
Abstract
Background:
Patient selection for either total knee arthroplasty or unicompartmental knee arthroplasty remains controversial. The latter has several reported advantages over total knee arthroplasty, but it also appears to have significant drawbacks in terms of revision rates.
Aims:
This study aimed to determine the influence of the preoperative degree of osteoarthritis on the risk of reoperation following unicompartmental knee arthroplasty.
Methods:
Surgery was carried out on 294 knees in 241 patients between 2001 and 2012 at a single institute, using cemented Oxford phase III unicompartmental knee arthroplasty. The mean age at the time of operation was 67 years, and the mean follow-up time was 8.7 years.
Results and Conclusion:
The knees with a preoperative Kellgren–Lawrence grade of 0–2 osteoarthritis had a higher risk of reoperation than those with a Kellgren–Lawrence grade of 3–4 (odds ratio = 1.89; 95% confidence interval, 1.03–3.45; p = 0.04). In addition, the knees with a medial joint space width of more than 1 mm or a high medial/lateral joint space width ratio had an increased risk of reoperation. In conclusion, we suggest that unicompartmental knee arthroplasty should only be performed in cases showing severe osteoarthritis in preoperative radiographs, with medial bone-on-bone contact, and a medial/lateral ratio of <20%.
Keywords
Introduction
Knee osteoarthritis (OA) is a common joint disease that may cause severe pain and lead to a reduced quality of life. In those aged 60 years and above, the prevalence of symptomatic OA is 9.6% in men and 18% in women (1). Total knee arthroplasty (TKA) is the gold standard option for the treatment of symptomatic OA of the knee when conservative treatment is insufficient. In addition to TKA, unicompartmental knee arthroplasty (UKA) may be used for the treatment of knee OA that is isolated to a single compartment. UKA appears to be a desirable procedure, as some advantages over TKA have been reported, including faster recovery time, reduced perioperative morbidity and mortality, a subjective preference for a more normal-feeling knee, lower cost, and improved time to return to work and sport (2, 3). However, the national arthroplasty registers consistently report a three to fivefold increase in crude cumulative 8- to 10-year revision rates for UKA compared with TKA (4–9). The reasons for this higher revision rate are not fully established.
Oxford phase III (Biomet, Warsaw, IN) has been the most common UKA used in Finland (4128 UKAs) with a 10-year cumulative revision risk of 17.1% (10). In all the major national arthroplasty registers, the survivorship of UKA is lower than that of TKA (4–9). Surgeon’s low experience and low operative volume have been found to be significantly associated with the UKA failure rate (7, 11–13). In addition, a mild or moderate degree of OA in preoperative radiographs is associated with increased risk of reoperation and dissatisfaction following knee replacement compared with severe OA (5, 13). It has been suggested that measurement of preoperative medial joint space width, or medial/lateral (M/L) joint space width ratio, should be used to assess the severity of OA (5). However, joint space width measurements are not validated or generally used in clinical practice.
The aim of this study was to assess preoperative degree of OA in patients with UKA and determine whether mild OA and a low Kellgren–Lawrence (KL) grading are associated with a higher revision rate in Oxford UKA patients (14).
Patients and Methods
A total of 294 cemented Oxford phase III UKAs were performed in 241 patients, of which 37% were male (108/294), with symptomatic OA between 2001 and 2012 in a single institution. The mean age of the patients was 67 years (range, 37–88 years). The mean follow-up time was 8.7 years (range, 1.9–13.5 years). Data were collected from the hospital’s patient records, including the following parameters: age, gender, date of primary UKA, follow-up time, preoperative medial and lateral joint space widths, preoperative KL grading, and date of revision if any.
Radiological Assessment
Preoperative radiographs were taken with each patient standing upright in front of the film cassette with knee in full extension or in 20° flexion. The x-ray beam was aimed horizontally at the joint line. From the preoperative radiographs, the medial and lateral joint space widths were measured in the middle of the respective compartments. The M/L joint space ratio was calculated from these measurements and expressed as a percentage (5). All the measurements were carried out by two senior orthopedic surgeons from digitalized radiographs. In addition to these measurements, the preoperative degree of OA was assessed using the KL scale. The preoperative weight-bearing radiographs were not available for 24 (8%) knees (not included in analyses).
Statistics
Continuous variables were described by mean and standard deviations, and categorical variables were described using frequencies and percentages. The associations between the reoperation and potential risk factors (gender, preoperative medial joint space width, preoperative M/L ratio, and KL-grade) were analyzed using logistic regression. The results were expressed by odds ratios (ORs) and 95% confidence intervals (95% CIs). Reoperation was defined as any operation performed on the UKA knee after the primary operation. Values of p < 0.05 were considered statistically significant. Statistical analysis was carried out using SAS for Windows, Version 9.3 (SAS Institute Inc., Cary, NC, USA).
Results
A total of 53 of 294 UKAs (18%) underwent revision. The average time between primary operation and revision was 3.7 years (range, 0.1–10 years). The reasons for revisions were component loosening (13 knees (12 tibial and 2 femoral components)), persistent pain (12 knees), progression of OA (12 knees), dislocation of the meniscal bearing (7 knees), intra-operative fracture or technical failure in the primary operation (6 knees), and infection (2 knees).
A total of 21.5% (40/186) of female patients and 12.0% (13/108) of male patients had a revision. Female patients had an increased risk of revision compared with male patients (OR = 2.00; 95% CI, 1.02–3.94; p = 0.04). The age of the patients was not associated with risk of revision (OR = 1.03; 95% CI, 0.99–1.06; p = 0.14).
Preoperative KL-grade was 0–2 in 110 knees (40.7%), and 3–4 in 160 knees (59.3%). Of the knees rated KL 0–2, 23.6% (26/110) had a revision and 13.8% (22/160) of KL 3–4 had a revision. The patients with KL 0–2 had higher risk for revision compared with KL 3-4 (OR = 1.89; 95% CI, 1.03–3.45; p = 0.04).
Preoperative high medial joint space or M/L ratio was associated with a higher revision rate (Figs 1 and 2). If the preoperative M/L ratio was ⩽20%, the reoperation rate was 10% (n = 10), and if the preoperative M/L ratio was >80%, the reoperation rate was 33% (n = 4). If the preoperative medial joint space was <1 mm, the reoperation rate was 11% (n = 13).
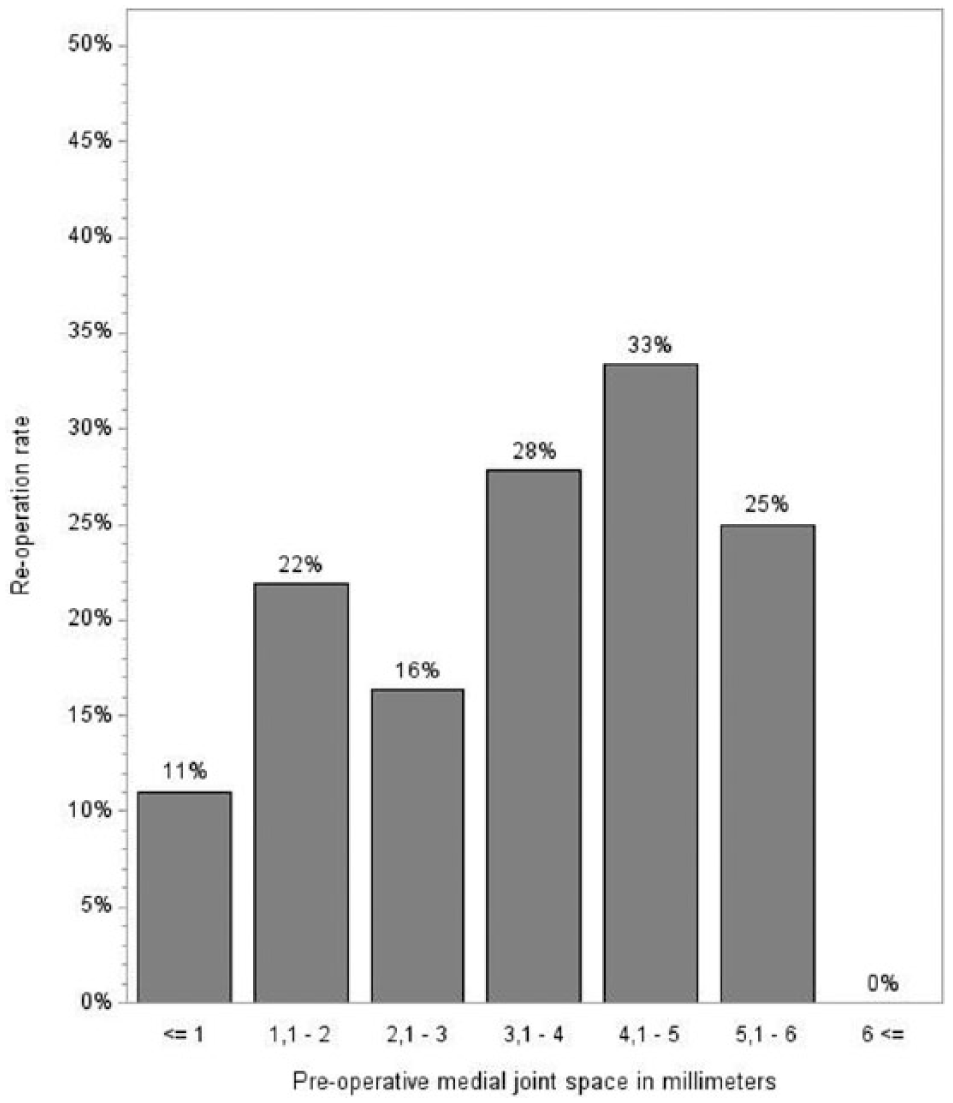
Preoperative thickness of medial joint space associated with reoperation rate: 1.1–2 versus ⩽1 mm, OR = 2.26, 95% CI, 0.99–5.17, p = 0.05; 2.1–3 versus ⩽1 mm, OR = 1.58, 95% CI, 0.61–4.08, p = 0.35; 3.1–4 versus ⩽1 mm, OR = 3.11, 95% CI, 1.23–7.87, p = 0.02; 4.1–5 versus ⩽1 mm, OR = 4.04, 95% CI, 1.30–12.59, p = 0.02; 5.1–6 versus ⩽1 mm, OR = 2.04, 95% CI, 0.43–12.31, p = 0.25.
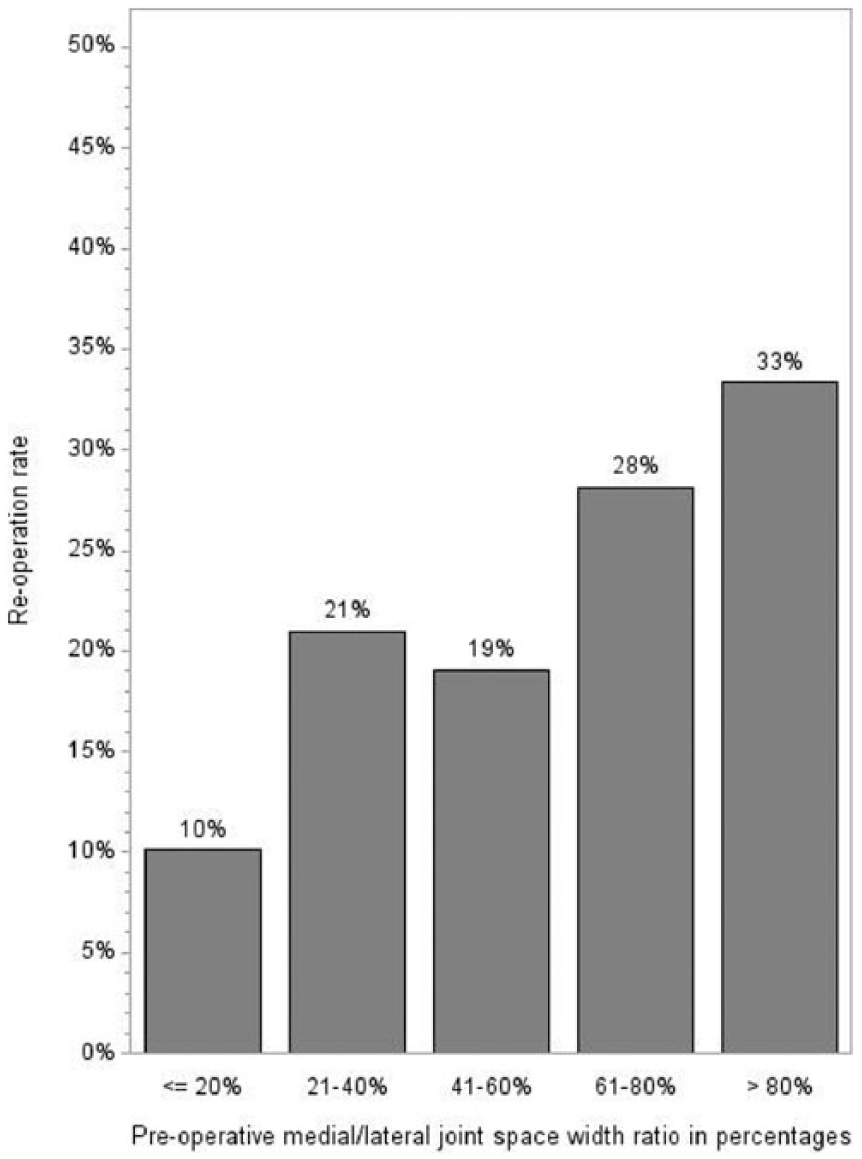
Preoperative M/L ratio associated with reoperation rate: 21%–40% versus ⩽20%, OR = 2.36, 95% CI, 1.02–5.50, p = 0.05; 41%–60% versus ⩽20%, OR = 2.09, 95% CI, 0.76–5.75, p = 0.15; 61%–80% versus ⩽20%, OR = 3.48, 95% CI, 1.27–9.57, p = 0.02; >80% versus ⩽20%, OR = 4.45, 95% CI, 1.14–17.45, p = 0.03.
Discussion
The revision rate of UKA has been consistently reported to be higher compared with TKA, and the reasons for higher revision rate have not been fully established. It has been suggested that symptomatic patients who has radiologically mild OA have an increased risk for revision. This study was conducted to assess preoperative degree of OA in patients undergoing UKA and determine whether mild OA and a low KL grading are associated with a higher revision rate in Oxford UKA patients. In this study, the overall UKA revision rate was high (18%). All the operated patients had symptomatic OA, but a significant number of UKAs were performed on patients with radiologically mild OA (45.6%, KL 0–2). We found that in addition to female gender, radiologically mild OA (KL grade 0–2) in preoperative radiographs increased the risk of revision (OR = 1.89).
The higher revision rate of UKA compared with TKA may be associated with the severity of the preoperative OA. The Oxford UKA’s developing group has reported a superior 94% rate of survival at 10 years when the original Oxford UKA indications are respected (full thickness cartilage loss and anteromedial OA with bone-on-bone contact) (15). In the recently published UKA studies, radiologically mild OA has been associated with high reoperation or revision rates, and there is a potential risk that UKAs are performed on patients, who are symptomatic, but whose knee OA is radiologically not severe enough to justify UKA (5, 16). The results of this study are similar to those of previous studies. In addition, we observed that the surgeons have expanded UKA indications, as only 54% of the operated knees had KL 3–4 OA and a 33% medial joint space of 2 mm or less. It appears that expansion of the UKA indication to radiologically milder OA may be a problem, at least in Finland at a national level, as similar results have been reported from another independent hospital without any national guidelines or indications for performing UKA (5). Unfortunately, it appears that adoption of the information from the manufacturer and education of surgeons with regard to setting indications for the Oxford UKA has not been successfully.
Degenerative changes of the knee (narrowing of the joint space, partial thickness, loss of cartilage, and degenerative meniscus rupture) are relatively common findings in middle-aged and elderly people, even if the knee is asymptomatic. Therefore, in symptomatic patients, degenerative changes are not always the cause of the pain. On the basis of the results of this study, UKAs are potentially performed on patients for whom knee pain does not originate from OA, and these patients have an increased risk of unsatisfactory results and subsequent UKA revision for any reason. This phenomenon is similar in TKA patients, as those suffering from mild or moderate OA are also at risk of dissatisfaction following this procedure (16). Furthermore, patients with pain following UKA may be more likely to have a revision than patients with pain following TKA (17).
In this study, the most common reason for revision was component loosening, especially in the tibial side (11/13 of the loose implants). The relationship between radiologically mild OA and component loosening is not clear. We propose that in dissatisfied patients any abnormal radiological findings are believed to be related to patients’ symptoms, leading to unnecessary revisions and unsatisfactory results after the revision. An example of this is a misdiagnosis of loosening; radiolucent lines are a common finding adjacent to cemented UKAs, and they may be falsely diagnosed as component loosening, particularly on the tibial side (18, 19). However, in this study, the overall UKA revision rate was high (13.8% at a mean 8.7 years) even if patients had sufficient indication in terms of degree of OA (KL 3–4). In the medial side, the optimal condition for adequate cement fixation is not always achieved, due to the mall cementing area, sclerotic bone, and lack of cancellous bone. The cementing technique of medial UKA is demanding, and the high rate of implant loosening may reflect the surgeons’ lack of experience in performing UKAs.
Our study has some limitations. Among them is that the effect of procedure volume per surgeon on revision rate was not separately assessed. Furthermore, the study design was observational and retrospective, and therefore also vulnerable to other omitted variables, which may have confounded our findings. Information regarding potentially important variables, such as comorbidity, was unavailable, as was important clinical information, such as measurable patient-reported outcomes data. Furthermore, preoperative radiographs were taken with each patient standing upright in front of the film cassette with knee in full extension or in 20° flexion. Radiographs taken in full extension may underestimate the degree of OA. However, we think that the effect of this bias on our results is minor.
On the basis of the results of the study, we conclude that Oxford UKAs are frequently performed in patients whose OA is radiologically not severe enough to justify the UKA procedure. This may be a significant reason for the discrepancy between the different survivorships of UKA and TKA in unadjusted arthroplasty data. We strongly recommend that in the preoperative, standing, weight-bearing radiographs, the degree of knee OA should be KL 3 or 4, the thickness of the medial joint space should be <20% of the thickness of the lateral joint space, and the medial joint space must be <1 mm. Other treatment choices, such as high tibial osteotomy, should be considered in patients not satisfying these criteria.
Footnotes
Acknowledgements
The study is a register-based retrospective study. Institutional review board approval is not demanded in Finland in this type of studies.
Declaration of Conflicting Interests
One of the authors, T. Niinimäki, has had paid presentations for Stryker, DePuy, and Biomet. Other authors don’t have conflicts of interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.