
Abstract
Background:
Some hip fracture patients need one or more reoperations because of complications following initial operative treatment.
Aims:
The aim of this study was to identify all further surgical interventions in a cohort of patients with hip fractures over a period of 8 years after index fracture. Immediate direct costs of these reoperations were also calculated.
Material and Methods:
This retrospective study investigated 221 consecutive patients with hip fractures operated on at two different hospitals in southeastern Finland. The study period in hospital A was from 1 February 2003 to 31 January 2004, and in hospital B from 1 February 2003 to 30 April 2004. About 50% were femoral neck fractures, 41% trochanteric fractures, and 9% subtrochanteric fractures. Patients’ medical records were checked from the hospital records and confirmed manually. Short- and long-term complications were recorded. Survival analysis was performed using a life-table method. The actual costs for reoperations and other further procedures for each patient were calculated using diagnosis-related groups–based costs for both hospitals in 2012.
Results:
A total of 20 patients (9%) needed reoperations. Overall, 10 patients (8.9%) with a femoral neck fracture (n = 112), 8 patients (8.7%) with trochanteric fracture (n = 92), and 2 patients (10.5%) with subtrochanteric fracture (n = 19) were reoperated on. The median interval between the primary operation of the acute hip fracture (n = 20) and the first reoperation was about 300 days (range: 2 weeks to 82 months). Among the women reoperated on, the excess mortality was lower than among those undergoing a single operation. The median costs of treatment per patient with one or more reoperations were €13,422 in hospital A (range: €1616–€61,755), €11,076 in hospital B (range: €1540–€17,866), and €12,850 in the total study group (p = 0.43). In the case of infections (3 patients), the mean costs per patient were €28,751 (range: €11,076–€61,755).
Conclusions:
Almost 10% of hip fracture patients required reoperations, and these reoperations caused significant direct costs to health care. However, direct costs account for only approximately 25% of the first year’s total costs. These costs should be taken into account when evaluating the economics of hip fractures and the burden of health care.
Introduction
Hip fracture is the most common reason for surgery after injury among the elderly people. More than 7000 (7300 in 2010, unpublished data) new hip fractures occur in Finland (population 5.3 million) every year, with an annual cost of €21,700 per patient in 2009 (1). According to an earlier Finnish prospective study, the average annual costs per patient were approximately 2.5 times higher for patients who lived in the community prior to the fracture but after which remained in institutional care (2). Reoperations decrease the likelihood of patients returning home postoperatively (3).
The surgical treatment of hip fractures is somewhat controversial, and many national guidelines have been published (4–7). According to the literature, most of the studies concerning reoperations are short-time follow-up studies (30 days to 4 months) (8, 9). Some studies with a longer follow-up period (1–5 years) have also been reported (10–13).
The aim of this study was to identify all further surgical interventions after the initial operative treatment of patients with hip fractures with a follow-up period of 8 years and to calculate the immediate direct costs of the reoperations.
Material and Methods
Originally, we prospectively collected 221 consecutive patients with operated hip fracture (index fracture, diagnoses S72.0–S72.2) (International Classification of Diseases–10, ICD-10) at Päijät-Häme Central Hospital (A), located in the city of Lahti, and at North Kymi Hospital (B), located in the city of Kouvola, in southeastern Finland. The study period in hospital A was from 1 February 2003 to 31 January 2004 (12 months), and in hospital B from 1 February 2003 to 30 April 2004 (15 months). Written informed consent was obtained from all patients or from their relatives. The study design has previously been described in detail (14).
Medical records of all patients were checked manually by the authors (P.L., T.H., and J.P.K.) to confirm all reoperations after the index hip operation. The records of hospitals and local health-care centers were reviewed. The follow-up time was 8 years. The follow-up protocol was approved by the local ethics committees.
Immediate direct costs of reoperations for each patient were calculated using the diagnosis-related groups (DRG)-based prices of both hospitals in 2012. One patient was reoperated on in a private clinic, and the cost was identified from the clinic’s price list in 2012.
Survival analysis was performed using the life-table method. In this method, the observed survival rates of the groups are compared with survival rates based on sex- and age-specific life tables for the whole population of the same age in Finland. The calculations of the survival rates are based on the individual life expectancies of the target population for the target years (reference population) (15, 16). The relative survival curve of the reference population would be 1.00. If the survival curve of the group remains below the survival of the reference population, there is excess mortality in the group (Fig. 1). The deaths were obtained from the Finnish Cause of Death statistics. The follow-up time of survival was from 1 February 2003 to 2 May 2011 (98 months = 8 years).
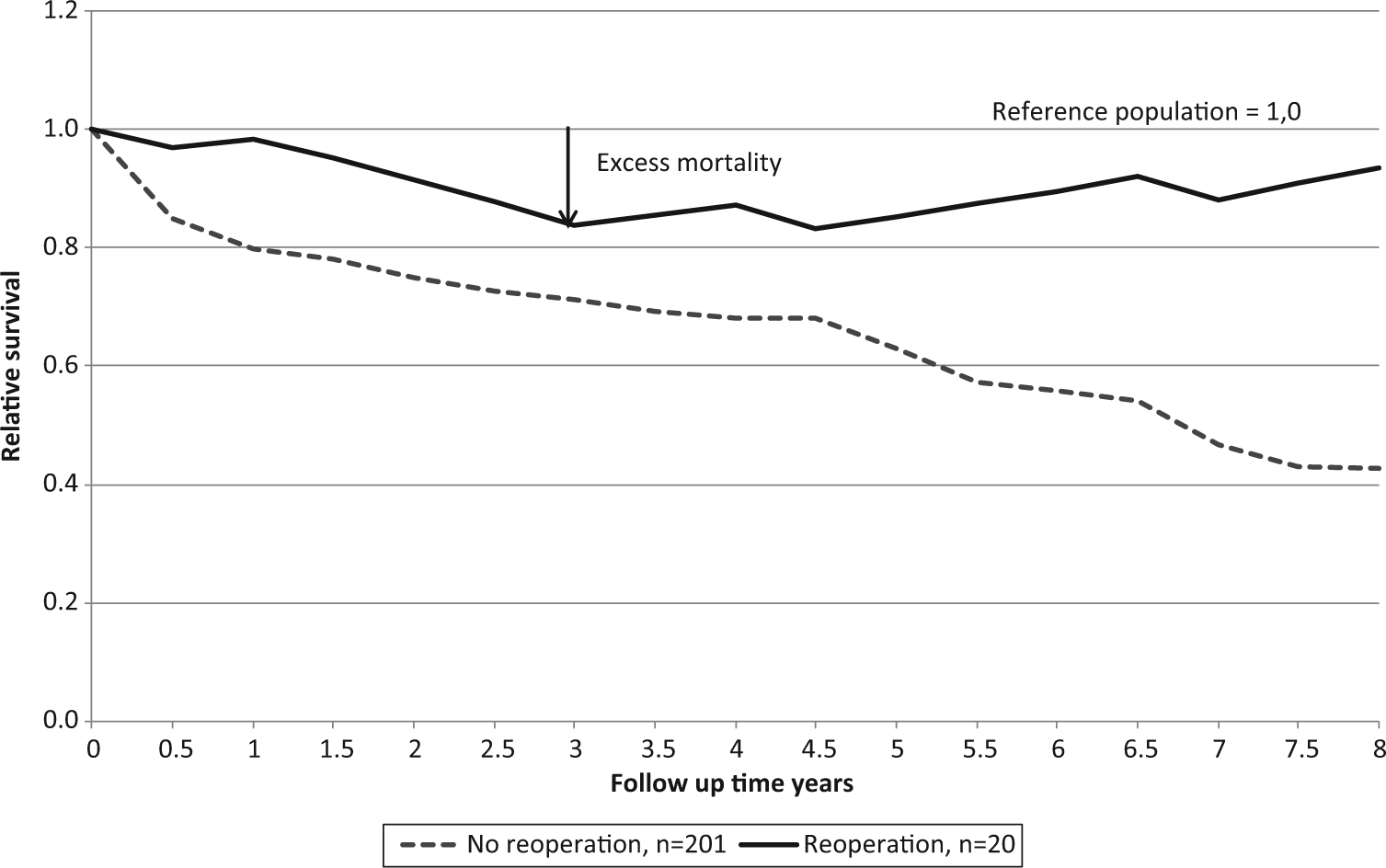
Survival of reoperated and not reoperated hip fracture patients.
Statistical Analysis
Differences between the groups were analyzed using the t-test, two-way analysis of variance (ANOVA), and Chi-square test. Fisher’s exact test was used when appropriate. The Greenwood formula was used in testing the expected and observed death rates within the groups.
Results
During the primary study, a total of 221 consecutive patients (156 women and 65 men) with an acute hip fracture were enrolled in the study: 120 patients in hospital A and 101 patients in hospital B. In hospital B, there were 2 patients who sustained a second hip fracture on the contralateral side during the primary study. The total number of hip fractures was thus 223. The mean age of females at the time of the index hip fracture was 80.5 years (standard deviation (SD) = 10 years) and that of males was 73 years (SD = 12 years; p < 0.001). Only 5 patients were younger than 50 years of age (range: 47–49 years). In the baseline patient characteristics (sex and age), there were no significant differences between the two hospitals (14).
The hip fractures were distributed as follows: 50% were femoral neck fractures, 41% trochanteric (per- or intertrochanteric) fractures, and 9% subtrochanteric fractures. All hip fractures were operated on according to standard procedures used in 2003–2004: femoral neck fractures with two or three cannulated parallel screws or dynamic hip screw (DHS), with hemiarthroplasty or total hip replacement. Trochanteric and subtrochanteric fractures were operated on using a DHS or an intramedullar nail. All patients were operated on.
Reoperations
A reoperation was performed on 20 of 221 patients (9%): on 13 of 120 patients (10.8%) in hospital A and on 7 of 101 patients (6.9%) in hospital B (p = 0.316). Reoperations among patients with a femoral neck fracture were performed in 10 of 112 cases (8.9%), among patients with trochanteric fracture in 8 of 92 cases (8.7%), and in patients with subtrochanteric fracture in 2 of 19 cases (10.5%) (Table 1).
Patients with reoperations (n = 20).

Neck: femoral neck fracture; Troch: trochanteric fracture; AM: Austin-Moore endoprosthesis; TH: Thompson endoprosthesis; DHS: dynamic hip screw; Screw: 2 or 3 cannulated screws; IMN: intramedullary nail; THA: total hip arthroplasty; HA: cemented hemiarthroplasty; PJI: prosthetic joint infection.
Private clinic price.
The femoral neck fracture was noticed before the reoperation. Before the primary operation the fracture was classified as a pertrochanteric fracture.
In hospital A, 68 patients had a femoral neck index fracture. Of these patients, 37 were operated on using uncemented hemiarthroplasty, 14 with cemented hemiarthroplasty, 5 with total arthroplasty, and 12 with cannulated parallel screws or DHSs. In hospital B, 43 patients had a femoral neck index fracture. One of these patients simultaneously had a pertrochanteric fracture. Of these 43 patients, 31 were operated on using cemented hemiarthroplasty, 1 with total arthroplasty, and 10 with cannulated parallel screws or DHSs. The most common reasons for reoperations in patients with femoral neck fracture were aseptic loosening of uncemented hemiarthroplasty, avascular necrosis of the femoral head, or nonunion of the fracture. In cases with trochanteric or subtrochanteric fractures, the most common reasons for reoperations were, correspondingly, nonunion of the fracture, penetration of the screw, or failure of the osteosynthesis (Table 1).
The median interval between the primary operation of the acute hip fracture and the first reoperation (n = 20) was about 300 days (range: 2 weeks to 82 months). In 8 patients, more reoperations or closed reductions were needed (3 cases in 2 weeks after the first reoperation, 1 case in 2 months after the first reoperation and 4 cases in 2 months after the second reoperation). One patient needed eight operations.
Postoperative deep wound infection was a reason for one reoperation (0.4%; 1/223). In two further procedures, the reasons were deep wound infection and a prosthetic joint infection (PJI) (10%; 2/20)
Mortality and Survival
At the end of the 8-year follow-up, 74% (164 of 221) of the patients, 77% (120 of 156) of women and 67% (44 of 65) of men had died. There were no differences in mortality between the hospitals.
At the time of the index hip fracture, the mean age of the 7 men reoperated on was 66.8 years (SD = 15.7) and that of the 13 women reoperated on was 74.6 years (SD = 10.3; p < 0.001). The mean ages of the men (74.1 years (SD = 11.0)) and women (81.9 years (SD = 9.6)) undergoing a single operation were higher than for those who were reoperated on (p < 0.01). At the time of the first reoperation, the mean age of the seven men reoperated on was 67.6 years (SD = 15.7) and of the 13 women reoperated on 76.1 years (SD = 10.8; p = 0.18).
At the end of the 8-year follow-up, 13 of the 20 patients reoperated on were still alive (4 men and 9 women; mean age in women 79.8 years and in men 67.4 years). A total of 7 patients reoperated on died during the follow-up (3 men and 4 women; mean age in women 83.3 years and in men 78.3 years).
The mean age of the surviving women who were reoperated on and that of the surviving women undergoing a single operation were similar (79.9 years). Correspondingly, the mean age of the 4 surviving men who were reoperated on (67.5 years, SD = 17.1) was lower than the mean age of the 17 surviving men undergoing a single operation (78 years, SD = 12.2; p = 0.17)
The excess mortality was lower among patients reoperated on than among those who were not (Fig. 1). However, this was noticed among women only (Fig. 2). More deaths than expected were observed among women undergoing a single operation (p < 0.001).
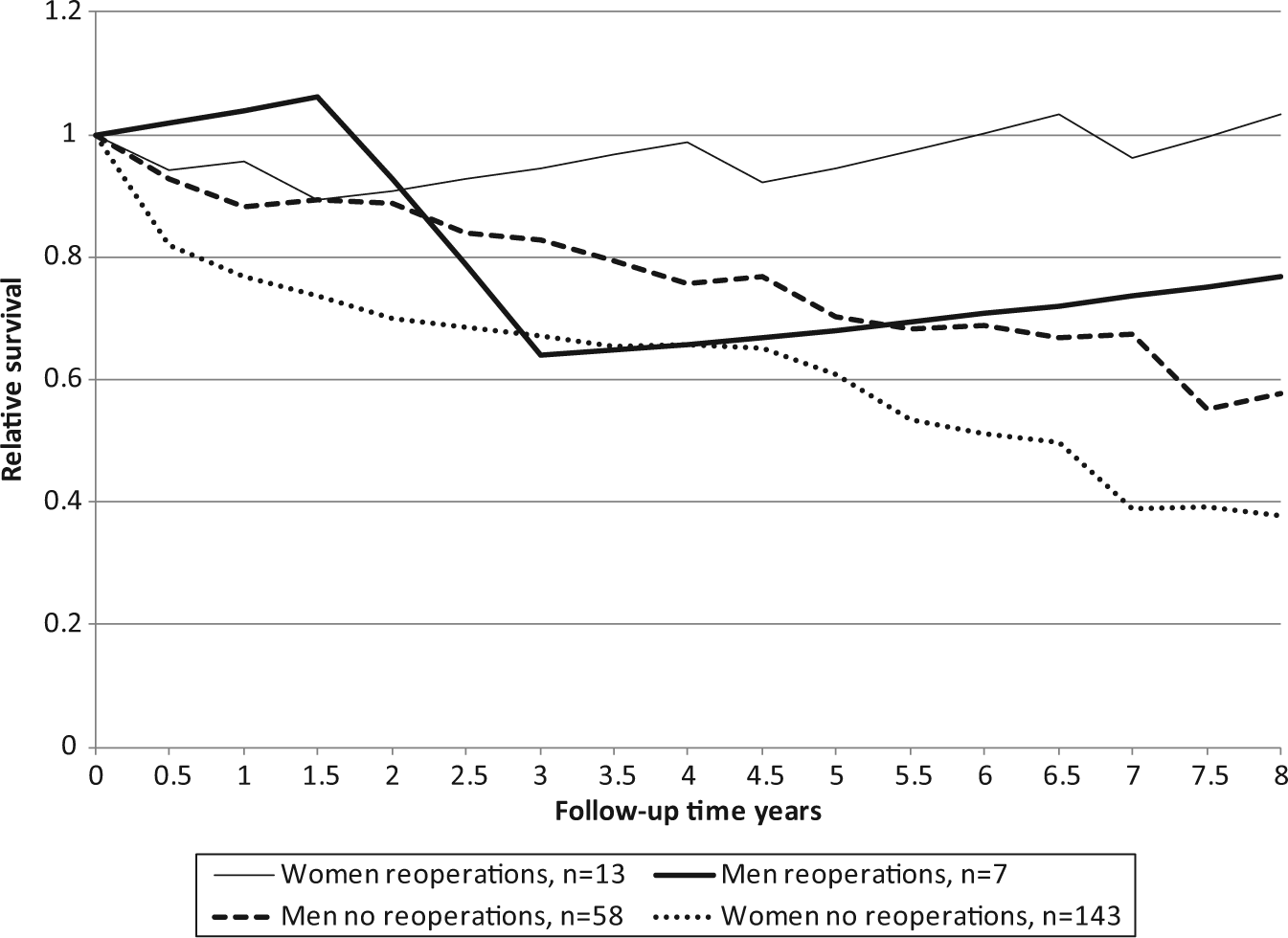
Survival of reoperated and not reoperated hip fracture patients according to gender.
Costs
The total direct costs of reoperations were €282,211: €206,275 in hospital A and €75,946 in hospital B (Table 1). The median costs of treatment per patient with one or more complications were €13,422 in hospital A (range: €1616–€61,755), €11,076 in hospital B (range: €1540–€17,866), and €12,850 in the total study group. There were no significant differences in the costs between the two hospitals (p = 0.43) or between genders in either hospital (p = 0.26). In the case of deep infections, the mean costs per patient (3 patients) were €28,751 (range: €11,076–€61,755) (Table 1).
Discussion
This study is one of the longest follow-up studies in the literature analyzing reoperation rates and costs following hip fracture. The main objective of hip fracture treatment among the elderly is to ensure that the patient returns home and recovers his or her pre-fracture level of function. This represents a challenge in treating these patients. Reoperations are needed fairly often, especially regarding femoral neck fractures.
A major strength of our report is that we manually checked all patients’ hospital and primary health-care center records in order to obtain all reoperations after the index hip fracture. This improves the reliability of our study. The possibility of some cases being missed because patients were reoperated on in other hospitals was minimal. If this were the case, the aftercare of these patients would have taken place in the study hospitals or in the local health-care centers, and thus included in our study. We noticed one patient who was reoperated on in a private clinic, with the aftercare taking place in the local health-care center.
The major limitation of this study is that the number of reoperations was small. In addition, we only counted the costs of reoperations in acute hospital care. Hence, the costs of health center stay, nursing home stay, municipal home care, visits to the outpatient department, patients’ own share of the hospital and outpatient department costs, transportation costs, and extra medication costs remained uncounted (2).
According to the Norwegian Hip Fracture Register, of the 35% of reoperations performed in a 1-year follow-up of 14,757 undisplaced and displaced femoral neck fractures, 11% were undisplaced fractures operated on with internal fixation, 21% were displaced fractures operated on with internal fixation, and 3% were displaced fractures operated on with hemiarthroplasty (12). The Swedish National Hip Fracture Register from 2010 reported the 20% reoperation rate in treating femoral neck fractures being made up of 9% with osteosynthesis, 6% with hemiarthroplasty, and 5% with total arthroplasty (follow-up time = 0.5–1.5 years) (17). In patients with trochanteric fractures, the reoperation rate was only 2% (plate and screws) and 3% (short intramedullary nail) (17). Results from the Finnish National Database study of 14,915 patients treated for trochanteric fracture with extra- or intramedullary implants showed a reoperation rate of 11.1% in the first year (95% confidence interval (CI) = 10.4%–11.8%) versus 8.9% (95% CI = 8.1%–9.7%), respectively (p < 0.0001) (18).
In this study, 9% of the patients required one or more additional operations as a result of a complication of the primary operation. Of the first reoperations, 65% were performed during the first year after treating the acute hip fracture, and 85% within 2 years. Only 10% of the first reoperations were performed after 3 years. A Swedish study reported a reoperation rate of 18% for basicervical hip fractures after a median follow-up of 4.8 years (range: 2.2–8.8) (19). Of the first reoperations, 80% were performed within 1 year and 92% within 2 years (19).
A previous study showed that reoperations for a fractured hip after the failure of the primary operation are associated with an increased mortality shortly after the second operation, but return to normal compared to those for the standard population within 6 months postoperatively (20). Another recent study showed no significant difference in mortality in the first 3 months between patients reoperated on and controls (3). However, after that time, mortality among patients reoperated on was significantly higher than in the control group, and these patients were less likely to return to their own home (3). Our study reported better survival rates in women reoperated on than in those who were not. This is most probably explained by the higher mean ages at the time of index fracture of the women undergoing a single operation compared to those reoperated on. However, at the end of follow-up, the women had the same mean age, whether reoperated on or not. In our previous study, the excess mortality after primary operation was lower among men than women (11%, 13%, 20%, and 22% at 1, 2, 3, and 4 years postoperatively, respectively, vs 23%, 28%, 26%, and 38%) (16).
The Finnish National Hip Fracture Database of PERFormance, Effectiveness and Costs of Treatment episodes (PERFECT) includes hospital-specific follow-up data for at least 1 year for each patient and currently covers the period 1999–2009 (1). The PERFECT database includes information on all inpatient and outpatient hospital care, residential home care and care in service homes with 24-h assistance, special reimbursements, prescription drug purchases, and deaths (1). Furthermore, it includes information on hospital-specific costs of all hip fracture patients during the period 2007–2009. According to the PERFECT database, the annual average total costs per hip fracture patient in Finland were €21,700 in 2009 (range: €17,205–€25,544): €19,254 in hospital A and €24,000 in hospital B. This does not include possible reoperations.
According to our study, about 10% of all hip fracture patients needed one or more reoperations, and the total average immediate direct costs per patient due to reoperations were about €14,110, which should be taken into consideration when counting the total costs in hip fracture treatment. However, these costs were caused only by acute care. According to an earlier Finnish prospective study on the total 1-year costs in 106 consecutive hip fracture patients, only 25% of all costs were caused by acute hospital care (2). Total 1-year costs are thus about three to four times higher than the acute care costs. In the case of deep wound infections, the corresponding acute care costs were €28,751. Postoperative infections needing reoperations might therefore be over double the additional direct medical costs of acute care compared to other reoperations.
A few important aspects should be contemplated when considering ways of reducing the number of reoperations. The influence of the surgeon’s experience is important in hip fracture treatment. Most hip fractures are operated on during resident duty hours and by surgical residents. According to a Danish study, the rate of reoperations during a 6-month follow-up period in technically demanding hip fracture cases was lower among experienced surgeons or supervised registrars than among unsupervised registrars (8.8% (95% CI = 4.0%–13.5%) vs 17.1% (95% CI = 13.3%–20.8%), p<0.01) (21). Hence, the most technically demanding cases should be operated on during office hours when the best knowledge and better consulting possibilities are more easily available.
In addition to paying attention to the time of surgery, reoperations can be reduced by adjusting the treatment algorithms, as was shown in a Danish study (13). In that study, reoperations were reduced from 18% to 12% by implementing an easy-to-use surgical algorithm for all hip fracture patients. Even though some part of the reduction in these reoperations can surely be explained by better scores according to the American Society of Anesthesiologists physical grading score (ASA grade), particularly in the reduction of infections, treating unstable trochanteric fractures with intramedullary osteosynthesis instead of DHS, and femoral neck fractures more often with prosthesis rather than osteosynthesis, well-considered algorithms will most probably reduce the risk of reoperations. Algorithms could also be used to direct those most demanding cases to office hours.
The index femoral neck fracture patients were operated on in hospital A mainly with uncemented hemiarthroplasty, and in 4 of 37 cases (11%), reoperation was needed. A total of 3 patients (8%) were operated on with uncemented hemiprosthesis and 1 patient with cemented hemiprosthesis. In hospital B, only 1 patient (1 of 31, 3%) in the cemented hemiarthroplasty group needed reoperation. Our results are in line with the results of the Swedish and Norwegian Hip Arthroplasty Registers, which showed that uncemented hemiarthroplasties led to reoperations more often than cemented implants (22, 23).
Conclusion
Hip fractures create a substantial burden on society and the individual. Complications and subsequent reoperations increase this burden substantially. Based on the current data, about 10% of all hip fracture patients operated on needed one or more reoperations during an 8-year follow-up period. Of all reoperations, 85% were performed during the first 2 years after the primary operation. Reoperations, especially in the case of infections, increase the direct and indirect medical costs and decrease the likelihood of these patients returning home postoperatively. These costs should also be taken into account when evaluating the economics of hip fractures, and all means possible should be used to decrease the risk of complications and subsequent reoperations in hip fracture patients.
Footnotes
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
This research was supported by grants from the EVO Foundations of Kouvola Health Center and the Päijät-Häme Health-Care District.