
Abstract
Background and Aims:
Blunt abdominal trauma can lead to substantial organ injury and hemorrhage necessitating open abdominal surgery. Currently, the trend in surgeon training is shifting away from general surgery and the surgical treatment of blunt abdominal trauma patients is often done by sub-specialized surgeons. The aim of this study was to identify what emergency procedures are needed after blunt abdominal trauma and whether they can be performed with the skill set of a general surgeon.
Materials and Methods:
The records of blunt abdominal trauma patients requiring emergency laparotomy (n = 100) over the period 2006–2016 (Helsinki University Hospital Trauma Registry) were reviewed. The organ injuries and the complexity of the procedures were evaluated.
Results:
A total of 89 patients (no need for complex skills, NCS) were treated with the skill set of general surgeons while 11 patients required complex skills. Complex skills patients were more severely injured (New Injury Severity Score 56.4 vs 35.9, p < 0.001) and had a lower systolic blood pressure (mean: 89 vs 112, p = 0.044) and higher mean shock index (heart rate/systolic blood pressure: 1.43 vs 0.95, p = 0.012) on admission compared with NCS patients. The top three NCS procedures were splenectomy (n = 33), bowel repair (n = 31), and urinary bladder repair (n = 16). In patients requiring a complex procedure (CS), the bleeding site was the liver (n = 7) or a major blood vessel (n = 4).
Conclusion:
The majority of patients requiring emergency laparotomy can be managed with the skills of a general surgeon. Non-responder blunt abdominal trauma patients with positive ultrasound are highly likely to require complex skills. The future training of surgeons should concentrate on NCS procedures while at the same time recognizing those injuries requiring complex skills.
Keywords
Introduction
One of the key requirements in managing blunt trauma patients is to control major hemorrhage before the development of coagulopathy, which is associated with increased mortality (1). Commonly, significant and sometimes fatal sources of bleeding after high-energy trauma are located in the abdomen (2), warranting rapid and determined actions during trauma laparotomy (3).
With the increasing fragmentation and sub-specialization in surgical training—at least in Europe and Nordic countries—the overall expertise and experience in managing complex and multiple abdominal organ injuries has diminished. In most non-trauma centers, blunt abdominal trauma (BAT) following abdominal organ injuries is managed by elective surgery-oriented visceral and vascular surgeons and not by more broadly trained general surgeons as in the past (4). This poses challenges to the in-house surgeon on call, not just in operative management but also decision-making. Indications for emergency laparotomy at initial presentation include hemodynamic instability with evidence of intra-abdominal bleeding, peritoneal signs, and diaphragmatic tears (5). In addition, intraoperative decision-making in selecting the appropriate strategy—damage control or definitive repair—requires experience. Rapid control of bleeding and contamination can save valuable time, prevent physiological exhaustion, and sometimes decrease the risk of coagulopathy (6).
Recently, based on a pilot randomized controlled trial, Harvin et al. (7) suggested a more limited role for damage control laparotomy in BAT patients. Previous studies have shown the association between specific abdominal injuries and outcome, but there is little research on the ability of general surgeons to perform emergency laparotomy procedures with the same efficiency and safety as organ-specific surgeons. In patients with penetrating thoracic injuries, the general surgeon can manage life-threatening situations by means of simple procedures (8).
As general surgical techniques seem to be shifting to more specific sub-specialties, courses such as Definitive Surgical Trauma Care (DSTCTM) teach the basic principles and skills of emergency laparotomy, which are mainly needed during the acute phase to control intra-abdominal bleeding and leakage of bowel content. These procedures have previously been classed as either non-complex or complex skills depending on the surgical expertise needed, for example, hepatic procedures such as simple perihepatic packing versus vascular isolation, anatomical lobectomy, or even orthotopic liver transplantation (9).
The aim of this study was to identify the emergency procedures needed in BAT patients in the European trauma setting. We hypothesized that the evaluation and treatment of different intra-abdominal injuries could be carried out by a general surgeon with non-complex surgical skills and a sub-specialized organ surgeon with complex surgical skills is rarely needed.
Methods
In this retrospective study, each patient case was manually reviewed for inclusion and evaluation. We identified patients entered in the trauma registry of Helsinki University Hospital (Helsinki Trauma Registry (HTR)). The hospital’s catchment area is nearly 2 million, and between 1 January 2006 and 31 December 2016, the number of blunt trauma patients aged over 16 with a New Injury Severity Score (NISS) (10) of over 15 was 4146. From this population, we included patients with open abdominal surgery (Nordic Medico-Statistical Committee (NOMESCO) “J” and “K” procedures) within 24 h after injury (11). Based on surgery reports, we excluded patients as follows: laparotomy due to diversion stomas (n = 5), decompressive laparotomy due to major retrohepatic hematoma without other interventions (n = 1), and negative explorative laparotomy (n = 1).
Procedures calling for “complex skills” were defined based on the extent of surgical experience needed in emergency laparotomy, that is, where the skills of a general surgeon would probably be insufficient, and the expertise of an organ-specific surgeon would be required (Fig. 1). According to Ahmed and Vernick (9), these procedures were specified as major hepatic resection, juxtahepatic venous repair, and access and/or repair of major vascular injuries including supraceliac aortic clamping, proximal parts of the superior mesenteric artery and vein, abdominal aorta, inferior vena cava (IVC), portal vein, and common and internal iliac arteries and veins (Fig. 2). Thus, based on surgical reports, each procedure during emergency laparotomy was evaluated as either “need for complex skills” (CS) or “no need for complex skills” (NCS). Hemodynamic status at initial resuscitation was described as follows: responder (increased and sustained blood pressure after fluid bolus), transient (increased blood pressure, followed by recurrent hypotension after fluid bolus), or non-responder (no improvement in blood pressure after fluid bolus). The administrative board of HTR approved this study, which is in accordance with the Declaration of Helsinki. Statistical analysis was performed using SPSS version 25 (IBM, New York, United States). The normality of the variables was tested and presented as means, and ranges were calculated from the variables. One-way analysis of variance (ANOVA) was used to investigate differences between CS and NCS groups.
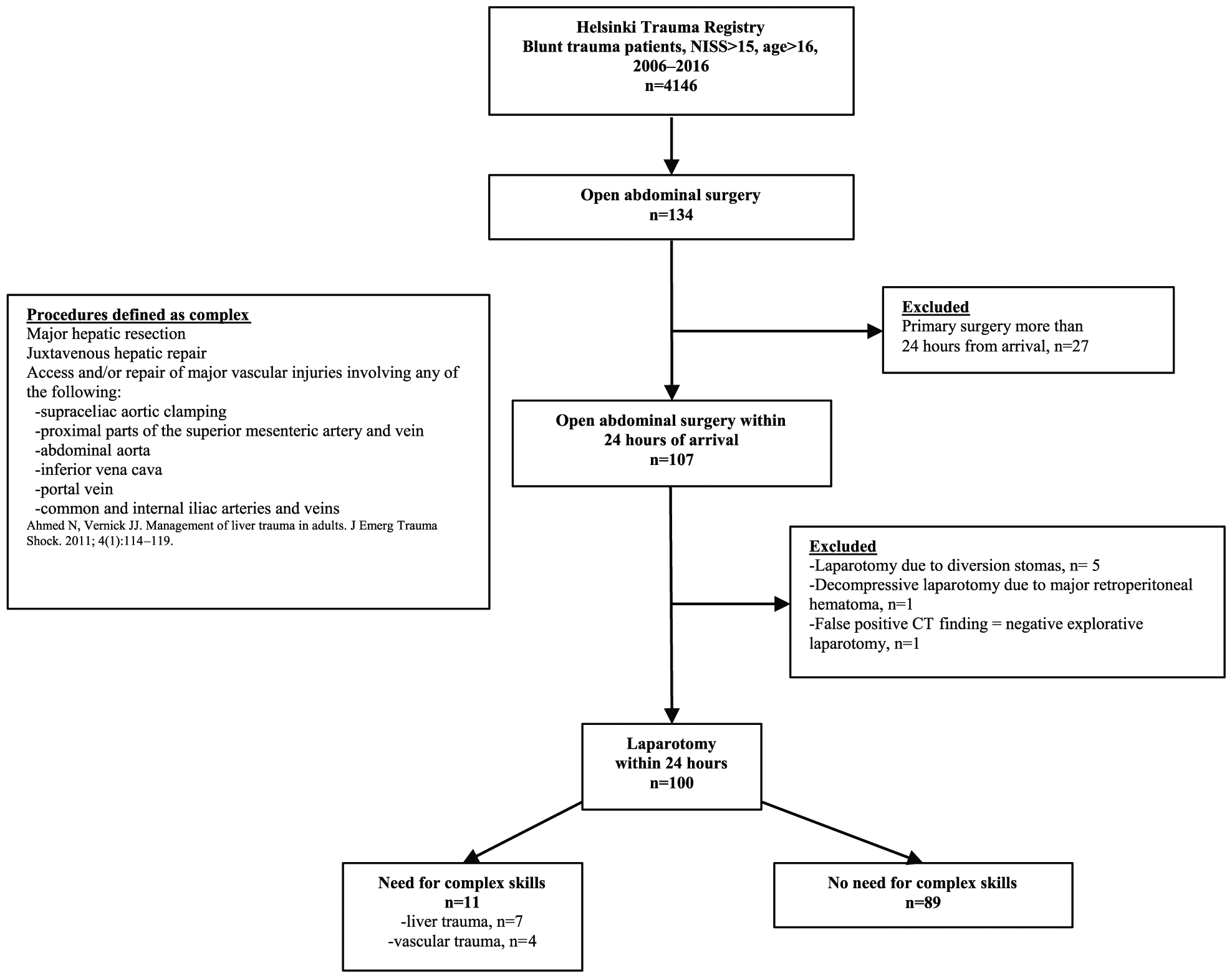
Flowchart of the study cohort.
Severe blunt upper abdomen injury involving the liver and root of the superior mesenteric artery.
Results
The basic characteristics of the BAT patients are shown in Table 1. Altogether 100 (CS = 11, NCS = 89) emergency laparotomies were performed during the study period. The Injury Severity Scores (ISS) and NISS were higher (48.4 and 56.4) in the CS group than in the NCS group (31.5 and 35.9; p < 0.001 in both). The main reason for the blunt abdominal injuries was high-energy trauma, with motor vehicle accidents (MVAs) including motorcycle accidents (MCAs) accounting for 51 (51%) of all injuries. The CS group had a lower systolic blood pressure (mean 89 vs 112, p = 0.044) and higher mean shock index (heart rate/systolic blood pressure: 1.43 vs 0.95, p = 0.012) on admission compared with the NCS group. The CS group had 8 (73%) non-responder patients compared with 32 (36%) in the NCS group, and a shock index of over 0.9 was more prevalent in the NCS group—the differences, however, were not statistically significant. Perioperative mortality in the CS group was 7/11 (64%) and in the NCS group 2/89 (2%) due to exsanguination, while total mortality was perioperatively 10 (10%) and postoperatively 9 (9%) in the whole study population (Table 1).
Basic patient characteristics and hemodynamic status on arrival.
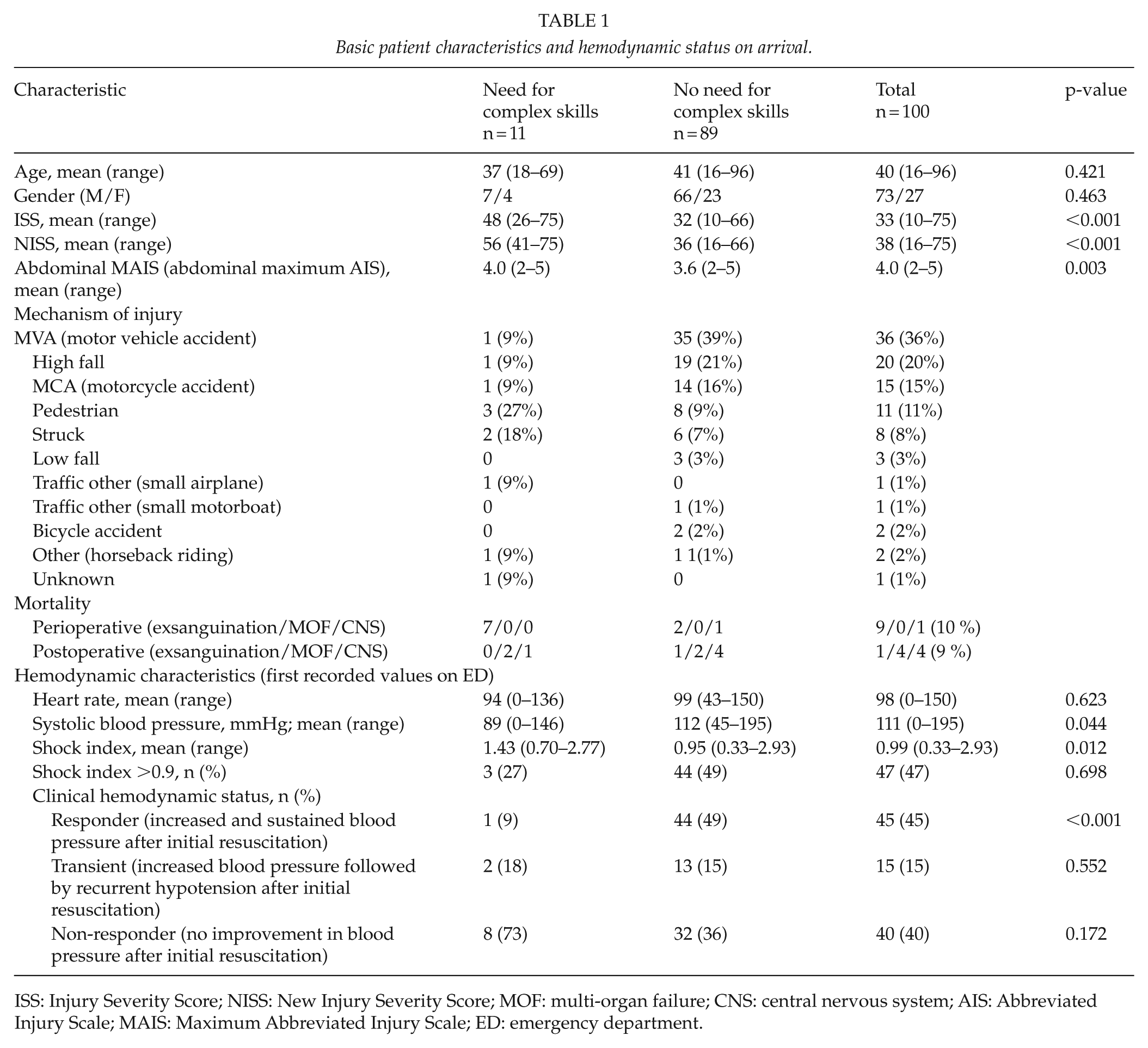
ISS: Injury Severity Score; NISS: New Injury Severity Score; MOF: multi-organ failure; CNS: central nervous system; AIS: Abbreviated Injury Scale; MAIS: Maximum Abbreviated Injury Scale; ED: emergency department.
Table 2 shows the reasons for emergency laparotomy. Patients with hemodynamic instability with positive ultrasound (US) findings without computed tomography (CT) underwent 14 explorative laparotomies (CS, n = 5, 45%; NCS, n = 9, 11%). Based on the CT finding laparotomy was performed on 6 (54%) patients (5 unstable, 1 stable) in the CS group and on 67 (75%) in the NCS group. Altogether eight stable patients underwent laparotomy due to clinical signs (NCS: peritonistic n = 6, elevated intra-abdominal pressure (IAP) n = 2) with CT not indicating laparotomy.
Reason for emergency laparotomy, n (%).
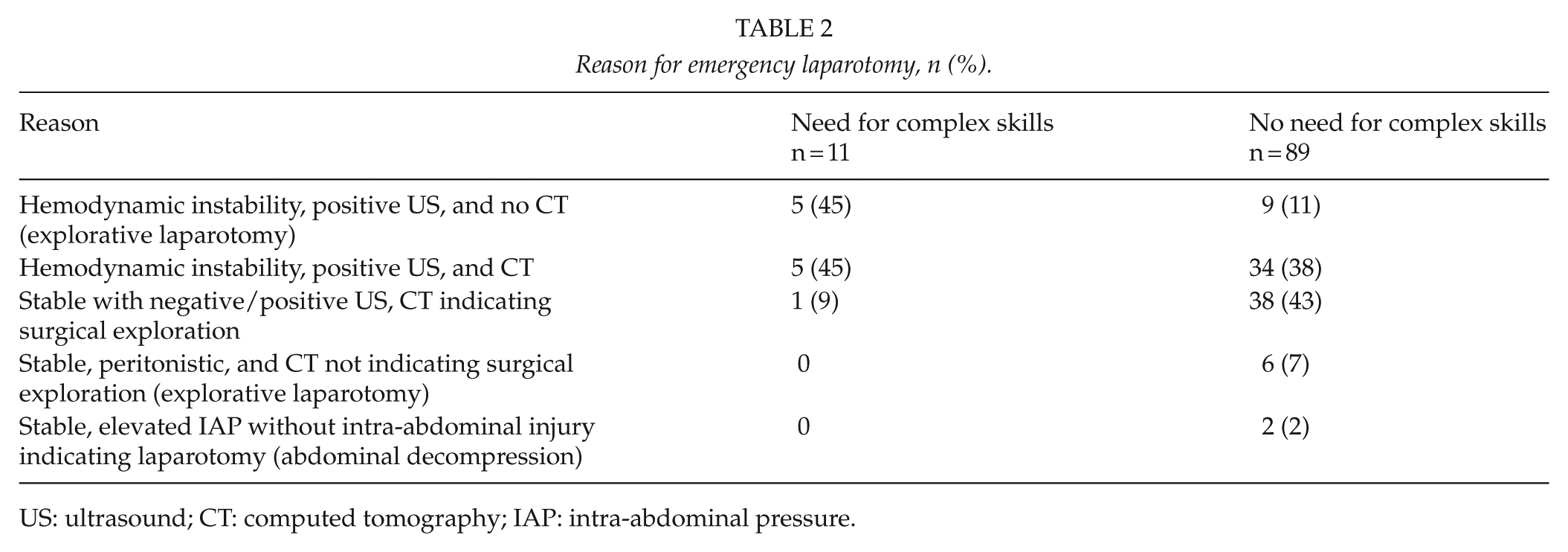
US: ultrasound; CT: computed tomography; IAP: intra-abdominal pressure.
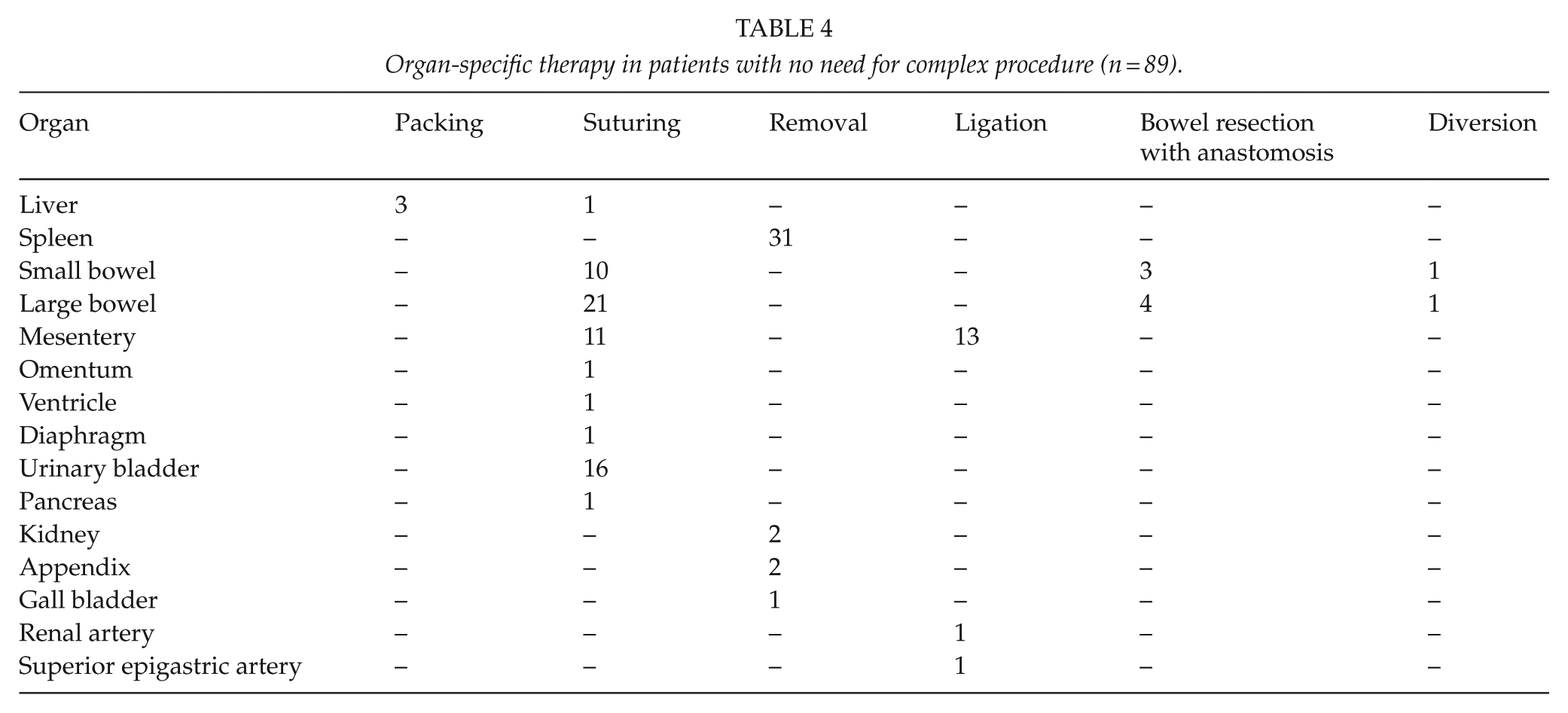
Of the 11 patients requiring a complex procedure, the bleeding site was either the liver (n = 7, 64%) or a major blood vessel (n = 4, 36%; Table 3). The mean Organ Injury Score (OIS) based on the American Association for the Surgery of Trauma (AAST) classification was 4.6 (range 3–5). Table 3 presents the complex procedures together with the detailed site of injury. Non-complex procedures performed on laparotomy are shown in Table 4.
Injury and surgical procedure characteristics of patients needing complex skills (n = 11).
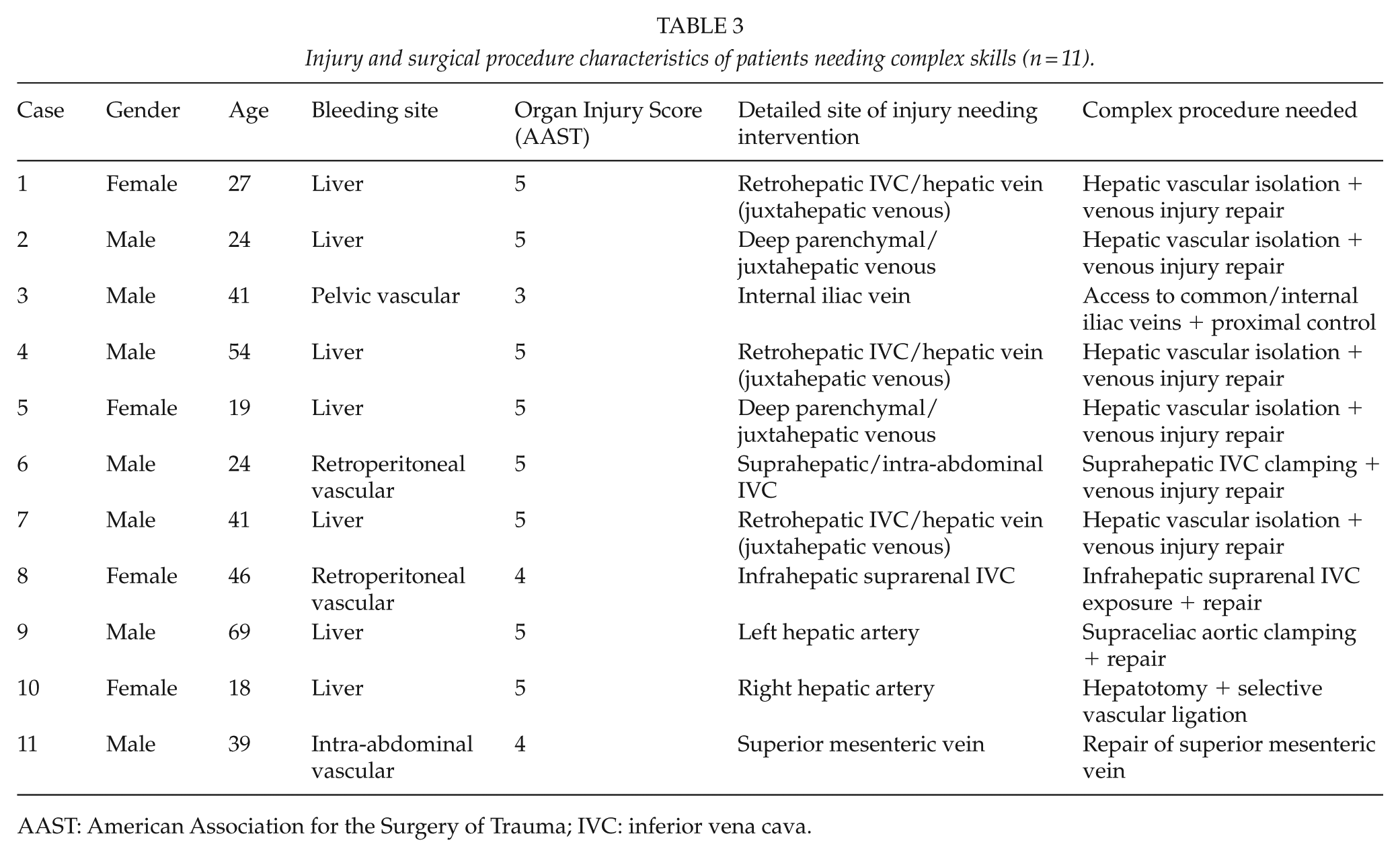
AAST: American Association for the Surgery of Trauma; IVC: inferior vena cava.
Organ-specific therapy in patients with no need for complex procedure (n = 89).
Discussion
This study presents findings and procedures performed in emergency laparotomies after BAT in a European tertiary-level trauma center. Our findings demonstrate that during open abdominal surgery after BAT most of the surgical skills required are non-complex and thus fall within the skill set of general surgeons. Complex procedures seem to be needed in major liver or vascular injuries, which carry a high risk of mortality to begin with. Doll et al. (8) have demonstrated similar results with penetrating thoracic trauma patients: they concluded that an acute life-threatening trauma can usually be managed with non-complex thoracic surgery skills. The results of this study show that this also applies to BAT patients.
According to the literature, high-energy trauma—especially MVAs—can cause BAT requiring open abdominal laparotomy (12). This was also seen in our data. Furthermore, when comparing the severity of injuries, the CS group had significantly higher ISS, NISS, and Maximum Abbreviated Injury Scale (MAIS) than NCS, which is in line with earlier finding of Krige et al. (13). The CS procedure patients died as a result of exsanguination while the deaths of the NCS patients were recorded as being due to multi-organ failure (MOF) or trauma of the central nervous system (CNS). These findings highlight the need for rapid control of hemorrhage, which can lead to fatal coagulopathy in BAT patients with CS-requiring injury.
The onset of coagulopathy related to massive hemorrhage after trauma has a major role in perioperative or postoperative mortality (14). In BAT, parenchymal organ injuries or vascular trauma pose an elevated risk of death due to hemorrhage, which should be dealt with promptly by the on-call surgeon (15). In this study, the patients who needed a CS procedure were usually non-responders on arrival, and as Ahmed and Vernick concluded (9), CS procedures need surgeons with sub-specialty skills. Therefore, the on-call physician should pay special attention to hemodynamically non-responder BAT patients as they could require an urgent CS procedure done by an expert surgeon. Our data show that half of the NCS group were responders, whereas transient responders may not be determined as needing CS or NCS based on hemodynamic stability on arrival. In addition, hemodynamic instability could be a sign of a high-grade organ injury. In this study, 8 out of 100 would require CS, whereas 36 of non-responder patients had injuries that could be managed by a general surgeon (NCS).
Hemodynamic status is the major focus in decision-making when treating BAT patients (16). In this study, CS group patients were more hemodynamically unstable than NCS group patients. All CS group patients except one underwent US but were given no CT scan preoperatively, whereas in the NCS group more CT scans were used to guide the treatment. Thus, it seems that complex procedures are not only difficult to perform but cannot be thoroughly planned due to limited preoperative imaging. Interestingly, only two patients had an elevated IAP without any imaging findings indicating the need for laparotomy within 24 h of arrival. This is fewer than previous studies have reported (17).
According to AAST, a high-grade liver injury predicts poor survival (18). After evaluating the detailed site of injury needing surgical intervention, liver injuries associated with hemodynamic instability were the most common (19). In addition to liver injuries, 36% of the CS patients had major vascular injuries. Interestingly, all of these vascular injuries were classified as venous injuries. The sites of venous injuries needing a CS procedure were major vessels due to difficult surgical access and fragility of the vascular structure.
The main site of bleeding in NCS patients was the spleen, which was generally treated by simple splenectomy. Similarly, simple saturation of the urinary bladder, saturation of serosal defects of the small and large bowel, and ligation of mesentery were performed in treating BAT patients. All these skills should be within the capability of a general surgeon (20, 21).
The aim of this study was not to focus on the surgical treatment of intra-abdominal injuries but to analyze the nature and severity of the injuries observed in emergency laparotomies after blunt injury, and to assess the level of surgical experience needed to treat these injuries in an initial laparotomy. Endovascular trauma management has been evolving in recent years and is providing new ways to treat acute trauma patients. New treatment facilities are mostly equipped with hybrid trauma management facilities which are capable of rapid endovascular management. Thus, in these facilities, some of the patients operated due to bleeding can, in the future, be treated without open surgery and this could reflect in the proportion of patients needing open surgery. Simple follow up with monitoring the patients can be used with stable patients without any other reasons for operative treatment (22). However, BAT patients have high amount of concomitant injuries—such as bowel injuries—requiring surgical interventions which should be taken in consideration when deciding the correct treatment for BAT patient.
In this study, we observed a high intraoperative mortality rate related to juxtahepatic liver injuries. In temporary bleeding control of such injuries, the possibilities provided by ECMO (extracorporeal membrane oxygenation) and new and developing endovascular techniques, such as retrievable covered caval stent grafts allowing free flow and endovascular occlusion balloons, will very likely become part of novel treatment protocols. The increasing use of endovascular trauma management will further emphasize the role of education, training, and team work between different medical specialties.
In the era of surgical sub-specialization (23, 24), where a single-organ surgeon does not operate on acute trauma patients on a daily basis, such surgeons should receive training from different surgical fields to equip them to act in emergency situations. The findings of this study highlight the injuries involved and the skills a surgeon should possess to be able to treat hemodynamically stable or unstable BAT patients. Although our study has limitations—such as its retrospective design—the data gathered from our tertiary-level trauma center show how the general surgeon can handle most of the procedures needed during emergency open abdominal surgery. In future, trauma surgery training should emphasize the general surgeon skills mentioned above and provide the physician with tools for decision-making and recognizing an acute situation where a procedure requiring CS should be performed in which sub-specialty surgery is mandatory.
Conclusion
Based on our data, the majority of patients requiring open abdominal surgery within 24 h of arrival can be managed by a general surgeon. Non-responder BAT patients with positive US are highly likely to require CS. The future training of trauma surgeons should concentrate on NCS procedures while at the same time recognizing injuries requiring CS.
Footnotes
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.