
Abstract
Purpose:
To describe patient characteristics and to compare outcomes of children undergoing rigid intramedullary nailing of tibial fractures as compared with those operated on using elastic intramedullary nailing.
Methods:
A retrospective review of 26 children who have undergone flexible intramedullary nailing of tibial fractures and 30 children with rigid nailing at our university hospital between 2008 and 2017. The patient charts and radiographs were evaluated to identify demographic characteristics and several variables were measured preoperatively, as well as 6–12 weeks postoperatively in addition to final follow-up radiographs.
Results:
Twenty-six patients (26/26, 100%) treated with a flexible nail and 14 patients (14/30, 46.7%) treated with a rigid nail had open proximal tibial physis (p < 0.001). An acceptable postoperative alignment was obtained in 20 patients (20/26, 76.9%) in the elastic stable intramedullary nail group and in 29 patients (29/30, 96.7%) in the rigid group (p = 0.026). Some complications occurred in four patients (4/26, 15%) in the elastic stable intramedullary nail population and seven patients (7/30, 23%) in the rigid intramedullary nail population (p = 0.46). Malunion occurred in six patients (6/26, 23%) in the elastic stable intramedullary nail group and in none of the patients treated with a rigid intramedullary nail (p = 0.005).
Conclusion:
Younger children with tibial fractures who weight 50 kg or less and with proximal tibial growth plates wide open can be treated with elastic stable intramedullary nail while more mature adolescents benefit from rigid intramedullary nailing.
Keywords
Introduction
Tibial fractures are the third most common fracture site in pediatric patients under 16 years (1, 2). Non-operative management using closed methods and cast immobilization is usually the treatment of choice for closed, minimally displaced fractures (3, 4). Operative techniques using elastic intramedullary nailing, plate fixation, or external fixation are, however, indicated when it is not possible to achieve and maintain acceptable alignment by non-operative means until union occurs. These indications include open fractures, fractures complicated by compartment syndrome and with comminuted and unstable fractures (5, 6). In addition, internal fixation has become increasingly popular as operative treatment of pediatric fractures is increasing in general (7). In a recent study, Stenroos et al. stated that one in three pediatric tibia shaft fractures is currently treated operatively (1). Elastic nailing is preferred in surgical stabilization of pediatric shaft fractures because the low risk of infection; it allows early mobilization and it does not cross the physis. Several studies have shown good outcomes with flexible intramedullary nailing (3, 8, 9). However, possible complications using this technique include axial deviations and delayed unions. The lack of rigidity of flexible nailing is associated with a higher risk of malunion in older and heavier children (10–12).
There is very limited data on rigid intramedullary nailing in the pediatric population. It has been generally contraindicated to use rigid intramedullary nailing across the open proximal tibial physis except at the end of the growth period because of concerns about growth disturbance (5).
Our aim was to describe the pediatric patient population undergoing rigid intramedullary nailing and to compare its surgical outcomes with those children receiving elastic intramedullary nailing. The hypothesis was that younger and more light patients with displaced tibial fractures more often received elastic intramedullary nails, and this resulted into less accurate reduction than in older adolescents treated with rigid intramedullary nailing.
Material and Methods
Patients and Study Design
This was a retrospective study of 56 patients under 16 years with a tibial diaphyseal fracture who were treated with intramedullary nailing at our university hospital during 2008–2017. Twenty-six patients were treated with a flexible intramedullary nail (see Figs 1 and 2) and 30 patients with a rigid nail (see Figs 3 to 5).

Anteroposterior and lateral radiographs of a 10-year-old boy with a left open tibial fracture.

Anteroposterior and lateral radiographs of the patient in Fig. 1 3 years after flexible intramedullary nailing showing union of the fracture.

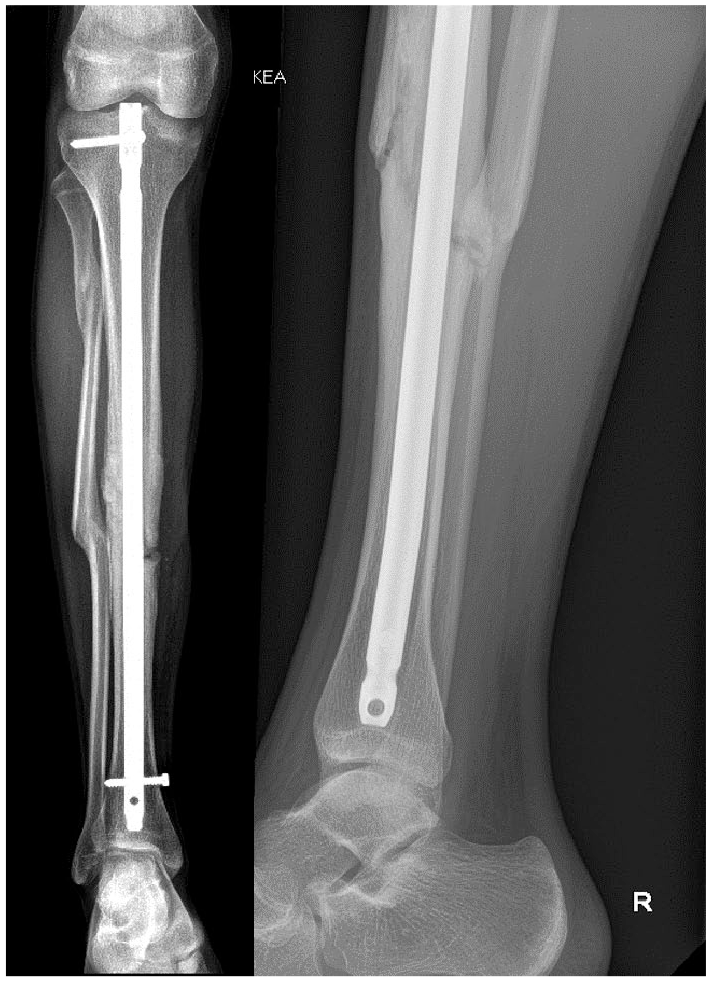
14-year-old boy with a right open tibial fracture. Anteroposterior and lateral radiographs on a splint before surgical management.

Anteroposterior radiograph of the patient in Fig. 3 immediately after rigid intramedullary nailing.
Clinical examinations, radiographs preoperatively and immediately postoperatively, at 6–12 weeks, and at the final follow-up were systematically analyzed. The mean follow-up time in elastic stable intramedullary nail (ESIN) group was 12 months and 10 months in rigid intramedullary nail (RIN) group. Clinical examinations included skin (wound, viability, and tension due to fracture dislocation), neurovascular status (dorsalis pedis and posterior tibial arteries, color of skin, capillary reaction; motor and sensory function of peroneal and tibial nerve), and signs of compartment syndrome (pain not responsive to opioids, passive lengthening of muscles, and active movement of lower leg muscles). Compartment syndrome was diagnosed based on clinical status.
Operative Methods
The RIN was inserted using the transligamentory approach. Two precontoured ESINs were inserted through two skin incisions made on the lateral and medial sides below the proximal tibia metaphysis (0.4× medullary canal). No tourniquet was used during intramedullary nailing.
Definitions
An acceptable postoperative alignment was defined as less than 5° of angulation in any direction, less than 10 mm shortening, and less than 10 mm dislocation. Significant lower limb length discrepancy was >10 mm. (13.) Malunion was defined as more than 5° of angulation in any direction, more than 10 mm shortening, or significant rotatory malalignment (>30°). When a patient did not demonstrate a three-cortex union at 16 weeks, a term delayed union was used.
Statistical Methods and Ethical Committee Approval
Mean values (standard deviation (SD)) are given. For incidence calculations, numbers (percentages) are reported. An X2-test was used for categorical comparisons. Ethical committee approval was granted by our university hospital. Due to the retrospective nature of the research, no informed consent was requested by the committee.
Results
Patient Characteristics
The mean age of the children undergoing elastic intramedullary nailing was significantly lower as compared with those undergoing rigid intramedullary nailing (mean age 11.47 years, SD 2.43 vs 15.02, SD 0.74, p < 0.001). Twenty-six patients (26/26, 100%) treated with flexible nail and 14 patients (14/30, 46.7%) treated with rigid nail had open proximal tibial physis (p < 0.001). Four (4/26, 15.4%) of the ESIN patients and 12 of the rigid population (12/30, 40%) had an open tibial fracture (p = 0.042). Four (4/26, 15.4%) of the ESIN group and 10 of the RIN group (10/30, 30%) developed compartment syndrome and required fasciotomy (p = 0.122). Of the fasciotomies, three fasciotomies in the ESIN group (3/4, 75%) and eight fasciotomies in the RIN group (8/10, 80%) were performed at the time of index surgery and the remainder as separate surgeries (see Table 1).
Clinical characteristics of the study groups.
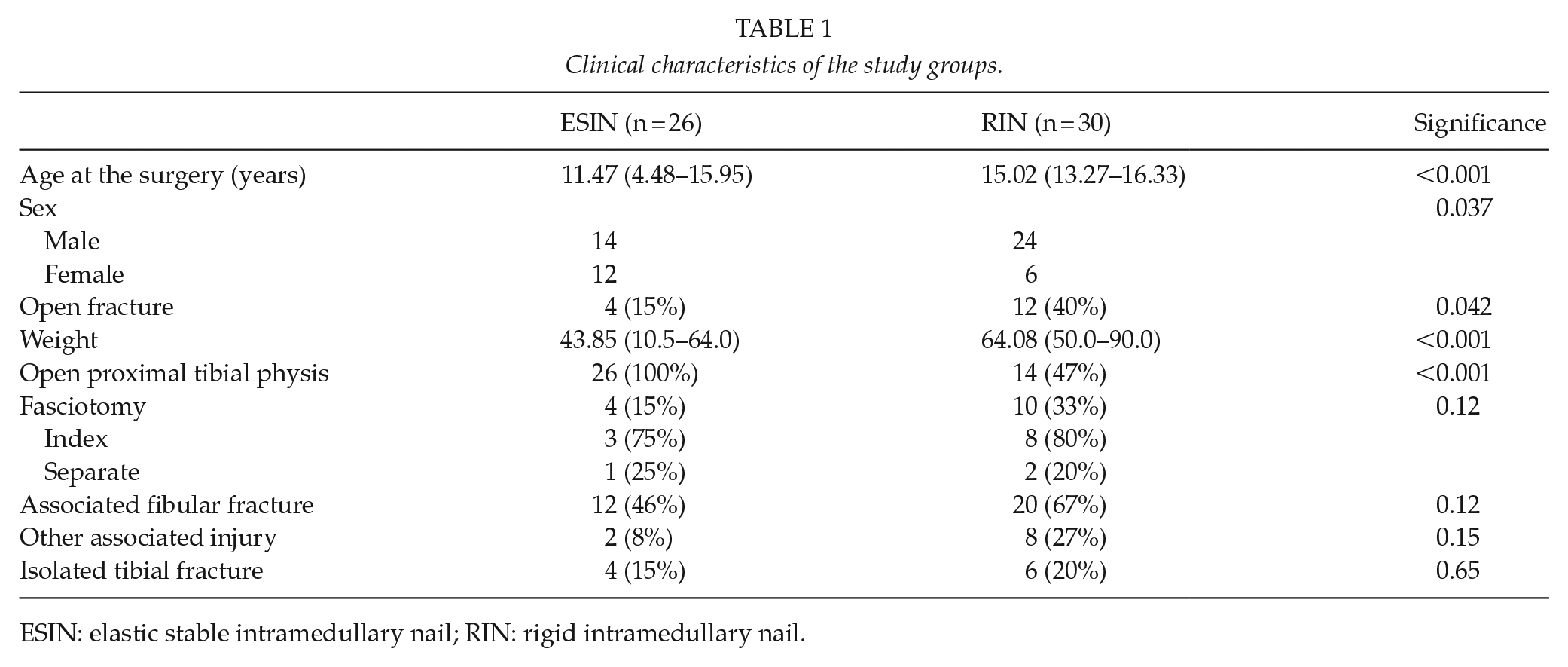
ESIN: elastic stable intramedullary nail; RIN: rigid intramedullary nail.
In the ESIN group, an associated fibular fracture was present in 12 cases (12/26, 46.2%) and 20 cases (20/30, 66.7%, p = 0.12) in the RIN group, respectively. Two patients (2/26, 7.7%) in the ESIN group had other associated injuries (metacarpal fracture and skin excoriation) and eight patients (8/30, 26.7%) in the RIN group; these injuries included the following: traumatic pneumothorax, rib fracture, vertebral fracture, talus fracture, metatarsal fractures, spleen rupture, rhabdomyolysis, and humeral fracture (p = 0.15). Four (4/26, 15.4%) patients in the ESIN group and six (6/30, 20%) patients in the RIN group had no associated injuries (p = 0.65). The mean operation time in ESIN patients was 1 h 23 min (SD 35 min, median 1 h 22 min) and in RIN patients 2 h 50 min (SD 1 h 17 min, median 2 h 15 min).
Radiographic Outcomes
An acceptable postoperative alignment was obtained in 20 patients (20/26, 76.9%) in the ESIN group and in 29 patients (29/30, 96.7%) in the rigid group (p = 0.026). The mean coronal angulation was 2.4° (SD 2.2) in ESIN group and 1.4° (SD 1.4) in RIN group (p = 0.07). The mean sagittal angulation was 3.4° (SD 2.9) in ESIN patients and 1.8° (SD 1.4) in RIN patients (p = 0.019). Of those not fulfilling the acceptable alignment, two patients in the ESIN group (2/6, 33.3%) and one patient in the RIN group (1/1, 100%) had a persisting coronal malalignment (varus or valgus angulation of more than 5°). The rest of the ESIN patients not fulfilling the acceptable alignment (4/6, 66.7%) had sagittal malalignment. In the ESIN population, all patients showed evidence of fracture healing within 16 weeks. In the RIN group, five patients (5/30, 17%, p = 0.029) had a delayed union during the follow-up and two of these patients (2/5, 40%) had dynamization as an additional surgery. Malunion occurred in six patients (6/26, 23%) in the ESIN group versus none of the patients treated with RIN (p = 0.005). Radiographic outcomes are shown in Table 2.
Radiographic outcomes of the study groups.
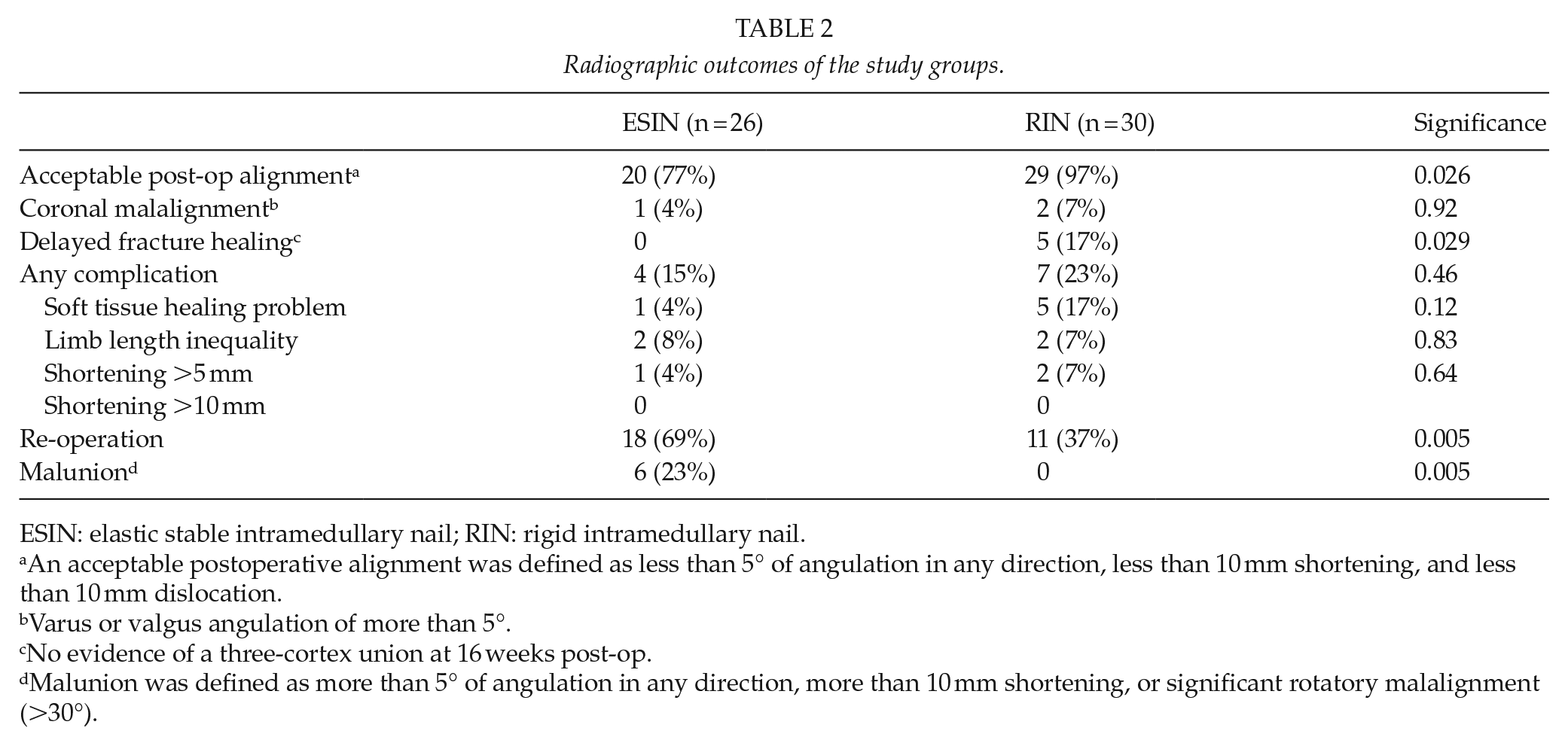
ESIN: elastic stable intramedullary nail; RIN: rigid intramedullary nail.
An acceptable postoperative alignment was defined as less than 5° of angulation in any direction, less than 10 mm shortening, and less than 10 mm dislocation.
Varus or valgus angulation of more than 5°.
No evidence of a three-cortex union at 16 weeks post-op.
Malunion was defined as more than 5° of angulation in any direction, more than 10 mm shortening, or significant rotatory malalignment (>30°).
Effect of Weight (<50 kg vs >50 kg)
Twelve patients treated with ESIN weighed <50 kg and eight patients >50 kg (five patients had no weight data). The mean weight of the patients was 43.9 kg (SD 13.20 kg). Of those not fulfilling the acceptable alignment, one patient aged 12 years and weighed >50 kg (1/6, 16.7%). No patient weighted less than 50 kg in the rigid population, and the mean weight was 64.1 kg (SD 11.84 kg). The mean weight of the ESIN group was statistically lower than that of the RIN group (p < 0.001).
Complications
Any complication occurred in four patients (4/26, 15%) in the ESIN population and seven patients (7/30, 23%) in the RIN population (p = 0.46). One patient (1/26, 3.8%) in the ESIN group and five patients (5/30, 17%) in the RIN group had soft tissue healing problems. Two ESIN patients (2/26, 7.7%) had limb length inequality as did two patients in the RIN group (2/30, 6.7%) at the end of the follow-up.
Eighteen patients in the ESIN group underwent nail removal (18/26, 69.2%). In the RIN group, re-operation was needed for 11 patients (11/30, 36.7%, p = 0.005; five dynamization, one nail removal, one skin graft, two fasciotomies, no re-nailing, and one proximal locking screw was placed through open proximal tibial physis and later needed repositioning to a lower position). One death occurred due to multi-organ failure after rigid intramedullary nailing. The nail removals were performed as planned surgeries.
Discussion
Rigid intramedullary nailing at the end of the growth period is not associated with a risk of clinically significant growth disturbance. Flexible intramedullary nailing does not provide similar control of the fracture alignment as rigid nailing does. Elastic nailing is one of the most commonly used fixation methods for pediatric long bone fractures, but it may result in non-union in older and heavier children (3, 11, 14).
Validity of the Data
This single-center study is limited due to its retrospective, non-randomized nature, and limited number of cases. A small number of patients (n = 4) were lost during follow-up, and the patients were not routinely followed until skeletal maturity. The radiographic quality of reduction and internal fixation was analyzed by an independent reviewer. Patients in the rigid intramedullary nailing group were significantly older and heavier than children in the flexible intramedullary nailing group.
Comparison with Previous Studies
Despite the many advantages of flexible intramedullary nailing, it does allow potential loss of reduction as compared with rigid nailing. In addition, a short period of immobilization is usually needed. In previous studies, the rate of delayed healing was shown to vary by around 10% (4, 15). Gordon et al. found that patients with delayed union were older (14.1 years) than their study population as a whole (11.7 years), and they concluded the lack of stability to be the key factor behind the delayed healing (11.) Court-Brown et al. reported a series of 36 adolescents with tibial fractures and open proximal physes treated with reamed intramedullary nailing. There were no long-term complications associated with the injury to their proximal tibial physes and no malunions (16.)
There are no previous comparative studies evaluating the outcomes of flexible versus rigid intramedullary nailing in children with open tibial physis. In this study, rigid intramedullary nailing controlled the fracture alignment significantly better than flexible intramedullary nailing and was not associated with a risk of growth disturbance. We hypothesize that adolescents with an open physis may undergo rigid intramedullary nailing as the smooth nail fills the entry point through the physis and continued growth is possible.
Conclusion
Younger children with tibial fractures who weight 50 kg or less and with proximal tibial growth plates wide open can be treated with elastic stable intramedullary nailing while more mature adolescents benefit from rigid intramedullary nailing as rigid nailing allows more precise fracture alignment without increased risk of growth disturbance.
Footnotes
Author Contributions
S.W.-K. contributed to the data acquisition, analysis, and interpretation of data. I.H. contributed to study design, data analysis, and interpretation of data. Both the authors contributed to drafting and critical revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I.H. is the consultant for Medtronic.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.