
Abstract
Purpose:
The aim of this systematic review was to evaluate the risk of parastomal (PSH) and incisional hernias (IH) after emergency surgery for Hinchey III–IV diverticulitis, with comparison between the Hartmann procedure and other surgical techniques.
Methods:
The Cochrane Library, Embase, PubMed (MEDLINE), Web of Science and Scopus databases were systematically searched. The primary endpoint was parastomal hernia incidence. The secondary endpoint was incisional hernia incidence.
Results:
Five studies (four randomized controlled trials and one retrospective cohort) with a total of 699 patients were eligible for inclusion. The PSH rate was 15%–46% for Hartmann procedure, 0%–85% for primary anastomosis, 4% for resection, and 2% for laparoscopic lavage. The IH rates were 5%–38% for Hartmann procedure, 5%–27% for primary anastomosis, 9%–12% for primary resection, and 3%–11% for laparoscopic lavage.
Conclusions:
Both the parastomal and incisional hernia incidences are poorly evaluated and reported, and varied greatly between the studies.
The risk of permanent colostomy is significant after emergency Hartmann procedure (HP) for diverticulitis. 1 According to the literature, half of patients with permanent colostomy after rectal cancer operation will have a parastomal hernia (PSH). 2 However, the prevalence of PSH after colostomy for diverticulitis operation remains poorly evaluated.
Incisional hernia (IH) risk after elective surgery for diverticulitis ranges from 11% to 15%. 3 IH prevalence after emergency surgery for diverticulitis is rarely reported.
We hypothesized that patients undergoing surgery for complicated diverticulitis are at high risk for PSHs and IHs. Therefore, the aim of this review was to evaluate the IH and PSH rate after diverticulitis surgery and compare different surgical techniques for Hinchey III–IV sigmoid diverticulitis in relation to PSH and IH.
Material and methods
The systematic search was performed using Cochrane Library, Embase, PubMed (MEDLINE), Web of Science, and Scopus without any restrictions for language or study design. All randomized controlled trials (RCTs) and cohort studies comparing HP with other surgical treatment options for Hinchey III–IV diverticulitis were systematically searched and all studies reporting either IH or PSH rate were included, regardless of the definition of hernia, length of follow-up, or diagnostic method used. The primary endpoint was PSH rate and the secondary endpoint was IH rate.
Results
Of the 5952 identified studies, 5 were included in this systematic review and meta-analysis (4 randomized controlled trials (RCTs) and 1 retrospective cohort) with a total of 699 patients4 –8 (Table 1). The PSH rate was 15%–46% for HP, 0%–85% for primary anastomosis, 4% for resection, and 2% for laparoscopic lavage. The IH rates were 5%–38% for HP,4,7,8 5%–27% for primary anastomosis,7,8 9%–12% for primary resection,5,6 and 3%–11% for laparoscopic lavage.4,6,7 None of the studies defined PSH as an outcome. The follow-up methods varied between clinical examination, telephone interview, patient record review, and question form sent by mail, but the proportion of patients clinically assessed at outpatient clinics remained unclear (Table 1). Due to heterogeneity of study design, follow-up methods, follow-up time, and lack of both PSH and IH as outcome, no meta-analysis could be conducted.
Study characteristics.
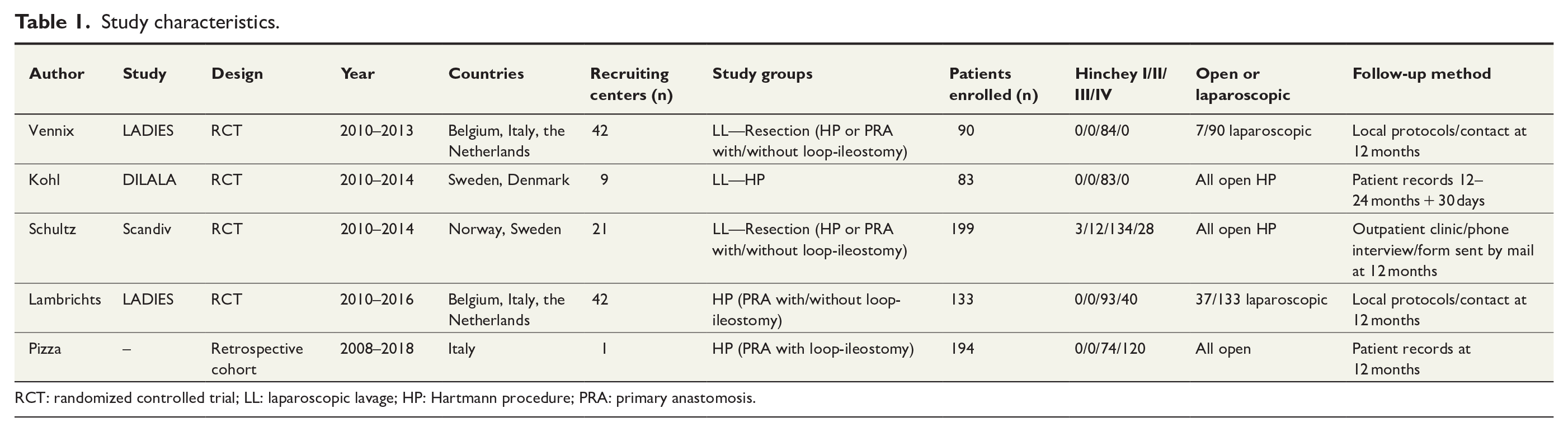
RCT: randomized controlled trial; LL: laparoscopic lavage; HP: Hartmann procedure; PRA: primary anastomosis.
Conclusion
This systematic review highlighted the lack of adequate research on PSH and IH rates after emergency surgery for complicated Hinchey III–IV diverticulitis. As a result, post-operative hernia prevalence probably remains underestimated. Both the PSH and IH reporting varied greatly between the studies. For future RCTs, researchers are encouraged to pay more attention to hernia diagnosis, symptoms, and prevention after surgical treatment for Hinchey III-IV diverticulitis.
PROSPERO registration number: CRD 42020216003.
Footnotes
Author contributions
E.M. contributed to conception of the review; acquisition, analysis, and interpretation of the data; drafting of the work; and approval of the submitted version. T.R. contributed to conception of the review; acquisition, analysis, and interpretation of the data; critical revision of the work; and approval of the submitted version. J.R. contributed to interpretation of the data, critical revision of the manuscript, and approval of the submitted version. F.M. contributed to conception of the review; acquisition, analysis, and interpretation of the data; critical revision of the work; and approval of the submitted version. J.H.K. contributed to conception of the review; acquisition, analysis, and interpretation of the data; drafting and critical revision of the work; and approval of the submitted version.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.M. reports consultancy fees by Medtronic; T.R. reports Surgeon Service Agreement with Intuitive; F.M. reports speakers’ honorarium and research grants by Bard Davol, consultancy fees by CMR surgical, speakers’ honorarium and research grant by Dynamesh, speakers’ honorarium and proctorship by Intuitive Surgical, and speakers’ honorarium and consultancy fees by Medtronic; J.R. reports no conflicts of interest; and J.H.K. reports no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.