
Abstract
Purpose:
We present our endoscopic technique for treating ejaculatory duct and seminal vesicle diseases with a holmium laser.
Materials and methods:
Fifteen patients with persistent hematospermia were enrolled in this study from June 2007 to April 2014. All patients had failed medical treatments. All patients were evaluated with transrectal ultrasound and pelvic computed tomography or magnetic resonance imaging. We performed endoscopic treatment with a semi-rigid ureteroscope after dilation using a guidewire and ureteral serial dilator. A holmium laser was used to incise the obstructed ejaculatory duct, coagulate hemorrhagic mucosa, and fragment stones in the ejaculatory duct or seminal vesicles. Stones were removed using a basket and forceps.
Results:
The mean duration of hematospermia was 30.6 months. Mean patient age was 45.3 years. The mean serum levels of prostate-specific antigen and testosterone were 1.36 and 4.95 ng/mL, respectively. No operative complications were encountered. Mean operative time was 35.4 min. Seven patients had ejaculatory duct or seminal vesicle stones, which were subsequently determined to be carbonate apatite, mucin, struvite, and calcium oxalate dehydrate stones. Mean duration of follow-up was 32.1 months. Although two patients showed recurrent hematospermia 11 and 12 months after the operation, hematospermia resolved in 13 patients (86.7%). The infertile patient showed an improved semen finding and had a successful pregnancy.
Conclusion:
Endoscopic treatment using a holmium laser is minimally invasive and was effective for treating ejaculatory duct and seminal vesicle diseases, which are the main cause of hematospermia.
Keywords
Introduction
Hematospermia is a relatively rare condition but is most prevalent in young men with a mean age of 37 years (1). Symptoms are generally of 1- to 24-month average duration. However, it is difficult to determine the exact cause of and treat intractable, persistent hematospermia. Ejaculatory duct and seminal vesicle diseases, which are the main causes of hematospermia, have been evaluated using revolutionized imaging techniques, including transrectal ultrasound (TRUS), and pelvic computed tomography (CT) or magnetic resonance imaging (MRI) (2, 3). Endoscopy had also been used as a minimal invasive modality to diagnose and treat (4, 5). We present cases of persistent hematospermia caused by ejaculatory duct and seminal vesicle diseases, which were managed by endoscopic treatment using a novel technique.
Material and Methods
Fifteen patients with persistent hematospermia were enrolled from June 2007 to April 2014. All patients had failed medical treatments, including antibiotics, anti-inflammatory drugs, or anti-androgen agents. They underwent a physical examination, urinalysis, and blood tests, including prostate-specific antigen (PSA), testosterone, and coagulation-related tests. Prostate massage, microscopic examination, and polymerase chain reaction analysis using prostatic secretions (Chlamydia, Mycoplasma, and Ureaplasma) were performed in patients with questionable prostatitis symptoms. Patients also underwent a TRUS and pelvic CT and/or MRI. Patients with acute prostatic inflammation or high serum PSA level were excluded. One patient had hematuria. One patient complained of infertility for 3 years, and a semen analysis showed oligospermia with a low ejaculate volume.
All operations were performed by a single surgeon. Patients were placed in the lithotomy position under spinal anesthesia. The urethra and verumontanum were examined using a 22F cystoscope. A 0.038-in guidewire was inserted into the ejaculatory duct orifice, and a ureteral serial dilator was inserted over the guidewire to 10F. If an ejaculatory duct obstruction was detected, the orifice was incised using a holmium laser (0.6 J, 10 Hz) with a 200-µm fiber (Fig. 1, Video 1). A semi-rigid ureteroscope (Stortz, Tuttlingen, Germany; 7F, 6°, length 34 cm, distal tip 6.5F) was inserted into the ejaculatory duct and seminal vesicles. Any abnormal lesion was biopsied, and hemorrhagic mucosal lesions were coagulated with the laser (0.4 J, 10 Hz). If a stone was detected in the ejaculatory duct or seminal vesicle, it was fragmented with the holmium laser (0.8 J, 10 Hz) and removed using a 4F stone basket and forceps (Fig. 2, Video 2). The stone was analyzed by Fourier transform-infrared spectroscopy (6). After the procedure, the hematoma and stone particles were washed with irrigating saline, and a urethral Foley catheter was inserted overnight.
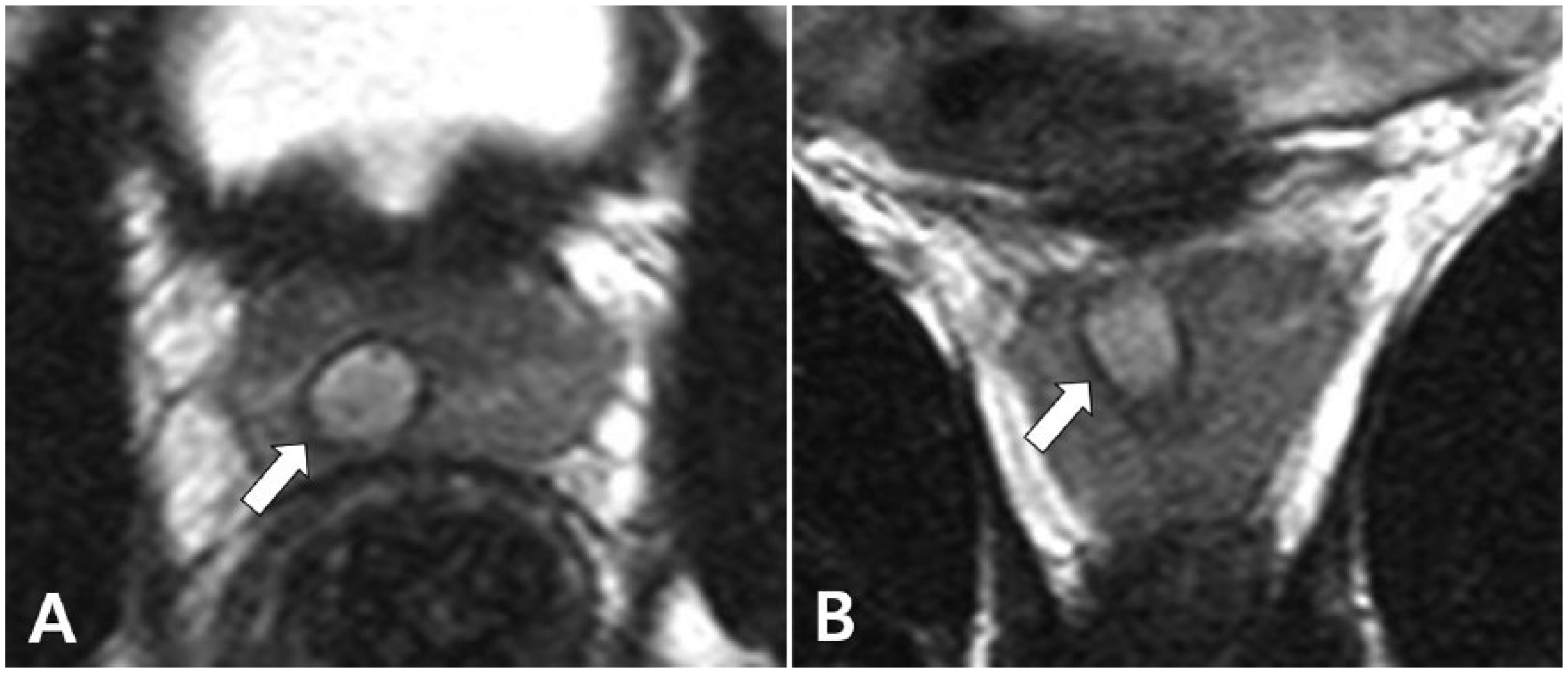
A 32-year-old man, with persistent hematospermia and infertility. (A) Axial and (B) coronal T2-weighted images demonstrate a right dilated ejaculatory duct with tiny stones and in-homogenous fluid.
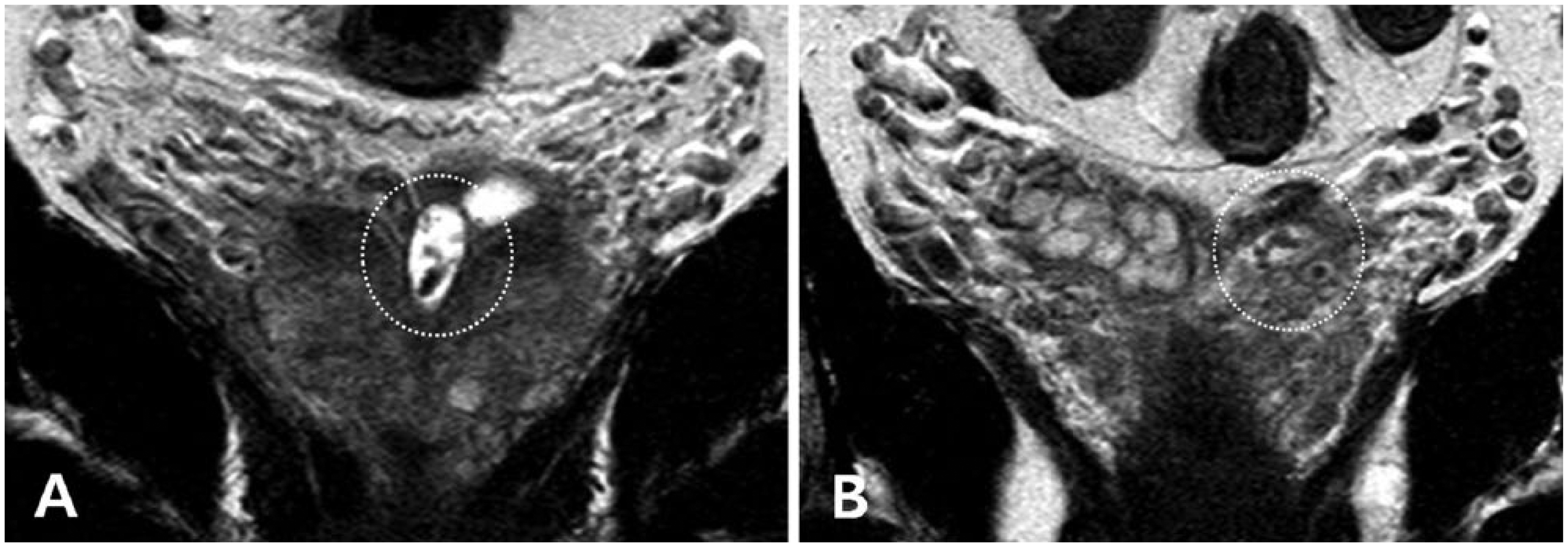
A 59-year-old man, with persistent hematospermia and ejaculatory pain. Coronal T2-weighted images demonstrate multiple stones (dotted circle) in the (A) left dilated ejaculatory duct and (B) seminal vesicle.
This study was approved by the institutional review board of our institution.
Results
The mean duration of hematospermia was 30.6 months (range, 4–72 months) in 15 patients. Mean patient age was 45.3 years (range, 13–68 years), and body mass index was 25.0 kg/m2 (range, 18.0–30.8 kg/m2). The mean serum levels of PSA and testosterone were 1.36 ng/mL (range, 0.44–2.08 ng/mL) and 4.95 ng/mL (range 2.12–9.48 ng/mL). No patient had a coagulation disorder. Mean operative time was 35.4 min (range, 13–68 min). No operative complications occurred, and all patients were discharged on postoperative day 1.
Ejaculatory duct obstructions were found in 10 (66.7%) of 15 patients. Stones were detected in the ejaculatory duct or seminal vesicles in seven patients (46.7%). The stone compositions were carbonate apatite in three patients, mucin in two, struvite in one, and calcium oxalate dehydrate in one. Hemorrhagic lesions were found in five patients (33.3%). All lesions were treated with the holmium laser. A seminal vesicle biopsy was performed in two patients and revealed chronic inflammation.
The mean duration of follow-up after the operation was 32.1 months (range, 6–80 months). Although two patients showed recurrent hematospermia 11 and 12 months after the operation, respectively, hematospermia resolved in 13 patients (86.7%). The infertile patient showed an improved semen finding, and his wife was pregnant 6 months postoperatively. Significant changes were observed in the preoperative and postoperative 2-month semen parameters, including ejaculate volume (0.5 and 1.5 mL) and sperm concentration (5.2 × 106/mL and 10.2 × 106/mL).
Discussion
A patient with persistent or recurrent hematospermia may be fearful of cancer and visit the urologist quickly (1, 7–10). If the specific cause is not found, the patient may become very anxious. The common causes of hematospermia are diseases of the ejaculatory duct, seminal vesicles, and prostate, which can be treated with transurethral endoscopy. Nevertheless, it remains challenging to determine a significant cause and definitive treatment for persistent hematospermia. Endoscopy has been used in patients with hematospermia. It is useful to observe seminal vesicle and ejaculatory duct (11).
Among the main causes of hematospermia, obstructions, stones, and inflammation of the ejaculatory duct and seminal vesicles have been managed by endoscopy with acceptable results. An ejaculatory duct obstruction is typically managed with a transurethral incision at the duct opening (12). Manohar et al. (13) divided ejaculatory duct obstructions into levels using TRUS. The obstruction was opened using a hook electrode and endoscissors (2-mm mini-shears) through a nephroscope and was confirmed with methylene blue. Cuda et al. (14) used a balloon dilator (Boston Scientific Uromax Ultra System) and pressure of 8 atm. The ejaculatory ducts were dilated to 18F. A few reports have mentioned pregnancies occurring after transurethral resection of the ejaculatory duct, and the risk of converting to a complete obstruction and azoospermia was not low (12, 15). We found a more effective treatment for an obstruction of the ejaculatory duct because we incised with a laser and dilated the obstruction with a ureteral serial dilator. We also report a successful pregnancy after the operation in one patient who was infertile. His ejaculate volume and sperm count analysis had improved.
Ejaculatory duct and seminal vesicle stones are extremely rare, and removal by endoscopy is challenging. The mechanisms of stone formation are unclear, and their composition varies, including carbonate apatite, magnesium ammonium phosphate, calcium oxalate, calcium phosphate, and uric acid (4, 5, 14, 16). We also found several compositions, including carbonate apatite, mucin, struvite, and calcium oxalate dehydrate.
Gordon et al. (4) reported the first case of removing an ejaculatory duct calculus endoscopically to treat infertility. They used a 21F cystourethroscope and 7F alligator grasping forceps. The stone analysis revealed a calcium phosphate composition. Özgök et al. (5) reported the first endoscopic procedure for seminal vesicle stones. They inspected the seminal vesicles and retrieved stones using a flexible 6.9F ureteroscope through a utricular orifice and then passed a 15.5F rigid urethroscope and a grasper to remove the stones. Cuda et al. (14) also presented a case report of seminal vesicle stones. They conducted a cystoscopy and inserted a guidewire into the seminal vesicle. A 7F semi-rigid ureteroscope was passed over the guidewire, and the stones were fragmented with a 270-µm holmium laser fiber. Residual fragments were removed by irrigation and a basket. The ejaculatory ducts were balloon dilated to 18F using a Boston Scientific Uromax Ultra System to a pressure of 8 atm. We also used a semi-rigid ureteroscope with a 200-µm laser fiber, which passed the accompanying 4F stone basket through the one working channel. However, the stones were usually small and crisp, and laser firing was not always needed.
Endoscopic treatment for persistent hematospermia is a challenging procedure until now, and only a few studies have been published on the subject. Song et al. (17) treated 12 patients with intractable hematospermia. They used a 0.8-mm Zebra guidewire and a 7.3F rigid ureteroscope in the ejaculatory duct. Seminal vesicle stones were identified and removed with a grasper and basket. Xing et al. (11) performed transurethral seminal vesiculoscopy for 85 patients with hematospermia. They used a 7F or 8F rigid ureteroscope and injected levofloxacin to wash the seminal vesicles. The most frequent cause was stones, followed by obstruction and stricture, dysplasia, polyp, and a benign mass. They reported an excellent success rate of 97.6%. Han et al. (18) performed a transutricular seminal vesiculoscopy for 70 patients with hematospermia. The success rate was 78.6% at the 12.3-month follow-up, and the recurrence rate was 10%.
Although the number of enrolled cases was limited, our study produced some significant results. The follow-up time of 32.1 months was relatively longer than that in previous reports. We used a novel technique to overcome a challenging operation. First, a guidewire and ureteral serial dilator were used to dilate the ejaculatory duct. A semi-rigid ureteroscope was then inserted easily after dilation to 10F. Second, a holmium laser was used to incise the obstructed ejaculatory duct, coagulate hemorrhagic mucosa, or fragment stones in the ejaculatory duct or seminal vesicles. A holmium laser can be safely activated 0.5–1 mm from the mucosal wall (19). It incises and coagulates precisely using a photothermal mechanism and fragments all stones regardless of composition. We completed all operations without a technical failure or operative complication.
Conclusion
Endoscopic treatment with a holmium laser is effective for diseases of the ejaculatory duct and seminal vesicles, which are main causes of hematospermia. This novel technique was minimally invasive and had acceptable reproducibility. This technique may come under the treatment guidelines for persistent hematospermia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This article was supported by Wonkwang University in 2014.