteral stones are not very common during pregnancy, they are still challenging to diagnose and treat. There are several ambiguities related to diagnostic imaging, medical therapy, PCN/ureteral stent reliability, ureteroscopic safety, surgical method, and follow-up protocol during pregnancy. 14
Review question/objective
The quantitative objectives are meant to identify the prevalent used strategies for urolithiasis management in pregnancy as well as evaluation their effectiveness and safety. More specifically, the objectives intend to shed some light on the effectiveness and safety of treatment methods, including expectant management, medical expulsion therapy (MET), transurethral lithotripsy (TUL) using pneumatic or laser, and temporizing treatments such as ureteral stents and PCN, ureteroscopic stone removal (URS), extracorporeal shock wave lithotripsy (ESWL), or percutaneous nephrolithotomy (PCNL).
Methods
Inclusion criteria
Types of participants
The quantitative component of this review considered pregnant women with urolithiasis.
Types of intervention(s)
The quantitative component of the review entailed studies that evaluate various treatment method for urolithiasis, including expectant management, MET, TUL using pneumatic or laser, and temporizing treatments such as ureteral stents and PCN, URS, ESWL, or percutaneous nephrolithotomy (PCNL).
Types of outcomes
This review considered studies that include the following outcome measures:
Primary outcomes: The stone-free rate following different therapeutic approaches.
Secondary outcomes: The frequency of used methods to manage urolithiasis during pregnancy, as well as obstetric complications, including the risk of uterine contraction, preterm labor, threatened abortion, UTI, or LUTS, or fetal outcomes.
Types of studies
The quantitative component of the review entailed all interventional studies (randomized controlled trial or quasi-experimental), and in the case of their absence, observational studies including cohort, cross-sectional, or case–control.
The proposed systematic review was conducted in accordance with the Joanna Briggs Institute methodology for systematic reviews of effectiveness evidence. 15 The current protocol is registered in PROSPERO (No. CRD42020209054).
Search strategy
The search strategy aims to find both published and unpublished studies in the Cochrane Library, MEDLINE (PubMed), Web of Science, Scopus, ProQuest, and Google scholar databases. A three-step search strategy was utilized in this review. An initial limited search of MEDLINE was undertaken, followed by analyzing the text words, including the title and abstract, and the index terms used to describe the article. Later, the second search using all identified keywords and index terms was undertaken across all included databases. Third, the reference list of all identified reports and articles was searched for additional studies. Studies published in any language and date were considered for inclusion in this review (Appendix I).
We screened reference lists from relevant published studies, including trials, systematic reviews, meta-analyses, and narrative reviews.
To search the pointed databases, the keywords provided by the MeSH tool were used in combination with Boolean operators. Initial keywords to be used were as follows:
“Urolithiasis” OR “nephrolithiasis” OR, “ureter*,” OR “kidney,” OR “renal” AND, “Stone” OR “calcul*,” OR “colic,” AND “gestation*” OR “pregnan*.” The full search strategy is attached as Supplemental file.
Study selection
All identified citations were collated and uploaded into EndNote, and duplicates were removed after the search. Two independent reviewers screened titles and abstracts for assessment against the inclusion criteria for the review. The full text of selected citations was assessed in detail against the inclusion criteria by two independent reviewers. Reasons for exclusion of full-text studies that do not meet the inclusion criteria were recorded and reported in the systematic review. Any disagreements that arose between the reviewers at each stage of the study selection process were resolved through discussion or with a third reviewer. The search results were reported in full in the final systematic review and presented in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (Fig. 2). 16
Assessment of methodological quality
Quantitative papers selected for retrieval were assessed by two independent reviewers for methodological validity prior to inclusion in the review using standardized critical appraisal instruments from the Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument (JBI-MAStARI). Any disagreements between the reviewers were resolved through discussion or with a third reviewer. Following the critical appraisal, studies that did not meet a certain quality threshold were excluded.
Data extraction
Quantitative data were extracted from papers included in the review using the standardized data extraction tool from JBI-MAStARI. The extracted data included specific details about the interventions, population, study methods, outcomes of significance to the review question, and specific objectives.
Dealing with missing data
We tried to obtain any relevant missing data, such as the number of screened and randomized analysis populations from the study authors.
Data synthesis
Statistical meta-analysis was performed using the Mantel–Haenszel method with Comprehensive Meta-Analysis software (ver. 2.2; Biostat, Englewood, NJ, USA). Heterogeneity was statistically calculated using the standard I2 test. In the present meta-analysis, I2 > 50% and a significance level of p < 0.10 for Cochran’s Q was considered as clinically important heterogeneity. A random or fixed model was used, based on heterogeneity analysis. Furthermore, a funnel plot was generated to assess publication bias. The results were presented in a narrative form where statistical pooling was not possible.
Evidence synthesis
Literature search and description of studies
During the electronic databases searching, hand-searching, and reference checking, we found 3349 publications till August 2021. After removing the duplicated studies, 1992 studies were screened in the title/abstract stage. The full-text of 62 articles was evaluated and finally, 36 studies met our inclusion criteria in our qualitative evaluation and 32 studies in the quantitative stage. Additional information on the selection process is presented in the PRISMA flow diagram (Fig. 1).
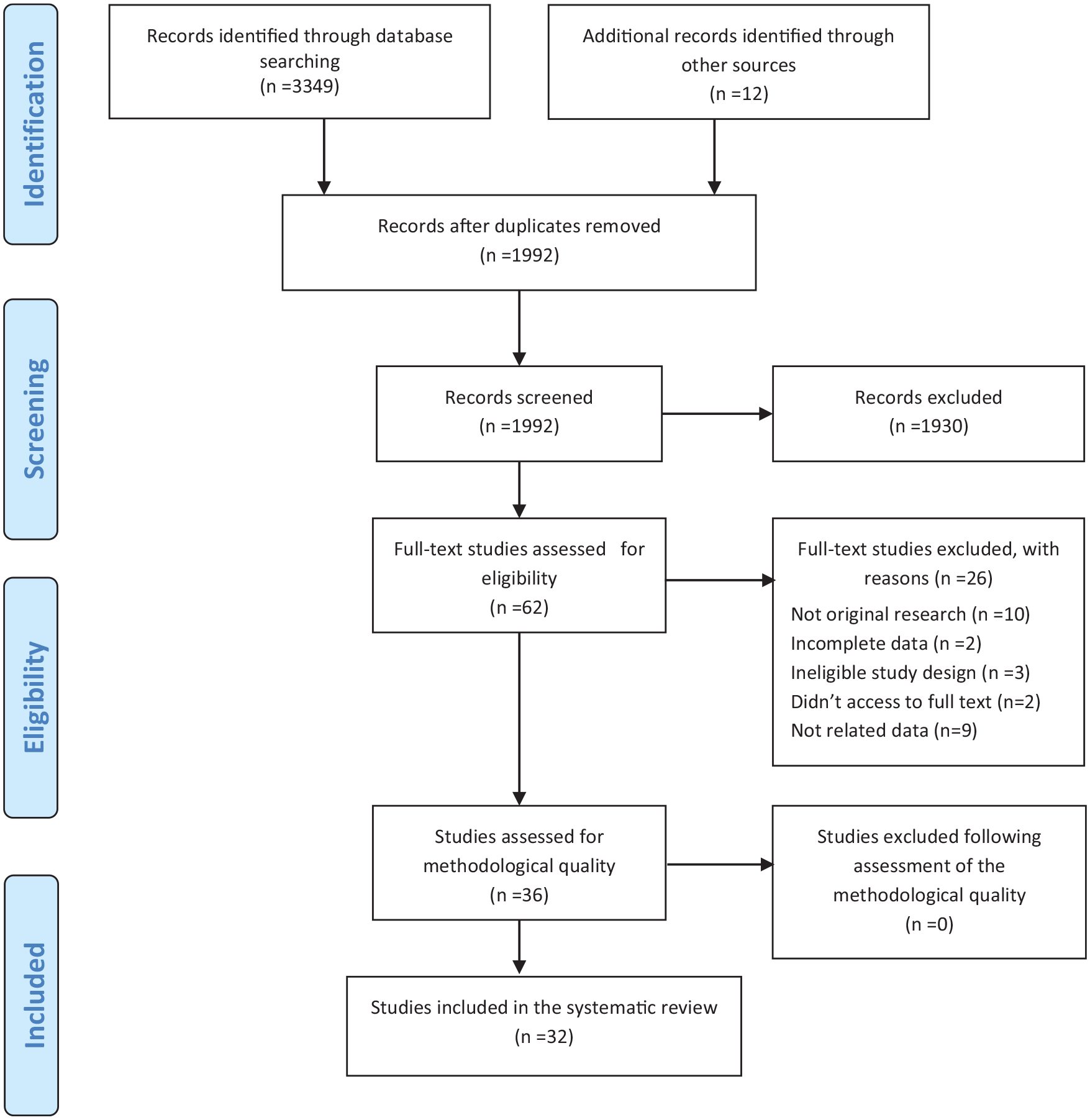
Search results and study selection and inclusion process.
Risk of bias in the included studies
Methodological quality assessment using the JBI appraisal checklist is presented in Table 1. According to the results, most of the studies had either medium or low quality.
Critical appraisal results: results of studies quality according to the JBI critical appraisal checklists.
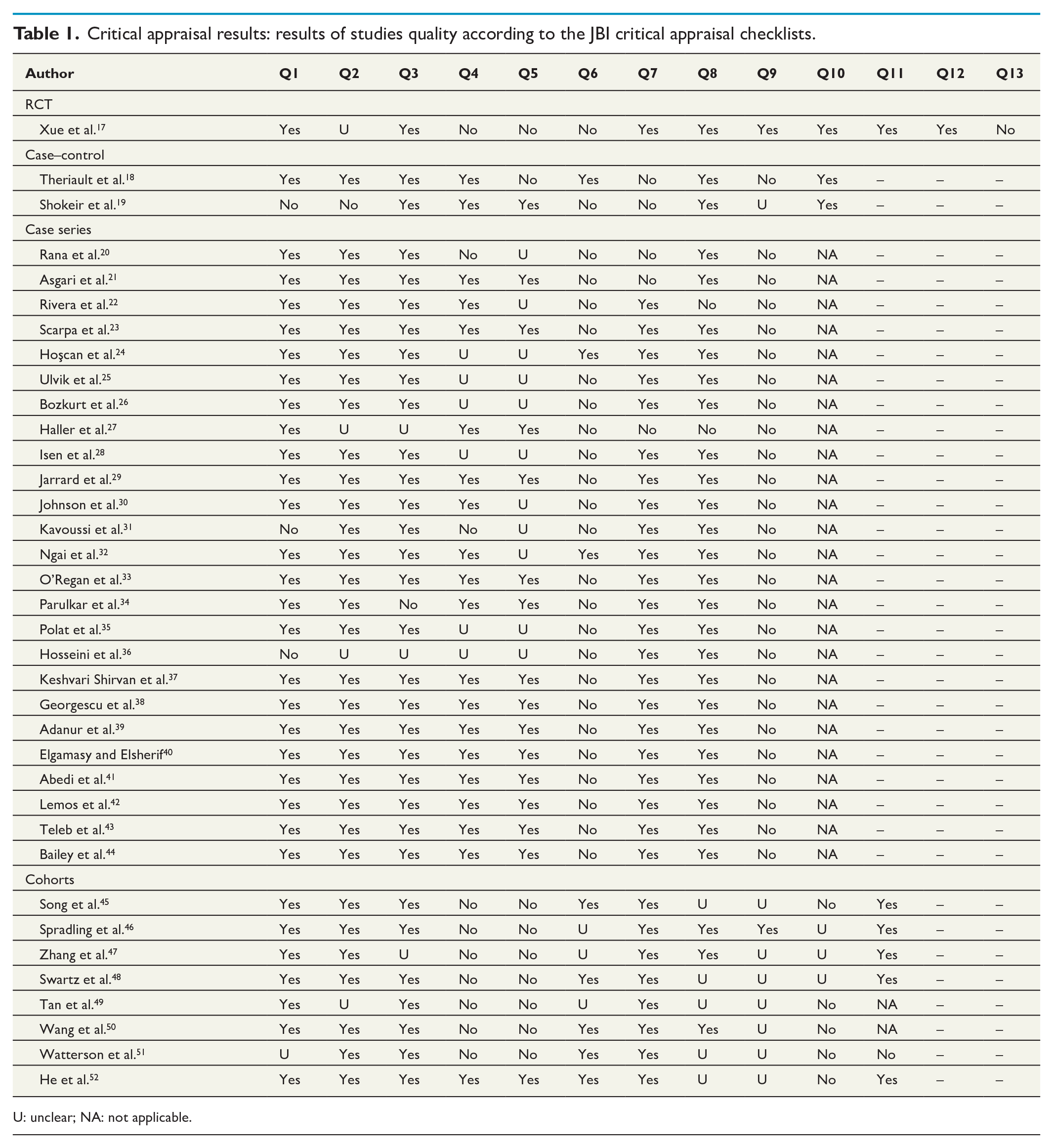
U: unclear; NA: not applicable.
Summary of the evidence
In all, 25 studies were case series, 8 cohort, 2 case–control, and 1 randomized control trial. The stone-free rate and symptoms relief following different urolithiasis management methods in pregnancy was 77.5% (95% CI: 70.8%–83.0%, I2: 81.49), and 77.7% (95% CI: 71.5%–82.9%, I2: 77.85), respectively.
The minimum reported stone dimension was 5.1 mm, and the maximum was 22.2 mm. In the other cases, the mean size was in a range of 7–8 mm. The calculi were located in the different parts of ureter. However, the distal ureter was the predominant part, and the proximal and mid ureter were in the next rank.
Colicky pain or flank pain was reported in most of the cases. Other complications were hematuria, nausea and vomiting, irritative voiding, fever, and abdominal pain.
A total of 2852 pregnant women 16–44 years old and with gestational age of 9–38 weeks were managed conservatively (n = 465), stent placement (n = 1272), or underwent medical therapy with tamsulosin (n = 96), PCN during pregnancy or post-delivery (n = 133), ESWL (n = 6) in unknown pregnancy cases, stone removal with forceps, grasper, or basket (n = 111), TUL laser (n = 215), TUL pneumatic (n = 220), TUL pneumatic or laser (n = 308), push-back (n = 12), or either nephrectomy or nephrostomy (n = 1). The results of the different management method frequency used are summarized in Table 2.
The frequency of any management method used for urolithiasis during pregnancy.
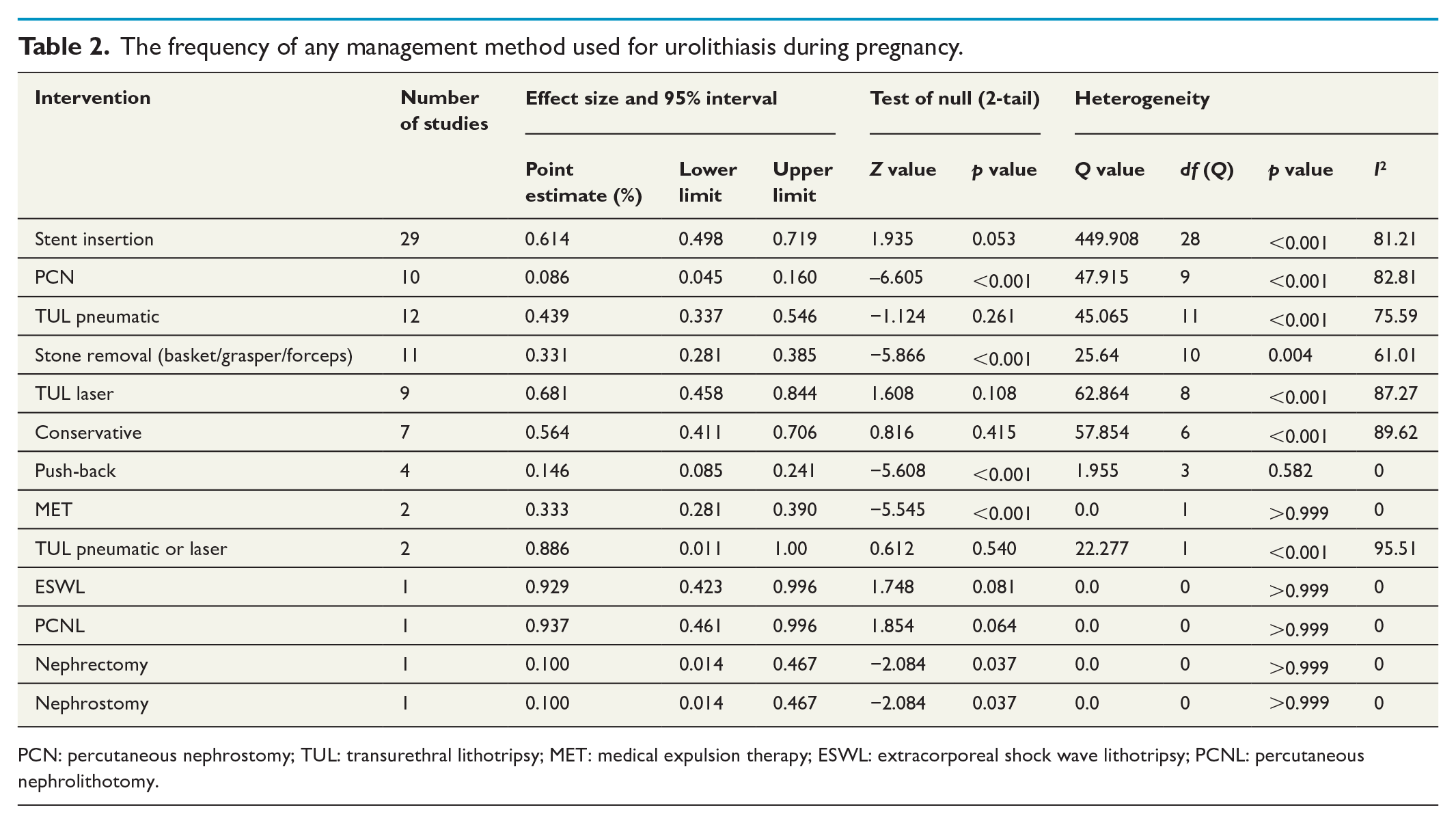
PCN: percutaneous nephrostomy; TUL: transurethral lithotripsy; MET: medical expulsion therapy; ESWL: extracorporeal shock wave lithotripsy; PCNL: percutaneous nephrolithotomy.
Descriptive studies
Conservative management
Seven studies reported the outcomes of conservative management in 465 pregnant women.
The results for stone-free rate showed that this method is 54% effective in stone expulsion (95% CI: 22.2%–82.8%; I2: 86.18%), while in controlling of symptoms its efficacy was 61.7% (95% CI: 33.7%–83.6%; I2: 95.14%) (Fig. 2).
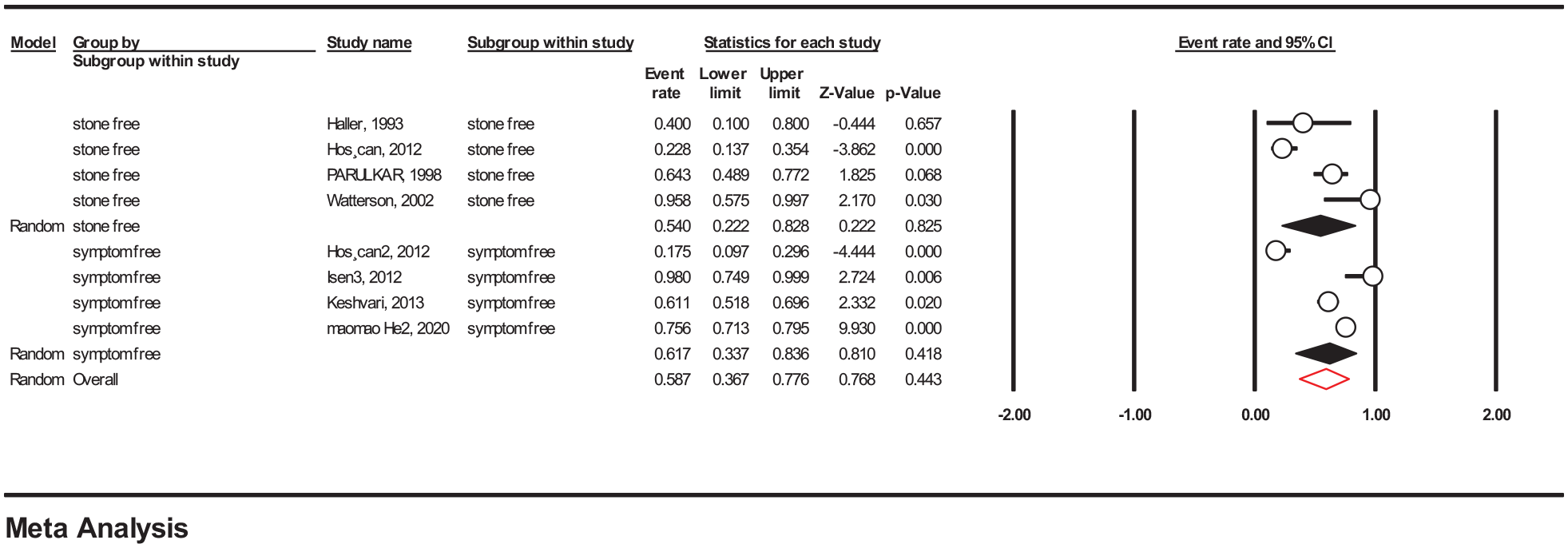
Efficacy of conservative management in controlling urolithiasis.
Medical expulsive therapy
Two studies reported the outcomes of medical expulsive therapy with Tamsulosin. Theriault et al. 18 used Tamsulosin with a dose of 0.4 mg once a day for 6 days on 69 pregnant women. They demonstrated spontaneous passage rate in the MET group 58% (25/48) compared with 43% (29/76) in the control group, without statistical significance (p = 0.18). Another retrospective cohort study with O’Regan et al. 33 on 26 women with a median duration of antepartum tamsulosin exposure of 3 days was accompanied without any maternal or neonatal side effects and was assumed that this method is safe in pregnancy as an adjunctive therapy for urolithiasis (Supplemental file, Table 3).
Stent insertion
The common management method for urolithiasis in the included studies belonged to stent insertion (n = 29 studies). The results showed that this method is effective in 79.9% of pregnant women (95% CI: 70.4%–87%, I2: 93.21%).
Instrumental stone extraction or push back
Eleven studies were eligible to be included in the systematic review and meta-analysis on the frequency of stone removal using any device such as grasper, basket, or forceps. The stone-free rate following stone extraction was 95.4% (95% CI: 80.2%–99.1%; I2: 0%) that was evaluated on three eligible studies for meta-analysis (Supplemental file, Table 3).
Stone push-back was applied in four studies with a point estimate of 0.146 (95% CI: 0.085–0.241; I2: 0%).
Pneumatic or laser lithotripsy
Of a total 23 studies which used holmium, YAG laser, or pneumatic TUL to manage pregnancy urolithiasis, the point estimate was 0.541 (95% CI: 0.427–0.650; I2: 89.97%) (Fig. 3).
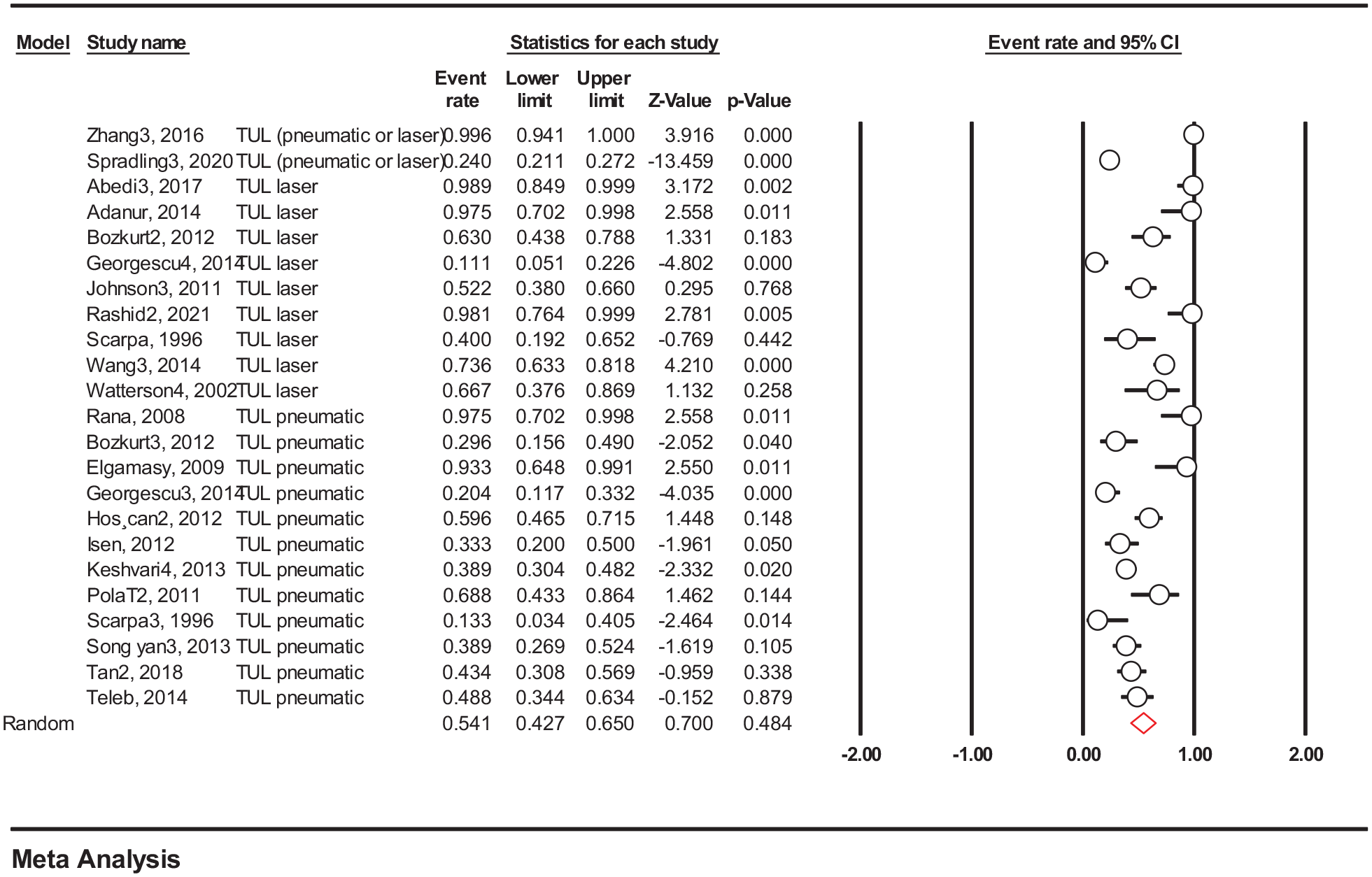
Frequency of pneumatic or laser TUL to manage urolithiasis.
In two studies, the authors did not report the exact type of TUL, and mentioned that they used pneumatic or laser lithotripsy. The point estimate was 0.886 (95% CI: 0.011–1.00; I2: 95.51) (Table 2), and a stone-free rate of 53.3% (95% CI: 29.3%–75.9%; I2: 0) (Supplemental file, Table 3).
A total of 12 studies reported the outcomes of pneumatic lithotripsy, and 9 studies used laser TUL. The point estimates for pneumatic TUL were 0.439 (95% CI: 0.337–0.546; I2: 75.59%), and for laser TUL 0.681 (95% CI: 0.458–0.44; I2: 87.27%) (Table 2).
The stone-free rate for these modalities were 88.5% (95% CI: 82.1%–92.8%, I2: 0%), and 76.4% (95% CI: 67.8%–83.2%, I2: 56.75%), respectively (Supplemental file, Table 3).
PCN
Ten studies reported the use of PCN to manage pregnancy nephrolithiasis, and reported a point estimate of 0.086 (95% CI: 0.045–0.160; I2: 82.81%). In terms of this method’s efficacy, only two studies were eligible for meta-analysis and the results showed 94.6% of efficacy (95% CI: 69.9%–99.36%, I2: 0%).
Other methods
Asgari et al., 21 in a retrospective study, gathered the data of 636 women of reproductive age and observed that six pregnant women out of the total cases underwent ESWL during the first trimester of pregnancy. Surprisingly, no detectable malformations or chromosomal anomalies were reported, and this method’s efficacy was near 100% (Table 2 and Supplemental file, Table 3).
Pain management
Only one study 51 was based on pain management during pregnancy, and in the other included studies, the symptoms of patients were reported as the efficacy of therapeutic method in conservative management,21–24 and one study following stent insertion. 25
Xue et al. 17 examined the analgesic efficacy of intracutaneous sterile water injection (n = 21) compared with oral paracetamol (n = 24) in pregnant women with acute renal colic using a visual analog scale (VAS) system. The results showed no statistically significant difference in pain score between the two groups at baseline, but sterile water injection was superior to oral paracetamol at different time points after treatment.
Publication bias
There was no evidence of publication bias in favor of studies reporting a high stone-free rate in ureteroscopy with or without instrumental stone extraction using Egger’s test (intercept = 0.506, t value = 0.789, two-tailed p = 0.431) (Fig. 4).
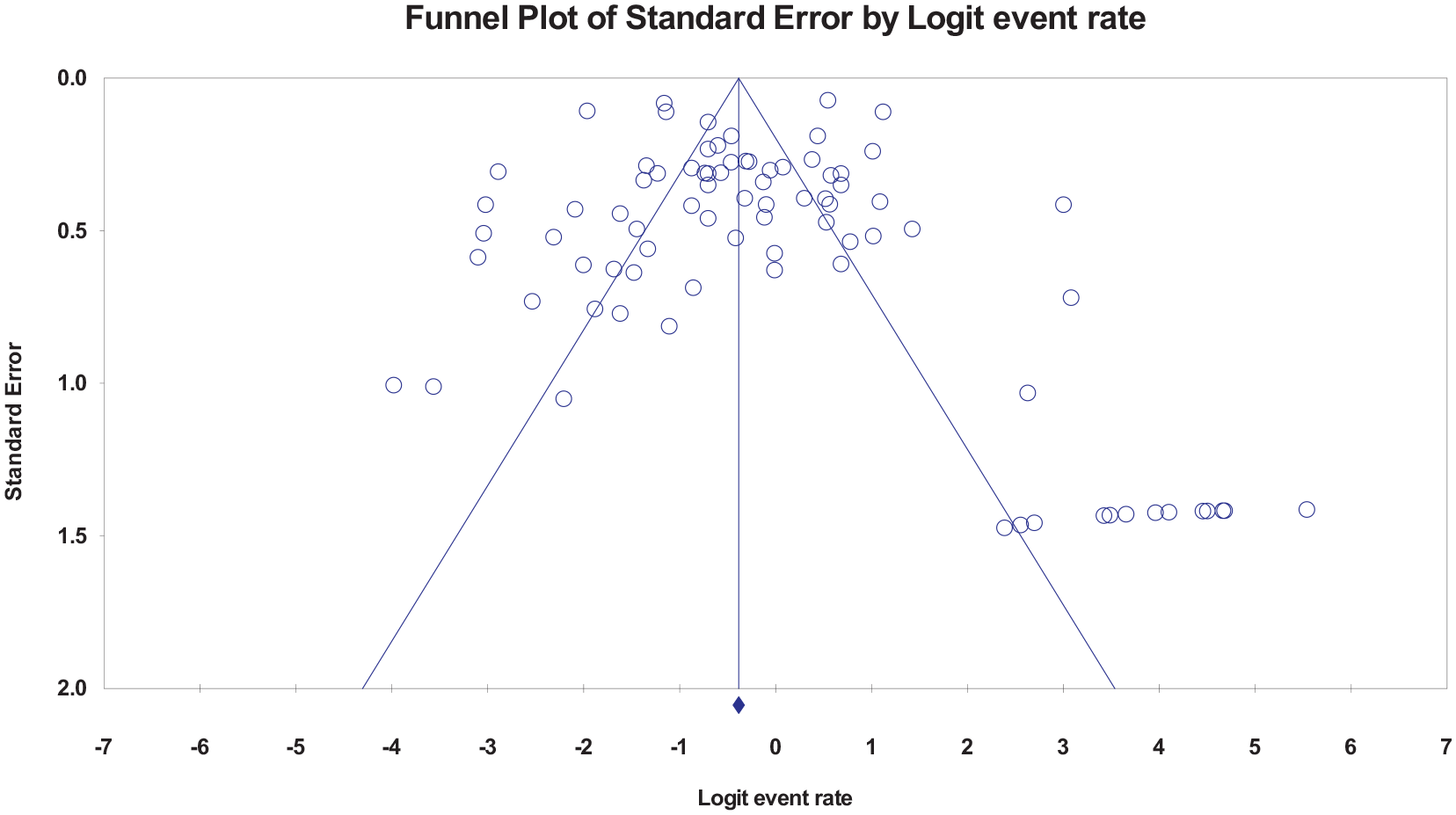
Publication bias of the included studies.
Pregnancy outcomes
Birth weight
In four studies, no low birth weight was reported. Asgari et al. 21 reported a median 2.85 (2.22–3.45) kg for the infants of mothers who were exposed to ESWL during pregnancy.
In the study of Song et al., 45 the infants mean birth weight in 21 pregnancies following lithotripsy was 3276 g. In the PCN group, the mean birth weight was 3250 g (in 16 cases), and 3400 g for neonates of 17 mothers with internal ureteral stent.
Haller et al. 27 reported that in 10 mothers who underwent conservative, ureteral stent, or nephrostomy, the mean birth weight in two neonates was greater than 4000 g, one was 3840 g, and the other 5 were between 3280 and 3480 g. The twins weighed 2030 and 2130 g.
Bailey et al. 44 reported an appropriate infant birthweight for gestational age (mean (SD) 3.47 (0.88) kg in the MET group versus 3.4 (0.56) kg in the control group infants.
Safety of different procedure in pregnancy
Of the included studies for systematic review and meta-analysis, 234 adverse events were reported out of 3144 pregnancies to be following one of the treatment methods.
Less than 10% of pregnant women experienced adverse events. The common reported events were encrustation of stent (n = 6), LUTS (n = 3), and stent migration (n = 3). Premature uterine contraction and UTI were the other common reported events following pneumatic or laser TUL, stone removal, and stent. The results of meta-analysis are illustrated in the Supplemental file, Table 4. Other therapeutic or palliative management methods were accompanied with rare adverse events.
Discussion
During pregnancy, the ureteric stone is a diagnostic and therapeutic challenge. This study was aimed to assess the effectiveness and safety of management strategies of urolithiasis during pregnancy. Our results showed that among 32 included studies for meta-analysis, the common reported method was stent insertion (n = 29 studies), and pneumatic (n = 12), laser (n = 9) and stone removal using one of the devices (basket, grasper, or forceps) (n = 11) were in the next ranks. In seven studies, the authors reported the outcomes of conservative management and the results showed that the stone-free rate was 54%, and symptoms relief occurred in 62% of women. The efficacy of stent in stone expulsion was 79.9% among seven eligible studies, 94.6% among PCN use in two included studies, 88.5% for pneumatic lithotripsy (n = 7 studies), and 76.4% for laser lithotripsy (n = 4 studies), or 95.4% for stone removal method. In addition, adverse events were reported in less than 10% of pregnant women. The commonest adverse events were LUTS, UTI, stent encrustation, or premature uterine contraction. However, methodological quality assessment using the JBI appraisal checklist showed that most studies had medium or low quality. There was no publication bias in the included studies. In addition, all procedures were reported that seems safe in terms of birth weight and completion of the full-term pregnancy except preterm labor (n = 6), and one threatened abortion which was resolved with appropriate treatment. Only two fetal losses were detected following DJ stenting or ureteroscopy and basket use to removal stone out of 15 women due to pyelonephritis and preterm labor in the second trimester of pregnancy. 34
Urolithiasis during pregnancy is one of the leading causes of abdominal pain and subsequent hospital admission during the pregnancy. 1 From the etiological point of view, anatomical and physiological changes during the pregnancy may impact the potential stone formation and make pregnant women more susceptible to kidney stones.53,54 Yet, studies could not detect a significant incidence difference between pregnant and nongravid women. 1 As the most common non-obstetric complication during the pregnancy and an anxiety-provoking experience, 9 potential serious risks, suggested careful diagnostic and management strategies for urolithiasis during pregnancy. 53 US is the initial diagnostic modality in pregnant women with potential renal colic. After overcoming the diagnostic limitation of using X-rays, CT, and IVU during pregnancy, there are still challenges regarding the first-line treatment of urolithiasis during pregnancy.
In case of no indications for acute intervention, the American Urological Association (AUA) guidelines endorsed initial management with conservative treatment. Studies reported up to 80% of the spontaneous passage rate in pregnant women, which is significantly higher than that in non-pregnant women. 55 This finding seems exaggerated, and it may be associated with misdiagnosis and poor follow-up. 56
Using antibiotics and symptom control with analgesia and anti-emetics as well as aggressive fluid resuscitation should be considered in case of decision-making for a conservative treatment approach. This protocol should be followed up with serial US. 1 The size and location of stones are two determinative factors in the rate of successful conservative treatment. α-blockers, such as tamsulosin and calcium channel blockers, as commonly utilized medication in the general population, increase the chance of stone passage 57 and are thought to be safe during pregnancy (category B medication). 58
In our meta-analysis, one study was eligible for the tamsulosin efficacy evaluation, and the results showed that 62.3% of pregnant women responded to this method satisfactorily, and the stones were passed.
In case of failed expectant management and required urinary drainage, ureteral stents can be placed during the second or third trimesters of pregnancy under local anesthesia or intravenous sedation. 28 Frequent exchange of either ureteric stents or nephrostomy tubes every 4–6 weeks 1 should be considered due to accelerated encrustation of foreign bodies in the urinary tract during pregnancy. 53 Our results confirmed these adverse events among the included studies (8.8%), which were the common reported adverse events. Stent encrustation was easily removed with postpartum ESWL of the stent calcification,29,32,34 stent replacement in 9, 11, and 17 weeks of pregnancy postoperative in three cases, 50 stent change in the interval of 3–4 weeks in four patients, 45 removing hard DJ stent by ureteroscopy in one case, 49 or complete stone fragmentation and/or removal of encrusted ureteral stents using the holmium:YAG laser. 51
During the first trimester and in the case of large stone burden, sepsis, or pyonephrosis, PCN is also a helpful intervention, which can be performed under local anesthesia with US guidance.1,29 Its efficacy is near 100%.
The drawbacks of temporary drainage and delaying of definitive stone management until the postpartum period highlighted a need for another intervention for the management of urolithiasis during pregnancy. At present, TUL is considered a definitive surgical management strategy in the case of spontaneous stone passage failure. 59 Our results showed that after stent insertion, the commonly used methods to manage urolithiasis during pregnancy is either pneumatic or laser lithotripsy, and the stone-free rate was 88.5%, and 76.4%, respectively.
Previous studies showed that due to the risks of anesthesia, URS should be avoided during the first trimester. 60 In our meta-analysis, the common complications following pneumatic/laser lithotripsy, and stone removal were premature uterine contraction, and preterm labor, even though they were rare.
There are also other contraindications, such as sepsis and large volume or multiple stones for ureteroscopic lithotripsy. 31 Our systematic review study found an acceptable safety and efficacy for URS during the pregnancy. Holmium YAG laser lithotripsy and pneumatic lithotripsy are the currently recommended methods during pregnancy. 20 An Update Meta-Analysis study in 2017 found a shorter mean operative time as well as better early and delayed stone-free rate for holmium YAG laser lithotripsy compared with pneumatic lithotripsy, 61 but there is not enough evidence for these comparisons during the pregnancy. 1 These results are not in accordance with ours that showed that the efficacy of pneumatic TUL was greater than laser lithotripsy (88.5% versus 76.4%).
Another stone management method is shock wave lithotripsy in non-pregnant individuals. Although Asgari et al. 21 is the only study which assessed shock wave lithotripsy during pregnancy, they did not report any detectable associated malformations or chromosomal anomalies; shock wave lithotripsy and PCNL are contraindicated during the pregnancy.53,54 Miscarriage, congenital malformation, intrauterine growth retardation, and placental displacement are the complications of shock wave lithotripsy and PCNL that require longer operative times and prone position of the patients.54,62,63 Laparoscopic or open surgery is the choice method when it remains the only option and only in the second trimester of the pregnancy. Generally, urologists, obstetricians, radiologists, and anesthesiologists should be consulted for achieving the best decisions for each patient and safe outcomes for both mother and infant.9,54
To our knowledge, the current systematic review and meta-analysis is the first study on the efficacy and safety of the different modalities for urolithiasis in pregnancy. Although we performed a quantitative synthesis on the efficacy assessment, in most studies, the authors used different methods in this regard, that may affect the results of study.
Conclusion
The results showed that stent, pneumatic or laser lithotripsy, and URS were the commonest used method in the included studies, and can be an effective and safe treatment approach without major maternal or neonatal complications, and could be introduced as an effective and safe therapeutic method for urolithiasis during pregnancy; however, most of the included studies had moderate quality according to the results of critical appraisal checklists. Further prospective studies are needed to reach a conclusion.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969221145774 – Supplemental material for Management of urolithiasis in pregnancy: A systematic review and meta-analysis
Supplemental material, sj-docx-1-sjs-10.1177_14574969221145774 for Management of urolithiasis in pregnancy: A systematic review and meta-analysis by Hanieh Salehi-Pourmehr, Sona Tayebi, Nooriyeh DalirAkbari, Amir Ghabousian, Fateme Tahmasbi, Fatemeh Rahmati, Amirreza Naseri, Reyhaneh Hajebrahimi, Robab Mehdipour, Mahdi Hemmati-Ghavshough, Ali Mostafaei and Sakineh Hajebrahimi in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The regional ethics committee of Tabriz University of Medical Sciences (IR.TBZMED.REC.1400.859) approved of the current study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by Tabriz University of Medical Sciences, Grant No: 68661.
Prospero registration number
The current protocol is registered in PROSPERO (No. CRD42020209054).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.