
Abstract
Introduction:
Incisional hernia is common after abdominal surgery. Watchful waiting carries the risk of incarceration and a need for emergency intervention. The aim of this study was to examine the risk of postoperative complications after emergency versus elective incisional hernia repair.
Methods:
Patients above 18 years of age undergoing open incisional hernia repair in Denmark in 2017–2018 were identified in the Danish Ventral Hernia Database. Patients were grouped according to elective or emergency hernia repair. The primary outcome was postoperative complications requiring operative intervention within 90 days, and the secondary outcome was postoperative length of stay.
Results:
We included 1050 patients, of whom 882 were admitted for elective and 168 for emergency operation. Patients undergoing emergency repair were older (64.7 years vs 59.2 years, p < 0.001), more often smokers (25.8% vs 13.6%, p = 0.003), and more often had a Charlson comorbidity score ⩾2 (26.8% vs 19.2%, p = 0.005) compared to patients undergoing elective repair. In a multivariate regression analysis, emergency compared to elective operation (OR = 2.71, 95% CI = 1.4–5.25, p = 0.003) and retromuscular compared to onlay mesh placement (OR = 2.14, 95% CI = 1.08–4.24, p = 0.013) were factors significantly associated with increased risk of postoperative complications. In a subgroup analysis including only emergency repairs, risk of complications after retromuscular mesh placement was even higher (OR = 10.12, 95% CI = 1.81–56.68, p = 0.008).
Conclusion:
Emergency incisional hernia repair was associated with increased risk of postoperative complications and this risk was accentuated with retromuscular mesh placement. The use of retromuscular mesh in the emergency setting should be avoided, and the abdominal wall could either be closed by sutures or additional onlay mesh.
Keywords
Introduction
Incisional hernia is common among patients after major abdominal surgery and affects 20%–30% of all patients undergoing midline laparotomy (1–3). Incisional hernia affects quality of life (4,5) and on a longer term there is risk of strangulation, acute bowel obstruction, and incarceration (6). Retromuscular mesh placement and a tension-free closing of the abdominal wall is today’s golden standard for repair of incisional hernias. The open procedure is commonly known as the Rives–Stoppas procedure, and various moderations over this procedure exist (7).
Incisional hernia repair is however not without risks of morbidity and recurrence (8,9). Because of this, watchful waiting is a common clinical praxis when dealing with symptom-free patients and appears to be safe in many cases (10). Certain factors, such as age, female gender, and hernia size, have been shown to affect the risk of emergency incisional hernia repair (11).
Planned elective surgery is preferable in most surgical settings, and our hypothesis for the current study was that this statement also accounts for incisional hernia repair.
The primary aim of this study was to evaluate the postoperative outcomes after elective and emergency open incisional hernia repair on a nationwide basis. Second, we sought to assess factors associated with a poor postoperative outcome after emergency repair.
Methods
Surgeons in Denmark have been reporting data on incisional hernia operations to the Danish Ventral Hernia Database since 2007 (12). The database contains information on hernia type and size, repair method including the use of mesh, and layer for mesh placement. The database also contains data on the type of admission, whether this was elective or emergency surgery. Furthermore, data on smoking status, height, and weight have been reported to the database since 2017 (12).
Smoking and obesity are known factors to increase morbidity and mortality in hernia patients, and these factors are therefore relevant to take into account when assessing the risks of postoperative complications (13).
The Danish National Patient Registry is a nationwide database including all patients’ encounters with the public healthcare system. By using each patient’s unique personal identification number, data from the Danish Hernia Database and the Danish National Patient Registry were merged, giving information on readmission diagnoses, reoperation codes, and comorbidity status (12).
Only patients above 18 years of age were included; furthermore, in order to adjust for smoking and obesity, we only included patients operated in the period 2017–2018. Patients operated using minimally invasive techniques, here under laparoscopic approach, were excluded in order to ensure a homogeneous population.
Smoking was registered as current smoking at the time of admission. Previous smoking was not available from the database. Body mass index (BMI) was calculated from height and weight, and categorized as <25, 25–30, and >30 kg/m2, respectively. Obesity was defined as a BMI > 30 kg/m2. Charlson comorbidity index (CCI) was calculated based on concurrent diagnoses and categorized in groups depending on score of 0, 1, or ⩾2 (14).
The primary outcome of this study was reoperation within 90 days, and the secondary outcomes were time to hospital discharge and rate of readmissions. To examine potential predictors of adverse outcomes after emergency hernia repair, we performed a subgroup analysis of only patients undergoing emergency operation.
Statistics
Binary variables are presented in numbers with percentages, continuous variables as median with standard deviation (SD). Groups were compared with chi-square test and Student’s t-test.
First, a multivariate logistic regression analysis was done in the entire study population. Variables adjusted for were selected a priori on the basis of existing literature: age, BMI, CCI, smoking, mesh placement, and finally status as either elective or emergency operation.
Second, another multivariate logistic regression analysis was done, as a subgroup analysis, this time only on the emergency patients, including all of the variables above. Patients with missing values were included in the model.
All analyses were performed with R (version 3.2; R Foundation for Statistical Computing, Vienna, Austria). P-values less than 0.05 were considered statistically significant.
The study was approved by the Danish Data Protection Agency (Journal No. VD-2018-354, I-Suite: 6599).
Results
A total of 1050 patients underwent open incisional hernia repair in the period 1 January 2017 to 31 December 2018, of which 882 (84%) were elective and 168 (16%) emergency procedures. The mean age of patients undergoing emergency repair was significantly higher than patients undergoing elective repair (64.7 years vs 59.2 years, p < 0.001). The hernia defect was longer in the emergency group (10.8 cm vs 8.7 cm, p = 0.04), whereas the width of the defect was comparable.
More patients undergoing emergency repair were active smokers (25.8% vs 13.6%, p = 0.003) and had higher comorbidity with CCI > 2 (26.8% vs 19.2%, p = 0.005) compared to patients undergoing elective repair (Table 1).
Demographic data on patients undergoing open incisional hernia repair in Denmark from January 2018 to December 2019.
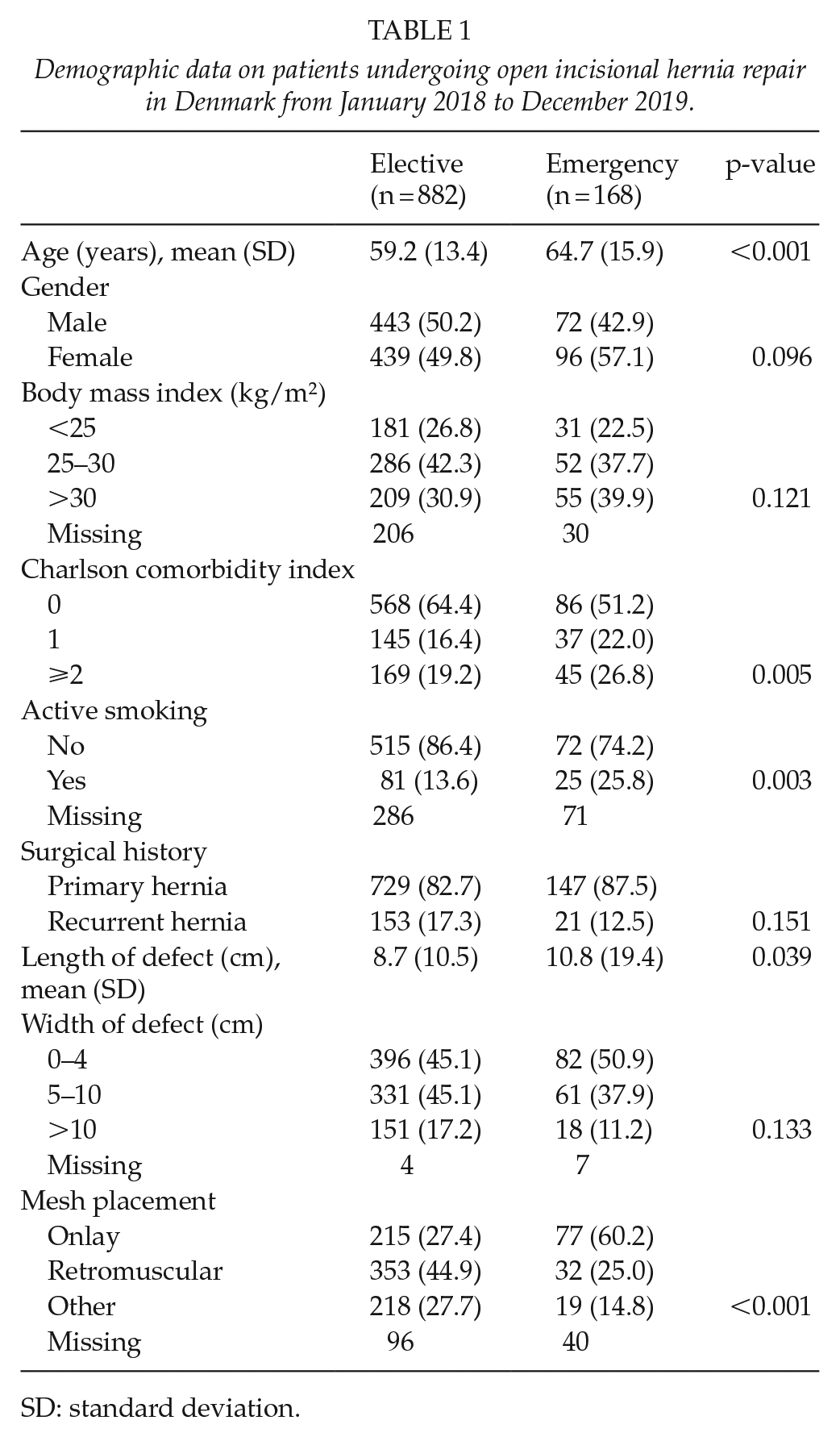
SD: standard deviation.
Emergency repair was associated with longer length of stay (8.5 days vs 3.6 days, p < 0.001), a higher incidence of readmissions (26.2% vs 17.5%, p = 0.011), and reoperations (28.0% vs 12.7%, p < 0.001) compared to elective repair. Most postoperative complications were registered as superficial wound infections, and this more often occurred in emergency hernia repair (10.7% vs 4.2%, p < 0.001) (Table 2).
Outcomes of patients undergoing open incisional hernia repair in Denmark from January 2018 to December 2019.
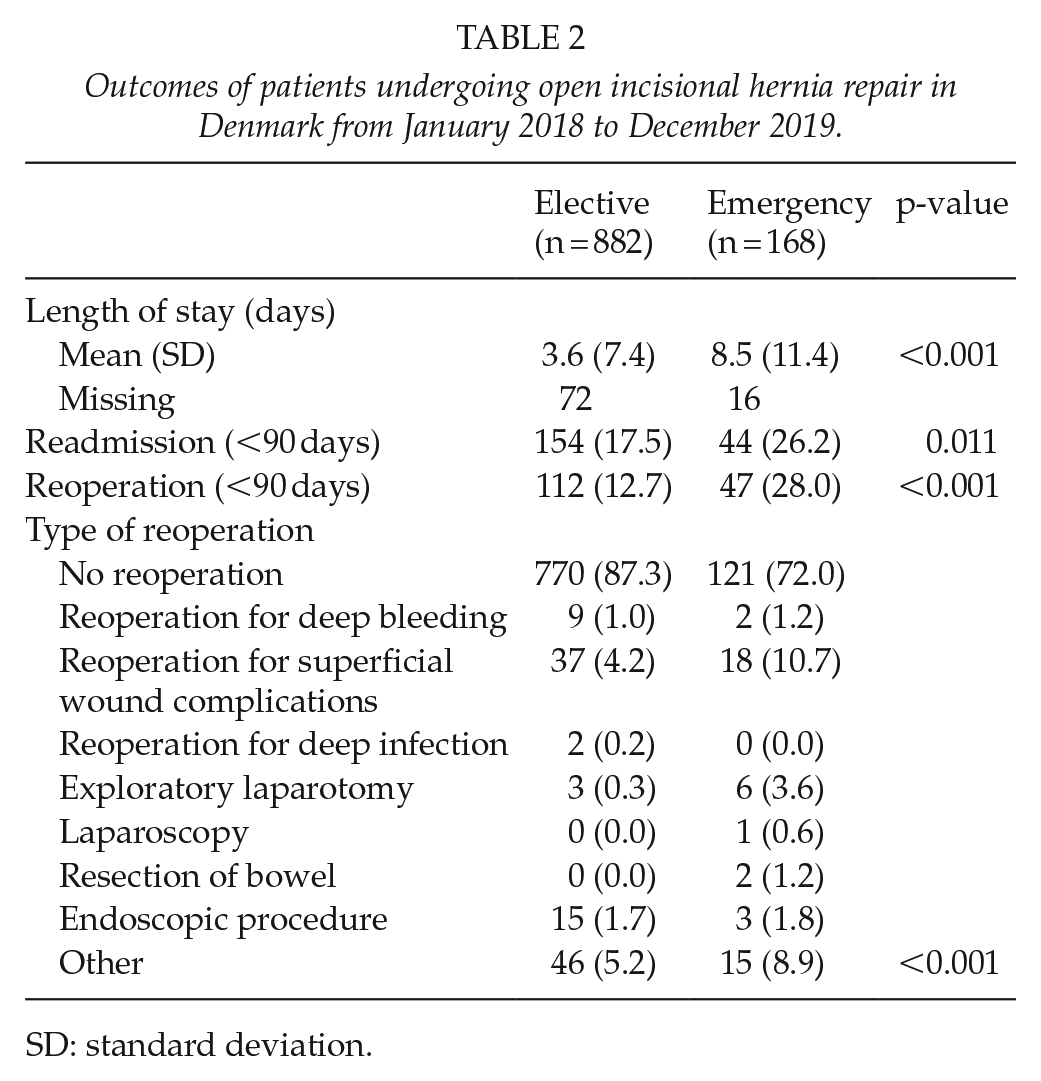
SD: standard deviation.
In the multivariable regression analysis, we found that emergency was associated with a significantly increased risk of 90-day reoperation (OR = 2.71, 95% CI = 1.4–5.25, p = 0.003) compared to elective operation. Other variables associated with an increased risk of reoperation were CCI > 2 (OR = 1.93, 95% CI = 1.13–3.31, p = 0.016) and retromuscular mesh placement (OR = 2.14, 95% CI = 1.08–4.24, p = 0.029) (Table 3).
Multivariate logistic regression model on reoperation within 90 days after open incisional hernia repair in Denmark from January 2018 to December 2019.
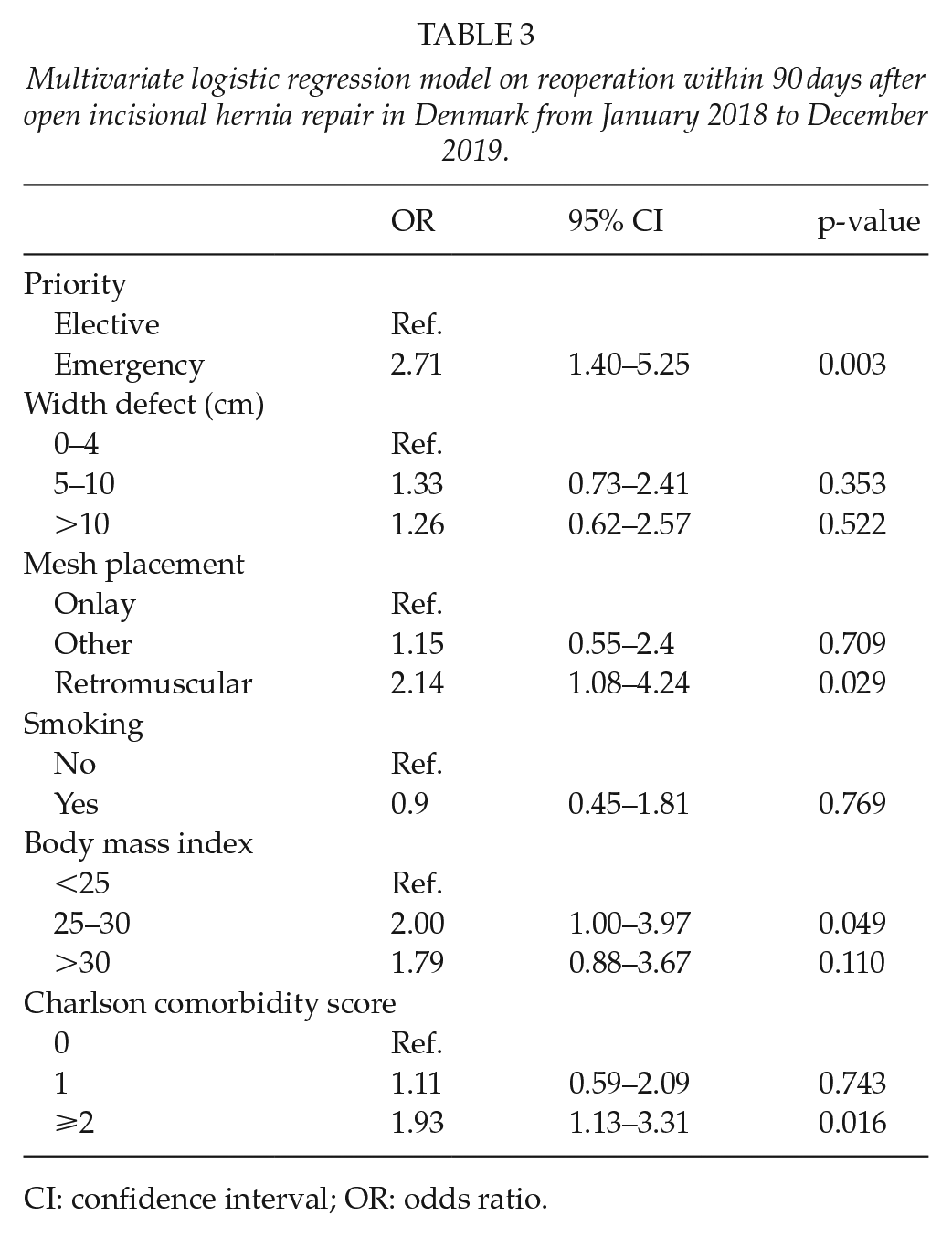
CI: confidence interval; OR: odds ratio.
Subgroup Analysis of Patients Undergoing Emergency Repair
The subgroup analysis of patients undergoing emergency repair yielded similar results, but with a significantly increased risk of reoperation in patients with retromuscular mesh placement (OR = 10.12, 95% CI = 1.81–56.68, p = 0.008) compared to mesh placement in the onlay position (Table 4).
Subgroup analysis: multivariate logistic regression model on reoperation within 90 days after emergency open incisional hernia repair in Denmark from January 2018 to December 2019.
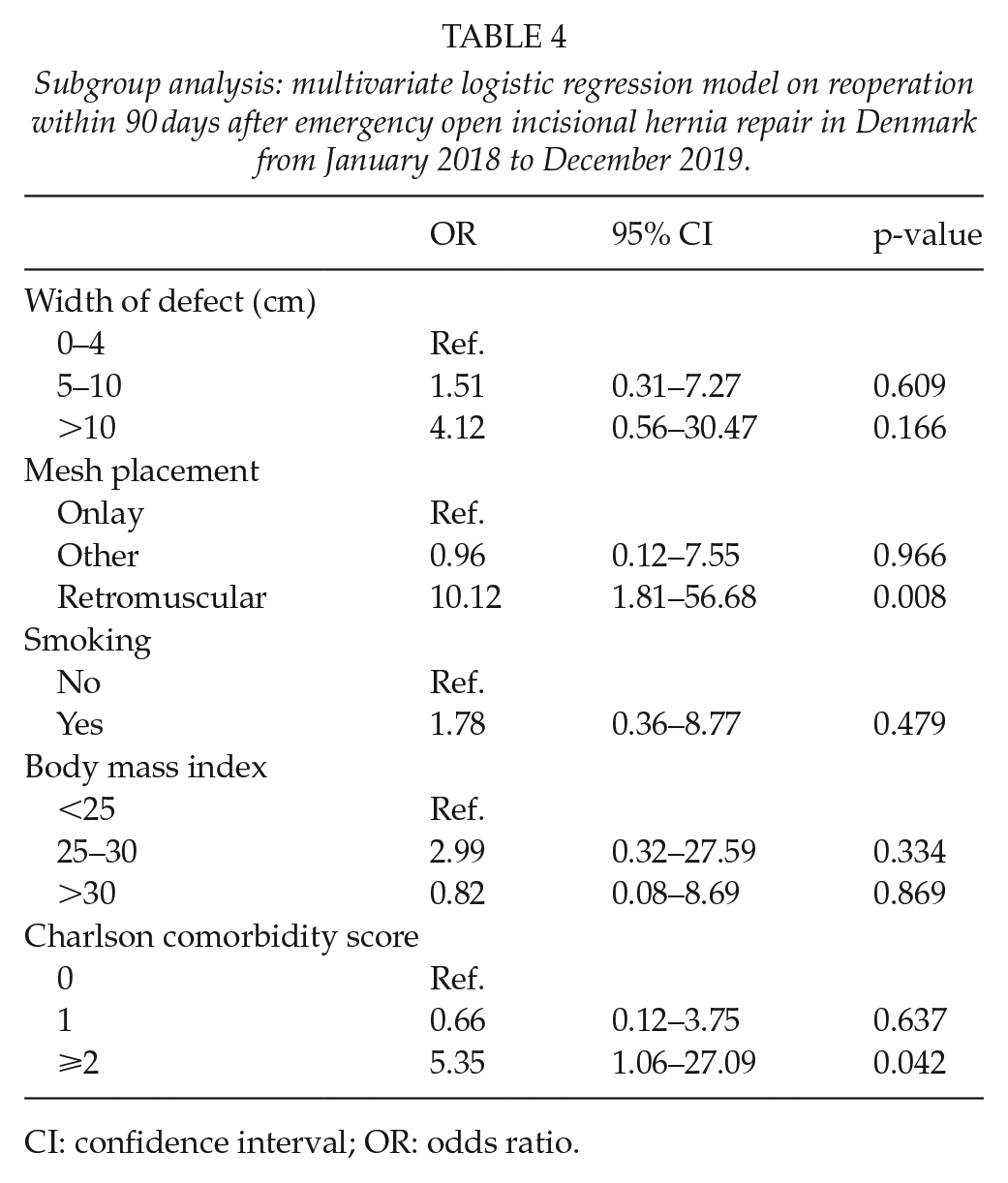
CI: confidence interval; OR: odds ratio.
Discussion
In the current nationwide study, we found an increased risk of postoperative complications after emergency repair compared to elective open incisional hernia repair. Retromuscular mesh placement was also significantly associated with increased risk of postoperative complications, and this association was found to be even stronger in a subgroup analysis of patients undergoing emergency repair. From the results of the subgroup analysis, it is feasible to deduct that the increased risk of reoperation associated with retromuscular mesh placement in the total population was indeed driven by reoperations in the emergency group.
The reason for an increased risk of complications after emergency repair probably is due to small bowel obstruction caused by hernia incarceration, concomitant bowel resection, derangement of electrolytes, and postoperative bowel paralysis. Furthermore, emergency hernia repair may be performed by surgeons with expertise in other areas than abdominal wall surgery, which may influence the outcome.
Previous studies have demonstrated poor outcomes of emergency incisional hernia repair compared to planned elective surgery (8,15,16). In a 2013 cohort study, using data from the Danish Hernia Database on patients with incisional hernias undergoing surgery in the period 2007–2010, Helgstrand et al. (11) found an increased rate of 30-day reoperation in emergency repair compared to elective repair, and these results correspond well with the findings of the present study. Helgstrand et al. furthermore found that female gender, increasing age, and hernia defect <7 cm were all independent risk factors for emergency operation. Data on smoking and obesity were not available from the Danish Hernia Database at the current time.
An American single-center cohort study from 2014, including 497 patients undergoing ventral hernia repair, found no significant differences in postoperative complications between emergency and elective repairs after adjusting for comorbidities. The authors argue that postoperative complications in emergency surgery is in fact related to comorbidity rather than to the emergency procedure itself, and that prior efforts should be made to optimize comorbidities before surgery (17).
In the current study, emergency patients were older, more comorbid, and more often smokers, perhaps because these patients are more often advised against elective surgery. Although adjusting for various comorbidities in our current model, emergency operation still stood out as an independent risk factor for postoperative complications. The choice between surgical repair and watchful waiting is up to debate in recent years (18). Although the long-term mortality is not reduced in patients undergoing incisional hernia repair compared to those subjected to watchful waiting, the fascial defects seem to increase in size when waiting for repair, making a subsequent abdominal wall reconstruction more complicated (19). The results of the current study does not answer whether watchful waiting is a feasible treatment strategy, but however shows that emergency repair indeed is undesirable.
The use of retromuscular mesh placement remains the golden standard in incisional hernia repair. However, the significantly increased risk of postoperative complications in emergency hernia repair using retromuscular mesh placement suggests that this method should be preserved for planned elective surgery undertaken by trained hernia surgeons. Previous studies in many other surgical fields have shown clear correlations between volume of procedures and complication rates, on the individual level of surgeons (20–23). Conventional closing of the abdominal wall with perhaps use of an onlay mesh should preferably be used in the emergency setting. Technically less challenging onlay mesh technique in the emergency setting is associated with low recurrence levels compared to suturing (20,24) and does not seem to be associated with increased surgical site infections in clean and clean-contaminated surgical fields (25). Onlay mesh has previously been associated with increased risk of hernia recurrence and postoperative seromas compared to retromuscular mesh though (26,27).
The current study has limitations. There was no information available on complications that did not require readmission to the hospital or surgical intervention, meaning that many less serious surgical site occurrences were not accounted for. Furthermore, no information on loss of domain was available. The use of retromuscular mesh placement in the acute setting perhaps represents the more complicated hernias in our population, where the need for lateral release is pivotal in order to obtain closure of the abdominal wall. However, hernia size was adjusted for in the multivariable model. Furthermore, follow-up time is short, and recurrence rates could therefore not be included. Information on waiting time for both elective and emergency repair, as well as time of surgery and duration of surgery was not available from the database. Furthermore, there was no data on whether the patients having an emergency repair had been evaluated for elective repair previously. This information could have been interesting, in order to evaluate the reasons why elective repair was not performed. Also, information on potentially planned reoperations in the emergency group was not available from the database. Inclusion time was limited to 2017–2018 in order to include newly added variables such as smoking and BMI, which consequently might have compromised the statistical significance of some of our findings. Although smoking and obesity were adjusted for in our model, an element of confounding by indication cannot be entirely ruled out. In the current study, smoking and obesity did not significantly increase the risk of reoperation, which may be due to type 2 error; however, we were not able to fully validate these variables due to anonymized data and therefore quality of the variables might vary.
In conclusion, we found that emergency open incisional hernia repair was associated with poor postoperative outcomes and longer length of stay, and further that retromuscular mesh placement in patients undergoing emergency repair was associated with less favorable results. Thus, we propose that increased awareness on offering elective incisional hernia repair in due time is considered, and further that retromuscular mesh placement in emergency incisional hernia repair perhaps should be reserved to selected patients and only surgeons with abdominal wall expertise. Further studies on the risk–benefit relation of expectancy at the risk of emergency surgery versus elective planning of incisional hernia repair are still warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The study was approved by the Danish Data Protection Agency (Journal No. VD-2018-354, I-Suite: 6599)