
Abstract
Background and Aims:
To compare the health-related quality of life in patients with narrow gastric tube and whole stomach reconstructions after oncologic esophagectomy.
Material and Methods:
In a prospective randomized single-center study from 2007 to 2008, 104 patients underwent esophagectomy for cancer. To assess health-related quality of life, the questionnaire (European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 and the Oesophagus-Specific Quality of Life Questionnaire 18) was administered at 3 weeks, 6 months, 1 year, and 2 years after surgery.
Results:
The perioperative complication rate was 26.9% in narrow gastric tube group and 48.1% in whole stomach group (P = 0.31). At the time of 3 weeks after surgery, the reflux and dyspnea scores were higher in whole stomach group than in narrow gastric tube group, which meant that the patients in whole stomach group suffered more severe problem. At the time of 6 months and 1 year after surgery, the reflux scores were lower in narrow gastric tube group than in whole stomach group, which revealed that there were less problems of reflux in the patients of narrow gastric tube group; meanwhile, the score of physical function scale in narrow gastric tube group was higher conversely, which suggested that the patients gain a better status in physical function. Nausea and vomiting is the only notable symptom that was worse in whole stomach group at the time of 2 years after surgery, which suggested that patients in whole stomach group suffered more severe nausea and vomiting.
Conclusions:
Narrow gastric tube reconstruction may be a good alternative choice for patients undergoing oncologic esophagectomy in view of better health-related quality of life after the surgery.
Introduction
Esophageal cancer is the sixth most common cause of cancer death. The overall survival after surgery is only 42% and 31% at 5 and 10 years, respectively (1). Esophageal resection is the most established treatment that could offer a cure for patients with esophageal cancer in early stage, but it is associated with high incidence of postoperative complications (i.e. anastomotic leakage, anastomotic stricture, reflux, and cardiopulmonary complication) (2). In such a disease that has a high morbidity and poor prognosis, survival alone may inadequately describe outcome. Researchers have paid more attention to patients’ health-related quality of life (HRQL) (3). The HRQL is generally accepted as an important and relevant outcome measure to assess the result of cancer therapy in patients undergoing oncologic surgery (4).
On the contrary, the standard surgical procedure of esophagectomy for cancer is still in debate. The most frequently used technique is open transthoracic esophagectomy with a 2- or 3-field lymph node dissection, an isoperistaltic gastric tube reconstruction and a hand-sewn end-to-side anastomosis located on the left side of the neck. This procedure of isoperistaltic narrow gastric tube reconstruction (NGT) was proposed by Akiyama et al. (5) in 1972. It is widely applied nowadays and contributes to 79%–90% of all the esophagectomy for cancer worldwide (1). This study is designed to compare the HRQL in patients with gastric tube reconstruction and whole stomach (WS) reconstruction after esophagectomy for cancer.
Material and Methods
Patients’ enrollment
Between September of 2007 and July of 2008, 104 of 112 consecutive patients who underwent surgery for esophageal cancer in our department were included in this prospective study. Eight patients with tumors infiltrating into other organs or distant metastases were excluded. Patients were randomized to receive either NGT reconstruction (n = 52) or WS reconstruction (n = 52). Informed consent was obtained from all patients, and the study was approved by the local ethics committee. Esophagectomy was performed on all patients with localized esophageal cancer.
Surgery
The gastric tube substituting the esophagus was created by serial applications of a linear cutting stapling device, TLC 55 (Ethicon, Stockholm, Sweden). The stapler was fired as many times as needed to divide the stomach from the lesser curvature along the axis of the greater curvature, creating a 3- to 4-cm wide tube. The distance between the incision and pylorus was approximately 5–10 cm, depending on how many times the stapler was fired. The stomach was mobilized and an anastomosis was created between the end of the esophagus and the fundus of the stomach at a distance of 5 cm from the incision of gastric tubularization. A pyloroplasty was done routinely in both groups, without Kocher maneuver. For the patients with tumor located in the upper one-third of the esophagus, a cervical anastomosis was performed; for those with tumor located in the lower two-thirds of esophagus, an intrathoracic anastomosis was created. As there were only five anastomoses performed in neck in this study (two in NGT group and three in WS group), the result of this research should be primarily about patients who have undergone intrathoracic anastomosis.
Irrespective of site of anastomosis, all gastric tubes were placed in the posterior mediastinum. All patients were admitted into the intensive care unit (ICU) after surgery. The same protocol of enteral nutrition or intravenous nutrition is followed. Proton pump inhibitors (PPIs) were used for the first week after surgery in both groups. The adjuvant chemotherapy of docetaxel and cisplatin was provided to all patients.
HRQL assessment
A questionnaire based on the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC-QLQ-C30) and the Oesophagus-Specific Quality of Life Questionnaire 18 (QLQ-OES18) was delivered to patients at 3 weeks, 6 months, 1 year, and 2 years after surgery. The QLQ-C30 contains scales and items addressing functional aspects of HRQL and symptoms that commonly occur in patients with cancer (6). The QLQ-OES18 contains 18 questions (items) in a similar layout and response format to the core questionnaire. It was designed for use in patients with esophageal cancer undergoing surgery, chemotherapy, radiotherapy, and endoscopic treatment. Follow-up questionnaires were delivered to patients’ home by the students in our medical university. At their home, students will oversee whether all data are finished by patients themselves. Students are required to take a photo together with the visited patients to make sure that questionnaires are not fabricated. All patients completed this questionnaire at regular intervals throughout the study.
Randomization
Randomization was performed in the operating room in a blind manner for both the patient and the surgeon, using the sealed envelope technique after patient eligibility was confirmed. The envelopes are not opened until the moment of incision. Patients were randomized to receive either WS reconstruction or NGT reconstruction. This protocol was designed to prevent surgeon-specific selection bias. The method of reconstruction is also blind for the medical and nursing staff in the ICU.
Statistical analyses
Scores derived from the questionnaires were linearly transformed into a 0–100 scale according to the EORTC scoring manual. A higher score in the functional and global HRQL scales represented a higher level of function and better global HRQL, whereas a higher score on symptom scales and items indicated more severe symptoms. All data analyses were performed by using the statistical software SPSS 13.0. Mean scores and standard deviations (SDs) were calculated. The unpaired t-test was used to examine statistical significance at the 5% level for the difference of scores between the two groups. P value of <0.05 was regarded as significant. In addition, the data were also analyzed using nonparametric method, and the results were comparable with the parametric method.
Results
Clinical outcomes
All 104 patients (including 81 males and 23 females) were followed until death or the end of the study period. The follow-up rate was 100%. The average age was 60.1±6.7 years. Table 1 showed the patient characteristics. There were no differences in age, sex, preoperative diet, forced expiratory volume in 1 s (FEV1 (%)), tumor site (7), histopathologic cell type, and tumor, node, metastasis (TNM) pathologic stage (8) between groups.
Patient characteristics.
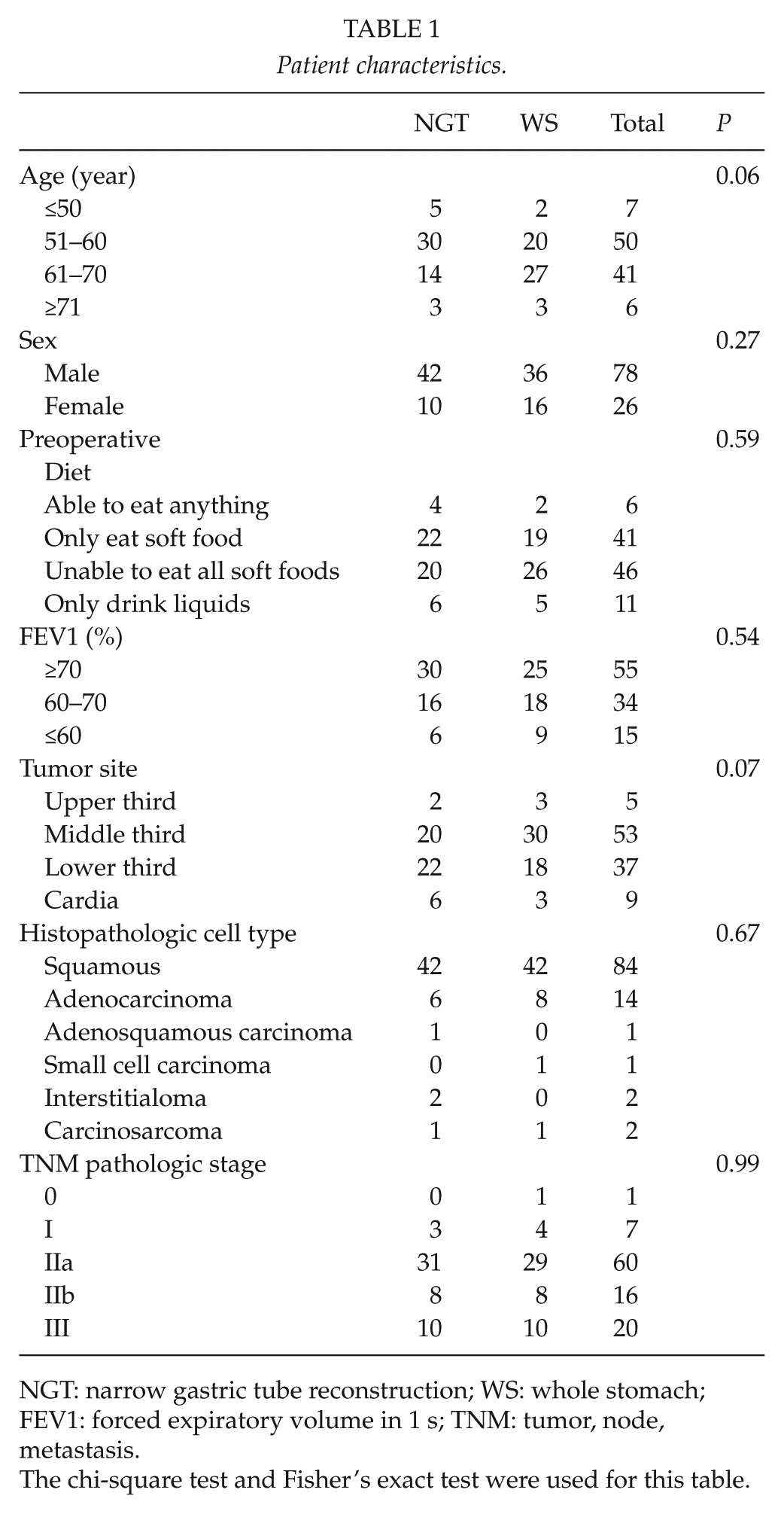
NGT: narrow gastric tube reconstruction; WS: whole stomach; FEV1: forced expiratory volume in 1 s; TNM: tumor, node, metastasis.
The chi-square test and Fisher’s exact test were used for this table.
There is no hospital mortality in NGT group, while two patients died in WS group (Table 2). The postoperative complication rate was 26.9% in NGT group and 48.1% in WS group (P = 0.31, Table 2). The rate of postoperative reflux esophagitis (RE) (9) and cardiopulmonary complication in the WS group was much higher (P < 0.05). During the entire follow-up of 2 years, 44 of the 104 patients died (15 in NGT group and 29 in WS group). Most deaths were caused by tumor recurrence and metastasis, except for one case where the cause of death was traffic accident. The cumulative survival rate at 2 years after surgery was 0.56 in NGT group and 0.44 in WS group (P = 0.14).
Hospital morbidity and mortality after esophagectomy.
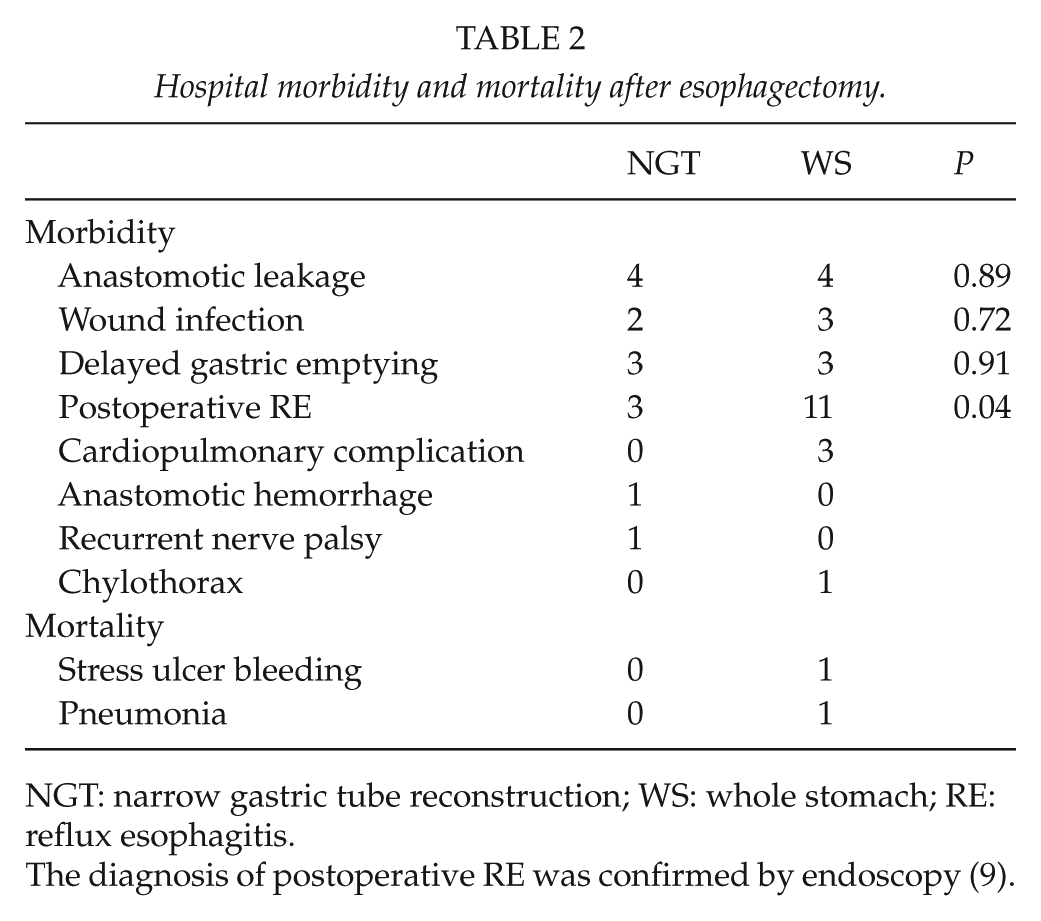
NGT: narrow gastric tube reconstruction; WS: whole stomach; RE: reflux esophagitis.
The diagnosis of postoperative RE was confirmed by endoscopy (9).
HRQL investigation
The response of the HRQL measures was 99.0% in total during the entire follow-up period (208/208 (100%) questionnaires were fed back in NGT group and 204/208 (98.1%) in WS group). Three weeks after surgery, the scores of most scales and items between groups were similar, except for reflux scale and dyspnea symptom item. However, at 6 months after surgery, the scores of physical function scale, eating scale, dysphagia scale, reflux scale, and dyspnea symptom item between the two groups presented statistical differences. Meanwhile, the scores of physical function scale and reflux scale between the two groups also presented statistical differences at 1 year after surgery. Nausea and vomiting is the only notable symptom that was significantly worse in WS group at 2 years after surgery, and the scores of the other scales or single symptoms did not show statistical differences (Fig. 1).
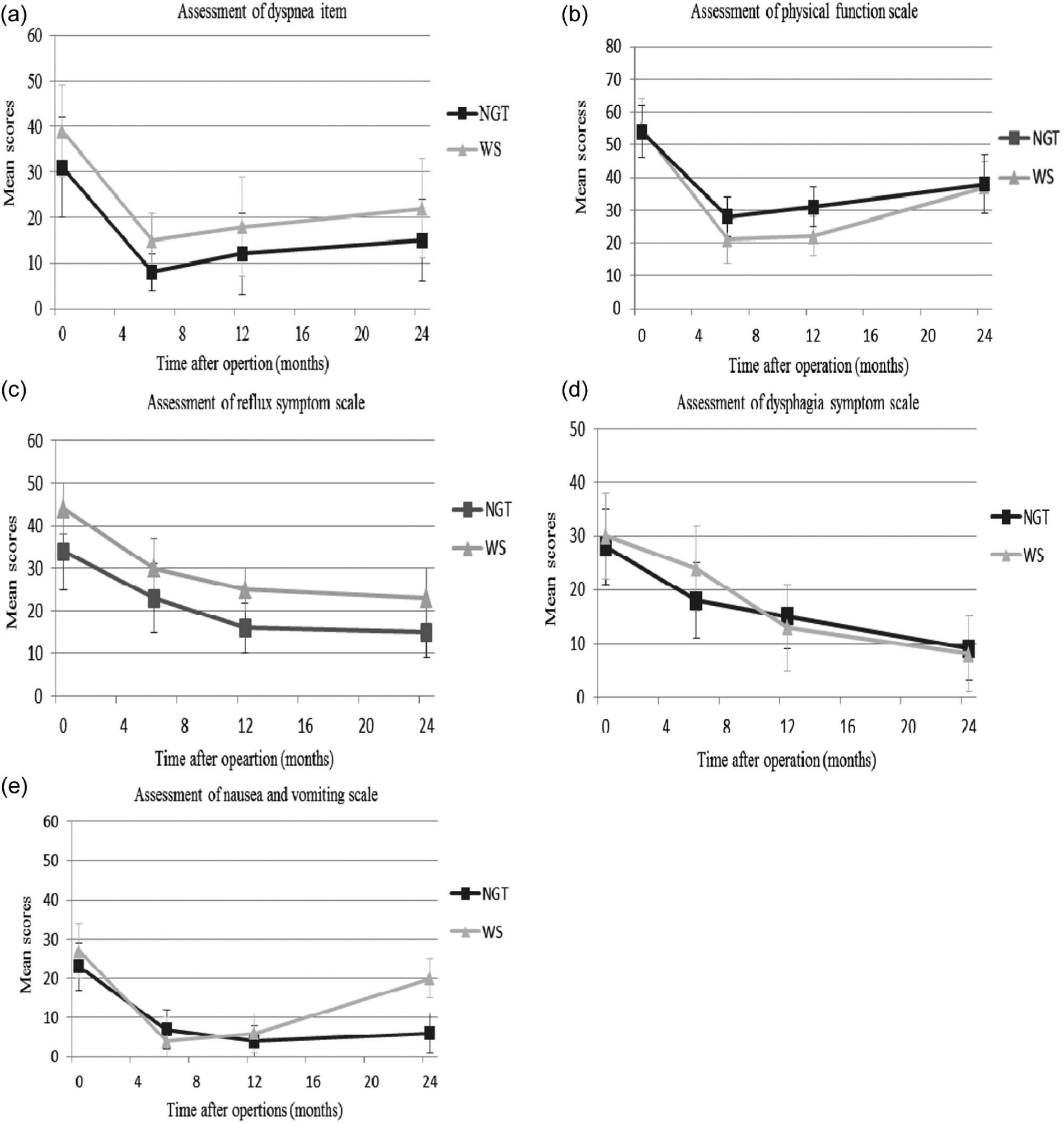
Assessment of A) dyspnea. B) Physical function. C) Reflux. D) Dysphagia. E) Nausea and vomiting between NGT group and WS group. Higher scores represent severe dyspnea, better physical function, severe reflux problem, severe dysphagia problem, and severe nausea and vomiting, respectively.
Discussion
HRQL was always assessed with the validated EORTC core questionnaire, EORTC QLQ-C30 (version 3.0), and with the esophageal site-specific module, EORTC-QLQ-C18. Both have been validated and proved to be useful quality-of-life assessment tools (6). Some studies have prospectively examined HRQL for patients undergoing esophagectomy using these instruments, and they have reported that most aspects of HRQL get worse in the early postoperative period, but this improves with time. These studies had short follow-up (less than 12 months) and methods of reconstruction were not analyzed (10–12). The data from our study are particularly important because they reveal that NGT may be a good alternative choice for patients undergoing oncologic esophagectomy in view of better HRQL after surgery.
Cardiopulmonary complication was distinctly more common in WS group than in NGT group in this study. Consequently, patients in WS group suffered more severe dyspnea during the entire follow-up (Fig. 1). This is in agreement with the conclusion of Viklund (13) that the occurrence of major types of complications, that is, cardiopulmonary complications, is the main predictor of reduced quality of life after esophageal cancer resection. The WS reconstruction theoretically has the disadvantage of compression on the lung and heart by the dilatation of the stomach with air or digestive solution to increase the possibility of cardiopulmonary complications (2, 14). This compression was recorded and measured by clinical symptoms such as chest distress, tachypnea, or dyspnea and changes on electrocardiogram (ECG), which occurs after overeating, and can be eased after fasting or vomiting. Thus, NGT reconstruction may be a better choice for patients with poor respiratory function.
Reflux is a common sequel of esophagectomy with gastric pull-up. It is considered to be caused by a reflux of gastric juices backward into the esophagus because of a defective gastroesophageal sphincter mechanism. Since this sphincter mechanism is destroyed by surgery, RE is an important postoperative complication. In addition, negative intrathoracic pressure and positive intra-abdominal pressure act together to promote reflux across the anastomosis, especially during the early period (15). NGT reconstruction has the advantage of suppressing acid secretion because of the truncal vagotomy and degradation of gastric mucosal blood supply (16, 17), avoiding the functional retention of gastric fluid because of the small residual gastric volume (18). PPIs were also introduced to all patients during the first week after surgery in our hospital because of increased risk for prolonged esophageal exposure to gastric acid and duodenal juice. It was confirmed useful for the treatment of RE as most patients showed endoscopic improvement in the severity of the reflux after treatment (9). However, we do not encourage the long-term use of PPIs because of its negative effect on the digestive system and the relatively lower incidence of RE in Asia (19).
Nausea and vomiting is the only notable symptom that was worse in WS group at 2 years after surgery (Fig. 1). We concluded that it is associated with motor recovery of stomach. The stomach used as an esophageal substitute is disconnected from the extrinsic innervation pathways after truncal vagotomy. Extrinsic denervation of the stomach reduces the postprandial motility index by an average of 62% (20). With time, the amplitude of contractions increases; peristalsis and the three phases of the classic migrating motor complex spontaneously reappear. Such a motor reorganization depends on the myenteric plexus in the gastric wall, which is capable of acting as a local brain that coordinates contractions of muscle fibers. Because most of the myenteric plexus in the gastric wall was preserved in patients of WS group, they presented less symptoms of nausea at 6 months after surgery. Over time, these cells could progressively be deactivated in case of recurrence and metastasis. In NGT group, the recurrence and metastasis of cancer would be less because tubulization of the stomach makes it much easier to skeletonize the lower two-thirds of the lesser curvature for lymph node clearance. Motor recovery is thus more marked in NGT group during follow-up (21).
The significantly better scores on physical function scale for patients in NGT group, especially at 6 months and 1 year after surgery, reflected a quicker postoperative recovery (Fig. 1). This is consistent with the results of Yoichi Tabira et al. (18). On the contrary, this indicated that although with a small residual gastric volume (a reduction of the gastric capacity by one-third on average after tubulization), the gastric tube preserved the physiological function of stomach well and can function as well as the WS reconstruction (22).
Patients in NGT group had a slightly higher cumulative survival rate at 2 years after surgery (0.56 in NGT group and 0.44 in WS group, P = 0.14). Most deaths were caused by tumor recurrence and metastasis. Chen et al. (23) reported that tumor recurrence was reported in about half of the patients during the first 3 years after surgery. The main sites of recurrence were mediastinal lymph node, liver, bone, and lung (23). Recurrence on these sites affects the HRQL. In NGT group, because tubulization of the stomach makes it easier to skeletonize the lower two-thirds of the lesser curvature for lymph node clearance, recurrence and metastasis of cancer would be less. A better survival and HRQL could thus be expected.
The result from this prospectively randomized study indicates that NGT may be a good alternative choice for patients undergoing oncologic esophagectomy in view of better HRQL after surgery.