
Abstract
Background and Aims:
The optimal extent of mesenteric resection in colon cancer surgery remains elusive. The aim was to assess the impact on perioperative morbidity and oncological outcome depending on the height of central vessel ligation in sigmoid resection for adenocarcinomas.
Material and Methods:
All cases of stage I–III sigmoid cancers, operated on with locally radical resections (2007–2009), were identified in the Swedish Colorectal Cancer Registry and categorized according to the position of the vascular ligature, that is, ligation of the inferior mesenteric artery, ligation of the superior rectal artery, or ligation of the sigmoid branches.
Results:
In total, 999 cases were identified and possible to categorize. Although higher ligation level yielded a higher number of lymph nodes, 3- or 5-year overall survival, 5-year disease-free survival, or recurrence rate did not differ between the groups (p = 0.79, p = 0.41, p = 0.67, p = 0.51). No differences in survival were detected after multivariate analysis adjusted for age, sex, T-stage, N-stage, American Society of Anesthesiologists classification, and adjuvant therapy.
Conclusion:
This large population-based study showed increased lymph node yield but no survival benefit or any decreased recurrence rate by high tie in resection of sigmoid cancer.
Introduction
The optimal extent of mesenteric resection in colon cancer surgery to maximize oncologic outcome with minimal complication rate remains elusive. The trend today is toward more extensive resection, reflected in the European and US guidelines (1, 2) and the introduction of complete mesocolic excision (CME) (3–7). The only randomized controlled trial (RCT) in the field, comparing survival after left hemicolectomy and left segmental resection (SR) (8), showed no benefit with central ligation regarding long-term survival but a tendency to increased postoperative morbidity with extended resection. More recent studies have not proven any benefit with central ligation apart from higher lymph node yield (9–11). There is no rationale in performing more radical resections if more limited resection is adequate regarding oncological outcomes (12–15).
The aim of this study was to assess the impact on perioperative morbidity, short- and long-term oncological outcomes, depending on the height of vascular ligation in resection with curative intent for sigmoid cancer.
Material and Methods
All cases registered in the Swedish Colorectal Cancer Registry (SCRCR) of adenocarcinoma, located in the sigmoid colon, operated with sigmoid resection or left hemicolectomy, between 1 January 2007 and 31 December 2009, were eligible for inclusion. Data were retrieved on 16 January 2015, corresponding to a mean follow-up time of 5.1 years (range: 5 – 8 years). The coverage, as compared to the Swedish cancer registry where registration is compulsory, was 94%, 98%, and 96%, respectively, for the years 2007–2009. Disease stage is registered and categorized according to the TNM system established by the Union for International Cancer Control (UICC) for tumor (T), lymph node involvement (N), and metastasis (M). Physical status is registered and categorized according to the American Society of Anesthesiologists (ASA) classification system. Date of death is automatically transferred from the Swedish Health and Welfare Statistical Databases on cause of death.
In SCRCR, the surgeon responsible for the resection is requested to indicate the position of the ligation of the mesenteric vessels (Fig. 1). The cases were divided into three groups based on the position of the vascular ligation as stated by the surgeon: high-tie (HT) ligation of the inferior mesenteric artery, low-tie (LT) ligation of the superior rectal artery defined by the branching of the left colic artery, and ligation of the sigmoid vessels (SR) (Fig. 1). Cases not possible to categorize according to these three defined groups, such as no vascular ligation stated or illogical combinations, were excluded. Emergency procedures imply strong influence on short- and long-term outcomes and choice of operative strategy and were therefore excluded. Stage-IV cases and locally non-radically resected cases were also excluded. Hence, the study population consists of elective, potentially curative resected cases only, to minimize other causes of disease and procedure-related influence on recurrence and long-term survival.
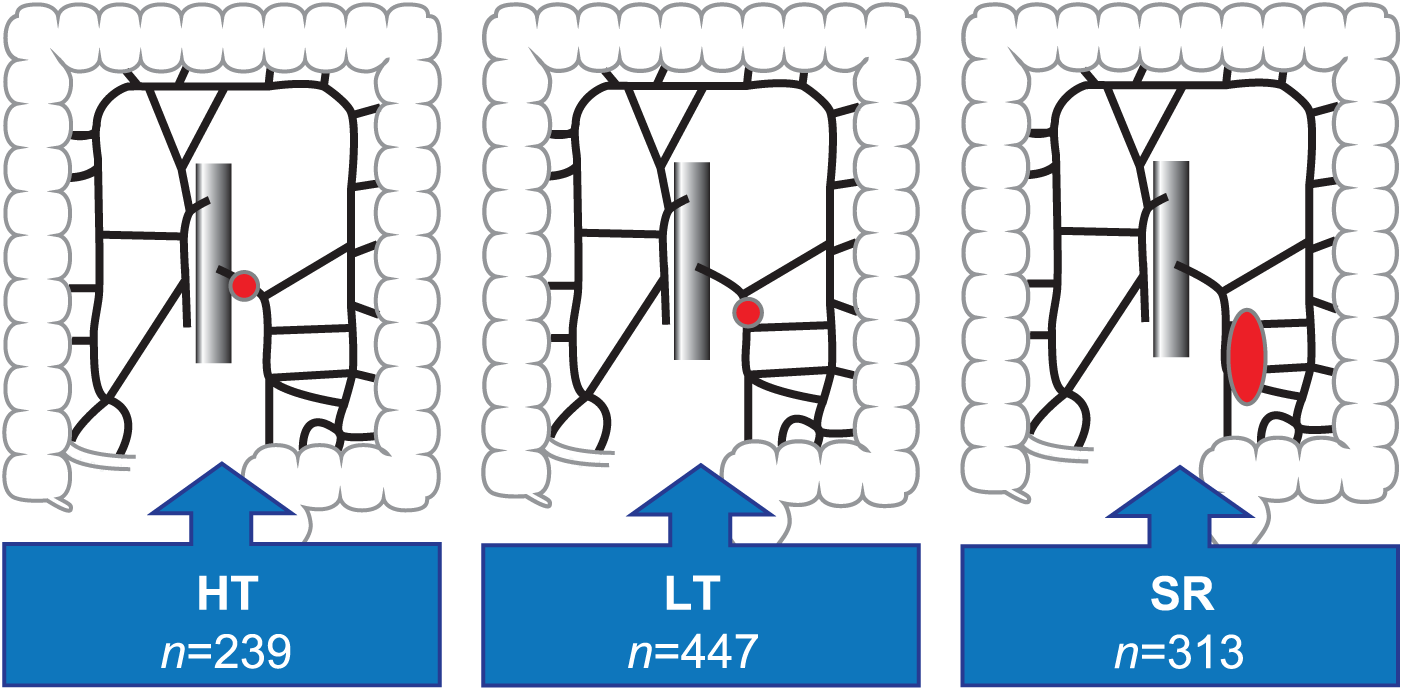
Illustration from the Swedish Colorectal Cancer Registry in which the surgeon responsible for the resection marks the position of the vascular ligature. The circles mark the position of vascular ligations in the study groups, based on this registration.
Relevant risk factors, that is, age, sex, T-stage, N-stage, ASA classification, and adjuvant treatment were assessed in multivariate analyses. A power calculation, performed to assess possible type-II error, showed that a difference in 5-year overall survival down to 5% would be possible to verify statistically with p < 0.05.
This study was approved by the Regional Ethical Committee at Lund University, Lund, Sweden (2010/296).
Statistics
All statistical calculations were performed in the IBM® SPSS® Statistics 22.0 (IBM Corporation, Somers, NY). Kruskal–Wallis test was used for group comparisons, and Cox regression was performed for multivariate analysis. The independent influence of each variable on mortality was expressed as a hazard ratio with 95% confidence interval. All p-values are two-tailed and values less than 0.05 was considered statistically significant. Data are presented as mean values and standard deviation when appropriate.
Results
Out of 1938 cases of adenocarcinoma in the sigmoid colon, 1515 cases (78.2%) were possible to categorize according to the placement of the vascular ligation in the three predefined groups (Fig. 1). No difference in the distribution of age, gender, ASA score, adjuvant treatment, TNM stage, survival, or recurrence was noted between the 1515 cases possible to categorize and the 423 cases not possible to categorize (data not shown). Elective operation was performed in 1312 cases of which 1078 were stage I, II, or III. Locally radical resection (R0) was performed in 92.7% of these cases which corresponds to a total of 999 cases that constitute the study population.
Characteristics of the study population are presented in Table 1. Mean age of the study population was 70.4 ± 11.2 years and 56.9% of the cases were males. The total amount of laparoscopic procedures was 8.8% (n = 88). Laparoscopic operation was performed in 8.8% for HT, 13.2% for SRL, and 2.6% for SR; p = 0.001.
Demographics of the study population.
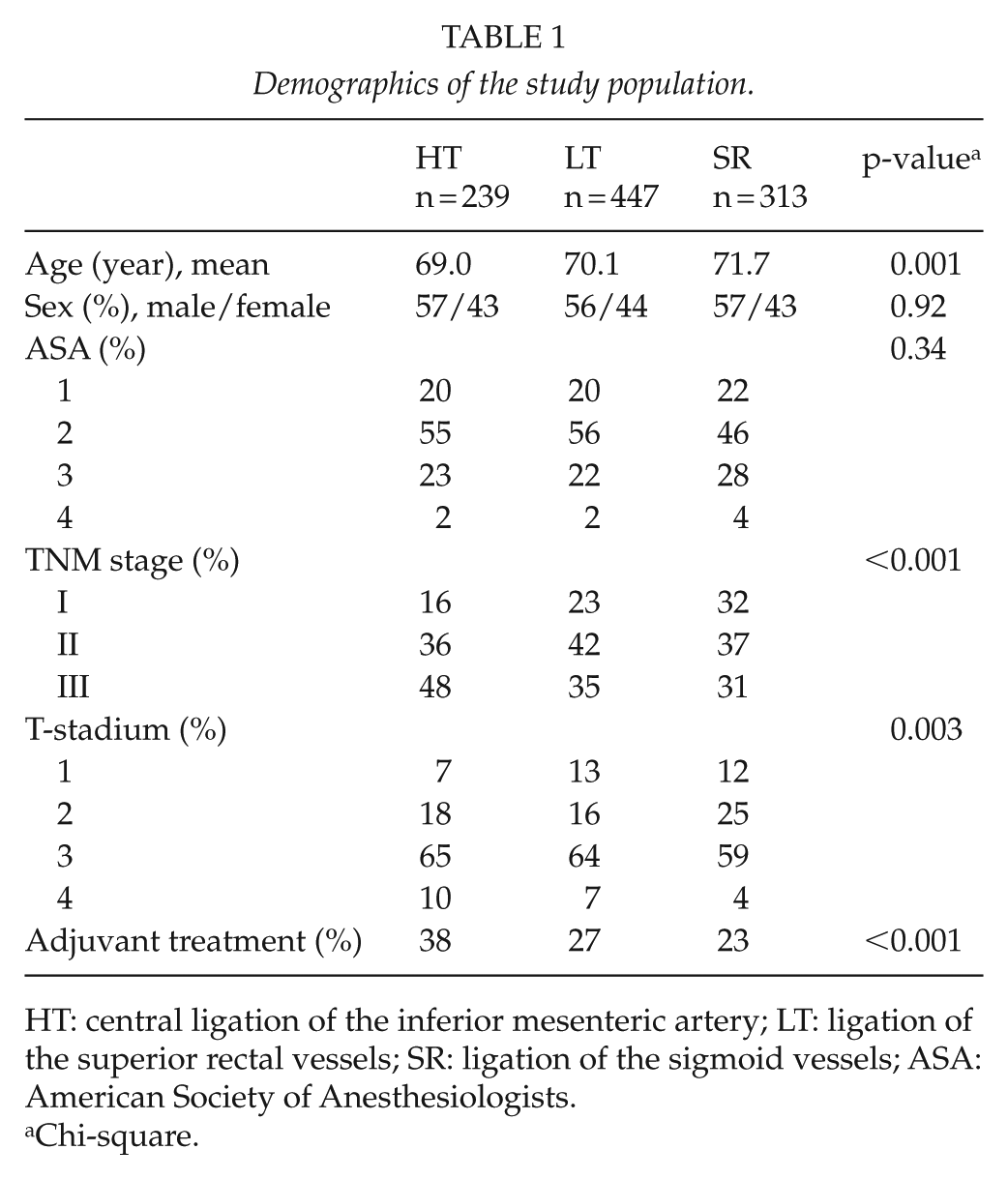
HT: central ligation of the inferior mesenteric artery; LT: ligation of the superior rectal vessels; SR: ligation of the sigmoid vessels; ASA: American Society of Anesthesiologists.
Chi-square.
Short-Term Outcomes
No difference was found between the groups in terms of 30-day postoperative mortality: HT, 2.5%; LT, 0.9%; and SR, 1.0%; p = 0.17. No difference in the number of complications, surgical or medical, was noted between the groups. A moderate increase in perioperative bleeding was noted with more extensive resection: HT, 307 mL (SEM: ±25); LT, 285 mL (SEM: ±15); and SR, 243 mL (SEM: ±25); p = 0.001. Excessive bleeding, defined as the upper quartile (>300 mL), was more common in more radical resection: HT, 27%; LT, 28%; and SR, 18%; p < 0.01. Prolonged operation time was also noted with 198 (SD: ±89), 189 (SD: ±71), and 148 (SD: ±64) min in HT, LT, and SR, respectively; p = 0.001. A higher rate of excessive operation time, defined as the upper quartile (>3.5 h), was noted in HT and LT compared to the SR group; p < 0.001.
Both the number of examined lymph nodes and the rate of positive lymph nodes were higher with HT. In total, 12 lymph nodes or more were analyzed in 69.1% of the cases (Table 2).
Oncological results depending on ligature height in elective sigmoid resections for adenocarcinoma stage I–III.
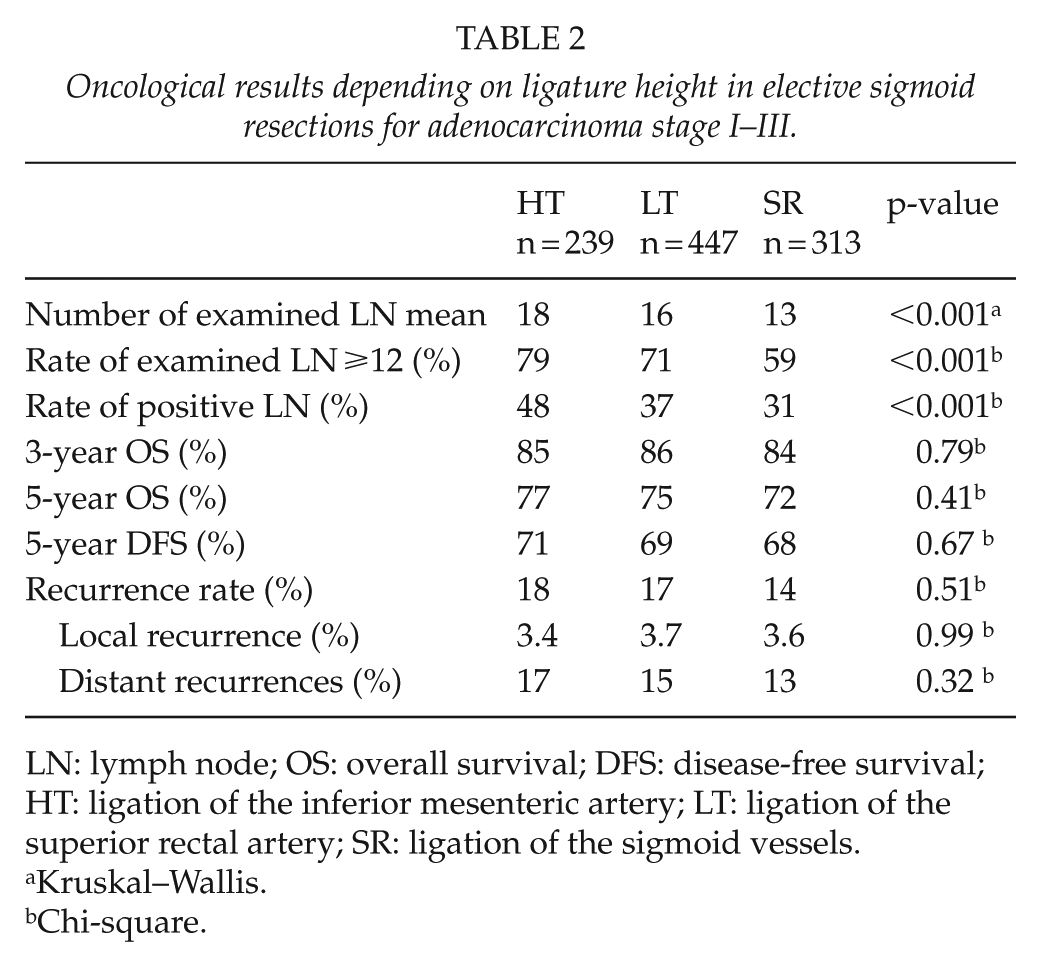
LN: lymph node; OS: overall survival; DFS: disease-free survival; HT: ligation of the inferior mesenteric artery; LT: ligation of the superior rectal artery; SR: ligation of the sigmoid vessels.
Kruskal–Wallis.
Chi-square.
Long-Term Outcomes
Overall survival of 3 and 5 years did not differ significantly between the groups. Neither 5-year disease-free survival nor recurrence rate differed between the groups (Table 2 and Fig. 2). Notably, no difference in local recurrence was found. In addition, no difference in long-term outcome was shown when comparing SR against the more conventional resection types, HT and LT, grouped together.
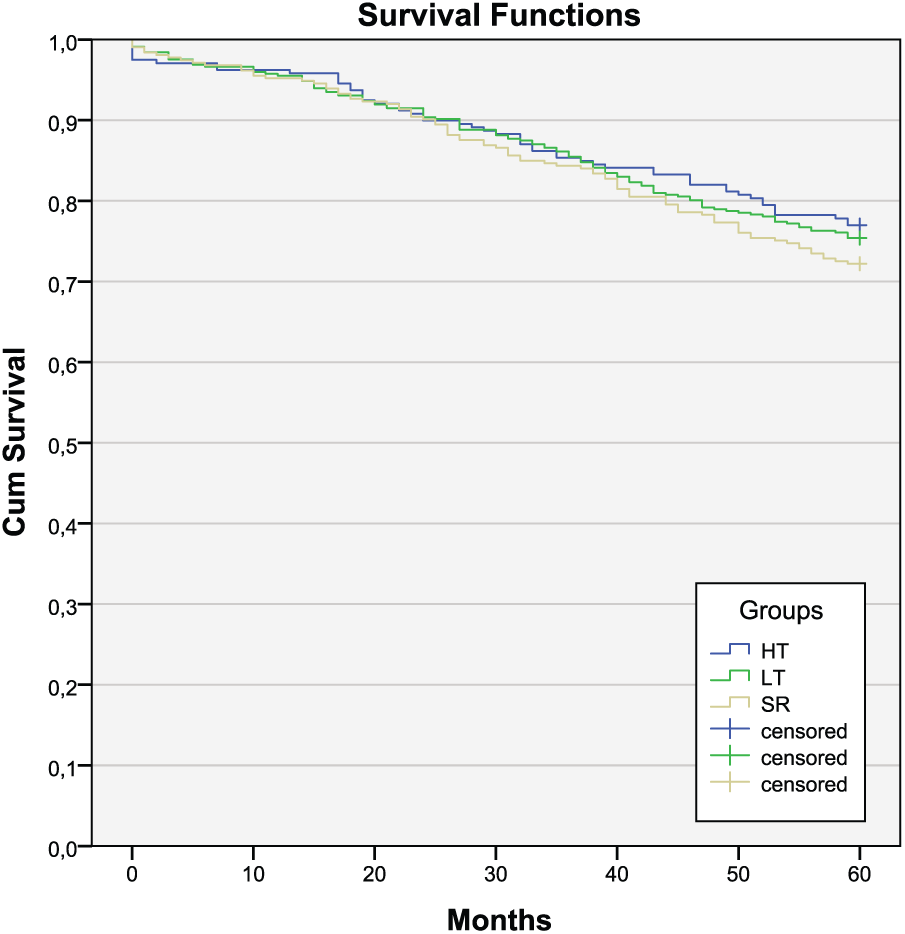
Kaplan–Meier curves depicting survival stratified on placement of central vascular ligature.
Multivariate analysis adjusted for age, sex, ASA classification, T-stage, N-stage, and adjuvant treatment did not show any differences in survival between the groups (Table 3). A subgroup analysis was performed in stage-III disease with an equivalent multivariate analysis adjusted for age, sex, ASA classification, and adjuvant treatment without revealing any significant differences between the groups (data not shown).
Cox regression, hazard ratio for 5-year overall mortality in elective sigmoid resections for adenocarcinoma stage I–III.
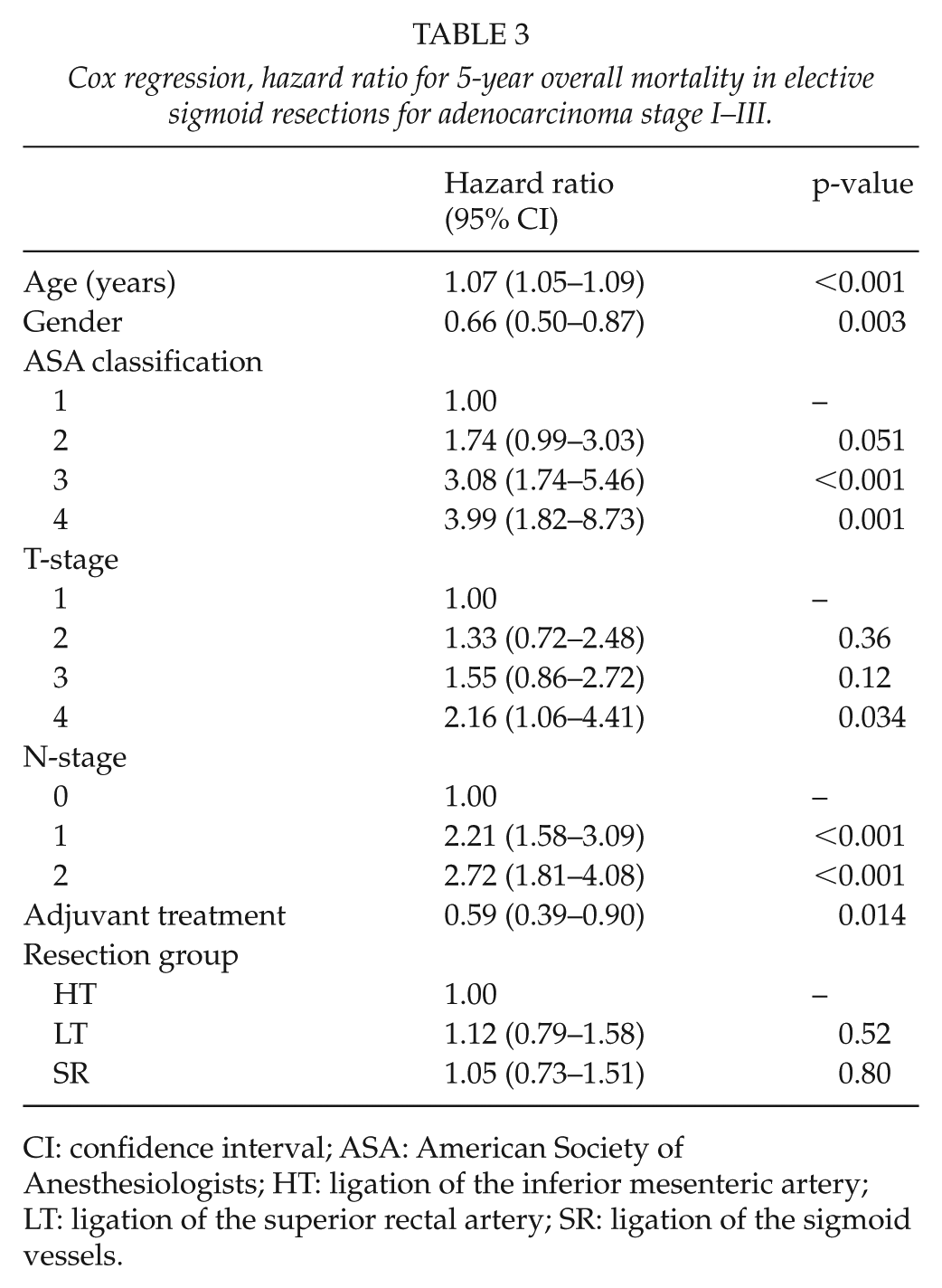
CI: confidence interval; ASA: American Society of Anesthesiologists; HT: ligation of the inferior mesenteric artery; LT: ligation of the superior rectal artery; SR: ligation of the sigmoid vessels.
Discussion
In this study on elective resection for sigmoid cancer, no survival benefit of more extensive excision of the regional lymphatic drainage could be noted, although a higher lymph node yield was noted. Even in stage-III disease, where the effect of more radical resection theoretically should be more pronounced, no discernible difference was observed.
Randomized trials have proven very difficult to perform in this field and so far only one has been published (8). It is cumbersome to perform large RCTs, and the results from RCTs have often been difficult to reproduce in a common population, probably due to selection bias in the recruitment process (16, 17). Hence, RCTs need to be followed by population-based studies to get the full picture. Registry-based population studies have the advantage that data are collected prospectively, although analyzed retrospectively, and give large study cohorts, reducing the risk of type-II errors (17). The SCRCR had a coverage of 94%–98% during the study period, which indicates a true population study (19). No difference was noted between the 1515 cases possible to categorize and the 423 cases not possible to categorize, regarding demography, survival, or recurrences. This minimizes the risk of selection bias and makes the results of this study more generally applicable. The sigmoid colon is, due to the vascular anatomy, suitable for studying the height of vascular ligation. The categorization in this study was based on ligature placement according to different vessels and unclear or illogical cases were excluded. Thus, we believe the model to be quite robust and the group categorization reliable.
The median age of our study population was 70.2 years which is higher than most recent studies on elective colon cancer surgery. The difference in age between HT and LT was 68.6 and 70.1 years (p = 0.042) possibly reflecting a more radical surgical approach in younger patients. The number of examined lymph nodes is comparable to most recent studies. As in other studies, HT produced a higher lymph node yield consequently giving a more solid base for correct staging (20). A higher rate of node-positive cases together with a higher proportion of ⩾12 examined lymph nodes in the HT group may imply a stage migration bias. If so, this would drive the results in favor of HT, which strengthens the finding that HT does not imply any survival benefit.
Although HT was associated with prolonged operation time and increased bleeding, no increase in 30-day postoperative mortality or number of complications was noted (21, 22). Our results correspond to other recent studies regarding 5-year overall survival in elective surgery, ranging from 67% to 89 % (23–26). The key finding of this study is the relationship between resection type and survival. Our results show a 5% difference in 5-year overall survival (77% versus 72%), though not statistically significant. Despite a large study population, the number of patients with tumor infiltration in apical nodes is low and the lack of statistical significance can of course be due to a type-II error. A subgroup analysis on the node-positive cases did, however, not reveal any significant difference. To assess the possibility of a type-II error, we performed a power calculation based on the size of the study population and 5-year mortality, indicating that a difference in survival of 5% or more was possible to verify statistically with p < 0.05. Furthermore, no difference in survival between the resection groups was noted in the multivariate analysis adjusted for T-stage and N-stage.
Intuitively, one expects that more radical resection would be beneficial, especially in stage-III disease. However, neither our studies nor other recent studies have been able to show any survival benefit (9, 20, 25–27). Kanemitsu et al. (22) claimed increased survival rate but it was an extrapolation that excision of involved apical nodes would cure the patient. Bertelsen et al. (18) reported a superior disease-free survival by CME surgery, but this was a comparison between hospitals and cannot be explained by CME practice alone. Unquestionably, HT gives a higher lymph node yield, but this does not necessarily lead to improved survival (9, 20, 25–27). Tumor spread into the apical mesenteric lymph nodes is associated to a bad prognosis (28), probably due to a concomitant distant spread. Possibly, it is not more radical surgery these patients need but more customized adjuvant chemotherapy. Hence, there is a need to identify prognostic and predictive markers for adjuvant treatment.
In this study, it was only possible to evaluate the height of vessel ligation. Other aspects of surgical technique, such as the plane of mesocolic excision, are not evaluated in routine pathology reports and not possible to analyze in this setting. Since this is not a RCT, the reason for the choice of position of the vascular ligation was not random. A more extensive resection was probably used in cases with macroscopically more advanced disease, indicated by a higher proportion of positive lymph nodes in the HT group. However, stage was adjusted for in the multivariate analysis, still without any differences between the groups. A higher proportion of HT resections were performed by colorectal surgeons. If this is associated with a higher proportion of patients operated on with CME technique is not possible to determine. However, if this would affect the outcome as suggested, it would drive the results in favor of HT, as would any stage migration.
The validity of the data in the registry is a matter of concern. It is not possible to accurately verify the placement of ligatures retrospectively but a recent study validating the position of the vascular ligation deemed the validity acceptable, with sensitivity 80.2% and specificity 90.1% (29). The higher lymph node yield in the HT group in our study supports that a more extensive surgery was indeed performed in this group.
In summary, the limitations of this study are the retrospective analysis (although of prospectively collected data) and the uncertain validity of the data on ligature placement. Moreover, a risk for selection bias cannot be totally ruled out due to the retrospective design. Adjuvant treatment, T-stage, and N-stage were not equally distributed between the groups; however, these variables were adjusted for in the multivariate analysis. Due to the non-randomized study design, there might however be other confounders not adjusted for.
The strength of this study is the population-based, large-sized, homogeneous study cohort of elective sigmoid resections, which enabled adjustments in multivariate analyses with strong power.
Conclusion
This large population-based study showed increased lymph node yield but no survival benefit or any decreased recurrence rate by high tie in resection of sigmoid cancer. These findings indicate a need to identify prognostic and predictive markers to improve adjuvant treatment rather than aiming at more extensive surgical treatment, as routine, in sigmoid cancer.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethical Committee of Lund University, Lund Sweden (2010/296).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by grants from Allmänna sjukhusets i Malmö stiftelse för bekämpande av cancer; Skane Regional Research Funds.