
Abstract
Background and Aims:
One by one, minimally invasive alternatives to established gastrointestinal procedures have become clinical routine. We have studied the use of laparoscopy in four common procedures—cholecystectomy, appendectomy, reflux surgery, and bariatric surgery—as well as in major resectional gastrointestinal surgery in Sweden.
Materials and Methods:
The National Patient Registry was used to identify all in-hospital procedures performed in patients above the age of 15 during 1998–2014, meeting our inclusion criteria. For each group, the annual number of procedures and proportion of laparoscopic surgery were studied, as well as applicable subgroups. Differences in age, gender, as well as geographical differences were evaluated in the most recent 3-year period (2012–2014).
Results:
In total, 537,817 procedures were studied, 43% by laparoscopic approach. In 2012–2014, the proportion of laparoscopic surgery ranged from high rates in the four common procedures (cholecystectomy 81%, appendectomy 47%, reflux surgery 72%, and bariatric surgery 97%) to rather low numbers in resectional surgery (4%–10%), however, increasing in the last years. In appendectomy and cholecystectomy, men were less likely to have laparoscopic surgery (42% versus 51% and 74% versus 85%, respectively, p < 0.001). Substantial geographical differences in the use of laparoscopy were also noted, for example, the proportion of laparoscopic appendectomy varied from 11% to 76% among the 21 different Swedish counties.
Conclusion:
The proportion of laparoscopy was high in the four common procedures and low, but rising, in major resectional surgery. A large variation in the proportion of laparoscopic surgery by age, gender, and place of residence was noted.
Introduction
Laparoscopic surgery is taken for granted by both surgeons and the general public at present. However, after Kelling’s pioneering inspection of the peritoneal cavity of a dog in the beginning of the 20th century, it took 60 years until diagnostic laparoscopic procedures were performed in routine care and an additional 30 years before reaching gastrointestinal surgery. Laparoscopy has several well-known benefits, for example, reduced postoperative pain, shorter hospital stay, improved cosmetic results, and shorter convalescence. However, these gains must be weighed against potential drawbacks, for example, increased technical demands and the blind entry of the first trocar, a new problem in laparoscopic surgery. In addition, to reduce the duration of surgery and improve safety, technical skills are also important for the whole operative team as many specialized instruments are used, all with multiple settings.
Based on earlier work on operative volumes in upper abdominal surgery (1, 2), we wanted to investigate the role of laparoscopy in four common procedures, that is, cholecystectomy, appendectomy, reflux surgery, and bariatric surgery, and evaluate the development in four fields of major resectional surgery (colorectal, esophago-gastric, liver, and pancreatic resections). The chosen procedures are characterized by quick transition in laparoscopic cholecystectomy, in contrast to a slow start in laparoscopic appendectomy, and an increased total number of procedures in reflux and bariatric surgery. In resectional surgery, on the other hand, many surgeons have been hesitant to adopt the laparoscopic approach, perhaps because of the specific oncological demands, for example, radical resection of the tumor and lymph node stations, risk of spreading the tumor peroperatively, as well as problems with extraction of the specimen.
The Swedish health care system is well suited for studying the use of different surgical techniques as most health care is recorded in national databases, always based on the individual’s unique 10-digit personal identification number (PIN). Data on in-hospital care are stored in the National Patient Register (NPR), kept by the National Board of Health and Welfare. NPR contains, among other variables, age, gender, place of residence, and type of surgical procedure. Since 1997, all surgical procedures have been classified according to the Swedish Classification of Operations and Major Procedures. As Swedish health care is publically funded and locally run by 21 counties, all individually responsible for the health care of their inhabitants, geographical comparisons can be of special interest.
The aim of this study was to describe the use of laparoscopy in gastrointestinal surgery by studying four common surgical procedures and four organ-related types of major resectional surgery in Sweden during 1998–2014. A secondary aim was to evaluate the use of laparoscopy with regard to differences in age, gender, and place of residence.
Materials and Methods
We performed a data extraction from NPR on all in-hospital procedures performed in 1998–2014 on individuals ⩾15 years of age, in the following eight fields: cholecystectomy (JKA20-21), appendectomy (JEA00-01), reflux surgery (JBC00-01 and JBW96-97), bariatric surgery (JDF10-98 and JFD03-04), colorectal resections (JFB20-97 and JFH10-96), esophago-gastric resections (JCC00-97, JDC00-97, and JDD00-96), liver resections (JJB00-96), and pancreatic resections (JLC10-96). Total number of procedures, proportion of laparoscopy, and, for applicable groups, different subgroups of surgical procedures were studied. Variations in the use of laparoscopy based on age, gender, and place of residence were studied in the most recent 3-year period (2012–2014).
Results
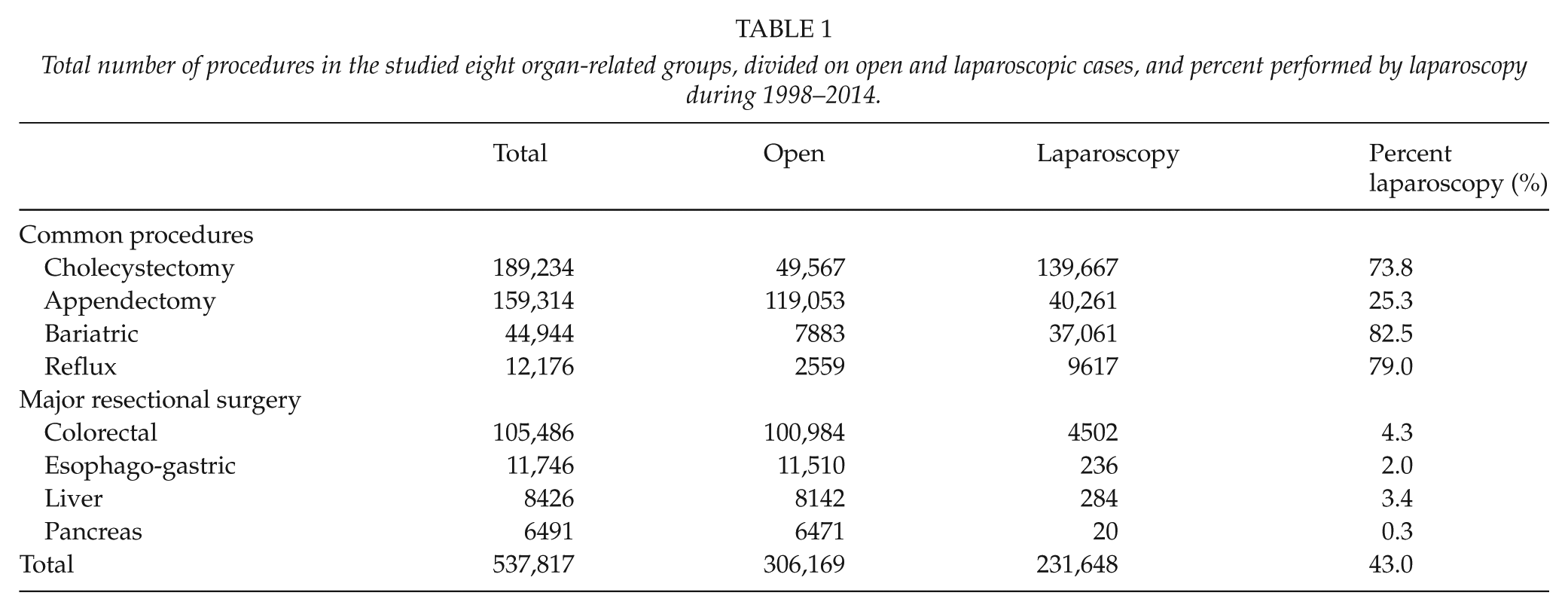
According to NPR, a total of 537,817 procedures were performed during 1998–2014 in the eight studied groups. The number of procedures in each group, open and laparoscopic, is listed in Table 1. As expected, cholecystectomy (n = 189,234) and appendectomy (n = 159,314) were the most frequent procedures, followed by colorectal resections (n = 99,674) and bariatric surgery (n = 44,944). In total, 43.1% of the procedures were performed by laparoscopic approach.
Total number of procedures in the studied eight organ-related groups, divided on open and laparoscopic cases, and percent performed by laparoscopy during 1998–2014.
The Use of Laparoscopy in the Four Common Procedures
The proportion of laparoscopic cholecystectomies was as high as 68% already in 1998 and increased to 82% in 2014. An almost fourfold rise in the proportion of appendectomies performed laparoscopically was seen during the study period, from 12% to 54%. In bariatric surgery, both the proportion of laparoscopy and the total number of bariatric procedures increased markedly during the study period, from 21.6% of 712 procedures to 97% of 5008 procedures. With a 10-fold increase in laparoscopic gastric bypass during the study period, laparoscopic bariatric surgery surpassed open in 2006. In 2012–2014, 98% of all gastric bypass and 93% of all gastric sleeves were completed by laparoscopic technique, while laparoscopy was used in 25% of duodenal switches, a procedure predominantly used in super obese patients (body mass index (BMI) > 50). The proportion of laparoscopy in reflux surgery was rather constant, 83%–81%; however, only a quarter of the total number of procedures remained in 2014 (303 versus 1310 in 1998).
Laparoscopy in Major Resectional Surgery
The evolution of laparoscopy in resectional surgery was rather slow, with no field passing 5% until 2011 (Fig. 1B). During the last years, a rise of laparoscopic use was seen in colorectal resections and esophago-gastric resections, both approaching 15% in 2014. In colorectal resections, the proportion of laparoscopy varied with the type of procedure and was highest in sigmoid resection (15% in 2012–2014). In esophago-gastric resections, a quick rise from 5% in 2012 to 30% and 9%, respectively, was seen. Laparoscopic liver resections noted a slow but steady increase to 7%. Very few laparoscopic pancreatic resections were registered, 2% in 2014; however, 6% of all distal pancreatic resections had been performed with laparoscopic technique.
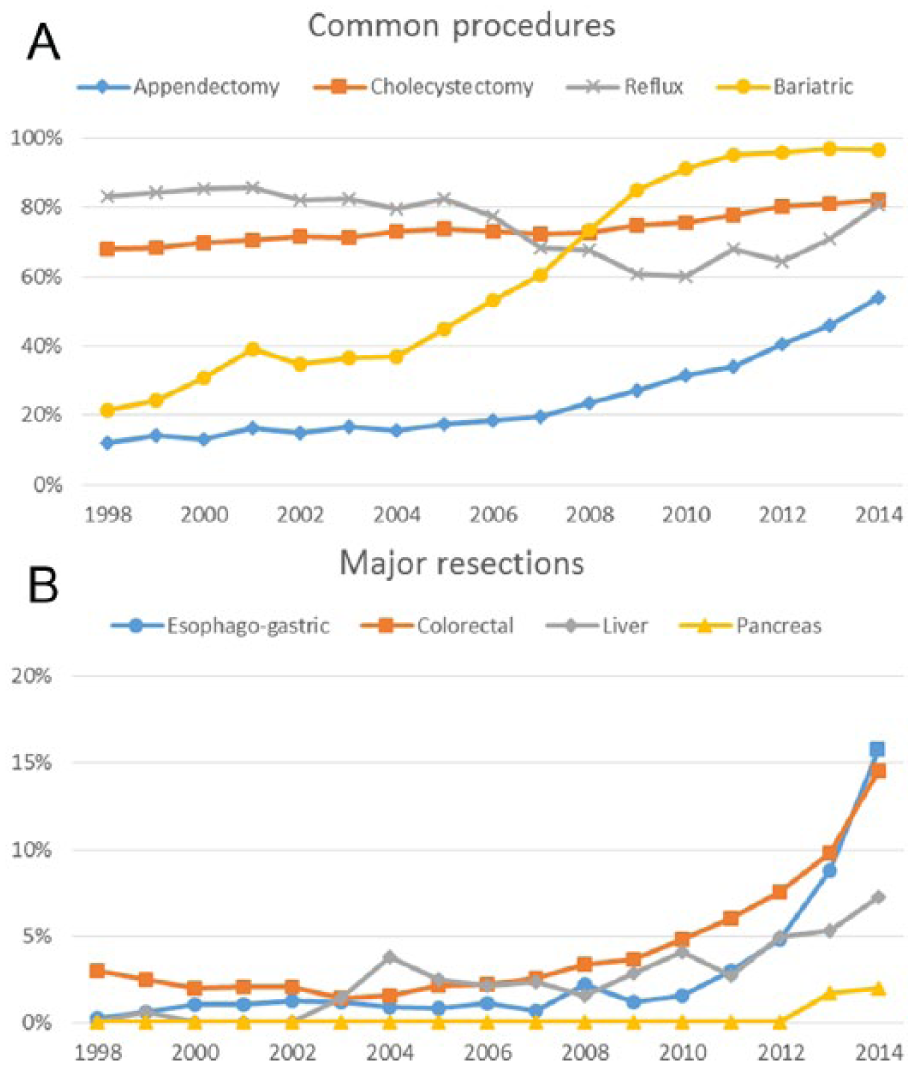
Proportion of laparoscopic surgery in the eight studied fields: A) common procedures and B) major resectional surgery.
Differences in Age and Gender
The large use of laparoscopy in cholecystectomy, appendectomy, reflux surgery, and bariatric surgery in the recent period made specific analyses possible. A difference in age and gender was seen in appendectomy and cholecystectomy, where the use of laparoscopy diminished with age and was less used in men compared to women (42% versus 51% and 75% versus 86%, respectively, p < 0.001 for both) (Fig. 2). In appendectomy, laparoscopy was 40% more common in women < 40 years compared to men in the same age group. No large gender or age differences in proportion of laparoscopy were seen in reflux or bariatric surgery.
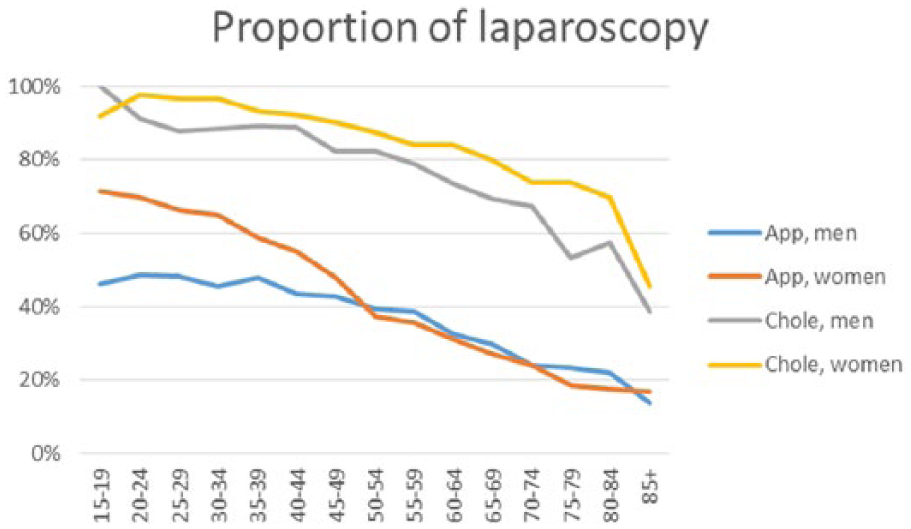
Proportion of laparoscopic cholecystectomies and appendectomies in 2012–2014 by age and gender.
Geographic Differences
In the recent period, appendectomy had been performed by laparoscopy in 43% of all cases nationwide, ranging from 17% to 80% in the 21 different counties, an almost fivefold difference (Fig. 3). The corresponding figures for laparoscopic cholecystectomy were 78%, with a span of 59%–91%. Small geographical variations were seen for the most common bariatric procedure, gastric bypass, performed by laparoscopy in 91%–100%. In reflux surgery and major resectional surgery, the number of laparoscopic procedures was too low to allow meaningful calculations.
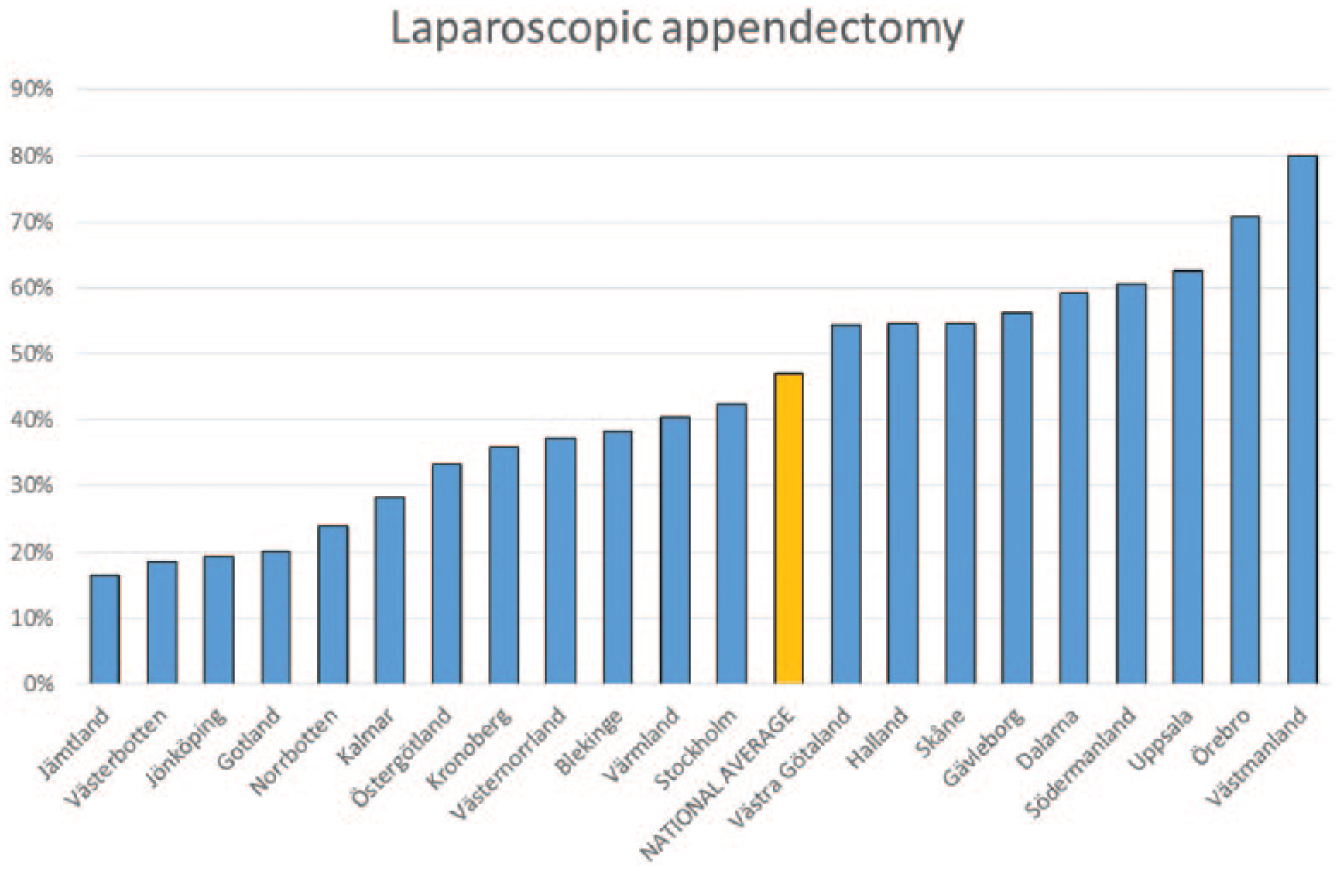
Use of laparoscopy for appendectomy in the 21 different Swedish counties, all autonomous on the use of health care for their citizens. Note the large variation, 17%–80%, and the national average of 43%.
Discussion
In this nationwide population-based study of gastrointestinal surgery in Sweden, we could establish that the proportion of laparoscopic surgery in 2012–2014 varied from high rates in the four common procedures (47%–97%) to rather low numbers in major resectional surgery (4%–10%), albeit, increasing in recent years. In bariatric surgery, a large increase in the use of laparoscopy was seen, 22%–97%, parallel to a 10-fold increase in the absolute number of procedures. In appendectomy and cholecystectomy, younger patients as well as women were more likely to have laparoscopic surgery. Substantial geographical differences were noted in laparoscopic appendectomy.
The introduction of laparoscopy in gastrointestinal surgery started with the first laparoscopic cholecystectomy by Muhe (3) in 1985. Although concerns about increased incidence and severity of bile duct injuries in laparoscopic cholecystectomies were raised (4), laparoscopy surpassed the open approach already in 1992/1993 in the United States (5) and Sweden. The minimized operative trauma and shorter hospital stay, two quickly noticeable up-sides of the laparoscopic approach (6), started the laparoscopic boom in gastrointestinal surgery.
Laparoscopic appendectomy has the advantage of an initial diagnostic examination (7). Thus, patients diagnosed of not having appendicitis can be treated promptly for their actual disease. As demonstrated in this study, laparoscopic appendectomy has been prioritized in women (40% more frequent in younger women than men in 2012–2014), probably because of a perceived risk reduction of female infertility. Apparently, in routine care, Swedish surgeons have been more prone to use laparoscopy in younger patients. This might be explained by cosmetic reasons as well as by a tendency to prioritize short hospital stay and postoperative recovery in professionally active patients. Laparoscopic appendectomy surpassed open technique in 2013/2014, 8 years later than in the United States (8). The slow transition in Sweden could partly be explained by reports of identical short-term morbidity and mortality (9) and lack of national data on reduced risk of small bowel obstruction after laparoscopic appendectomy, until recently (10).
Reflux surgery, the next field in line to introduce laparoscopy, struggled with initial technical difficulties, for example, the new demand of intraabdominal suturing for closing the hiatal defect and constructing the fundoplication. In 1996, laparoscopy surpassed open surgery in both Sweden and the United States; however, in Sweden, operative volumes have thereafter been reduced by 75%. This is perhaps due to suboptimal results during the initial period of over-exploiting (1, 11).
Although the worldwide epidemic of obesity requires multiple actions, bariatric surgery has been demonstrated to be a valid option. In Sweden and many other countries, the number of bariatric procedures has rocketed during the last decade. Laparoscopic approach surpassed open surgery in Sweden in 2006, 1 year later than in the United States (12). In 2008, laparoscopy was used in over 90% of the 340,000 procedures performed globally (13). Two specific drawbacks exist in laparoscopic bariatric surgery: risk of intraabdominal injuries during the passage of the first trocar through the thick abdominal wall (14–17) and the reduced formation of adhesions, allowing the small bowel to slide into mesenteric openings. The latter has created a rising demand for computed tomography (CT) scans and emergency re-laparoscopy in this increasing group of patients, an unexpected disadvantage of the laparoscopic concept.
Although laparoscopic resection for colon cancer was reported in 1991 (18), the general introduction of laparoscopy has been rather slow, in spite of the possibility of an extracorporeal anastomosis through the extended incision required for extraction of the specimen. Early reports on high incidence of port-site metastases (19) as well as problems to locate the tumor and deciding on resectional margins without tactile evaluation could be an explanation. In the United States, laparoscopy surpassed open surgery in 2006, while open surgery still dominates in Sweden (83% in 2012–2014). In the literature, both procedures have been associated with shorter hospital stay compared to open surgery (7 versus 9 days and 4–5 versus 7 days, respectively) (20, 21).
In esophageal resection, one of the largest operations in gastrointestinal surgery, minimal invasive esophagectomy (MIE), has several advantages, making surgical treatment possible for a group patients often burdened with considerable comorbidity. In a randomized study, surgical morbidity and postoperative respiratory complications as well as hospital stay were reduced by MIE, and surgery in the prone position reduced the risk of pulmonary infection and recurrent laryngeal nerve palsy, all compared to open surgery (22). In 2014, almost one-third of all esophagectomies in Sweden were performed by minimal invasive approach. Laparoscopic gastrectomy has, since its first introduction in 1994 (23), received increased attention in specialized centers. In the American National Cancer Database, minimal invasive gastrectomy (n = 331) was associated with shorter hospital stay, equivalent lymph node examination, and superior rates of R0 resection (24). The shorter hospital stay was verified in a systematic review (20,868 patients in 32 studies), which also demonstrated less blood loss and lower risk of complications (25). In addition, the risk of wound-related complications was lower after laparoscopy, although requiring an enlarged incision for removing the specimen.
After working with laparoscopic fenestration of liver cysts, laparoscopic liver resections were introduced in the early 90s (26). Although laparoscopic liver surgery is an expanding field internationally (1), the laparoscopic activity is rather low in Sweden, 6%, in 2012–2014. This is probably due to expected technical difficulties; however, the increasing numbers of local resections performed for unknown or small metastatic lesions could be a good way to increase the proportion of laparoscopic surgery, especially since most liver surgeons already use laparoscopic staplers in open procedures. Moreover, increased intraperitoneal pressure during a laparoscopic procedure can in fact be a way of controlling oozing hemorrhage, a special challenge in liver resections.
Despite that the first laparoscopic pancreatoduodenectomy was described as early as 1994 (27), the development of laparoscopic pancreatic surgery in Sweden has just begun according to our results, 2% in the last years. Interestingly, difficulties with preoperative staging yielded the first use of laparoscopy in this field, laparoscopic ultrasound, to improve staging and assessment of vascular involvement (28). Laparoscopy for neuroendocrine tumors of the pancreas has internationally gained more widespread use (29), and in the present material, an increased interest in laparoscopy was seen in distal pancreatectomies (6%), although tactile loss can be a problem as well as preservation of the spleen.
The registry-based design includes limitations, for example, calculations are done on existing data with no possibility to double-check entered codes in medical records. However, identical coding was used (Swedish Classification of Operations and Major Procedures), and all data are based on the patients’ unique PIN used in all contacts with the health care system. As NPR is limited to in-hospital procedures, laparoscopic day-care procedures, varying between 2500 and 4000 annually according to the National Board of Health and Welfare, are not included in this study. Moreover, the registry-based design has hindered us to look at the number of converted procedures, procedures started as laparoscopic but converted to open surgery, as these most often will be registered by the final result, an open procedure. Our figures, thus demonstrate the true number of laparoscopic procedures, those that were started and completed laparoscopically.
Conclusion
In this nationwide study on gastrointestinal surgery, the proportion of laparoscopy was high in the four common procedures, 47%–97% during 2012–2014, and rather low in resectional surgery, 4%–10%, however, increasing in the last years. Young age and female gender increased the chance of having laparoscopic appendectomy and cholecystectomy. This and the geographical differences in the use of laparoscopy warrant further discussion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.