
Abstract
Objective
To investigate the clinical efficacy of laparoscopic gastrointestinal emergency surgery and postoperative complications.
Methods
Data for 604 patients undergoing emergency gastrointestinal surgery between January 2013 and December 2018 were analyzed retrospectively. Treatment efficacy and postoperative complications were compared between 300 patients (control group) undergoing traditional laparotomy and 304 patients (observation group) undergoing laparoscopic surgery.
Results
Clinical features were significantly better in the observation group than in the control group, including duration of surgery (59.12 ± 10.31 minutes vs. 70.34 ± 12.83 minutes), intraoperative blood loss (41.21 ± 10.45 mL vs. 61.38 ± 9.97 mL), postoperative pain score (1.25 ± 0.25 points. vs. 5.13 ± 0.43 points), length of hospital stay (5.13 ± 0.24 days vs. 7.05 ± 0.13 days), and time to free activity (13 ± 2.96 hours vs. 22 ± 3.02 hours). The total complication incidence in the observation group was 3.9%, compared with 16% in the control group (16%). No significant differences in direct medical costs were recorded between the observation and control groups.
Conclusions
For patients undergoing emergency gastrointestinal surgery, laparoscopic surgery resulted in better clinical outcomes than traditional laparotomy without incurring additional costs. The potential clinical benefits of emergency laparoscopic gastrointestinal surgery warrant further study.
Keywords
Introduction
Acute appendicitis, peptic ulcer perforation, intestinal obstruction, colorectal rupture, and acute gastrointestinal hemorrhage are all commonly treated by emergency gastrointestinal surgery. These illnesses share clinical characteristics including acute onset, severe abdominal pain, and symptoms of diarrhea, nausea, and vomiting. 1 Cases can become life-threatening in the absence of immediate proper treatment, which generally entails traditional laparotomy. However, such treatment is inevitably associated with significant disadvantages including a large wound and prolonged post-operative recovery time. Rapid developments in laparoscopic surgery have recently revealed its potential for improving the efficacy and clinical outcomes of emergency gastrointestinal surgery. These include a smaller wound, shorter recovery time, enhanced safety, and surgical accuracy. With these apparent advantages, laparoscopic surgery could become the method of choice for performing emergency gastrointestinal surgery.2–4
Materials and methods
Study groups
In total, the outcomes of 604 patients undergoing emergency gastrointestinal surgery between January 2013 and December 2018 were analyzed retrospectively. All cases in the study period were included. The control group underwent traditional laparotomy, and the observation group received laparoscopic surgery. For all patients, diagnosis was confirmed on the basis of appropriate disease-specific criteria. Patients were all admitted without severe cardiovascular or brain disease. Data were compared between the groups to retrospectively evaluate the features of surgery and post-operative outcomes including the duration of surgery, intraoperative blood loss, post-operation pain score, duration of hospital stay, and incidence of complications. Comorbidities were also calculated. All details of ethical approval and human rights of this study were approved by the Institutional Patient Care and Data Use Committee of Wuhan University. Our findings revealed the clinically significant advantages of laparoscopic surgery and provide reference values for future research and clinical practice.
Surgical procedures
Patients in the control group underwent traditional laparotomy under general anesthesia for diagnosis and treatment. Those in the observation group underwent laparoscopic surgery under general anesthesia. The surgeons were all senior professors (male; 45–55 years old) in the GI Surgery Department with more than 15 years of experience. Drainage tube placement was based on the individual patient condition. 5 All surgical procedures conformed to clinical guidelines appropriate for specific gastrointestinal disease treatment including selection of the incision site and avoidance of intestinal adhesions.6,7
Clinical indices
The surgery-associated features analyzed and compared in this study were as follows: duration of surgery, intraoperative blood loss, post-operation pain score, duration of hospital stay, and incidence of complications. The pain score was determined 24 hours after surgery based on a visual analog scale and scored as follows: painless, 0 to 2; mild pain, 3 to 5; moderate pain, 6 to 8; and severe pain, 9 to 10. Complications were recorded during a 3-month postoperative follow-up period.
Cost analysis
Direct medical costs (admission fees, procedure fees, consumable fees, medication fees, and nursing fees) spanning from the time of patient admission to discharge were tabulated using hospital charge lists.
Statistical analysis
Statistical analysis was performed using SPSS 19.0 software (SPSS Inc, Chicago, IL, USA). Data were presented as the mean ± SD. Student’s t-test was used for comparison between groups. The χ2 test was used for enumeration data. P < 0.05 was considered significant.
Results
Patient profiles
Patient ages ranged from 17 to 79 years (mean, 40.1 ± 10.5 years). The 604 study patients comprised 240, 136, 128, and 100 cases of peptic ulcer perforation, acute appendicitis, colorectal rupture, and intestinal obstruction, respectively. The control group (n = 300; 160 men and 140 women; mean age, 39.2 ± 11.5 years) was treated via traditional laparotomy. The observation group (n = 304; 166 men and 136 women; mean age, 36.1 ± 10.2 years) was treated by laparoscopic surgery. According to the calculation and analysis of comorbidities, the two groups were comparable in terms of the severity of cases. There were no significant differences in patient profiles (as shown in Table 1) and case severity (as shown in Table 2) between the two groups (P > 0.05).
Patient profiles.

Unless otherwise indicated, data are presented as n (%).
Comorbidities.

Unless otherwise indicated, data are presented as n (%).
Comparative surgical and postoperative indices
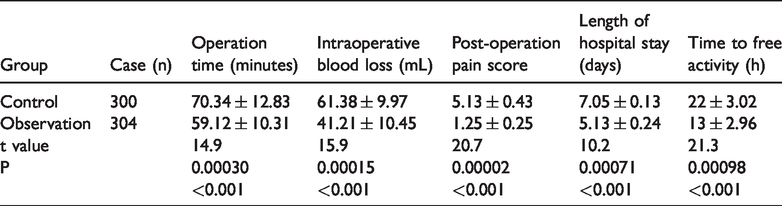
The mean duration of laparoscopic surgery was 59.12 ± 10.31 minutes in the observation group, which was significantly shorter than the mean surgical duration of 70.34 ± 12.83 minutes in the control group (P < 0.05). The results for other indices all indicated significantly improved outcomes (P < 0.05) for patients receiving laparoscopic surgery compared with traditional laparotomy as follows: intraoperative blood loss, 41.21 ± 10.45 mL vs. 61.38 ± 9.97 mL; postoperative pain score, 1.25 ± 0.25 points vs. 5.13 ± 0.43 points; duration of hospital stay, 5.13 ± 0.24 days vs. 7.05 ± 0.13 days; and time to free activity, 13 ± 2.96 hours vs. 22 ± 3.02 hours. These results are presented in Table 3.
Comparative surgical and postoperative indices.
Postoperative complications
As shown in Table 4, the incidence of postoperative complications was significantly lower for patients receiving laparoscopic surgery than in those undergoing traditional laparotomy. After 3 months of follow-up, the total complication incidence in the observation group was 3.9%, compared with 16% in the control group (P < 0.05). Laparoscopic surgery was not associated with any incidence of postoperative abdominal infection or septicemia, compared with rates of 4% and 1.3%, respectively, in the control group. All other examined complications were less frequent in the observation group than in the control group, including wound infection (0.7% vs. 2.7%), vomiting (1.3% vs. 4%), and nausea (2% vs. 4%). Disease subgroups were also analyzed. The results revealed remarkable advantages for laparoscopic surgery in all subgroup diseases, as shown in Table 5.
Comparative postoperative complications during 3 months of follow-up.

Comparative clinical indices of all subgroups.

Cost comparison
Costs were separated into several fee categories including hospitalization, laboratory, radiology, nursing, medication, anesthesia, consumables, and surgery. More specific itemized cost analysis requiring access to hospital financial system records was not possible this study. Total costs were divided into National Health Insurance (NHI) covered fees and uncovered fees (paid by patients). As shown in Table 6, no significant overall cost difference was observed between the control and observation groups (P > 0.05).
Comparison of medical costs (Chinese Yuan, RMB) between the observation and control groups.

Discussion
It is important to quickly and efficiently diagnose and treat cases of acute appendicitis, peptic ulcer perforation, intestinal obstruction, colorectal rupture, and acute gastrointestinal hemorrhage. Such cases can rapidly progress, and patients can experience severe symptoms and signs, including continuous and serious abdominal pain, board-like rigidity, signs of peritoneal irritation, and unstable vital signs. However, traditional laparotomy in the treatment of acute appendicitis and peptic ulcer perforation is usually associated with postoperative complications such as wound infection. The incidence of complications decreases sharply when laparoscopic surgery is employed. The feasibility of replacing laparotomy with laparoscopic surgery can be enhanced through more extensive clinical research and practice, leading to lower rates of misdiagnosis and post-operative complications.8–10 Moreover, research has revealed that establishing pneumoperitoneum for intestinal decompression in patients with intestinal obstruction improved treatment efficacy and led to better clinical outcomes including shorter durations of surgery, less intraoperative blood loss, lower postoperative pain scores, and shorter lengths of hospital stay.11–13
Minimally invasive laparoscopic surgery has been performed for 30 years, and continuous improvements in techniques and equipment have produced a reliable clinical procedure for emergency gastrointestinal surgery. 14 Compared with traditional laparotomy, laparoscopic surgery is more generally accepted, and it is associated with the relative advantages of smaller wounds, reduced pain, shorter operation time, less intraoperative blood loss, shorter length of hospital stay, and fewer complications.15–17 Additionally, it is possible through enlarged,multi-dimension viewing at higher defin-ition and greater illumination to perform laparoscopic surgery without opening the abdominal or exposing organs to the environment. This can lead to a lower incidence and severity of postoperative gastrointestinal irritation and adhesion. However, the technical demands of laparoscopic surgery require the availability of a highly skilled and qualified surgeon for preoperative assessment and emergency treatment. 18 Furthermore, there are seve-ral contraindications for laparoscopic surgery including severe cardiopulmonary dysfunction, coagulation disorders, and pregnancy.
The present study confirmed the aforementioned significant advantages of laparoscopic surgery compared with laparotomy for use in emergency gastrointestinal surgery. Laparoscopic surgery yielded significantly better outcomes than laparotomy in terms of the duration of surgery, intraoperative blood loss, postoperative pain score, length of hospital stay, and time to free activity. The same improved outcomes were observed for postoperative complications including wound infection, vomiting, nausea, abdominal infection, and septicemia. These clinical improvements were obtained in the absence of increased medical costs.
In conclusion, based on superior clinical outcomes and similar costs, the present study results demonstrate the clear value of laparoscopic surgery as a general approach for emergency gastrointestinal surgery.
Limitation
Because of the retrospective approach, our study had some limitations. This was not a randomized study. Data were collected only from one research center. It was difficult to quantify and standardize the ability and judgment of all surgeons. The comparison of all operative techniques was not as detailed as possible. The follow-up period for these two groups was only 3 months. Thus, randomized controlled trials should be conducted in the future to further clarify the relative merits of these two operations.
Footnotes
Acknowledgement
Ning Cui performed data collection and analysis. Ning Cui and Jun Liu wrote the manuscript. Haiyan Tan conceived this study. All authors declare there was no conflict of interest with any other third party.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics Statement
We have checked approval with our review board and received their exemption. We have de-identified the details such that the identity of the patients may not be ascertained in any way.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.