
Abstract

Introduction:
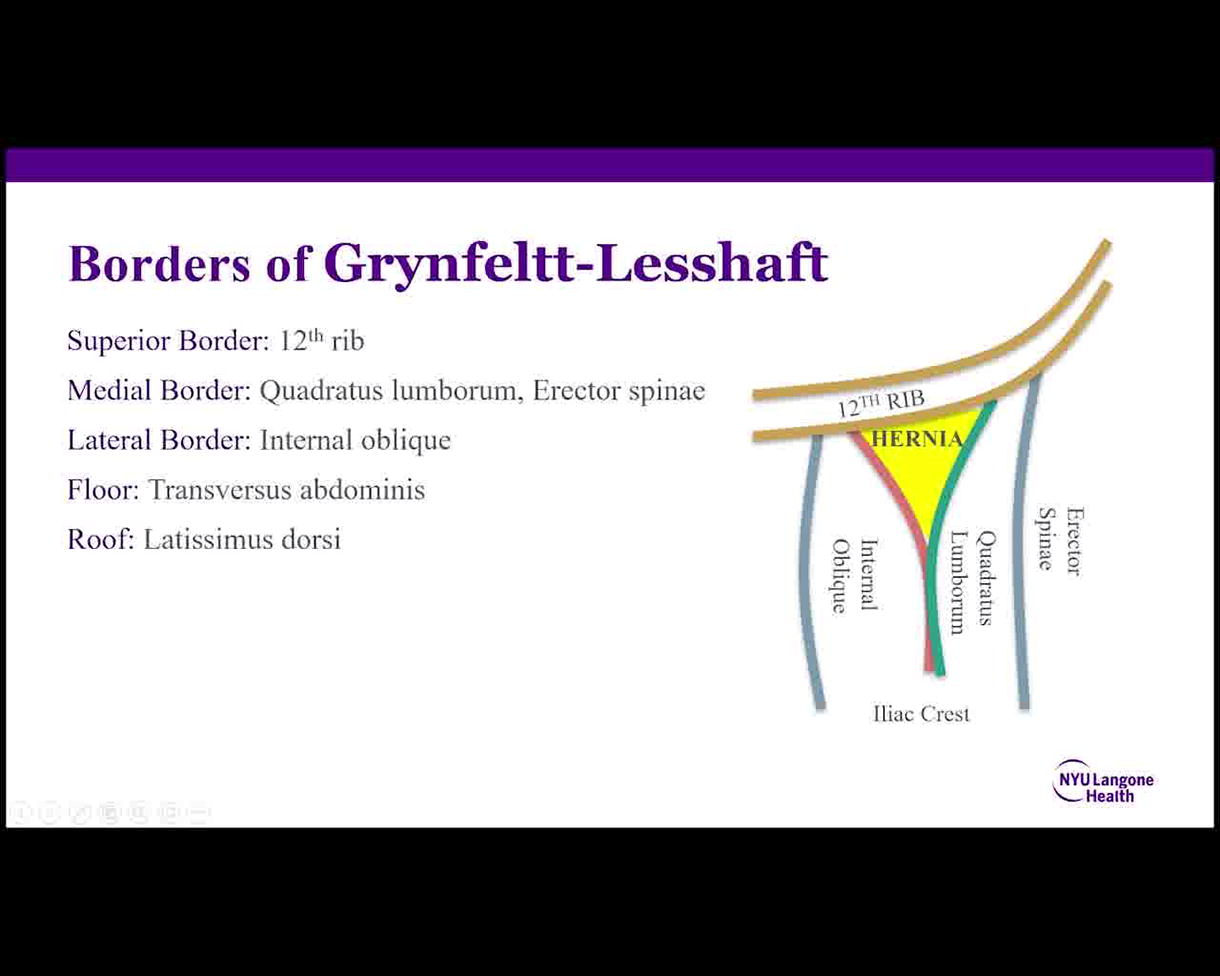
The Grynfeltt-Lesshaft hernia is an uncommon abdominal wall defect that typically presents as an asymptomatic bulge in the superior lumbar triangle and is often mistaken for a lipoma. 1 The superior border of the triangle is the 12th rib. The medial border is the quadratus lumborum or the erector spinae muscle. The lateral border is the internal oblique, which courses between the 12th rib and the iliac crest. The floor of the hernia is the weakened transversalis fascia, and the roof of the hernia is the latissimus dorsi muscle. Elective repair of the hernia is recommended to prevent complications involving the herniation of retroperitoneal and intraperitoneal structures as the defect enlarges over time. 2
Methods:
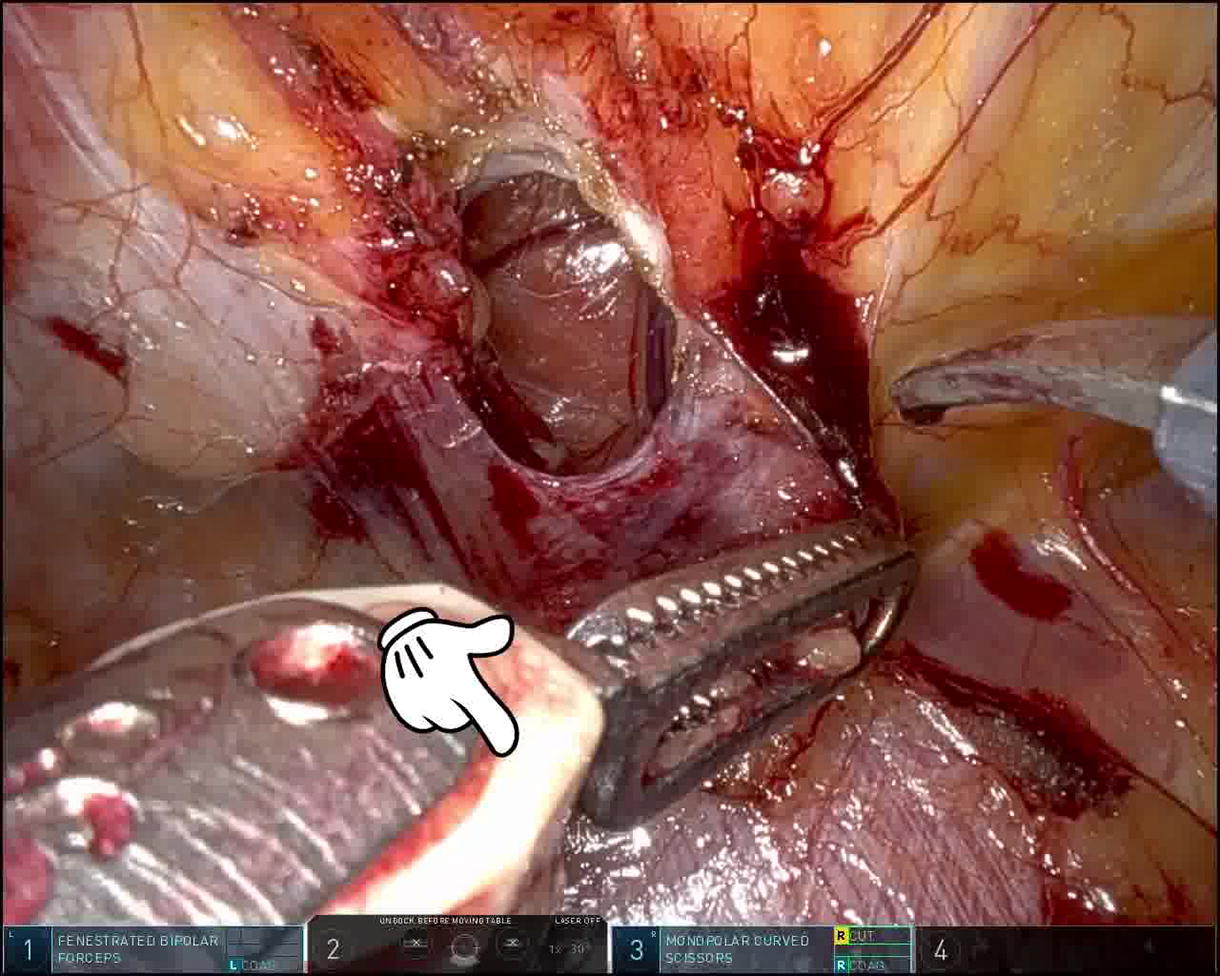
A 71-year-old female former smoker with a body mass index (BMI) of 25 kg/m2 and a past medical history of hyperlipidemia, bladder prolapse, and mitral valve prolapse presented with the complaint of a painful left posterior trunk lipoma. Her physical exam was pertinent for a reducible left flank mass, and she was diagnosed with a Grynfeltt-Lesshaft hernia. A computer tomography (CT) of the abdomen and pelvis confirmed this diagnosis by demonstrating a herniation of retroperitoneal fat below the 12th rib, through the superior lumbar triangle, causing the tenting of the latissimus dorsi muscle. The patient was scheduled for an elective robotic repair of the Grynfeltt-Lesshaft hernia with mesh. In the operative theater, she was placed in the right lateral decubitus position, and abdominal access was obtained. A transabdominal preperitoneal (TAPP) dissection was begun by separating the peritoneum from the attachments to the transversus abdominis muscle. Preperitoneal and retroperitoneal fat is lifted along with the flap, and the plane of dissection is intentionally kept close to the muscle layer as dissection is continued posteriorly and laterally. We note the transverse fibers of the transversus abdominis on the right-hand side of the screen, and the more vertically oriented fibers of the diaphragm in the upper portion, or left portion, of the screen. As dissection continues, the common trunk of the iliohypogastric and ilioinguinal nerves comes into view. Once the hernia is exposed, the contents are carefully reduced. The 12th subcostal nerve is carefully mobilized away from the hernia defect using cold shears to allow room for defect closure. Looking through the hernia defect, we can see the tented latissimus dorsi, creating the roof of the hernia. The borders of the superior lumbar triangle are nicely depicted here. The diaphragm and 12th rib are seen to the left of the defect. The subcostal nerve is seen in the foreground along with the quadratus lumborum. The internal oblique muscle is not seen, as it is covered by the transversus abdominis muscle on the right side of the screen. Looking caudally, we see the iliohypogastric and ilioinguinal nerve with their common trunk, and the lateral femoral cutaneous nerve is seen in the foreground. The defect is closed with an absorbable barbed suture. To allow for adequate mesh sublay, the psoas muscle is cleared of retroperitoneal fat. Eventually, the psoas stripe and a diminutive genitofemoral nerve come into view. The dissected space is measured, and a 15 × 15 cm, medium-weight, macroporous polypropylene mesh is introduced. It is positioned with a wide underlay, reinforcing the entire lumbar triangle. The mesh is sutured in place with interrupted Vicryl sutures, taking care to avoid the neuroanatomy or other critical structures. The psoas muscle is seen in the foreground during mesh fixation. The peritoneal flap is closed with an absorbable V-lock suture, excluding the mesh from the peritoneal cavity, thereby completing our repair. The total operative time was 90 minutes with an estimated blood loss of 50 milliliters.
Results:
The patient was discharged from the postanesthesia care unit on the same day of surgery. Her postoperative course was unremarkable. She was seen twice in the office, on postoperative days 14 and 55. She was afebrile and without the presence of a palpable flank mass, seroma, or incision erythema. She denies any complaints and reports resolution of her left flank pain.
Conclusion:
The Grynfeltt-Lesshaft hernia is a herniation of retroperitoneal and intraperitoneal contents through the superior lumbar triangle. The borders of the triangle are defined by the lower border of the 12th rib superiorly, the internal oblique muscle laterally, and the quadratus lumborum (erector spinae muscles) medially. The floor of the triangle contains the transversalis fascia aponeurosis, while the roof is comprised of the latissimus dorsi muscle. Herniation of abdominal content occurs due to the weakening of the transversalis fascia and the aponeurosis of the transversus abdominis. Due to its rarity, many surgeons are unfamiliar with lumbar hernias, often leading to delayed diagnosis. We present a case of a robotic minimally invasive repair of a Grynfeltt-Lesshaft hernia, highlighting pertinent anatomical considerations at each step of the repair.
The authors confirm their contributions to the article as follows: T.Z.: Methodology, project administration; H.H.: Data curation, investigation; A.S.: Resources; D.H.: Conceptualization, supervision. All authors reviewed the results and approved the final version of the article.
The authors have no conflicts of interest or obligations to report.
Funding: None.
The authors have received and archived patient consent for this video.
Runtime of video: 5 mins 16 secs.
Get full access to this article
View all access options for this article.