
Abstract
Background and Aims:
Incisional hernia development is a frequent long-term sequel after open abdomen treatment. This report describes a novel technique, the vacuum-assisted wound closure and permanent onlay mesh–mediated fascial traction for temporary and final closure of the open abdomen, with the intention to decrease incisional hernia rates. Primary aim was to evaluate incisional hernia development and secondary aims to describe short-term complications and patient-reported outcome.
Materials and Methods:
The basics of the technique is an onlay mesh, applied early during open abdomen treatment by suturing to the fascia in two rows with a 3- to 4-cm overlap from the midline incision, used for traction and kept for reinforced permanent closure. A retrospective case series, including chart review, evaluation of computed tomography/ultrasound images, and an out-patient clinical examination were performed. The patients were asked to answer a modified version of the ventral hernia pain questionnaire.
Results:
A total of 11 patients were treated with vacuum-assisted wound closure and permanent onlay mesh–mediated fascial traction with median follow-up of 467 days. Fascial closure rate was 100% and 30 day mortality 0%. Two of nine patients, eligible for incisional hernia follow-up, developed a hernia. Neither of the hernias were symptomatic nor clinically detectable. Six of 10 patients eligible for short-term follow-up had a prolonged wound-healing time exceeding 3 weeks. One of seven patients eligible for patient-reported outcome have had pain during the last week.
Conclusion:
The vacuum-assisted wound closure and permanent onlay mesh–mediated fascial traction is a promising new technique for open abdomen treatment and reinforced fascial closure. The results of the first 11 patients treated with this technique show a low incisional hernia rate with manageable short-term wound complications and few patient-reported disadvantages.
Introduction
When open abdomen (OA) treatment is needed, a temporary abdominal closure (TAC) technique has to be applied in order to protect the abdominal content and facilitate fascial closure. In a review by Atema et al. (1), it was concluded that a combination of negative-pressure wound therapy (NPWT) and fascial traction result in the highest fascia closure rates. The same conclusion was drawn in two guidelines on OA therapy published in 2018 (2, 3). The first technique utilizing this combination, the vacuum-assisted wound closure and mesh-mediated fascial traction (VAWCM), was described in 2007 from our institution (4). In this technique, a large mesh is divided in two halves and sutured to the fascial edge on each side of the incision. After applying the intra-abdominal part of the NPWT system, the meshes are sutured together under tension pulling the fascia toward the midline. At definitive closure, the meshes are removed and the facia was closed with a running suture. This technique enables fascia closure in 61%–100% reported in patients surviving the OA period (5, 6). By utilizing the VAWCM technique, the former problem with large ventral hernias can be avoided in most patients. However, more recent studies evaluating long-term complications after NPWT and fascial traction of any kind show incisional hernia (IH) frequencies between 21%–54% (7–11). Improvement of TAC techniques is desirable in order to prevent IH formation and subsequent need for additional surgery in these already severely afflicted patients.
The vacuum-assisted wound closure and permanent onlay mesh–mediated fascial traction (VAWCPOM) technique was developed at our institution, utilizing NPWT and permanent onlay mesh for fascial traction, in order to prevent IH. When terminating the OA therapy, the onlay mesh is left in place and used for fascia reinforcement. Furthermore, the improved attachment of the mesh to the fascia allows the applied traction to be increased. This might result in fewer dressing changes and shorter time to final closure.
The purpose of this report is to describe the VAWCPOM technique and to retrospectively evaluate short-term complications, IH development, and patient-reported outcome.
Material and Methods
The VAWCPOM Technique
The principles of the initial steps of the VAWCPOM technique
The rectus fascia is dissected free from subcutaneous fat for a distance of 3–4 cm around the incision.
The incision is reinforced using an non-absorbable 2-0 suture (reinforced tension line, RTL) as described by Hollinsky et al. (12) (Fig. 1A and 2A).
A 30 × 30 cm traction-resistant heavyweight polypropylene mesh is divided into two halves and sutured at its lateral margin to the fascia with narrow stitches using a non-absorbable running 2-0 suture, with the mesh overlapping the fascial incision by 3–4 cm in both lateral and cranial/caudal directions.
A second line of a running 2-0 suture is applied to the edge of the fascial incision including the RTL suture in every stitch (Fig. 1B and 2B).
The same procedure is performed with the other half of the mesh on the contralateral side where after the RTL suture is tied.
The OA NPWT system is applied and tucked far out intra-abdominally in all directions to prevent adhesions between the abdominal wall and viscera.
The mesh halves are trimmed and closed under tension over the intra-abdominal dressing, minimizing the gap between the fascial edges (Fig. 1C and 2C).
Perforated foam is applied above the closed mesh and is kept narrow enabling medial sliding of the skin (Fig. 1D).
The plastic drapes and the tubing set are applied. The therapy unit is set to −125 to −150 mmHg with continuous pressure. In patients with coagulopathy, the pressure applied might be lowered to minimize the risk of bleeding (Fig. 1E and 2D).
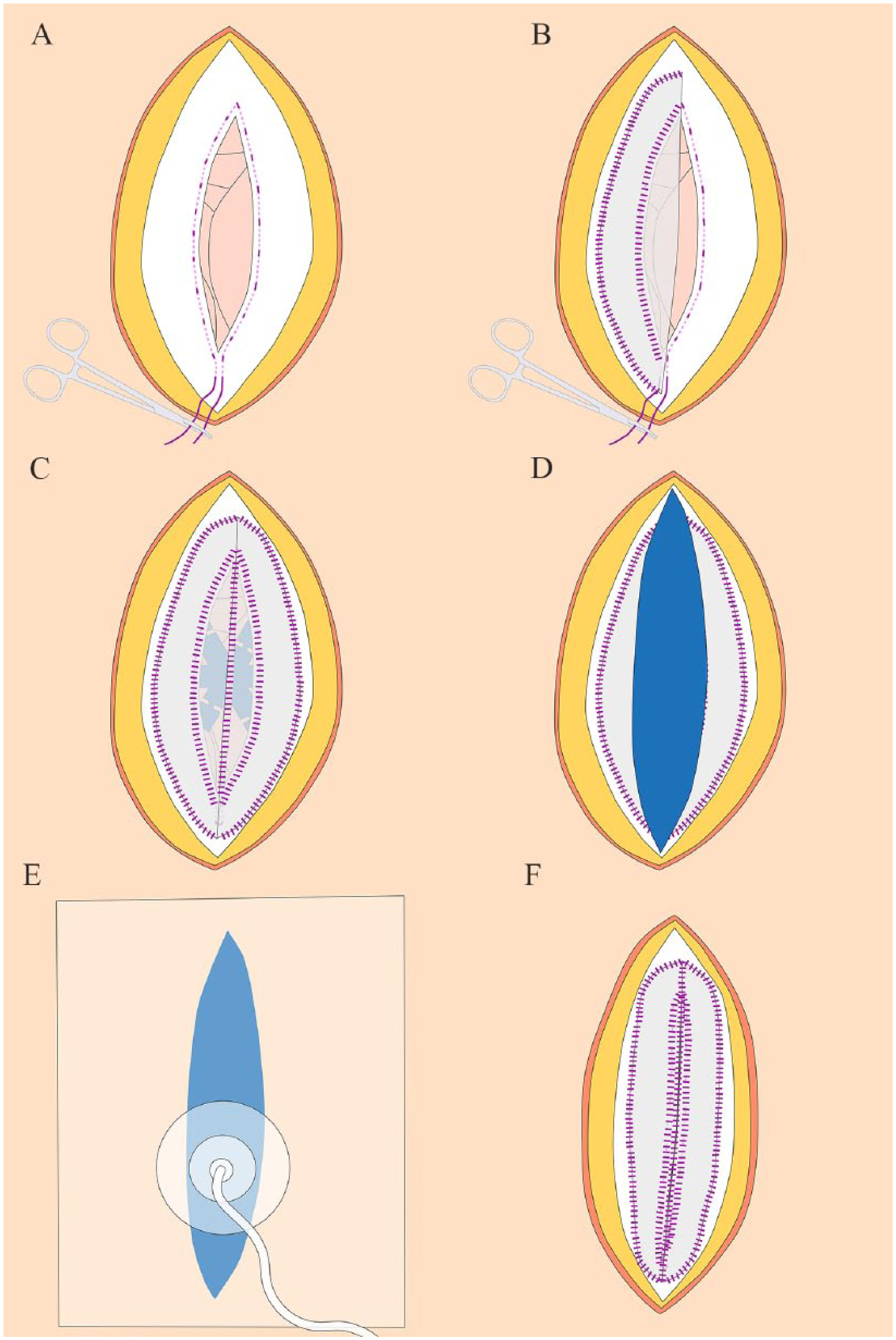
Schematic illustration describing the VAWCPOM technique: (A) the fascia is dissected free from subcutaneous fat on a distance of approximately 3 cm from the incision on each side, as well as cranially and caudally, and a reinforced tension line (RTL) suture is applied along the fascial edges. (B) The first half of the heavyweight polypropylene mesh is sutured to the fascia in double rows, one at the lateral margin of the mesh and the other along the fascial edge including the RTL suture. (C) The other half of the mesh is sutured in the same way, and the RTL suture is tied. The abdominal part of the NPWT system is placed as far out as possible before the two mesh halves are sutured together in the midline under tension. (D) The subcutaneous NPWT perforated foam is cut narrower than the skin gap. (E) The plastic drape and the tubing set is then applied, taking care to slide the skin edges medially. (F) When the fascial edges can be aligned, the abdomen is closed. Trim the mesh along the fascial edges on both sides and suture the mesh with small and narrow stitches. It is not necessary to suture the fascia. All suturing is done with non-absorbable sutures.
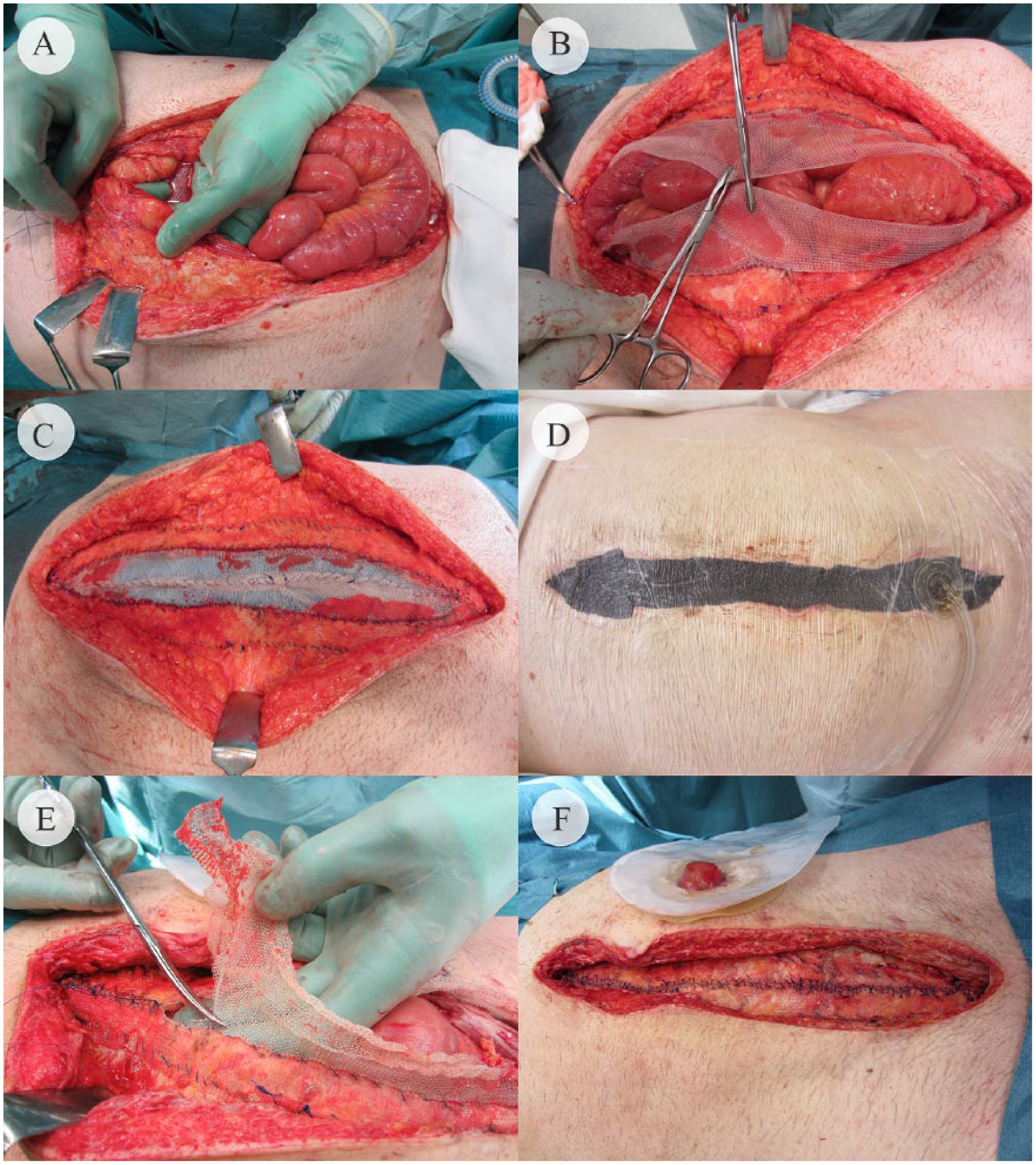
Operation photography describing the VAWCPOM technique: (A) the reinforced tension line (RTL) suture is applied along the fascial edge after the fascia has been freed from subcutaneous fat. (B) The heavyweight polypropylene mesh halves are sutured to the fascia in double rows, one at the lateral margin of the mesh and the other along the fascial edge including the RTL suture. (C) After the abdominal part of the NPWT system is placed as far out as possible, the two mesh halves are sutured together in the midline under tension. (D) The subcutaneous NPWT perforated foam is cut narrower than the skin gap, and the plastic drape and the tubing set are then applied, taking care to slide the skin edges medially. (E) and (F) The mesh is trimmed along the fascial edges on both sides and sutured with small and narrow stitches. It is not necessary to suture the fascia. All suturing is done with non-absorbable sutures.
Course of action at dressing changes performed every 48–72 h
Remove the subcutaneous perforated foam, open the mesh, remove the intra-abdominal dressing, take samples for bacterial culture, and perform lavage with warm saline solution.
A new intra-abdominal dressing is applied.
Any redundant part of the mesh is trimmed, and the mesh is tightened.
A new narrow subcutaneous foam, plastic drapes, and tubing set are applied.
Abdominal wall/fascial closure when fascial edges can be aligned
Remove the subcutaneous perforated foam, open the mesh, remove the intra-abdominal dressing, take samples for bacterial culture, and perform lavage with warm saline solution.
Trim the mesh to the level of the fascial edges on both sides (Fig. 2E).
Close the mesh with small and narrow stitches of a non-absorbable running 2-0 suture taking care not to fold the mesh or creating a ridge of mesh in the midline (Fig. 1F and 2F).
In case the conditions for skin closure is not optimal, apply subcutaneous NPWT for a few days before the skin is closed.
After closure of the skin, application of a NPWT system for closed incisions can be considered for an additional week.
The OA treatment with VAWCPOM can be initiated using either of two ways. If the patient is stable the onlay mesh and NPWT system can be applied at the first operation. In case of an unstable critically ill patient, a two-step procedure can be performed to save time and minimize the surgical trauma. The NPWT system is applied during the first operation without the onlay mesh, which instead is applied during the first dressing change. In this way, it is possible to stabilize the patient in the intensive care unit (ICU) before the more time-consuming application of the mesh is done. An algorithm for OA treatment used at our institution is presented in Fig. 3.
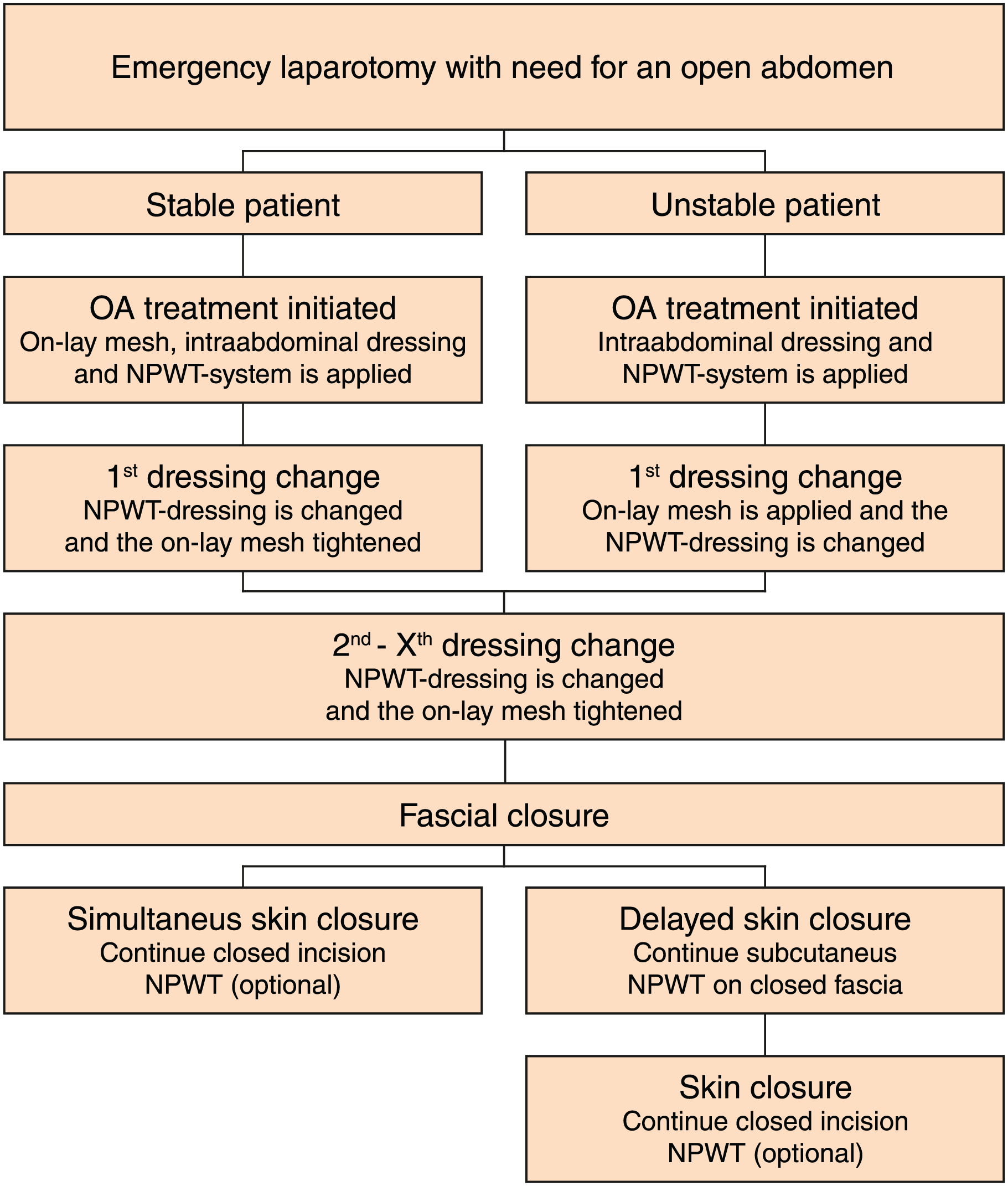
Algorithm for open abdomen treatment with the VAWCPOM technique.
Included Patients and Study Design
Consecutive OA patients treated with the VAWCPOM technique at the Department of Surgery, Skåne University Hospital, Sweden, between December 2014 and December 2016, were included in this retrospective case series. Patients were identified by searching the operation registers (surgical codes JAH30, JAH33, and DQ023).
Chart review
A chart review was performed, and data retrieved according to Tables 1 to 3. If patients had undergone computed tomography (CT) or ultrasound during the follow-up time for other indications, the images were examined in order to increase the possibility to diagnose clinically non-detectable IHs.
Patient characteristics at OA.
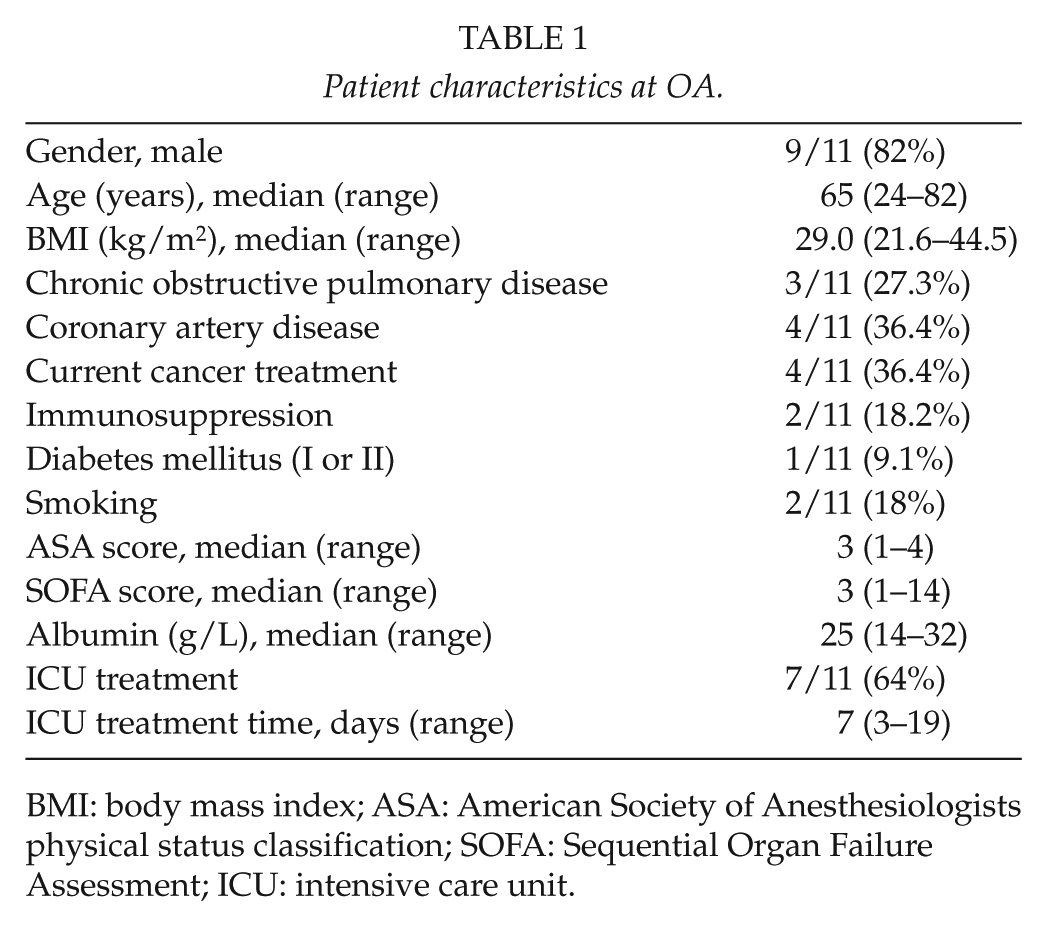
BMI: body mass index; ASA: American Society of Anesthesiologists physical status classification; SOFA: Sequential Organ Failure Assessment; ICU: intensive care unit.
VAWCPOM treatment details.
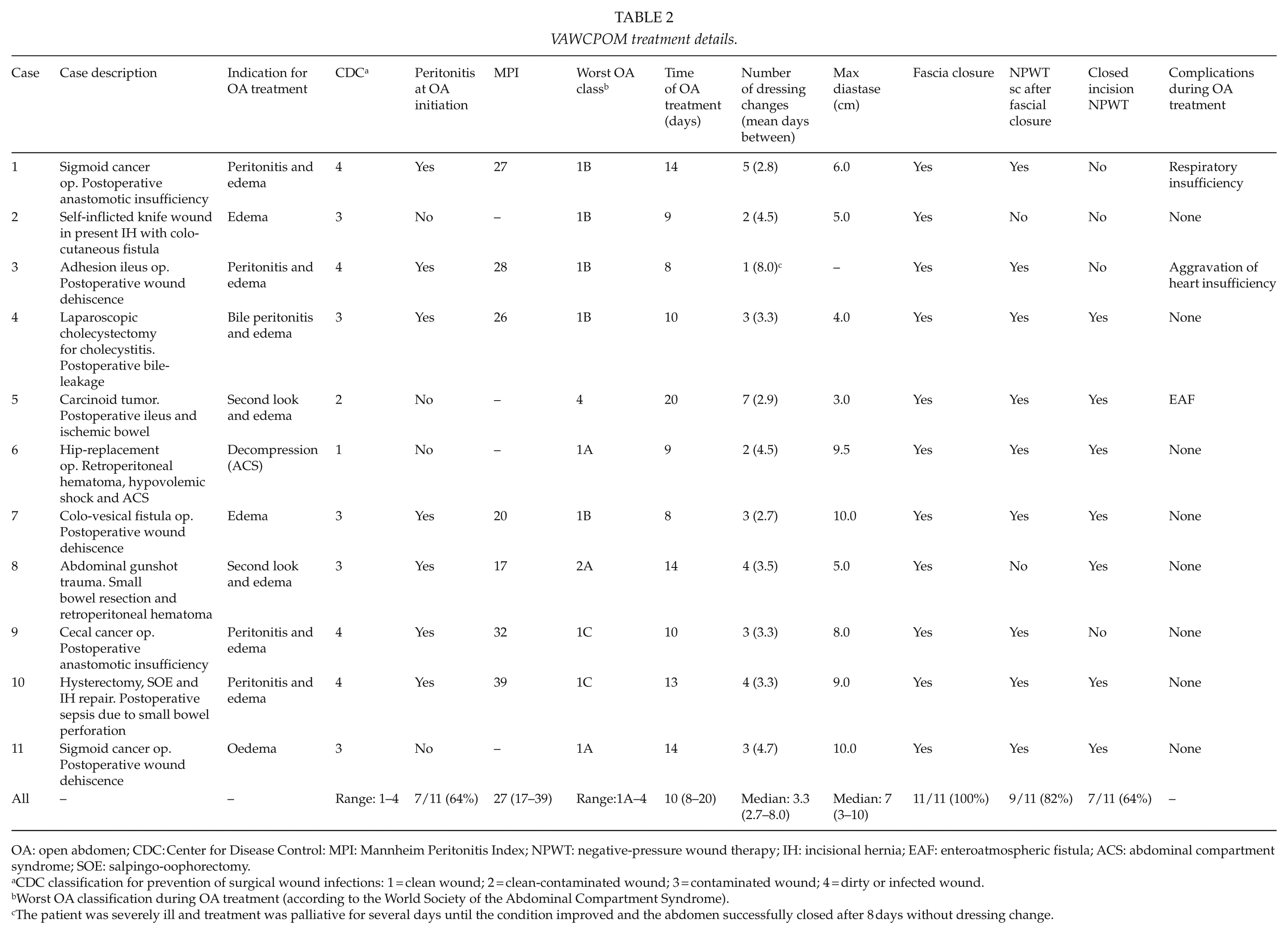
OA: open abdomen; CDC: Center for Disease Control: MPI: Mannheim Peritonitis Index; NPWT: negative-pressure wound therapy; IH: incisional hernia; EAF: enteroatmospheric fistula; ACS: abdominal compartment syndrome; SOE: salpingo-oophorectomy.
aCDC classification for prevention of surgical wound infections: 1 = clean wound; 2 = clean-contaminated wound; 3 = contaminated wound; 4 = dirty or infected wound.
Worst OA classification during OA treatment (according to the World Society of the Abdominal Compartment Syndrome).
The patient was severely ill and treatment was palliative for several days until the condition improved and the abdomen successfully closed after 8 days without dressing change.
Short- and long-term follow-up.
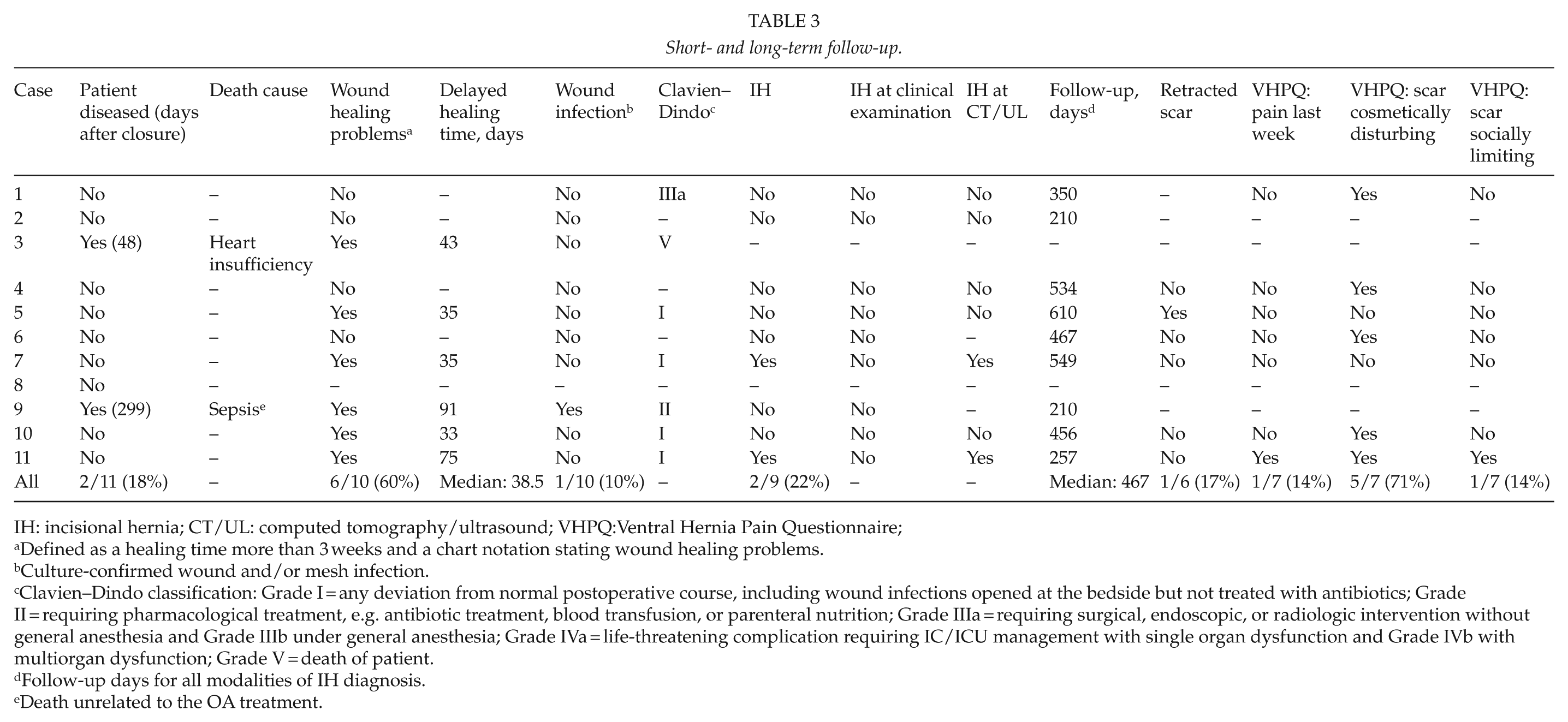
IH: incisional hernia; CT/UL: computed tomography/ultrasound; VHPQ:Ventral Hernia Pain Questionnaire;
Defined as a healing time more than 3 weeks and a chart notation stating wound healing problems.
Culture-confirmed wound and/or mesh infection.
Clavien–Dindo classification: Grade I = any deviation from normal postoperative course, including wound infections opened at the bedside but not treated with antibiotics; Grade II = requiring pharmacological treatment, e.g. antibiotic treatment, blood transfusion, or parenteral nutrition; Grade IIIa = requiring surgical, endoscopic, or radiologic intervention without general anesthesia and Grade IIIb under general anesthesia; Grade IVa = life-threatening complication requiring IC/ICU management with single organ dysfunction and Grade IVb with multiorgan dysfunction; Grade V = death of patient.
Follow-up days for all modalities of IH diagnosis.
Death unrelated to the OA treatment.
Assessment at OA initiation and during OA treatment
At OA initiation, the patient’s clinical status was evaluated with American Society of Anesthesiologists physical status classification (ASA) and with the Sequential Organ Failure Assessment (SOFA) score (13). When calculating the SOFA score, the worst value for each organ system noted from 12 h before, up to 12 h after the OA initiation, was used.
Contamination grade at OA initiation was classified according to the Centers for Disease Control and Prevention (CDC) classification for prevention of surgical wound infections (14).
For every OA intervention, that is, the OA initiation procedure, dressing changes and at fascial closure, the OA status was classified according to the OA classification system defined by the World Society of Abdominal Compartment Syndrome (15–17). Peritonitis, if present at OA initiation, was graded according to the Mannheim Peritonitis Index (MPI) (18). Causes for OA treatment were classified as follows: 1 = visceral edema and/or intra-abdominal/retroperitoneal swelling, reducing intra-abdominal space, making it mechanically impossible to close the abdomen; 2 = intra-abdominal deep infection/peritonitis with need for drainage; 3 = damage control and/or planned second look operation; and 4 = decompression in case of an abdominal compartment syndrome. Patients may have more than one of the abovementioned causes. Complications occurring during the OA treatment was noted.
Assessment of postoperative complications
Postoperative complications, that is, complications occurring after fascial closure, were graded and classified according to Clavien–Dindo Classification (19). Short-term wound complications were evaluated, and the wound-healing time was calculated from chart notations made by wound-specialized nurses. Prolonged healing was defined as healing time exceeding 3 weeks and chart notation stating wound-healing problems.
Clinical out-patient follow-up
Patients alive in August 2017 were invited to a clinical follow-up. A protocol-based clinical hernia examination was performed in upright and supine position during relaxation, straining, and coughing. It was noticed whether the scar was stuck to the underlying fascia or freely displaceable. The patients answer a modified version of the Ventral Hernia Pain Questionnaire (VHPQ) (20), approved by the inventors. Patients not able to attend the clinical examination answered the questionnaire by mail or telephone.
Patients operated with additional surgery through the onlay mesh was excluded from the out-patient clinical examination and from answering the pain questionnaire. However, the presence of an IH was evaluated at the additional surgical procedure. Follow-up time was calculated from the day of fascial closure to the day of clinical examination, last chart notation or day of the additional surgery, respectively.
Ethical approval
Ethical approval for this retrospective case series was not needed, as it is classified as a clinical quality evaluation according to the Regional Ethics Committee at Lund University, Sweden (2012/726). Patients were informed in writing and approved participation by answering the questionnaire.
Results
Assessment at OA Initiation and During OA Treatment
A total of 11 patients treated with VAWCPOM were identified and included. Patient characteristics at the OA initiation are presented in Table 1. VAWCPOM treatment details for each patient are presented in Table 2. Fascial closure rate was 100%.
One patient developed an anastomotic leakage during the VAWCPOM treatment that transformed into an enteroatmospheric fistula (EAF). Due to its location, deep down in the right side of the abdomen, it was impossible to locate during dressing changes. The fistula was managed successfully by drainage with a transcutaneous catheter placed as far out to the right side and as close to the fistula as possible, with continued VAWCPOM treatment. Adhesions were allowed to develop around the catheter, thereby creating a fistula separated from the OA, making it possible to close the fascia despite the fistula. Shortly thereafter, the fistula effluent ceased.
Mortality
There was no 30-day mortality. However, two patients died during follow-up. One patient was discharged to a nursing home but was re-admitted a few days later due to aggravation of heart insufficiency and died 48 days after fascial closure. The second patient died due to a septic condition not related to the VAWCPOM treatment after 299 days.
Assessment of Postoperative Complications
Postoperative short-term complications are presented in Table 3. One patient was lost to follow-up after discharge. Prolonged wound healing was seen in 6/10 patients. One patient developed a mesh infection treated conservatively with antibiotics for a prolonged period of time before a small part of the onlay mesh was extirpated, where after the wound was treated with NPWT until healing. Another patient was subject for a longer period of conservative wound treatment without NPWT. The remaining four patients’ delayed wound healing was due to a planned approach, where a shorter part of the midline incision was left for secondary healing after finishing NPWT. These patients were managed at the out-patient clinic by a nurse until the wound was healed. The average wound-healing time just exceeded 4 weeks in the patients with prolonged healing.
Clinical Out-Patient Follow-Up and the Modified VHPQ
Long-term complications, together with answers to the VHPQ are shown in Table 3. Nine patients were eligible for IH evaluation (one early death and one patient was lost to follow-up) and two (22%) developed an IH. None was detectable at clinical examination but diagnosed by CT or ultrasound performed for other reasons. Both hernias were located either in the upper or lower part of the midline above or below the onlay mesh. None of the patients reported any symptoms related to the hernia, and none had undergone IH repair during the follow-up period.
Seven patients answered the modified VHPQ. One patient was lost to follow-up, and three patients were not eligible (two deceased and one re-operated for stomal reversal with a midline incision). One patient (14%) had experienced pain during the last week. Five of seven (71%) found their scar cosmetically disturbing, and one (14%) also found it socially limiting.
Discussion
We describe a novel TAC technique for management of OA with vacuum-assisted wound closure combined with the application of a permanent onlay mesh for fascial traction and IH prevention (VAWCPOM). The results of the 11 first patients treated with the technique are promising with fascial closure in all patients, a relatively low IH rate without serious short-term wound complications or patient-reported disadvantages.
In this report, 9 of 11 patients were eligible for follow-up concerning IH formation, showing an IH rate of 22% after a median of 467 days. In comparison with the older VAWCM technique, this is a considerably lower incidence. None of the two patients had a symptomatic IH and none had undergone surgical repair. In both cases, the hernia was located above and/or below the mesh, and from the patient’s chart, we suspect that the cranial/caudal mesh coverage in these patients might have been insufficient. This stresses the need for good mesh coverage with at least a 3-cm overlap on healthy non-incised fascia both cranially and caudally, a fact we have become aware of during this retrospective evaluation. In the systematic review by Acosta et al. (5) from 2017, IH rates reported in two prospective and one retrospective study ranged between 21%–54%. Our result is in the lower part of this range, and we assume it may be further decreased as the treatment protocol for VAWCPOM is further implemented among surgeons.
In this small case series of patients, the mesh/fascia closure rate was 100%, but much larger numbers of patients are needed to determine the actual closure rate for the technique. However, there is no reason to believe that the new technique should perform worse than the old. With improved attachment of the mesh, a greater fascial traction can be applied, possibly increasing fascial closure rates. Another potential benefit when the fascial traction is increased is shorter time to fascial closure.
The use of a permanent mesh in contaminated surgical fields has been advised against, since the dominating previous experience has been that an infected mesh could seldom be salvaged (21). However, there are data indicating that the use of NPWT in case of mesh infections may provide a solution to this problem (22, 23). In addition, data from studies on prophylactic mesh in clean-contaminated situations, for example, for reinforcing incisions after colorectal surgery or for prevention of parastomal hernias, does not indicate crucial drawbacks concerning mesh-related complications (24). In our report, 9 of 11 patients had a contaminated or dirty/infected wound according to the CDC classification, and seven of those had peritonitis at OA initiation. We even experienced the development of an EAF during the VAWCPOM treatment in one patient. The fistula originated from a leaking anastomosis and was located deep in the abdomen, far from the applied intra-abdominal part of the NPWT system. It is impossible to say if the negative-pressure treatment caused the leakage and the formation of the EAF or not, but earlier research implicates that the negative pressure applied during VAWCM treatment does not propagate far beyond the intra-abdominal visceral protection sheet (25). Furthermore, a systematic review by Atema et al. (1) from 2015 showed that NPWT with mesh traction had a lower incidence of fistula formation in comparison with the other TAC techniques. The fortunate outcome in our patient with a closed abdomen, mesh in place, no mesh infection, and a closed fistula demonstrates that situations earlier believed to be deleterious can now be treated successfully. In our report, the majority of patients were contaminated when the synthetic mesh was applied. Only one patient developed a postoperative mesh infection and one had a noticeably prolonged healing time. In both patients, a substantial part of their wound-healing time was treated without NPWT. A more active approach could possibly have reduced the healing time for these two patients.
In an upcoming prospective study, there is an evident need for a defined protocol on how to handle wounds at OA termination and how to handle postoperative wound complications in VAWCPOM patients. Furthermore, it is important that the VAWCPOM technique is utilized in an optimal way for prevention of wound complications. A subcutaneous exposed mesh is known to cause significantly more wound complications, especially seroma formation, compared to fascia-covered meshes (21, 26–29). Despite this, the VAWCPOM technique advocates the onlay mesh position. The key for its success is that the onlay mesh is granulated before skin closure. Often, this is obtained during the OA treatment, but otherwise achieved by utilizing prolonged NPWT on closed mesh/fascia if needed. An alternative to the onlay position could be a retromuscular mesh, but for many of the patients in need of OA, this would have been an unnecessary additional surgical trauma. We have therefore chosen the simpler onlay position as the standard mesh placement.
In the patient-reported follow-up, one of seven patients had experienced pain during the last week, but the pain could easily be ignored and did not affect daily activities. The majority of the patients reported that they found their scar cosmetically disturbing, and a part of that group also found it socially inhibiting. After OA treatment, “ugly” abdominal scars are hard to prevent, but one effort that might be important is to routinely plan for secondary suture if subcutaneous NPWT is used after fascial closure.
This is a retrospective case series including 11 patients and interpretation of the results should be done with caution due to the retrospective context and few patients included. Discrepancies in pre-, peri- and postoperative management is expected and might influence the results. However, there were no operative data missing, and only one eligible patient was lost to follow-up.
In summary, this retrospective case series, including the first 11 patient treated with the novel VAWCPOM technique shows promising results with 100% fascial closure rate, no OA treatment–related mortality, manageable short-term wound complications, a low IH rate, and low incidence of long-term abdominal wall pain. Further evaluation, preferably in a prospective study, is needed before this novel technique can be introduced as a standard treatment regime.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.