
Abstract
Background and Aims:
Nodal involvement is the most important prognostic factor in colon cancer. Although theoretically appealing, it is not known if wider mesenteric excision improves the oncological result. The aim of this retrospective study was to investigate whether wider mesenteric excision yields a superior oncological result.
Material and Methods:
Depending on the resection length, 333 cases of locally radical right-sided hemicolectomies due to adenocarcinoma were compared for perioperative morbidity and mortality, disease-free survival, and long-term survival.
Results:
Postoperative mortality was significantly higher in the quartile with the longest resections, p = 0.003. In a multivariate analysis adjusted for age, stage, emergency operation, adjuvant chemotherapy, and year of operation, a negative relationship between resection length and 5-year overall survival was noted, p = 0.01. No differences in the causes of death or in the incidence of local or distant recurrences were noted between groups.
Conclusions:
Wider excision in right-sided hemicolectomies was not associated with any oncological benefit but an increased postoperative mortality and a decreased 5-year overall survival. These findings may suggest consideration to perform wide mesenteric resections routinely. Further research is warranted to define which patients benefit from wider resections.
Introduction
Despite advances in oncological treatment and multimodal approach, surgery is still the cornerstone in the treatment of colon cancer and a prerequisite for cure. Nodal involvement is the most important prognostic factor in colon cancer (1) and examination of at least 12 nodes is required for reliable staging (2, 3). Although appealing, it is not known whether a more radical excision of the mesocolon, and thus the locoregional lymphatic drainage, improves the oncological result (4). To our knowledge, there is only one randomized study addressing the issue of central ligation versus noncentral ligation (5). In a multicenter trial, Rouffet et al. (5) randomized left-sided colon cancer to either segmental resection with peripheral ligation of the vascular pedicle or classic left-sided hemicolectomy with central ligation of the inferior mesenteric vessels. No difference was found in long-term survival, but a numerical, although statistically nonsignificant, increase in early postoperative mortality was found in the left-sided hemicolectomy group.
The concept of complete mesocolic excision (CME) has been introduced in recent years and gained increasing acceptance (6–8), although not acknowledged as golden standard (9). One of the aspects in this concept is radical excision of the mesocolon by central ligation of the vessels. CME surgery removes more tissue compared with standard surgery and yields more lymph nodes (10, 11). Results from Erlangen and others, using the CME concept, indicate an increased 5-year survival rate and improved oncological result (7, 12).
The aim of this retrospective study was to test the hypothesis that wider mesenteric excision yields a superior oncological result.
Material and Methods
All patients operated on with right-sided hemicolectomy due to adenocarcinoma, in the cecum, ascending colon or hepatic flexure, between 1987 and 2001 at Malmö University Hospital, Sweden, were identified by the hospital inpatient registry. The medical charts and pathology reports were scrutinized. Patients with synchronous metastasis or nonradical resection were excluded. Thus, only R0 procedures in stage I–III cases were included in the study. The patients were followed 5 years postoperatively or until death.
Information on perioperative morbidity and mortality as well as development of locoregional or distant recurrences was retrieved from the medical charts. Data on tumor stage according to the tumor-node-metastases (TNM) classification, number of examined lymph nodes, resection margins, and length of resected bowel were collected from the pathology reports. Date and cause of death were collected from the Cause of Death Registry at the Swedish National Board of Health and Welfare, wherein both the main cause of death and contributing factors of deaths are registered.
No valid information on ligation sites could be collected from the medical charts. Thus, we used length of resected bowel as an indirect measure of mesenteric excision assuming that a more central ligation of the mesenteric vessels as well as excision of adjacent vascular branches generate wider excision of bowel, which has also been used by other authors (13, 14). The resection length was measured by the pathologist on formalin fixed specimens. A histogram of resected bowel length showed a unimodal distribution. The study group was divided into four groups by quartiles of total length of bowel resection (ileum and colon) for comparisons.
The causes of death were grouped as follows: colon cancer as sole diagnosis, metastatic colon cancer, any cancer, cardiovascular, infectious disease, and other causes.
Kruskal–Wallis test and chi-square test were used for group comparisons and Cox’s analysis was performed for multivariate analysis. All statistical calculations were performed in the IBM® SPSS® Statistics 17.0 (IBM Corporation, Somers, NY, USA). Survival is presented as 5-year overall survival. A p-value < 0.05 was considered statistically significant. Data are presented as mean values and standard deviation when appropriate. The study was approved by the Regional Ethical Committee at Lund University, Lund, Sweden.
Results
A total of 645 cases operated on with right-sided hemicolectomy for colon cancer stage I–III during the study period, 1987–2001, were identified via the hospital inpatient registry. Due to incomplete medical charts, 306 cases (47.4%) were excluded, ranging from 78.8% (1987) to 0% (2001). Another five cases were excluded due to nonradical resection, and one case was excluded due to concomitant major surgery. The remaining 333 cases were included in the study.
The mean age was 74.9 ± 9.9 years: 201 women, 132 men. In all, 262 cases (78.5%) were elective and 67 cases (21.5%) were emergencies; 4 cases were not possible to be classified. Overall, 171 tumors (51.5%) were located in the cecum, 131 (39.5%) in the ascending colon, and 30 (9.0%) in the hepatic flexure (one with missing data). In all, 33 (9.9%) of the cases were stage I, 170 (51%) stage II, and 130 (39.0%) stage III (Table 1). The study group was divided into four groups by quartiles of total length of bowel resection (Q1–Q4). Adjuvant chemotherapy was given to 7.5% of the patients, without any differences between the study groups (Table 1). No difference in the number of examined mesenteric lymph nodes was noted between the quartile groups. Furthermore, no difference in the incidence of lymph node metastasis was shown, and hence no difference in stage distribution (Table 1).
Demography of the material, divided into quartiles of total length of bowel resection.
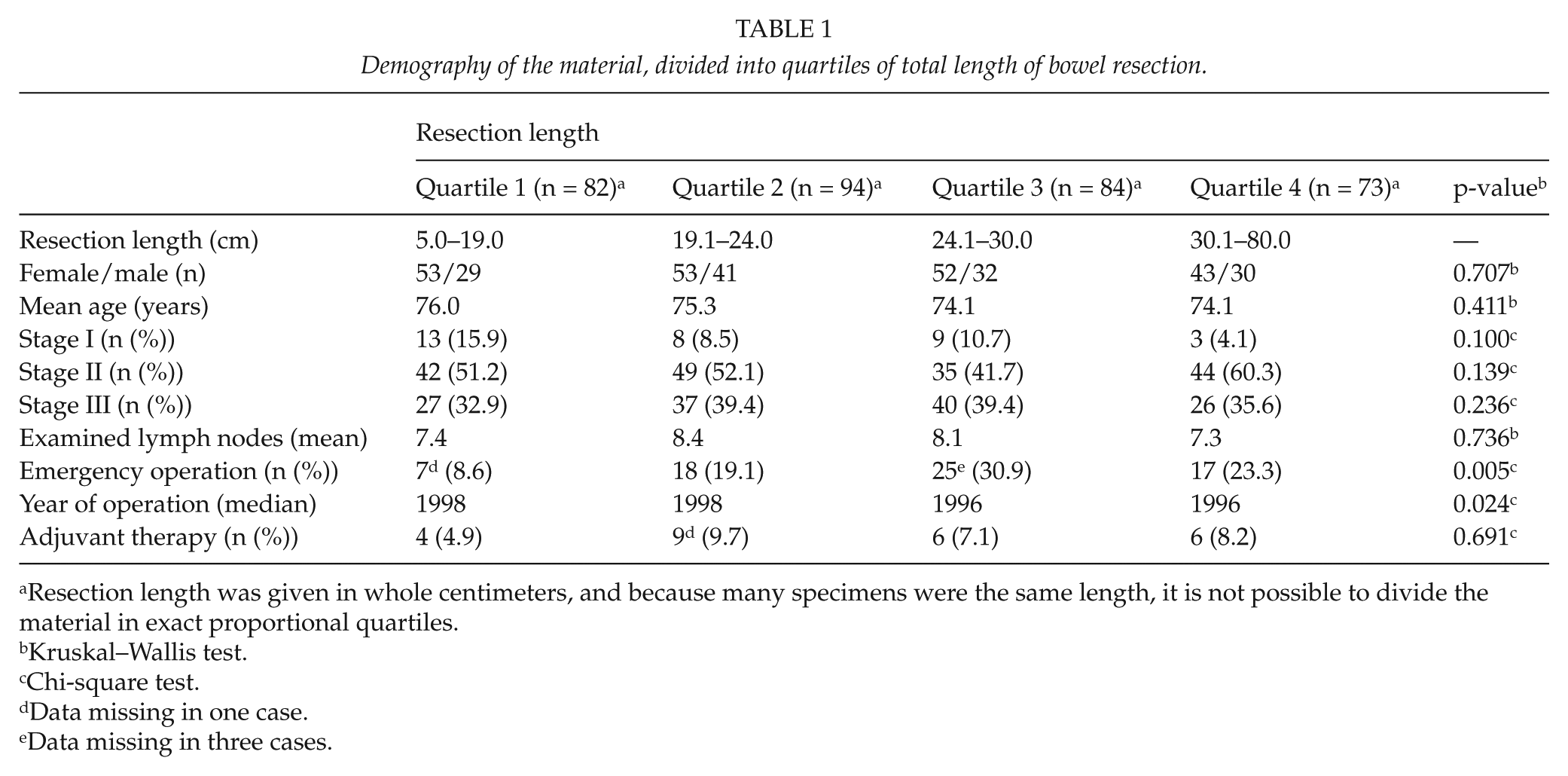
Resection length was given in whole centimeters, and because many specimens were the same length, it is not possible to divide the material in exact proportional quartiles.
Kruskal–Wallis test.
Chi-square test.
Data missing in one case.
Data missing in three cases.
In all, 10 patients died within 30 days postoperatively, corresponding to a 30-day postoperative mortality of 3.0%. The postoperative mortality was significantly higher in the Q4 group, 6 out of 73 patients (8.2%), compared to the Q1–Q3 group, 4 out of 260 patients (1.5%), p = 0.003. Causes of postoperative death were the following: heart related (3), kidney failure (2), obstruction (2), sepsis (1), pulmonary embolism (1), and ruptured aortic aneurysm (1), without any apparent difference between the groups. Of the 333 patients, 277 were alive after 1 year (83.2%) and 174 after 5 years of follow-up, corresponding to an overall 5-year survival of 52.3%. A Cox’s analysis was performed after adjusting for factors known to affect long-term survival, that is, tumor stage, age, emergency operation, year of operation, and adjuvant chemotherapy. Comparison of Q1–Q3 with Q4 showed a negative relationship between resection length and overall survival over time, p = 0.01 (Fig. 1). These figures include the 30-day postoperative mortality of 3.0%. In addition, after exclusion of the 30-day postoperative mortality (n = 323), a consistent negative relationship was noted between resection length and 5-year survival, p = 0.049.
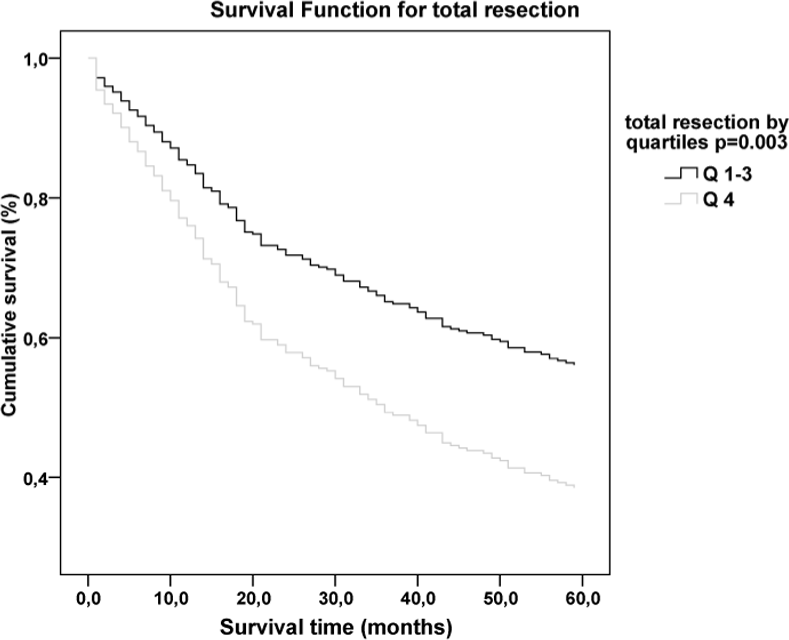
Relationship between resection length and overall survival over time.
After 5 years, 143 of the 260 patients in Q1–Q3 were still alive, compared to 31 of the 73 patients in Q4, corresponding to a cumulative survival of 55% compared to 42.5%, p = 0.058. Although less pronounced, an impaired survival was noted also in group Q3 (compared to Q1), p = 0.048 (Fig. 2). The impairment in survival was most pronounced in stage III disease, with a 50% decrease in the Q4 group compared to Q1–Q3, p = 0.047 (Table 2).
Source: Olofsson et al.
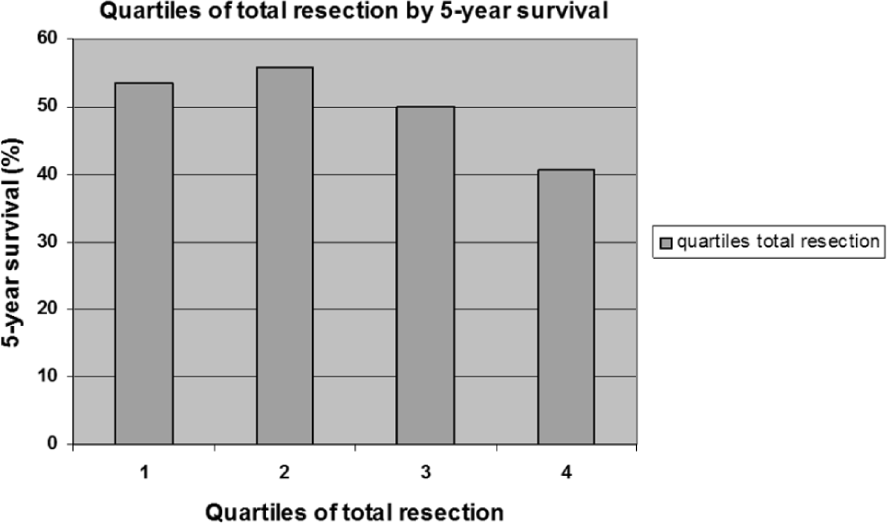
Relationship between quartiles of total resection length and 5-year survival.
Five-year overall survival stage by stage, depending on bowel resection length.
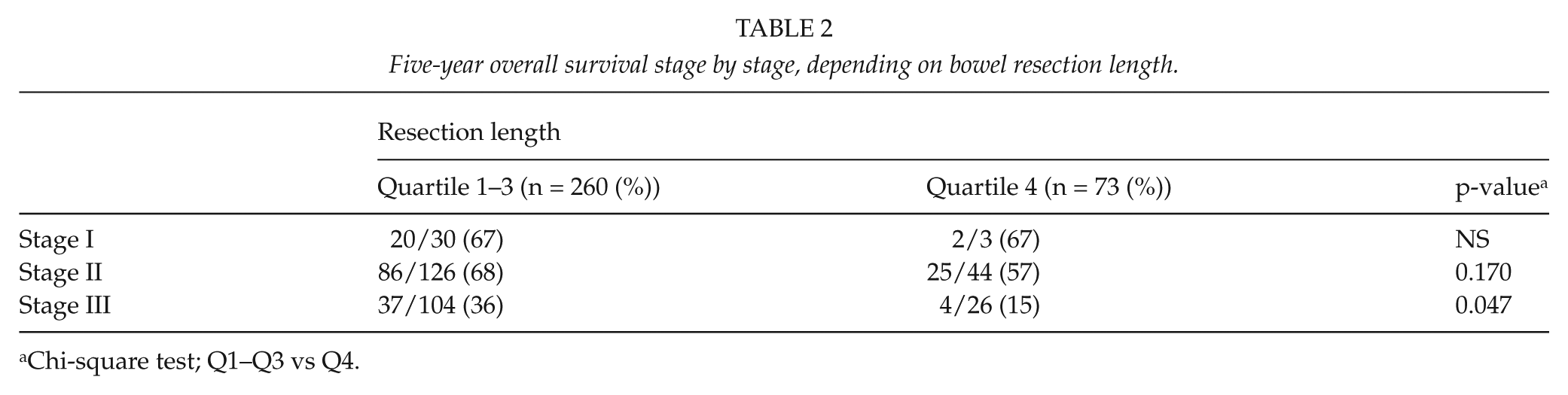
Chi-square test; Q1–Q3 vs Q4.
The cause of death was analyzed in the 211 patients who had died during follow-up, with a mean follow-up of 61.4 months. No difference in the cause of death was noted between the four quartiles (Table 3). Thus, no difference in cancer-specific mortality was noted. Furthermore, no difference in the incidence of recurrences, neither locally nor metastatic, was noted.
Cause of death in the 211 diseased, divided into quartiles of total resection length. Mean follow-up was 61.4 months. Several causes of death may have been registered for one individual patient.
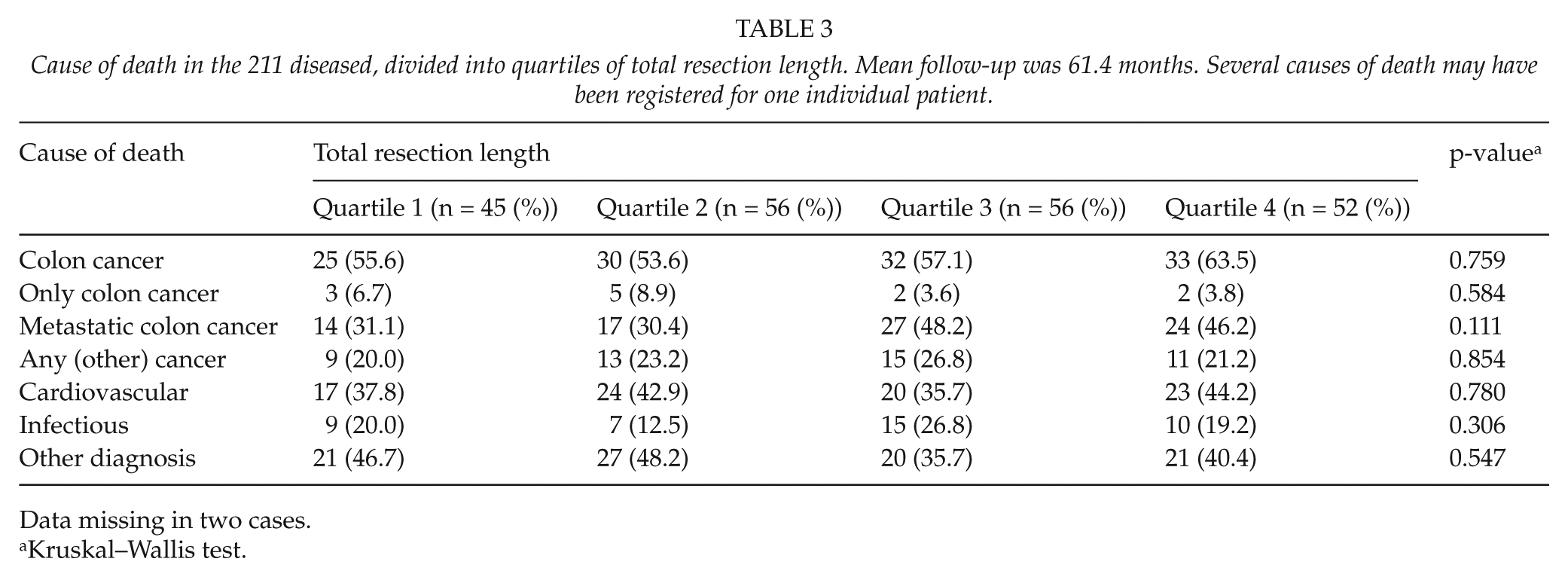
Data missing in two cases.
Kruskal–Wallis test.
Discussion
Despite little evidence, many guidelines and authors advocate a radical excision of the mesenteric lymphatic drainage in colon cancer (3, 5, 6, 9, 12). In this explorative study, we found that wider excision of the bowel in right-sided hemicolectomy was associated with an increased postoperative mortality and an impaired long-term survival. Furthermore, no decrease in local or distant recurrences and no increase in disease-free survival were noted in the group with wider excisions, adjusted for stage and other risk factors. Our results question routine use of wide right-sided hemicolectomy due to insignificant oncological benefit and increased mortality.
This study has a few shortcomings. First, resection length has no validated correlation to central vascular ligation, although there are some data to support this assumption (14, 15), and it has been used as a surrogate parameter for central ligation by other authors (13). The division of the material in quartiles cannot be interpreted as performing CME or not, it rather indicates the extension of mesenteric excision. Besides the level of the central ligature, other factors such as tumor location (16, 17), tumor stage (18), and presence of obstruction influence resection size. However, no differences in tumor stage and anatomical distribution of the tumors were noted between the groups, pointing that the surgeons’ preference was the main determinate for resection length. Irrespective of whether or not a wider resection correlates to the height of ligation, the results point out an association between wide excision and increased postoperative mortality as well as impaired long-term survival. Second, this study is a retrospective study and not a randomized trial. Therefore, we do not know the reasons for making or not making an extensive resection. However, all operations were performed by the same surgeons over a rather long time period in a well-defined population. No shift in surgical strategy was introduced during the period, and the operations were all performed before the CME concept was launched. Furthermore, the calculations were adjusted for age, stage, emergency operation, adjuvant chemotherapy, and year of operation. These circumstances give support for the results demonstrated, although no firm conclusions can be made due to the retrospective design.
The reduced long-term survival seen in this study may seem contradictory to the results published by the Erlangen group (6, 7, 12). However, central vascular ligation is only part of the CME concept. The dissection along the embryological plane of the mesentery fascia, leaving it intact as in total mesorectal excision (TME) surgery for rectal cancer, may be the most important aspect. Additionally, Erlangen is a center of excellence and the case mix differs. In the present study, the material is a defined cohort with significantly higher mean age (75 years compared to 65 years) and contains emergency cases and only some odd referrals. Although central ligation yields a larger number of examined lymph nodes (11, 16, 19, 20), it has failed to prove increased survival (16, 20). Furthermore, lateral spread more than 7–10 cm is an unusual finding (18, 21), and wide excision may not to be warranted routinely for clearance of lateral nodes (16).
A higher number of evaluated mesenteric lymph nodes is an independent factor for improved prognosis (22, 23). The low number of examined lymph nodes in the present study reflects a past era in pathology and might explain why there was no difference in the number of examined nodes in the different groups of resection length. The suboptimal pathology, especially in the earlier period, with a mean of only 7.9 examined lymph nodes has probably lead to underestimation of stage III disease and contributed to an unexpected low survival rate in this study. No differences in stage or number of examined lymph nodes were shown between the groups of different resection length, and the multivariate analysis was adjusted for year of operation and other well-defined prognostic factors including stage, age, and emergency operation. Subsequently, suboptimal pathology most likely did not influence the survival differences between the groups noted in our study.
No specific cause of the impaired long-term survival could be pointed out. We speculate that the larger surgical trauma imposes more strain on these elderly patients than previously assumed, leading to a more pronounced and prolonged deterioration of their general condition. A correlation between wider resection and length of operation was noted, indicating a larger surgical trauma in the Q4 group. Other mechanisms are likely to affect survival as well. However, more extensive bowel resection did not lead to any gut-failure, malnutrition, or renal failure due to enhanced fluid losses. Furthermore, no increased mortality due to infectious diseases, indicating deterioration of the immunological system, was noted.
In conclusion, wide excision in right-sided hemicolectomies was not associated with any oncological benefit but an increased postoperative mortality and a decreased long-term survival. The findings of this explorative study call for consideration about performing extensive mesenteric resections routinely and warrant further research to define subgroups who benefit from more extensive mesenteric resections and risk groups in which it should be avoided.