
Abstract
Objectives:
Quality of surgery has recently become an essential topic in the prognosis of colon cancer. Complete mesocolic excision for colon cancer has recently gained popularity with high-quality surgery. Patient specimens after complete mesocolic excision with central vessel ligation procedures have an integrity of the mesocolon and the yield of three fields of lymph node harvest. We apply the glacial acid, absolute ethanol, water, and formaldehyde solution to each specimen based on the Japanese classification of lymph node groups and station numbers. We aim to identify the distribution and status of lymph node metastasis according to each tumor site and some pathological characteristics related to this disease.
Methods:
A prospective cohort study was performed on 45 laparoscopic complete mesocolic excision surgery patients.
Results:
2791 lymph nodes were harvested after complete mesocolic excision surgery. The average number was 62.0 ± 22.3 nodes. The mean tumor size (in the largest dimension) was 4.2 ± 1.8 cm. The average length of the resected bowel segments was 29.1 ± 7.7 cm. There are 63 (2.3%) node metastases in 2791 lymph nodes, in which 17/45 (37.8%) patients had pN(+). The minimum positive node size was 1 mm. The positive pericolic lymph nodes (station 1) accounted for the highest rate, with 53 nodes (1.9%). The number of lymph nodes in young age ⩽60 is more significant than in older. The results were similar, with a more significant node retrieval in the group with a tumor size >4.5 cm and specimen length >25 cm. The number of lymph nodes in lower tumor invasive (pT1,3) was smaller than pT4. Our research shows that the cecum, ascending, and descending colon had greater nodes than others, with a mean number of 78.6, 74.2, and 71.3, respectively.
Conclusions:
The metastasis and harvested lymph nodes accounted for the highest rate of colon cancer in station 1 and the lowest rate in station 3. The number of retrieved lymph nodes was significantly associated with tumor location, size, specimen length, and patient age.
Introduction
Quality of surgery has recently become an essential topic in the prognosis of colon cancer (CC). 1 Complete mesocolic excision (CME) for CC has recently gained popularity with high-quality surgery. 2 This technique has become increasingly popular in recent years after evidence of increased disease-free survival (DFS) after CME in 2009. 3 Bertelsen et al. 4 report the 5-year outcomes with a significant reduction in recurrence to 9.7% in patients of the CME group versus 17.9% for those undergoing non-CME surgery in Union for International Cancer Control (UICC) 5th stage I–III for right-sided CC. And the mean nodal yield of the CME group was more than that of the control group (38 versus 21 nodes). The medical evidence on increased free disease survival after CME is mainly based on the results of some prominent authors such as Hohenberger, Bokey, and Bertelsen et al.3,5
En bloc resection of the colon and the mesocolon allows for precise CC staging and improves prognosis. 6 Patient specimens after CME with central vessel ligation (CVL) procedures have an integrity of the mesocolon and the yield of three fields of lymph node (LN) harvest.3,7 Especially, the extended longitudinal resection after CME with CVL significantly increased the lymph node yield (LNY). 8 Pathologic staging is the primary determinant of treatment and prognosis for patients with colorectal cancer, and LN status plays a significant role in the staging classification.9–12 International guidelines currently accept the concept that a minimum of 12 LNs is a quality measure. 12 However, the evidence is weak, and the debates are certainly still open on whether considering a limit of 12 nodes improves staging accuracy and prognosis. Despite this, more than one-quarter of patients are still incompletely resected by this standard. 13 The understanding of the lymphatic spread of CC is inconsistent. Hohenberger describes the spread as located in the pericolic LNs, but no more than 8 cm from the primary, and that it enters the LNs of central supply arteries, 3 while the range of regional LNs is divided according to feeding arteries about 10 cm from the tumor margin of the Japanese Society for Cancer of the Colon and Rectum (JSCCR). 14
The presence of metastatic LNs in the main group categorized as N3 using JSCCR classification was also not mentioned in the American Joint Committee on Cancer (AJCC) 8th and UICC 5th editions. And LN metastasis outside the regional LNs is classified as distant metastasis (M1) presenting in the JSCCR system but not in the AJCC and UICC classifications.14,15 CME colectomy has a more extended resected segment of the colon than traditional surgery and the complete mesentery with it, including regional LNs and those beyond regional LNs that belong to the tumor. We have, therefore, conducted a prospective analysis of our specimens to identify the distribution and status of LN metastasis according to each tumor site based on the Japanese classification of LN groups and station numbers. The assessment of LN metastasis in the main group is significant for CME with CVL procedure.
Methods
Patient cohort
A prospective cohort study was performed on patients undergoing laparoscopic CME surgery at the Digestive Surgery Departments between May 2021 and October 2022. This study was approved by the Institutional Review Board of our University (IRB Reference Number: H2021/443). Every patient gave written informed consent to take part in the study. Our cohort consisted of 45 patients, including 20 (46.7%) females and 25 (53.3%) males (ratio 1:1.2). Mean age was 60.9 years (median 60.9, range 28–88).
The database included patients with AJCC 8th stage I–III CC. Exclusion criteria were the presence of distant metastasis, multiprimary cancer in different locations, familial adenomatous polyposis or hereditary nonpolyposis, palliative resection, or an emergency operation.
These patients underwent laparoscopic colectomy with the CME and central vascular ligation principle at the feeding blood vessel branches that directly the tumor according to the Japanese Society of Colorectal Cancer guidelines for classification and treatment and Hohenberger’s principles of CME surgery.3,14,16 Fifty-one patients were included in this study, but three cases were converted to open surgery due to a large tumor, one case was peritoneal metastasis detected during surgery, one case did not perform CME technique with CVL, and one case changed the histopathological result after surgery.
The morphologic evaluation of the dissection plane in a surgical specimen is categorized based on the state of the dissection surface in the following ways 6 :
- Mesenteric plane: good-quality surgery, mesenteric surface intact, and smooth.
- Intramesocolic plane: the surgery is of moderate quality, with disruption not reaching the muscular layer in the mesocolon.
- Muscularis propria plane: poor-quality surgery exposing the muscularis propria.
Tumor histology: tumor grade was described as low grade: well differentiated, moderate grade: moderately differentiated, and high grade: poorly differentiated.
Database demographics and clinical data, such as the relationship between the number of LNs and age, sex, The American Society of Anesthesiologists (ASA) scoring system, 17 a nutrition risk score (NRS) based on quantitative subjective global assessment (Q-SGA), 18 tumor location, carcinoembryonic antigen (CEA), tumor size was calculated by the largest diameter of the tumor (cm), specimen length (cm), and AJCC 8th staging of patients, tumor histology were shown in Tables 1 and 2.
Associations of the number of retrieved lymph nodes with different clinicopathological parameters.
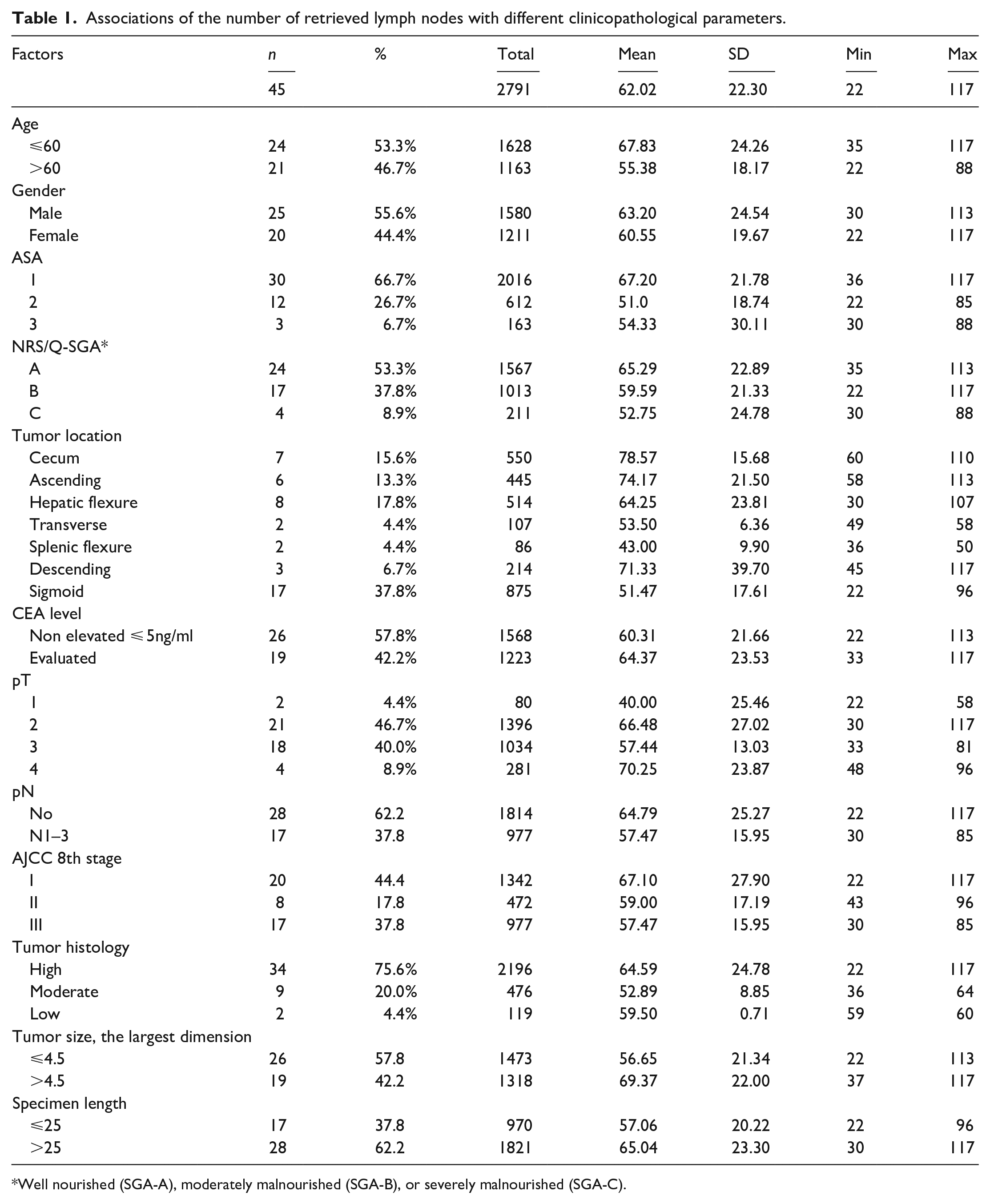
Well nourished (SGA-A), moderately malnourished (SGA-B), or severely malnourished (SGA-C).
Factors affecting the number of retrieved lymph nodes.

Negative binomial with log link.
p < 0.05.
The study’s primary outcome was to evaluate different clinicopathological factors determining the number and distribution of LNs and the rate of LN metastasis by tumor location and LN groups.
This study has been reported in line with the STROBE criteria. 19
Pathological examination
After taking the specimen from the patient, the surgeon team quickly analyzed and measured parameters such as the integrity of the mesentery and some macroscopic results on the specimen. The length of the large bowel, the length of the ileum for the right side, the distance from the tumor to the high vessel tie, the closest bowel wall to the high vascular tie, and other parameters were measured on each patient’s colon specimen using morphometric quantitation. This specimen opened along the colon and measured tumor size in three dimensions. Then, this was resected one-fourth of the tumor at the suspected site of maximal invasion, usually at the thickest site in the middle of the tumor or the site of serosa or internal retraction. This part of the tumor was fixed in a 10% formalin solution. The remaining part was intact, with the colon mesentery fixed in a GEWF solution (Glacial acid, absolute ethanol, water, and formaldehyde) within 6–12 h. All mesenteric specimens after fixation were carefully dissected by one surgeon to fully record the LNs by groups with a size ⩾1 mm. We dissected the visceral peritoneum of the mesocolon. Based on the color of the ivory-white LNs, which is different from the surrounding yellow fatty tissue, to identify the LNs. When we take the LNs, we determine their position with the surrounding blood vessels to determine the location of the LNs by groups and station numbers. LN groups were coded according to the Colorectal Cancer Society. 14 For example, group #201 is a pericolic LN belonging to LN station 1 of the ascending ileocecal colon. The GEWF solution whitens the LNs and yellows the mesenteric fat tissue to facilitate the retrieval of these nodes. Each LN group was contained in a numbered tissue cassette to avoid confusion. The tumor was routinely cut by 5 mm around the suspected maximal invasion site to evaluate the tumor depth and morphologic classification of the dissection plane. These LNs are placed into individual cassettes marked with the patient code and station number with a pencil. If the LNs are too large >1 cm, the LNs are split in half but not separated and then placed separately for this large-sized group.
Two gastrointestinal pathologists independently reevaluated the original histopathological slides. We analyze the tumor stage according to the AJCC 8th TNM classification. Histologic type and grading were analyzed according to the WHO guidelines. 20
100-ml GEWF solution includes 85-ml ethanol absolute (CAS No. 64-17-5), 10-ml formaldehyde 37% (CAS No. 50-00-0), and 5-ml acetic acid (CAS No. 64-19-7).
Statistical analysis
A generalized linear model with a negative binomial and log link function was utilized to examine the association between the number of LNs and the predicted variables. The incidence rate ratios and 95% confidence intervals (CIs) were employed to determine the relationship between the predictors and outcome. Statistical significance was identified at a level of p < 0.05. Statistical analysis was performed using SPSS version 20.0.
Results
With 2791 LNs harvested after surgery in 45 patients, the average number was 62.0 ± 22.3 nodes (range: 22–117). The mean tumor size (in the largest dimension) was 4.2 ± 1.8 cm. The average length of the resected bowel segments was 29.1 ± 7.7 cm. 86.7% of patients had the mesocolic plane, and 13.3% had the intramesocolic plane.
Associations of the number of retrieved LNs and clinicopathological parameters are shown in Table 1. Most patients had an ASA score of 1 with 66.7%, significantly higher than ASA 2 and 3. Most of them were classified as well nourished (SGA-A), with 53.3%. Tumor locations were unevenly distributed in the study, with sigmoid colon tumors accounting for the most at 37.8%, while transverse colon and splenic flexure were only 4.4% each. Pathologically staged after microscopic examination of the resected specimen (pTNM), pT2 and pT3 were 86.7%, and pN0 was 62.2%.
Factors affecting the number of LNs harvested are shown in Table 2. The number of LNs was independent of the CEA level and gender. The number of LNs in young age ⩽60 is more significant than in older. The results were similar, with a more significant node retrieval in the group with a tumor size >4.5 cm and specimen length >25 cm (Figure 1). Amounts of the LNs in pTNM stage II and III were less significant than in stage I. However, the number of LNs in lower tumor invasive (pT1,3) was smaller than pT4 (Figure 2).

Relationship between the tumor sites and the number of lymph nodes.

Relationship between the primary tumor (invasive carcinoma) (pT) and the number of lymph nodes.
There are 63 (2.3%) node metastases in 2791 LNs, in which 17/45 (37.8%) patients had pN(+). The minimum positive node size was 1 mm (Figure 3). Our data showed that positive pericolic LNs (station 1) accounted for the highest rate, with 53 nodes (1.9%). Otherwise, only 8 (0.3%) positives in intermediate LNs (station 2) and 2 (0.07%) positives in main LNs (station 3) according to the JSCCR 14 (Figure 4), (Table 3).

(a and b) The positive lymph nodes with 1 mm in size.
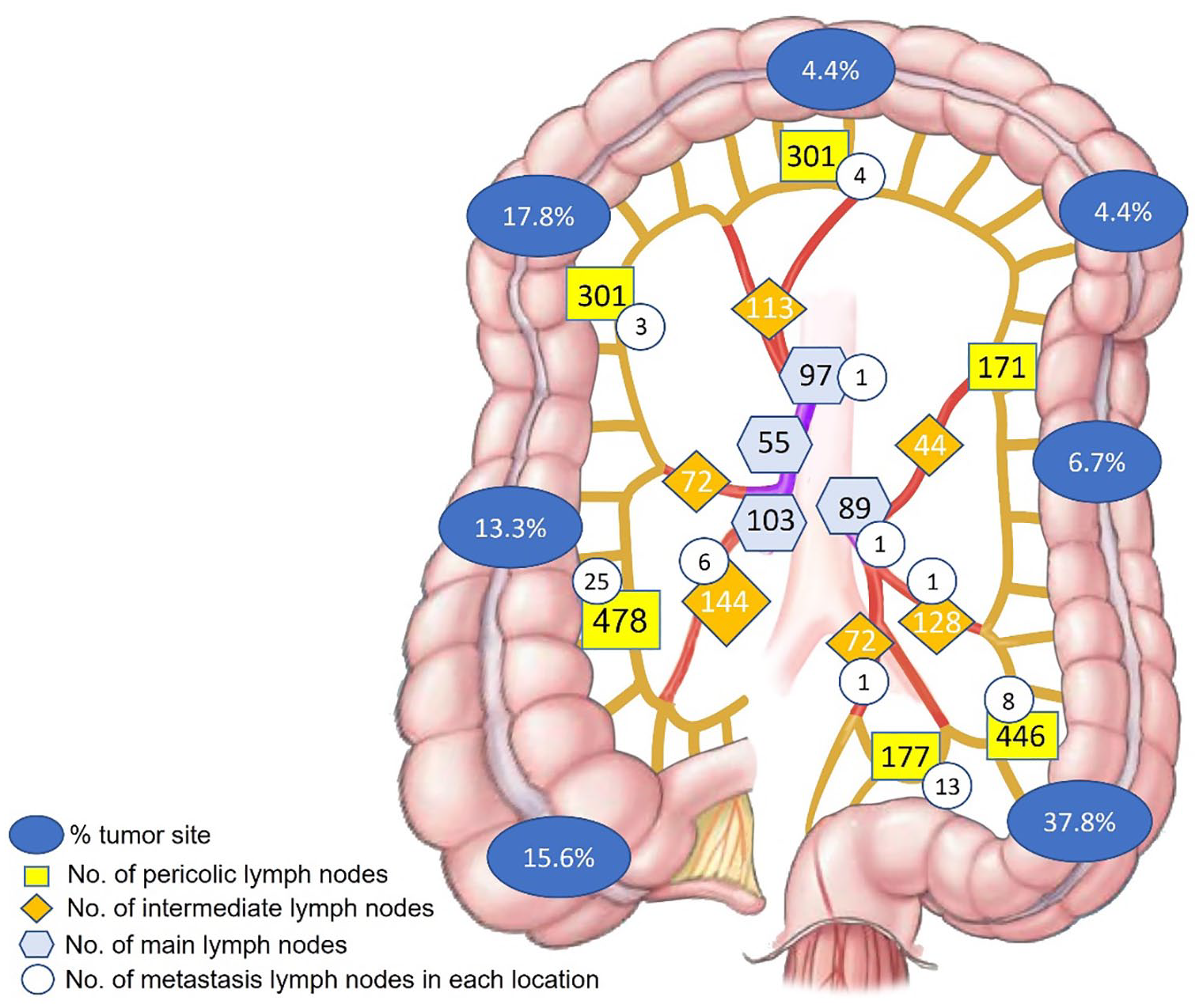
The quantity and distribution of lymph nodes following up the tumor sites and the rate of lymph node metastasis in each regional LN.
Total number of lymph nodes in every station.

No. nodes: number of lymph nodes.
Discussion
CME surgery is increasingly popular because it is associated with better survival and prognosis outcomes.3–5 The results of extended lymphadenectomy in CME colectomy help pathological LN analysis much more efficiently, especially the number of LN retrieval. 21 Our data indicated that using the GEWF solution increases the number of LN harvests, especially in the case of CME. The specimen with CME surgery had an entire regional mesentery submitted to LN examination. It underwent GEWF solution and dissection to find all LNs, whether as small as 1 mm in size. According to Brown et al., 22 83% of additional LNs were under 2 mm because LNs are white, which makes detection easier when GEWF is employed. In extra nodes identified, 75% of all positive nodes were under 2.0 mm in size. Märkl et al. 23 stated that small LNs (less than 1 mm) play almost no role in the proper histopathological LN staging. However, they agreed that the finding of relatively small LNs (1–5 mm) was crucial for precise LN staging and was prognostically significant, with a link between a high LN harvesting rate and a favorable prognosis in CC.
The average number of LNs in our results was 62.0 ± 22.3, similar to Ahmadi et al.’s 24 study, which revealed 61 and 71 median LNs per cadaver in the ascending mesocolon and sigmoid, respectively. The research of Hida et al. 25 showed that the mean number of nodes examined per patient was 76.4 after the clearing method was performed. For adequate CC staging, guidelines advise regional lymphadenectomy with an LNY of at least 12 LNs. 15 Several recent studies have shown that the more LNs are harvested, the better the results. For example, Simões et al. 26 showed that LNY 22 LNs was related to prolonged DFS and overall survival (OS), especially for right-sided CC. 26 Guan et al. 27 revealed that 5-year cancer-specific survival was significantly improved for stage I–III right-sided CC patients with ⩾15 LNs.
Most patients were on ASA score of 1 with 66.7% and well nourished (SGA-A) with 53.3%. The impact of ASA score and NRS evaluated on short- and long-term morbidity and mortality rates of CC patients undergoing curative surgery.28,29 However, a normal healthy (ASA1) and well-nourished patient had significantly higher harvested LN numbers than the other group. Tekkis et al. 30 showed that increasing age and ASA grade significantly reduced the average number of LNs retrieved from the resection specimens. Cancer development is the progression from the primary tumor site or metastasis in cancer through lymphatics. This progression is consistent with developing LNs and systemic metastases from a localized cancer. Ferris believed that the roles of lymphatics, nodal metastasis, and antitumor immunity are related. 31 We have not found a way to explain how the number of LNs and the patient’s physical condition relate to this study’s results. However, patients with good immunity, general health, and nutritional status seem to have more LNs.
The gender and CEA level did not affect the LN retrieval. Although the CEA level is independent of LNs, the 18-node standard could be viewed as an alternative to the 12-node standard supported by the AJCC 8th guidelines to improve long-term survival and accurately determine the nodal stage for patients with CEA-elevated (⩾5 ng/ml) CC. 32 There are few studies on the correlation between the number of LNs and gender. Ichimasa et al. 33 suggest that the attribution of the female is correlated with LN metastasis in pT1 colorectal cancer.
Similar to the study of Shen et al., 34 the number of LN retrieval was significantly associated with the length of resected segments, patient age, and tumor location. 12 The LNs retrieved in older patients were fewer in number. 30 Shen recognized that reactive LNs are enlarged and easier to identify than normal LNs. Hence, Guan et al. 35 recommended that the LN examination for young CC patients be assessed differently, using a 22-node measure that may be more appropriate for CC patients under 40. And the other study suggested that a nine-node measure was available for patients aged ⩾80. 36 On the relationship between the length of the segment and the number of LNs, the length >25 cm had more LNs harvested than the group ⩽25 cm. One of the essential conclusions from Shen’s study was that the length of resected bowel segment was associated with the number of LNs recovered. Regarding tumor location, depending on the type of resection, the number of LNs decreases from the proximal to the distal location.12,30,34,37 Our research shows that the cecum, ascending, and descending colon had greater nodes than others, with a mean number of 78.6, 74.2, and 71.3, respectively.
The number of harvested LNs is associated with higher tumor stage and size. 12 Betge et al. 12 showed that tumor sizes >4.5 cm and higher AJCC stages were significantly associated with LN count. According to our data, more LNs were obtained in the group tumor size >4.5 cm. Our data show that a higher number of LNs harvested were associated with T-classification, but high LN count is unrelated to the tumor stage. In the SEER database searched for pN0 CCs, Ning et al. 38 showed that retrieved LNs were identified as an independent prognostic factor, and at least 18 LNs were associated with favorable prognosis in patients with pN0 CC. And this showed an alternative cut-off value for survival analysis for pN0 classification. Following this database, Cai et al. 39 revealed that a minimum of 19 LNs must be examined for optimal survival and adequate node staging in LN-negative right-sided CC. Individuals with 19 or more LN retrieval had a greater prevalence of LNs metastasis than those with fewer than 19 nodes. Although the number of LN retrieval is not proportional to the tumor stage, it still helps pN classification accurately. Some studies have suggested an association between survival and LN harvest.26,36
Although tumor sites were unevenly distributed in the colon, we plotted a correlation between the harvested LN sites and the metastatic nodes in a total of 2791 nodes. The total metastasis LN rate was 2.3%. However, the number of patients who had pN(+) (positive regional LNs) was 17 (37.8%), which corresponds to the study of Bertelsen et al., 5 with 35% in the CME group. The evaluation of small LNs is also essential. In the study of Schrembs et al., 40 up to 51% of metastatic LNs were 2–6 mm in size. 40 Although the positive LN rate at station 3 was 0.07% of the total LNs, up to 2/45 (4.4%) patients have positive LNs detected at this station. LN metastasis determines the advanced stage of cancer progression and requires adjuvant treatment after surgery. Although the rate of central LN metastasis is low, LNs can metastasize in theory, so all regional LNs should be removed during surgery.
Detection and evaluation of metastatic LNs by manual LN dissection is the standard of many treatment facilities, even major centers in our country. However, a methylene blue solution or fat clearance process can optimize LN retrieval. 23 These LN retrievals showed a significantly higher number of LNs, from an average of 20.8 with manual LN dissection increased to 68.8 LN harvesting when they tested the entire residual mesenteric fat in Brown et al.’s study. 22 More importantly, the pTNM disease stage of the patients was increased. That said, careful examination of mesenteric LNs may be necessary to ensure accurate pN status. The use of solutions after surgery helps to diagnose the stage of the disease more accurately, specifically increasing the patient’s stage after surgery, helping to identify patients who need adjuvant treatment more accurately after surgery. Another study by Hernanz et al. 41 showed that the additional LNs increased to about 10, and 4.4% of LNs revealed tumor metastasis when using a fat clearance solution.
There are many solutions to fix and detect LNs after surgery, for example, acetone, alcohol-xylene, methylene, and GEWF. However, GEWF is safe, cheap, and easy to prepare. 9
However, we need to proceed with more sample sizes and patient follow-ups to assess better the relationship between harvested LNs and OS. Our data are continuously collected, and we will publish the results of surgery, treatment, and 3-year OS time after surgery. Additional studies of solution use after the GEWF solution should be continued at our facility and others, comparing the results of using this solution and not using it, and comparing the results of using this solution and another solution (Carnoy) so that this solution can be used routinely on specimens and can help diagnose the postoperative staging more accurately.
Conclusions
LN harvesting is determined by many factors, such as the extent of lymphadenectomy during surgery, the length of the resected bowel segment, the use of fat clearance solution on the postoperative specimen, and many other factors associated with clinicopathological parameters with LN dissection. Adequate nodal staging is important in the pTNM stage. This process is performed by good-quality colectomy surgery and pathologists to maximize the number of LNs.
The metastasis nodes and harvested LNs accounted for the highest rate in station 1 and the lowest rate in station 3 of CC. The number of retrieved LNs was significantly associated with tumor location, size, specimen length, and patient age.
Footnotes
Acknowledgements
We would like to thank all members of the Digestive Surgery Department and the Pathology Department for their efforts and support.
Author contribution
MT Nguyen, CT Dang, and AV Pham identified the study concept and design. MT Nguyen and AV Pham performed a draft and synthesis of the data. MT Nguyen, DD Le, and AV Pham conducted the statistical analysis. MT Nguyen drafted the manuscript; CT Dang, TBS Nguyen, NC Pham, MD Pham, HT Nguyen, DTD Phan, DVP Nguyen, TP Nguyen, PV Doan, and DS Nguyen revised it. All authors participated in the approval of the final version.
CRediT authorship contribution statement
MT Nguyen: Concept, Method, Data collection, Data analysis. Data curation, Writing—original draft, Writing—review and editing. CT Dang: Conceptualization, Formal analysis, revision. TBS Nguyen: Data collection, revision. NC Pham: Data collection, revision. DD Le: Software, Resources, Data curation, Data analysis. MD Pham: Data collection, revision. HT Nguyen: Data collection, revision. DT Dung Phan: Data collection, revision. DVP Nguyen: Data collection, revision. TP Nguyen: Data collection, revision. PV Doan: Data collection, revision. DS Nguyen: Data collection, revision. AV Pham: Concept, Method, Data collection, Data analysis. Data curation, Writing—review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Minh Thao Nguyen was funded by the PhD Scholarship Program of Vingroup Innovation Foundation (VINIF), code VINIF.2023.TS.115.
Ethics approval
Ethical approval for this study was obtained from the Institutional Review Board of Hue University of Medicine and Pharmacy (Approval Number/ID: H2021/443).
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.