
Abstract
Background and Aims:
Adult spinal deformity surgery has increased with the aging population and modern surgical approaches, although it has high complication and reoperation rates. The permanence of radiographic correction, mechanical complications, predictive factors for poor patient-reported outcomes, and patient satisfaction were analyzed.
Material and Methods:
A total of 79 adult patients were retrospectively analyzed at baseline and 1–9 years after adult spinal deformity correction between 2007 and 2016. Patient-reported outcomes (Oswestry Disability Index, visual analog scale, and Scoliosis Research Society–30 scores), changes in radiographic alignment, indications for reoperation, predictors of poor outcomes according to the Oswestry Disability Index and Scoliosis Research Society–30 scores, and patient satisfaction with management were studied.
Results:
Oswestry Disability Index and visual analog scale scores (p = 0.001), radiographic correction of thoracic kyphosis, lumbar lordosis, and pelvic retroversion (p ⩽ 0.001) and sagittal vertical axis (p = 0.043) were significantly better at 4–5 years of follow-up than at baseline. The risk for the first reoperation owing to mechanical failure of instrumentation or bone was highest within the first year, at 13.9% (95% confidence interval = 8.0%–23.7%), and 29.8% (95% confidence interval = 19.4%–43.9%) at the 5-year follow-up. Oswestry Disability Index and Scoliosis Research Society–30 total scores had a good correlation (r = −0.78; 95% CI = −0.86 to –0.68; p < 0.001). Satisfaction with management was correlated with patient-reported outcomes. Male sex and depression (p = 0.021 and 0.018, respectively) predicted poor outcomes according to the Oswestry Disability Index and/or Scoliosis Research Society–30 score.
Conclusion:
The achieved significant radiographic correction was maintained 5 years postoperatively. Despite reoperations, patient satisfaction and clinical outcomes were good. Depression and male sex predicted poor clinical outcomes.
Keywords
Introduction
Adult spinal deformities (ASDs) develop through multiple mechanisms that cause disability and reduce the health-related quality of life (HRQoL) (1, 2). Spinal deformity surgery has increased with an increase in the aging population and the development of modern medical and surgical approaches (3, 4). Few conservative treatments prevent the progression of symptomatic ASD (5). Sagittal balance is a combination of skeletal alignment and functional posture of the trunk (1). The main driver for deformity surgery is functional decline and clinical symptoms (6) and not radiographic severity. Restoration of radiographic sagittal alignment is associated with good outcomes (7), and age-related optimal values for correction have been described by comparing radiographic and patient-reported outcomes (PROMs) (1). Surgery is targeted at skeletal alignment, but the process of sagittal control remains, and a good radiographic result may be lost owing to aging or mechanical complications. Compared with hip and knee replacement, ASD surgery achieves poor outcomes (8). However, patient satisfaction with surgical treatment has not been widely studied, and the results have been controversial in relation to radiographic and PROM results. Operative techniques and patient selection have advanced in the 21st century; the amount of anterior surgery has decreased, but the combination of anterior and posterior techniques has increased (4). ASD surgery is associated with a variety of minor and major complications (9). Thus, risk control algorithms for patient selection have been created (10). Mini-invasive deformity surgery techniques have been introduced without reduction of complications (11).
Many PROMs of disability and HRQoL are used to evaluate the clinical outcome of deformity surgery, as radiographic correction is poorly correlated with patient satisfaction with management (12). The Oswestry Disability Index (ODI), EuroQol-5D, Short Form-36, depression scales, and different versions of the Scoliosis Research Society (SRS) deformity-specific questionnaires are common in clinical work, follow-up, and research. It is still unclear which combination of the outcome measures would be optimal in evaluating ASD (13). The optimal clinical application of the ASD surgery theories includes both analyses of the radiographic correction and the patient-reported data of outcome with instruments that are valid to measure the adult population after spinal deformity surgery.
This study aims to perform the first Finnish 1- to 9-year retrospective follow-up of changes in radiographic alignment and indications for reoperation after ASD surgery. The second aim of this study was to analyze the predictors of poor outcomes according to the ODI (14) and the recently validated Finnish adaptation of the deformity-specific SRS-30 (15) scores, as well as patient satisfaction with management among the heterogenous ASD population.
Patients and Methods
The data were collected retrospectively from patient records of our institution, which is the only tertiary-care spine clinic serving a population of 255,000. Inclusion criteria were age > 18 years, American Society of Anesthesiologists risk class ASA3 or less, and elective surgery with the main indication of correcting coronal or sagittal deformity of the spine between June 2007 and June 2016. The six patients who died of non-surgery-related causes (1 cancer, 1 Noonan syndrome related cardiac arrhythmia, 1 severe chronic obstructive lung disease, and 3 cardiovascular seizures) before the follow-up date of June 2017 were excluded from analysis. All radiographs and questionnaires related to clinical treatment during that time were included, and none were obtained for research only. All patients, accompanied with a trustee or family member, gave verbal informed consent to surgery. All patients underwent preoperative digital full spine standing radiography. Radiographic parameters including sagittal vertical axis (SVA), pelvic incidence (PI), lumbar lordosis (LL), PI-LL mismatch, pelvic tilt (PT), T1 pelvic angle (TPA), thoracolumbar maximum Cobb angle, thoracic kyphosis (TK), and T1 Slope (T1S) were measured preoperatively and 3, 12, 24, 36, and 48–60 months postoperatively. Proximal junctional kyphosis (PJK) was measured from postoperative radiographs, respectively, and compared with the immediate postoperative radiograph. A senior spine surgeon performed the measurements. Preoperative patients completed the ODI (14) and visual analog scale (VAS) for back and leg pain and, at follow-up, the ODI, VAS, and SRS-30 (15) questionnaires at follow-up. Demographic, comorbidity, and surgery-related data were collected from individual patient records. Patients were divided into satisfied (satisfied or very satisfied) or not satisfied (dissatisfied, very dissatisfied, or cannot tell) groups, depending on the answer to SRS-30 question 21 asking about satisfaction with the management of their spinal condition. The ODI was scored as 0–100 points, with a threshold value of ⩾40 representing severe disability. The SRS-30 domains were scored as 1–5 points, with high values indicating a good outcome score.
Statistics
The data are presented as means with standard deviations (SDs) and 95% confidence interval (CI), as minimum–maximum, or as counts with percentage. The characteristics of the study population are presented as means with SD or as counts with percentages. Statistical comparison between the groups was performed with a t-test, permutation test, chi-square test, or Fisher–Freeman–Halton test when appropriate. Repeated measures for radiographic parameters were analyzed using generalizing estimating equation models with an unstructured correlation structure. Kaplan–Meier curves were used to illustrate information on the cumulative risk of reoperation. The 95% confidence bands for the Kaplan–Meier estimate were calculated using the bootstrap method. Multivariate logistic regression was used to estimate odds ratios (ORs) and 95% CIs for poor outcomes. Correlation coefficients were calculated using Pearson method. Stata 15.0 (StataCorp LP, College Station, TX, USA) was used for analysis.
Results
The analysis included 79 patients, with median 65.0 (22–79) and mean (SD) age 64.3 (10.3) years, and 57 (72.2%) were female. The baseline data of diagnoses, comorbidities, complications, and operative methods are presented in Table 1. Men were significantly younger than women, 58.1(13.7) years versus 66.7(7.6) years (SD), respectively, (p < 0.001). Men had different indications for surgery (p = 0.043) and more neuromuscular comorbidities (p = 0.042) than women, of whom the majority had degenerative sagittal malalignment or scoliosis. No surgery-related deaths or deaths within 90 days postoperatively were found.
Descriptive data after adult spinal deformity corrective surgery: mean (SD) and count with percentage.
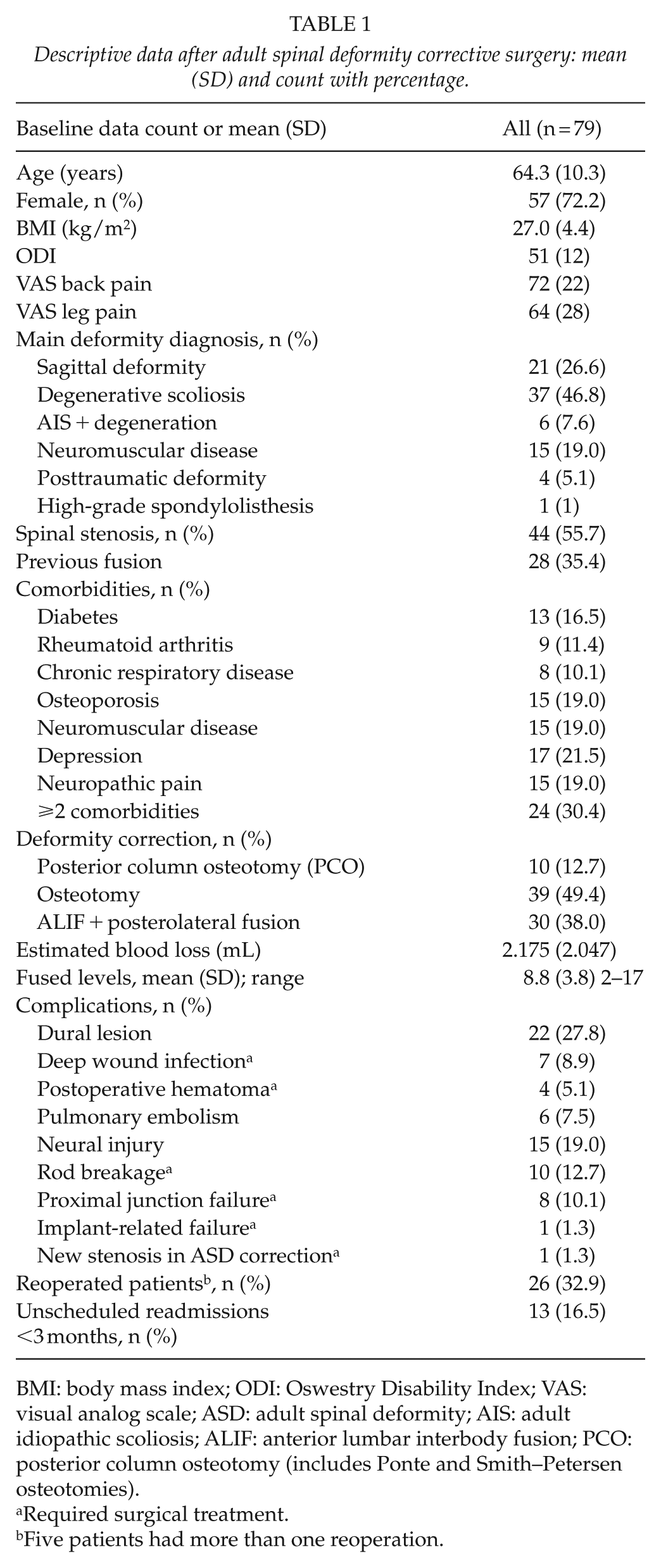
BMI: body mass index; ODI: Oswestry Disability Index; VAS: visual analog scale; ASD: adult spinal deformity; AIS: adult idiopathic scoliosis; ALIF: anterior lumbar interbody fusion; PCO: posterior column osteotomy (includes Ponte and Smith–Petersen osteotomies).
Required surgical treatment.
Five patients had more than one reoperation.
The ODI score decreased from 51 (12) to 34 (20), the VAS back pain score decreased from 72 (22) to 29 (26), and the leg pain score decreased from 64 (28) to 35 (30) mm, and the scores were significantly better (p = 0.001) at follow-up than at baseline. Of 15 (19%) patients with a postoperative motor deficit, 10 were reversible; 4 were irreversible; and 1 had a thoracic spinal cord infarct and paraparesis during the postoperative night. All patients with irreversible neural deficits recovered ambulation.
Radiographic sagittal parameters TPA, PT, TK, and PI-LL improved with surgery and the improvement was maintained at 4–5 years of follow-up (p ⩽ 0.001). SVA deteriorated after 2 years of follow-up but was still significantly better than at baseline after 5 years of follow-up (p = 0.043; Fig. 1). T1S increased minimally after the first postoperative year, but after 3 years, the decline in the angular parameter compared to that at baseline was significantly greater (p < 0.001; Fig. 1). A total of 12 patients had >10° added PJK and five had added lordosis without failure of the bone or implant or spinal stenosis at the proximal junction during follow-up compared to the immediate postoperative radiograph. None of the patients had implant- or bone-related complications at the distal junction of fusion. A total of 64 (81.0%) patients had fusion to the ilium and 11 (13.9%) to the sacrum.
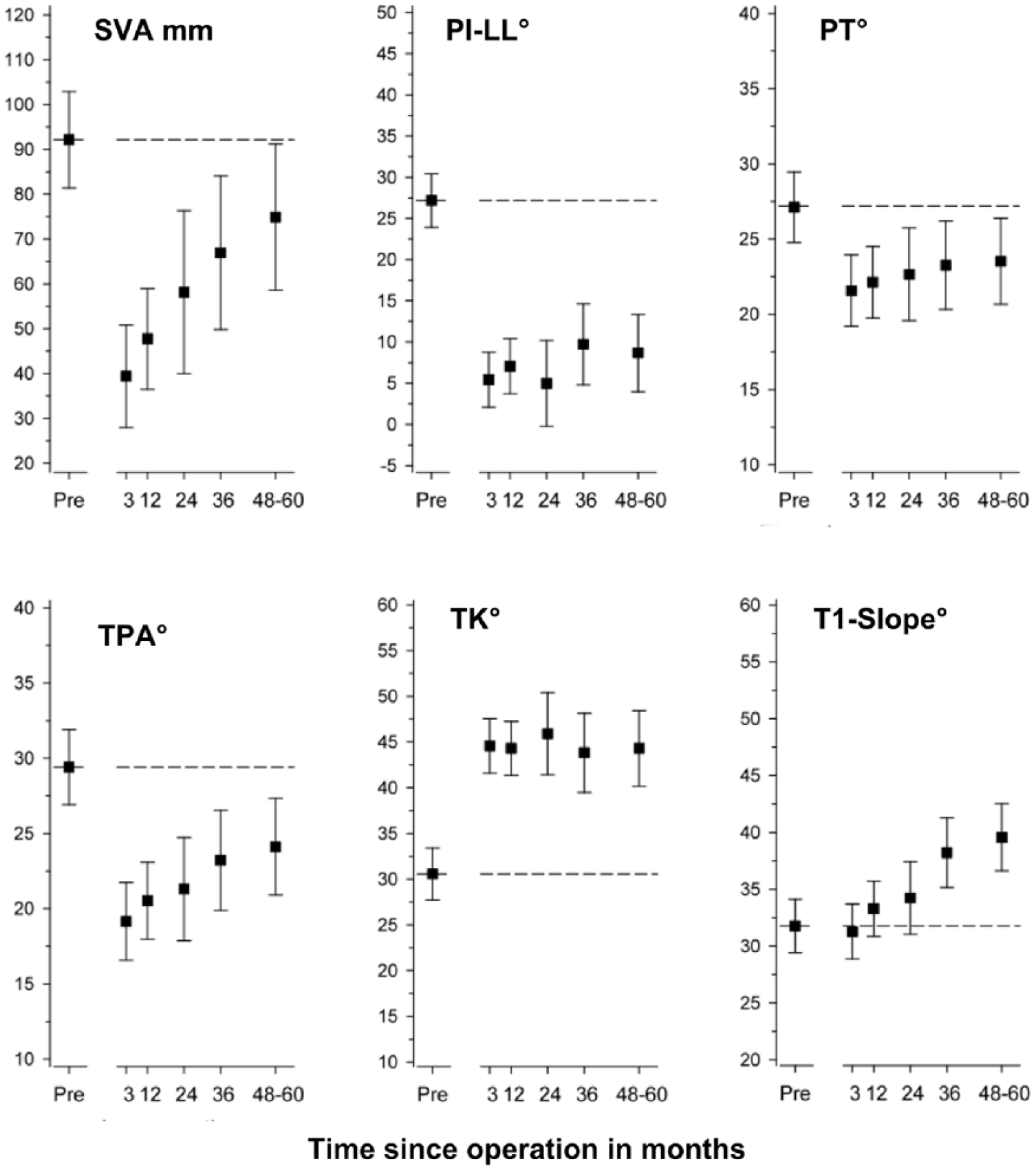
Preoperative and postoperative repeated measurements of the radiographic parameters with 95% confidence intervals after adult spinal deformity correction.
Risk for the first reoperation due to mechanical failure of instrumentation or bone was highest within the first year at 13.9% (95% CI = 8.0%–23.7%) and increased to 29.8% (95% CI = 19.4%–43.9%) during the 5-year follow-up (Fig. 2). Of 10 patients who underwent reoperation during the primary admission, 6 had deep or superficial wound infections and 4 had hematomas.
One patient had recurrent infection 4 years after the index surgery. Rod breakage was associated with chromium cobalt (CrCo) material in two-rod constructs (p = 0.003) and an increased number of fused levels (p = 0.004). Proximal junctional failure (PJF) was correlated with osteoporosis (p = 0.018). The severity of deformity, amount of correction, and other comorbidities were not significantly different between patients with and those without mechanical complications (Table 2).
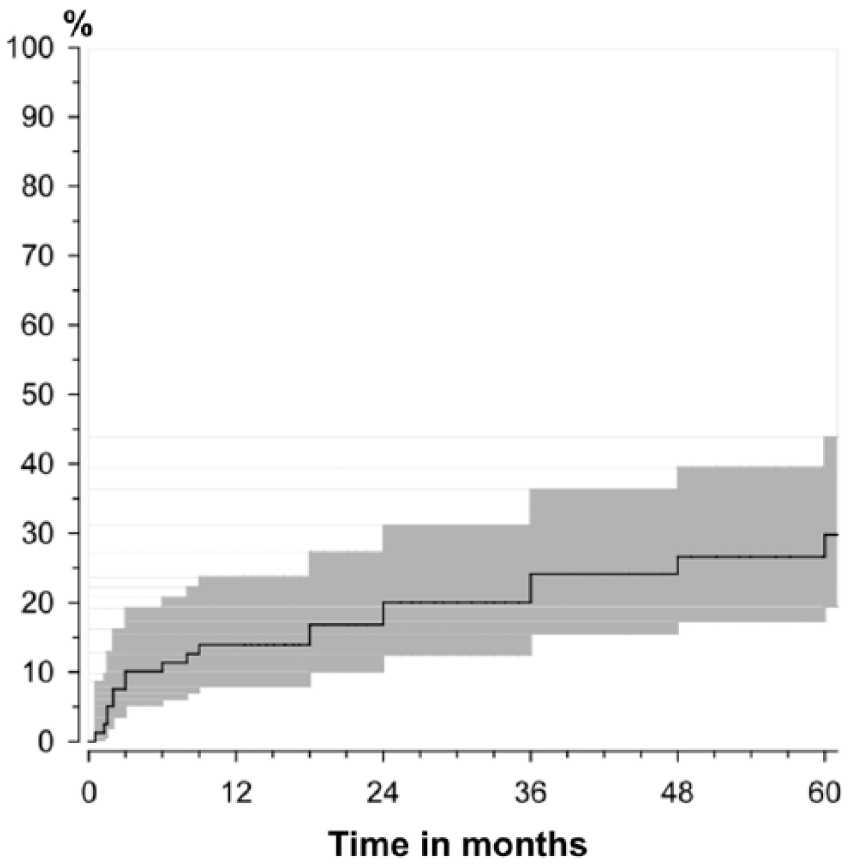
Probability (95% confidence interval) of the first reoperation after discharge from primary surgery. One year: 13.9% (95% CI = 8.0%–23.7%); cumulative probability at 5 years: 29.8% (95% CI = 19.4%–43.9%). Risk of reoperation for a mechanical problem was highest during the first postoperative year.
Mechanical complications after discharge from hospital: mean (SD) or count and percentage with statistical significance (*p<0.05) (t-test).
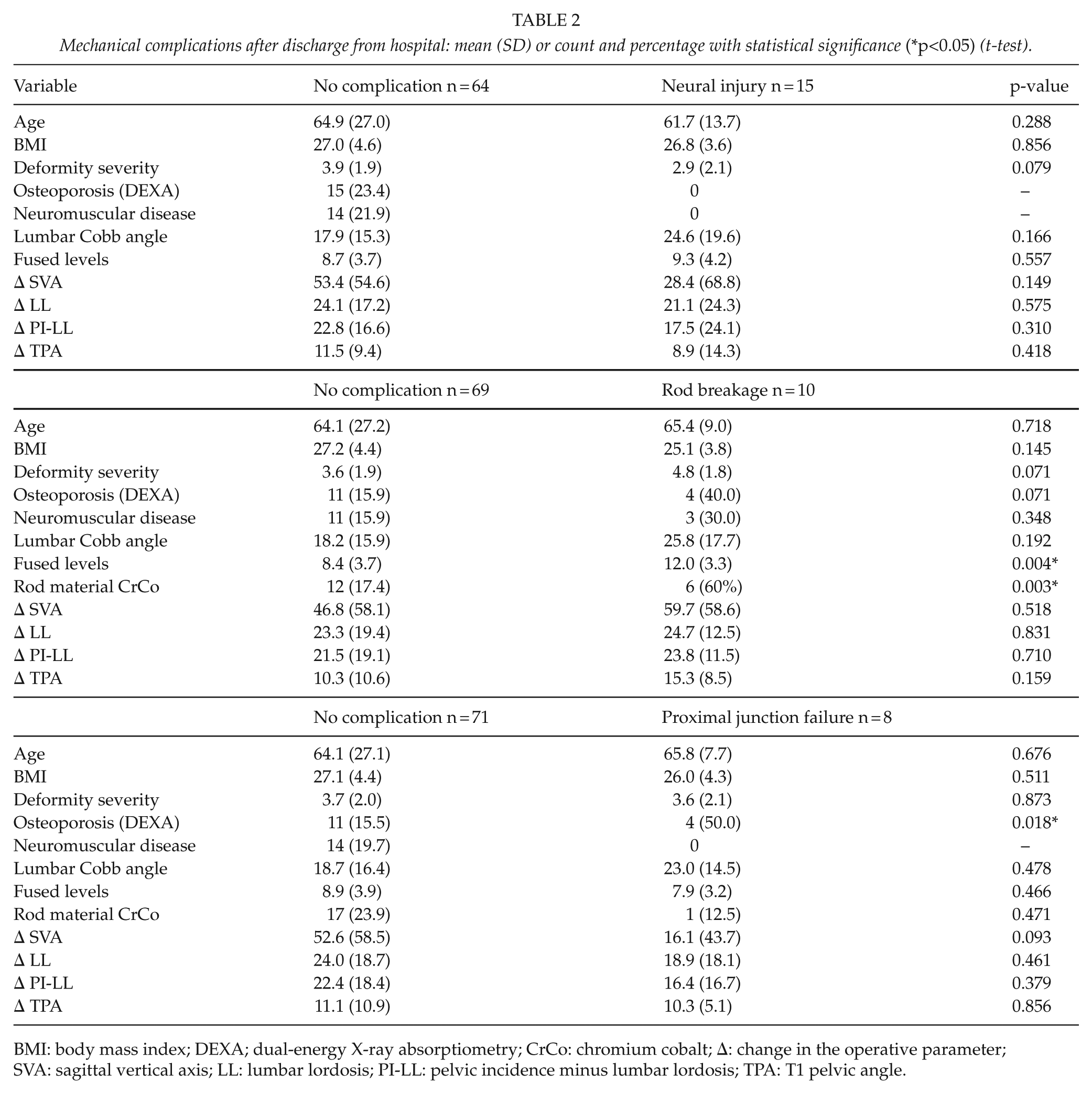
BMI: body mass index; DEXA; dual-energy X-ray absorptiometry; CrCo: chromium cobalt; Δ: change in the operative parameter; SVA: sagittal vertical axis; LL: lumbar lordosis; PI-LL: pelvic incidence minus lumbar lordosis; TPA: T1 pelvic angle.
According to SRS-30, 49 (62.0%) patients were satisfied or very satisfied with the treatment, and 57 (72.1%) would have the same operation again; 15 (19.0%) were neither satisfied nor dissatisfied, and 11(13.9%) were not sure about having the same operation. Among radiological parameters, only insufficient SVA correction and residual sagittal malalignment were correlated with patient satisfaction (p = 0.027). In other radiographic parameters, the amount of correction did not affect patient satisfaction. The SRS-30 total score was 3.28 (0.76). The best score in SRS-30 domains at follow-up was in Satisfaction with management, at 3.59 (1.10), and the worst was in Function, at 2.97 (0.91). At follow-up, the ODI and SRS-30 total scores showed a good correlation at r = −0.78 (95% CI = −0.86 to −0.68; p < 0.001); the patients satisfied with management had the best scores in both measures and vice versa (Fig. 3). The predictive indicators for the poorest 20th percentile outcome of ODI and/or SRS-30 scores were male sex and depression (Table 3).
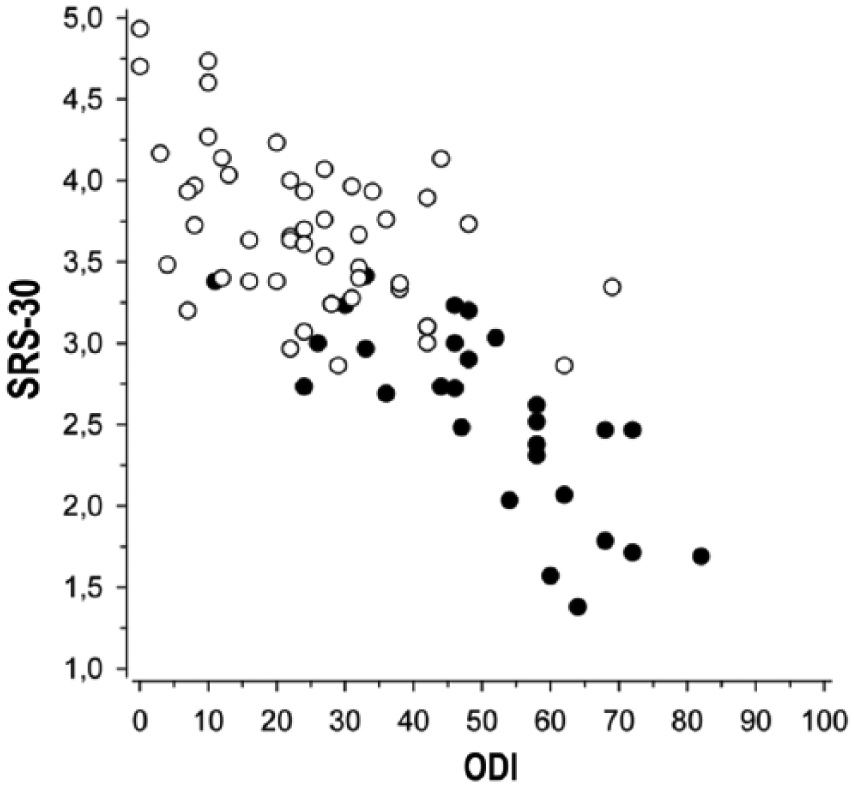
Correlation of SRS-30 and ODI total scores (r = −0.78; 95% CI = −0.86 to −0.68; p < 0.001) with distribution of patients satisfied (white dot) or dissatisfied (black dot) with spine management.
Predictive parameters for poor outcomes: patients with the worst 20th percentile of SRS-30 and/or ODI scores.
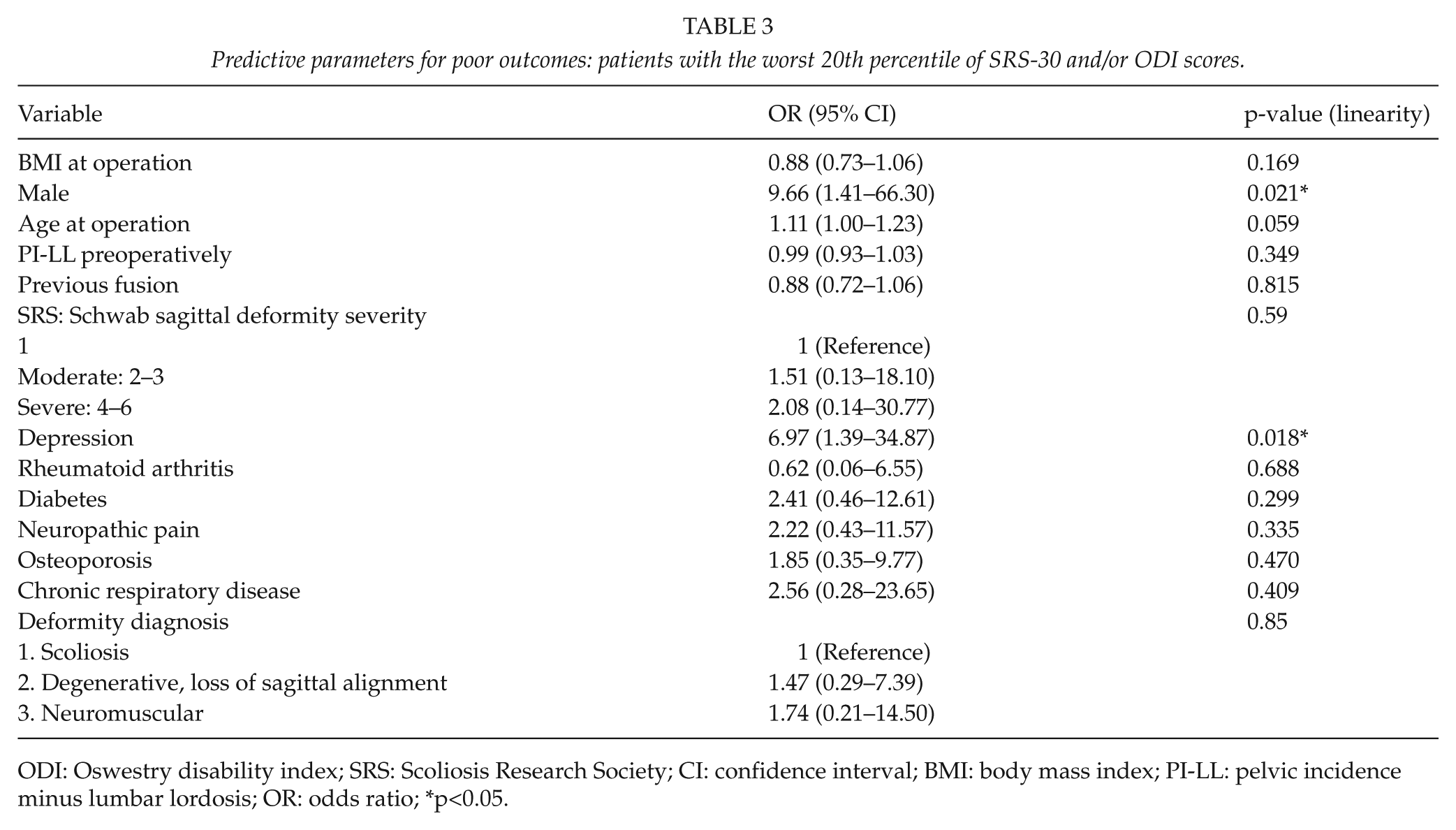
ODI: Oswestry disability index; SRS: Scoliosis Research Society; CI: confidence interval; BMI: body mass index; PI-LL: pelvic incidence minus lumbar lordosis; OR: odds ratio; *p<0.05.
Discussion
Surgery for degenerative spinal deformities is often performed in patients with several medical comorbidities rather than in healthy individuals. Our cohort was similar to surgically treated patients in previously published studies comparing operative and conservative treatments for ASD (5, 16). In this cohort, the correction of spinal alignment remained stable, and patient satisfaction and clinical outcomes were good despite typical deformity surgery-related complications.
The patients in this study were selected for elective surgery after a multidisciplinary process for somatic and psychological properties. ASA3 anesthesia risk class allows even severe comorbidities, but in this cohort, the medical conditions were properly stabilized preoperatively. Cardiac and vascular diseases were not analyzed as comorbidities, as these conditions were managed before surgery or patients were treated conservatively owing to excessive surgical risk. Even with these precautions, the typical perioperative complications for ASD surgery emerged to some extent.
In our study, indicators of global spinal alignment, that is, SVA and TPA, showed significant correction as good as PI-LL, which is the main surgical target for the correction of ASD (16). Whereas, PI-LL remained stable, the parameters dependent on sagittal balance, that is, SVA and TPA, started to deteriorate during the 5 years of follow-up. The T1S angle started deteriorating in parallel to the loss of global alignment, without changes in TK. PJK explained only a small part of the loss of sagittal balance. Successful surgical correction did not stop the deterioration of sagittal balance in our patients, but the long-term radiographic alignment and clinical outcome (ODI, VAS) remained significantly better than those at baseline.
High pelvic retroversion (by PT) is a compensation mechanism for lost sagittal alignment and results in hyperextension of the hip joint and loss of natural gait. PT correction in our study was significant, but the mean preoperative and postoperative values were both in SRS-Schwab modifier class + (20°–30°) of moderate sagittal disorder (17). The PT values also did not reach the PI-related optimum values of PT = 0.37*PI-7 described earlier among asymptomatic patients by Vialle et al. (18). Also Kondo et al. (19) found that even PT remains high in patients with thoracolumbar fusion to the pelvis and can improve balance and gait when the deformity is adequately corrected, which supports our results.
In this study, reoperations were divided into immediate events during the primary admission and those occurring late after discharge following the first operative treatment. Mechanical complications appeared after discharge from primary ASD surgery. The cumulative probability of reoperation in our study was highest during the first postoperative year, consisting mostly of PJF and mainly rod breakage thereafter. Scheer et al. (20) found similar results, except that their percentages at the 1- and 2-year follow-ups were higher. The known risk factors of PJF are a large degree of correction of coronal curves and sagittal malalignment, long fusion, older age, poor bone mineral density (BMD), previous fusion, and fusion to the pelvis (21). Our study only found a correlation with low BMD, fusion length, and PJF. This may be because of meticulous planning of surgery as well as choosing the method of correction aimed at optimal age- and PI-related sagittal correction. In the earlier cases in this study, the method of securing the proximal junction was different: transverse process hooks and sublaminar bands instead of vertebroplasty, perforated cemented pedicle screws (22), and off-label use of teriparatide (23), which may cause bias in our results.
CrCo 6.35-mm rods were used during 2010–2013, with the expectation of better coronal reduction capacity and greater ability to resist breakage than titanium rods. The rods functioned as expected perioperatively but were associated with a great amount of rod breakage at the area of maximal rod bending, which was also the site of maximal surgical correction of lordosis. Especially in osteotomies, the frequency of rod breakage was considerable and led to a change in the operative technique during the follow-up period, with the use of multiple hybrid 6.35/5.5 mm titanium (Ti) rods. In contrast to our study, Han et al. (24) found that CrCo material used in ASD fusion to the sacrum was more resistant to rod breakage but increased the amount of PJK. They used multiple CrCo rod constructs instead of a two-rod Ti construct, in contrast to the rod amounts used in our study. Our study population had no cage-, bone graft–, bone substitute–, or screw-related complications or reoperations, which have been described in other studies (25).
Surgical treatment is effective when spinal deformity is associated with pain and loss of function (6), despite the rate of complications and reoperations (26). In our study, patient satisfaction showed a linear correlation with the ODI and SRS-30 total scores, and these PROMs had a good mutual correlation. The ODI measures disability in relation to pain, but the SRS-30 also asks preoperative and postoperative questions about the managements’ effect on pain, function and activity, mental health, self-image, and satisfaction with surgical treatment. The majority of adult deformity patients considered pain relief as the best postoperative change and were satisfied with management, even among the patients whose level of activity or self-image remained unchanged or decreased after extensive spinal correction and fusion. This is supported by a previous multicentre study (27), according to which a pan-lumbar arthrodesis, irrespective of the proximal fusion end-point, does not deteriorate patient satisfaction on functional status. Scheer et al. (28) found that reduction of back pain improves outcomes more than reduction of leg pain. This may explain the high patient satisfaction in our study, despite preoperative or postoperative neuropathic symptoms, as the deformities were significantly corrected.
Hamilton et al. (12) found that patient satisfaction is not correlated with radiographic parameters or complications and only is moderately correlated with HRQoL measures, in partial contrast to our results. We tested both absolute radiographic values as well as the amount of individual change in radiographic parameters against patient satisfaction and found no correlation, except with regard to inadequate SVA correction and residual sagittal malalignment. Scheer et al. (29) reported a correlation between poor radiographic correction of sagittal alignment and worse outcome, and Yamada et al. (30) found that patients who achieved good SVA were satisfied, even when their LL correction was suboptimal, which support our results.
When many common risk factors such as advanced age and frailty, ASA risk class ⩾4, untreated severe osteoporosis, poor cooperation, body mass index (BMI) >35, and smoking were excluded in our analysis, only male sex and depression were found to be risk factors for a poor outcome measured with ODI and SRS-30. Depression, BMI, and severe baseline back and leg pain were risk factors for poor outcomes in a study by Smith et al. (31), but there was no association with sex. In our study, the baseline disability and pain were similar between sexes and did not predict poor outcomes in ODI or SRS-30. The male individuals in our cohort were younger, and their operative diagnoses consisted mainly of neuromuscular diseases, spondyloptosis, and post-fracture kyphosis, whereas the female individuals predominantly had degenerative sagittal or coronal deformities. This difference may bias the elevated risk ratio of the male individuals in our surgical cohort.
Limitations of the study were a small population with multiple etiologies of spinal deformity and limited baseline HRQoL measures. To our knowledge, this is the first analyzed and published study on radiological, clinical, and PRO results among Finnish ASD surgery patients. The strengths of the study were the long-term follow-up, the consecutive patient cohort representing the population of the area and the fact that patients were selected and operated upon by the same surgical team.
Conclusion
Long-term radiographic and patient-reported clinical outcomes after ASD surgery remained significantly better than those at baseline. Meticulous patient selection does not prevent all complications, but good patient satisfaction and outcomes can be achieved regardless of adverse effects. Risk for reoperation is highest during the first postoperative year. Depression was the only significant predictive factor for poor outcome after ASD surgery, independent of sex or indication for surgery.
Footnotes
Acknowledgements
Secretary Riitta Minkkinen’s efforts guaranteed good coverage of the follow-up outcome questionnaires.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved on 23 October 2012 by the Research Ethics Committee of the Central Finland Health Care District (identification: 17U/2012).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KK is currently receiving grants from Finnish Government Health Research Funding (grant no: B16201) and the Central Hospital of the Central Finland Scientific Committee Temporary Fund.