
Abstract
Background and Aims
A prospective long-term follow-up study of bioactive glass (BAG)-S53P4 and autogenous bone (AB) used as bone graft substitutes for posterolateral spondylodesis in treatment of unstable lumbar spine burst fractures during 1996–1998 was conducted.
Material and Methods
The lumbar fractures were fixed using posterior USS instrumentation. BAG was implanted on the left side of the fusion-bed and AB on the right side. The operative outcome was evaluated on X-rays and CT scans, and a clinical examination was also performed.
Results
The Oswestry score was excellent, and the mean pain score 1. The mean compression rate of the injured vertebral body was 25%. A solid bony fusion was seen on CT scans on the AB side in all patients and on the BAG side in five patients, and a partial fusion in five patients, resulting in a total fusion-rate of 71% of all fused segments in the BAG group.
Conclusions
Our long-term results show that BAG-S54P4 bone graft material is safe to be used as a bone graft extender in spine surgery.
INTRODUCTION
Instrumented posterior spondylodesis with trans-pedicular screw fixation and autogenous bone (AB) grafting is a standard operative procedure in treatment of unstable lumbar spine burst fractures (1 –3). AB harvested from the iliac crest is associated with an increased operation time, increased blood loss and postoperative morbidity. The risk of chronic donor site-related pain also should not be overlooked (4). A need exists for bone substitutes that will prevent the risks observed for the AB harvesting procedure and, ideally, provide a solid fusion. Several bone substitutes, including allograft bone, ceramics, bioactive glasses (BAGs) and demineralized bone matrix, have, therefore, been used to achieve a posterolateral fusion (5 –8).
BAGs are osteoconductive bone substitutes with unique biochemical characteristics. They form a chemical bond with hydroxyapatite, the natural bone inorganic salt, and provide a scaffold for new bone formation (9 –11). Composition of the glass, granule size and granule roughness are all important factors contributing to the cell and extracellular tissue reactions observed for BAGs (12). Over time, the BAG granules dissolve and are replaced by new bone.
BAG-S53P4 (53% SiO2, 23% Na2O, 20% CaO, 4% P2O5) is an osteostimulative, osteoconductive and antibacterial bone substitute (13). BAG-S53P4 was developed at the Åbo Akademi University, Turku, Finland. Pioneer clinical studies developing BAG for clinical use has been performed at the University of Turku and at Turku University Hospital. BAG-S53P4 gained European approval for orthopaedic use as a bone graft substitute in 2006. It has been used in craniomaxillary surgery and in several orthopaedic applications, such as in bone tumour surgery (14), but it has not been studied in the field of clinical spinal surgery.
The aim of this prospective 10-year study was to report the clinical and radiological findings in patients with unstable lumbar spine fractures treated with BAG-S53P4 and AB as bone graft substitutes.
PATIENTS AND METHODS
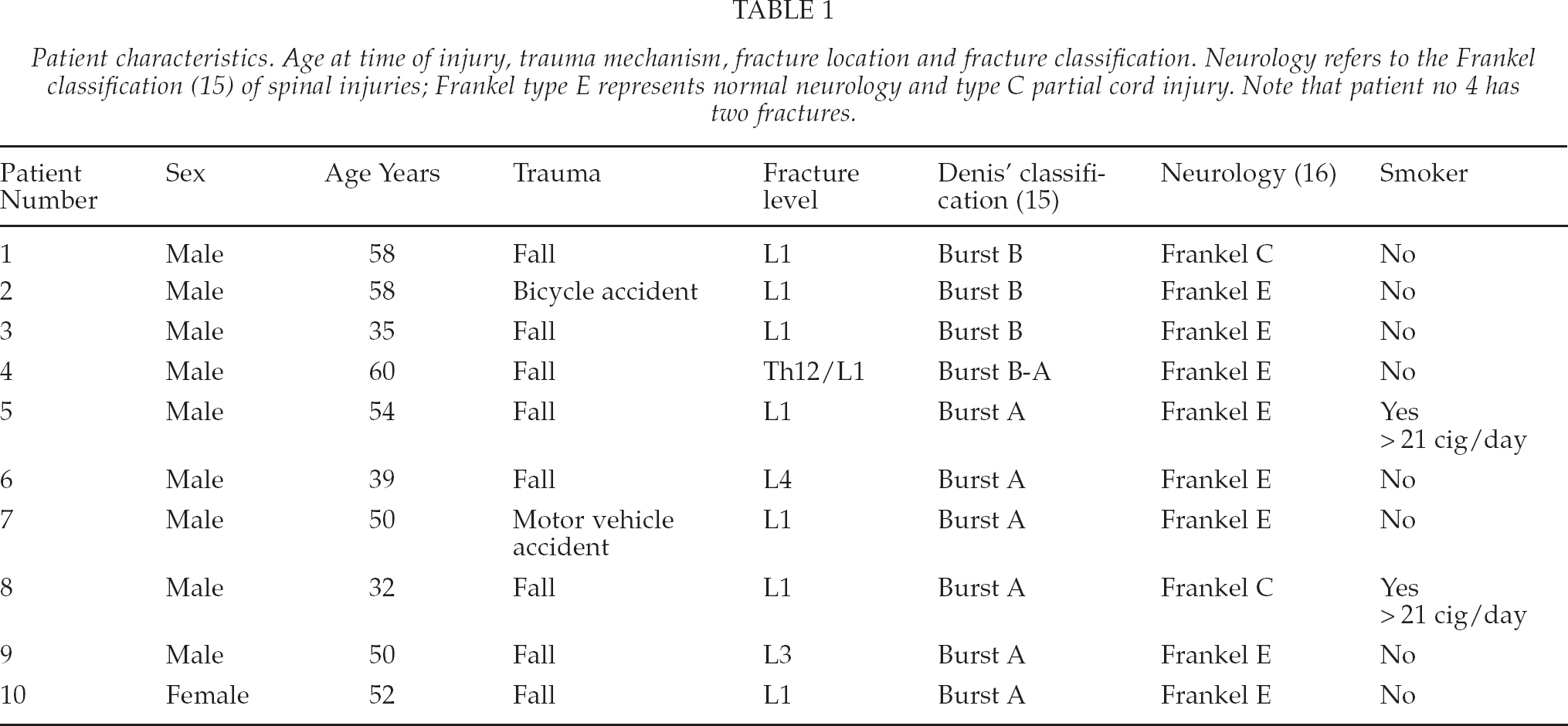
Sixteen patients aged 31–58 (mean 49, SD 10) years with an unstable lumbar burst fracture (one patient had sustained two fractures), classified according to Denis' classification (15), participated in this prospective study. Two patients had incomplete spinal cord injuries classified as Frankel C (16); the others were neurologically intact. None of the patients had undergone previous spine operations. Two patients were smokers. Age at time of injury, trauma mechanism, fracture location and fracture classification are summarized in Table 1.
Patient characteristics. Age at time of injury, trauma mechanism, fracture location and fracture classification. Neurology refers to the Frankel classification (15) of spinal injuries; Frankel type E represents normal neurology and type C partial cord injury. Note that patient no 4 has two fractures.
All patients were operated on at the Department of Surgery, Turku University Hospital in September 1996 to December 1998 by three senior surgeons (JH, EK and EG). All patients were operated on according to the following guidelines. Patients were lying prone on a straight radiolucent operation table. The lumbar fractures were reduced and fixed using posterior USS® instrumentation with titanium shanz screws (Synthes Finland). The USS® instrumentation was supplemented with posterolateral bone grafts decorticated from the lateral processes and posterior laminae. BAG-S53P4,(Abmin Industries, Turku, Finland which is manufactured today as BonAlive® by BonAlive Biomaterials, Turku, Finland) was implanted on the left side of the posterolateral fusion bed and AB on the right side. The mean amount of implanted BAG-S53P4 was 23 g (10–35 g). AB was harvested from the left posterior iliac crest.
All fractures were treated within 72 h of injury. The mean operation time was 166 min, and the mean blood loss was 1960 ml. Antibiotics, anti-thromboembolic prophylaxis and anti-inflammatory drugs were provided according to routine hospital procedures.
No deep or local wound infections were detected at the thoracolumbar level. One poly-traumatized patient had a wound-healing problem after an anterior cervical fracture plate fixation. The cervical wound infection resolved with systemic antibiotic administration, and oral antibiotics were ceased six months after the operation.
The primary follow-up included visits at the outpatient department at 3, 6 and 12 months postoperatively. The average sick leave was 180 days.
All patients were invited to a long-term follow-up visit approximately 10 years after the primary operation for a clinical and radiographic examination. The clinical examination included documentation of medical history, ongoing medication, smoking and alcohol consumption, possible adverse events, a visual analogue scale (VAS) pain scale (0–10) and the patient subjective satisfaction score graded as excellent, good, fair or poor. A subjective assessment of surgical outcome based on the Oswestry disability questionnaire was also made. The result was graded as 0% to 20% Minimal disability; 21%–40% Moderate disability; 41%–60% Severe disability; 61%–80% Crippled; 81%–100% “Bed bound”.
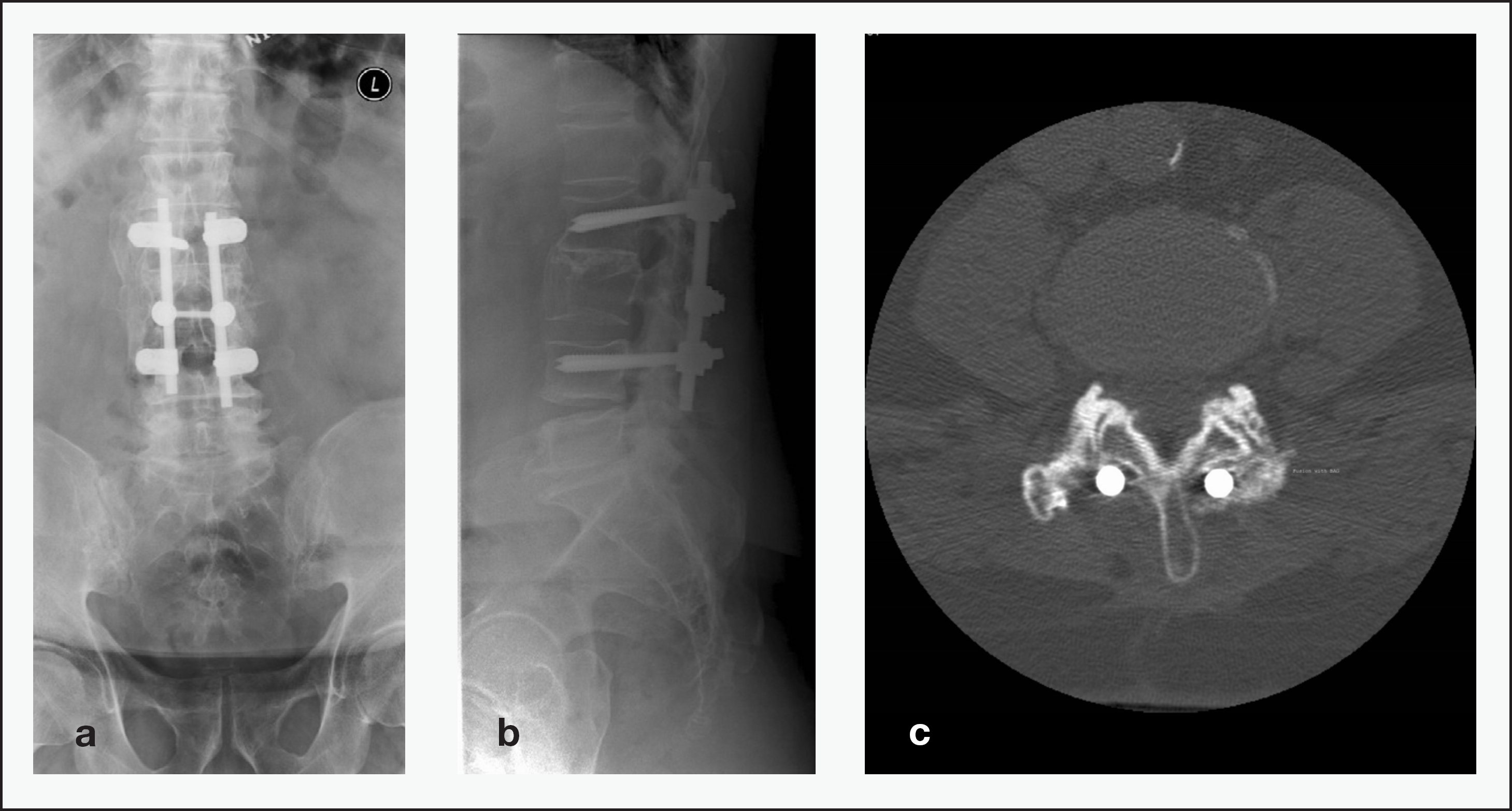
a) Antero-posterior, b) lateral view on X-ray and c) CT scan of instrumented spinal fusion of a L3 burst fracture 10 years postoperatively. Bioactive glass was implanted posterolaterally on the left side and autogenous bone on the right side. Fusion was observed on both sides on levels of L1–2, L2–3 and L3–4.
The imaging protocol included X-rays in flexion, in extension and in a neutral standing position (Philips Bucky Diagnostics C). Sagittal T1- and T2- weighted MRI images in addition to transaxial T2-weighted and coronal short-tau-inversion-recovery (STIR) images (Philips 1.5T Intera Power) and for CT (General Electric HiSpeed Qxi), both the transaxial and the reconstructed coronal and sagittal images were acquired of the lumbar spine. Fusion of the segments was primarily evaluated from the CT scans. The radiological outcome was graded as no = no or incomplete fusion, and yes = complete fusion. Adjacent segment degeneration was assessed from the MRI scans and graded as mild, moderate and severe degeneration. Disks with mild degenerative changes retained height and no Modic I or II endplate changes. Disks with moderate degenerative changes were identified by measurement of the disk height between 4–6 mm or possible Modic I or II endplate changes. Disk height lower than 4 mm and concurrent endplate changes were graded as severe disk degeneration. In addition, all patients older than 50 years at the time of injury underwent bone mineral density assessment of the left hip (DEXA GE Lunar Prodigy Full Size). Radiological data were transferred to clinical workstations (Carestream PACS, GE ADW 4.4) for evaluation and measurements. The radiological imaging was interpreted by a single radiologist (SK).
All parameters were collected on Case Report Forms and transferred to a computerized database for detailed analyses (NL). The study was conducted in accordance with the ethics principles that have their origin in the latest version of the Declaration of Helsinki, applicable regulatory requirements, including the standards of the International Organisation for Standardization, to Finnish law and regulations. The use of BG in a research setting for spinal application as well as the study protocol including the follow-up study was approved by the Ethics Committee of the Hospital District of Southwest Finland. The trial was registered at www.clinicaltrials.gov.
RESULTS
Ten patients (nine men, one woman) participated in the 10-year follow-up. Three patients had died from unrelated causes and three patients did not want to participate for personal reasons. No additional operations or hardware removals had been performed after the primary operation.
Seven patients rated their back as good or excellent and three as fair. The mean Oswestry score was excellent (12, range 0–46). The mean pain score (VAS 0–10) for radicular and back pain was 1 (range 0–4). All patients had returned to their jobs. At the time of the 10-year follow-up, five of the ten patients were retired on the basis of their age, none because of their medical condition.
No persistent problems associated with the bone harvesting area were detected at the 10-year follow-up. However, many patients reported that the local pain at the bone harvesting area lasted longer than the back pain itself.
Normal gait was observed in eight patients. Mild limping but walking without an aid was observed for two patients. Both patients demonstrated preoperative neurological compromise, i.e. partial spinal cord injury or spinal nerve root injury. None of the patients had any subjective deterioration in their walking ability and reported being able to walk more than 1000 m without stopping.
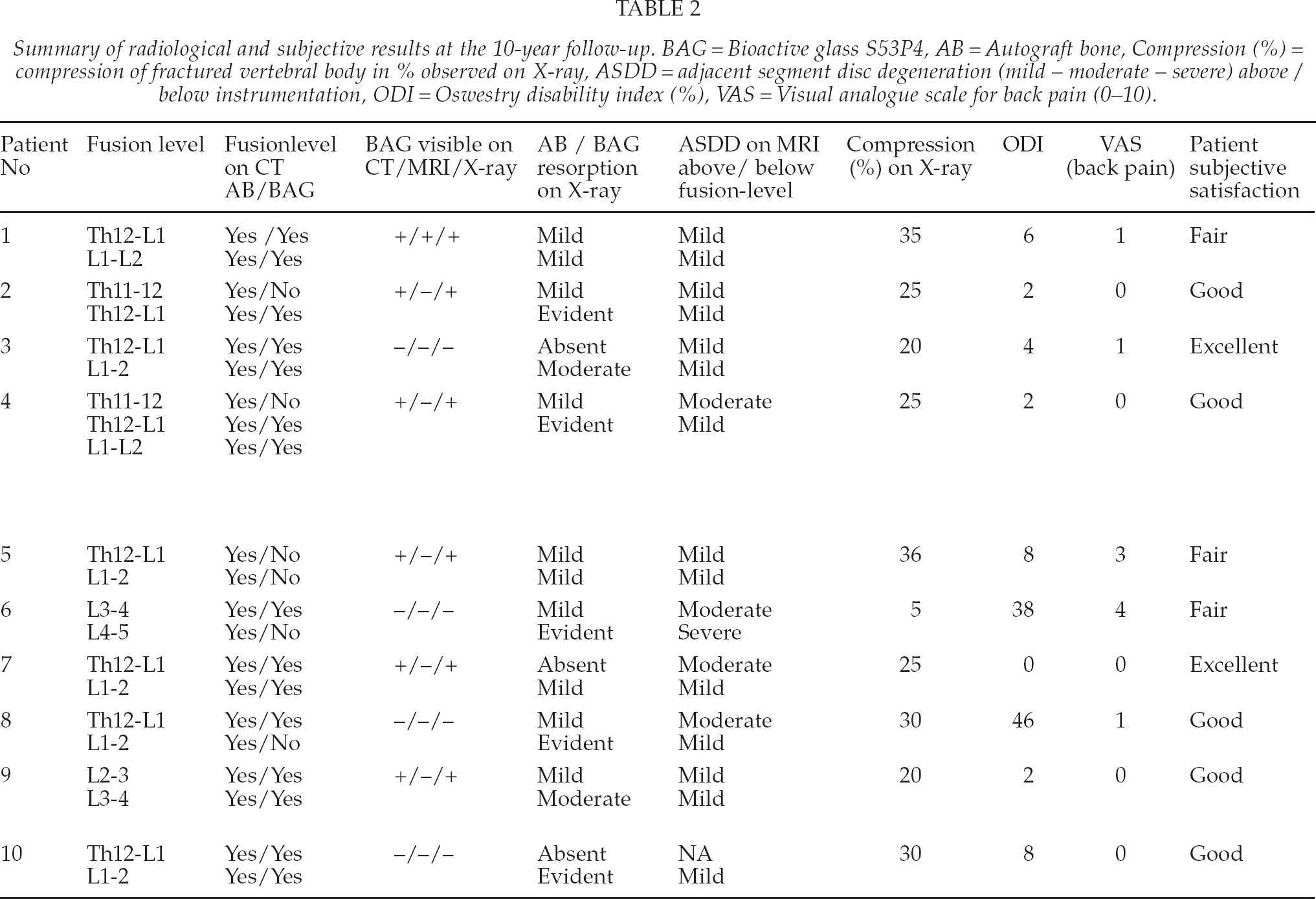
The radiological and subjective data are summarized in Table 2. All fractures had healed. The mean compression rate of the injured vertebral body was 25% (5–36%). The hardware appeared undamaged on X-rays at 12 months. At the long-term follow-up, hardware breakage was observed in one patient in one of the four screws. Despite the screw breakage, a solid bone fusion mass on both sides was noted on CT scans. The screw breakage was asymptomatic. No radiolucent lines or other signs of excessive bone resorption were present around the broken screw.
Summary of radiological and subjective results at the 10-year follow-up. BAG = Bioactive glass S53P4, AB = Autograft bone, Compression (%) = compression of fractured vertebral body in % observed on X-ray, ASDD = adjacent segment disc degeneration (mild — moderate — severe) above / below instrumentation, ODI = Oswestry disability index (%), VAS = Visual analogue scale for back pain (0–10).
A solid bony fusion was seen on CT scans on the side of the AB implantation in all ten patients. Resorption of the implanted graft was mild (N = 7) or absent (N = 3). On the BAG implantation side, a solid fusion on CT scans was seen in five patients and a partial fusion or a discontinuation in the fusion mass in five patients. The fusion mass was more solid on the AB side. On the BAG side a fusion-rate of 71% was achieved (15 segments out of 21 in total). However, in two patients in the BAG group an ectopic fusion was observed above the fusion-site. Resorption of BAG was mild (N = 3), moderate (N = 2) or evident (N = 5). BAG granules were still partially visible in six out of ten patients on CT scans.
No malpositioned Schanz screws were observed. Spinal stenosis was not observed; only limited disk degeneration was present in the adjacent segments. No significant deformities or signs of instability were clinically or radiologically observed. Flexion-extension radiographs demonstrated degenerative spondylolisthesis of 6–10 mm in two patients. These spondylolistheses were not at an adjacent level to the instrumentation and were not associated with clinical or radiological signs of spinal stenosis.
Osteoporosis was demonstrated in two of seven patients who underwent DEXA scanning (patient nos. 1 and 2). Mild osteopenia was a more common finding. Only one patient was associated with a mild osteoporotic single-level vertebral body compression fracture (patient no 1). Two patients were taking medication for osteoporosis.
DISCUSSION
AB with its osteogenic potential, osteoinductive factors and scaffold properties remains the golden standard for graft material used in posterolumbar spinal fusion. The rate of pseudoarthrosis using AB as graft material in spinal fusion has been reported to be 5–43% (6). Advances in instrumentation have diminished the rate to 10–15% (6). In this long-term study, a fusion rate of 100% was observed on the AB side based on CT images.
In an experimental bone healing model, using AB and BAG-S53P4 as bone graft materials for spinal fusion in the rabbit spine, new bone formation between the transverse processes was seen in all cases and solid fusions in 50–75% (17). In this study, BAG-S53P4 was used on one side as a stand-alone bone graft substitute. A solid fusion on CT scans was observed in five patients and a partial fusion in five patients. The subjective outcome was, however, good or excellent in 70% of the patients. This finding is in accordance with previously reported results that unilateral fusion and instrumentation are adequate to achieve successful clinical results. Furthermore, no significant association between radiological appearance of fusion and patients' clinical outcome has been detected (5). Nor has a correlation between radiological fusion observed on CT scans and subjective satisfaction emerged in this long-term follow-up.
CT is a very reliable method to assess bone fusion between the transverse processes. It is also the most sensitive method to determine whether BAG granules are still present in the fusion bed. The fact that some remnants of glass granules were still present in ∼50% of the patients after more than 10 years of follow-up is not surprising. Similar findings have previously been detected in benign bone tumour surgery using BAG-S53P4 as a bone graft substitute. The glass granules have also been observed to be incorporated in cancellous bone that appears more dense than normal bone (14).
BAG (45S5, Bioglass, Novabone) has been compared with AB in spinal fusion surgery of adolescent idiopathic scoliosis, with good results. The loss of correction of the main thoracic curve was slightly less in the BAG group than in the AB group. Blood loss and the complication rate were also significantly lower in the BAG group (18). One reason for the good results in the BAG group may be the operation technique, as local AB was mixed with BAG, i.e. BAG was not used as a stand-alone bone substitute. Good clinical and radiological results using BAG-S53P4 mixed with AB have been observed clinically by the authors in more than twenty patients (unpublished results).
Acharya and co-workers (5) reported a high resorption rate for a hydroxyapatite (HA)-BAG composite (Chitra-HABg) used as a stand-alone graft material in instrumented posterolateral fusion in degenerative spondylolisthesis or stenotic spine, in a similar study design as ours. The BAG composite was inserted in the left intertransverse space and AB in the right intertransverse space. The outcome of the study was excellent on the AB side, whereas 95% of the BAG composite cases showed a poor consolidation. Despite the radiological finding showing composite graft resorption, the clinical outcome (Oswestry index) was good in 16 out of 22 patients. One reason for the poor radiological results in the HA-BAG composite group may be the composition of the graft material. Chitra-HABg contains 80% HA and 20% of a BAG (sol-gel derived silica gel). HA is known to be relatively inert, showing poor biodegradation, which may hinder bone remodelling. Bone formation and the healing process have been observed to be faster using S53P4 than HA granules (19). The relative composition of the BAG in Chitra-HABg is unknown. The solubility of the glass is dependent of the composition of the glass, which also affects the bone forming process (20).
Other ceramic and ceramic composite materials have also been used in spinal fusion surgery. HA and β-tricalcium phosphate granules mixed with morselized AB have shown good results (6, 21). Local AB mixed with an apatite- and wollastonite-containing glass ceramic resulted in an 80% fusionrate for two-level spinal fusion in the absence of any spinal instrumentation (22). Calcium sulphate used as an extender with local AB compared with autologous iliac bone graft has yielded comparable results for two-level fusion (83–86%) and fusion size (8).
Allograft bone is highly osteoconductive, but its osteoinductive capacity is weak and it lacks osteogenic capacity (23). Concern also exists about possible spread of viral transmission diseases caused by, for instance, human immunodeficiency virus, hepatitis virus and feline leukemia virus. Furthermore, the production processes, including freezing, freeze-drying or sterilization of allograft bone, reduce the osteoinductive and osteoconductive capacity of the graft material. Use of allograft bone in posterolateral fusion can, therefore, be questioned.
One of the most common and potentially devastating long-term complications after spinal fusion is adjacent segment disease with significant junctional spinal stenosis (24). Increasing age and length of procedures are known risk factors for adjacent segment disease. The majority of the patients in our study were older than 50 years at the time of injury. However, only two motion segments were fused in most of the cases. This may be the most important reason for adjacent level degeneration not being a major problem in trauma patients after two- or three-level fusion at the 10-year follow-up.
Hip and wrist fractures are known to be associated with a high risk of other osteoporotic fractures (25, 26). The incidence of refractures (osteoporotic compression fractures) in the spinal column in this population was low, although osteoporosis was detected in two patients. This suggests that the risk of a new fracture is not drastically increased after a “high”-energy spinal column injury.
This report is the first long-term observation study on BAG-S53P4 as a bone graft material in posterolateral spondylodesis to treat unstable lumbar spine fractures of patients undergoing operative management. BAG-S53P4 used as bone graft material in spinal fusion seems to be a safe procedure, associated with a very low long-term complication rate. However, BAG-S53P4 used as a stand-alone bone substitute resulted in a solid fusion in only five of ten patients and cannot therefore, be regarded as efficient as AB in promoting solid fusion.
Our long-term results show that BAG-S54P4 bone graft material is safe to be used as a bone graft extender in spine surgery. The use of BAG as a bone graft extender and its efficacy to promote fusion as compared to other biomaterials used in spine surgery needs to be investigated in future studies.