
Abstract
Keywords
Over the past decades, there have been growing concerns about high-risk consumption of alcohol among adolescents, and several studies have linked early alcohol use and drunkenness to various consequences, including risky sexual behaviours, arguments, fights, accidents and health problems (Arata et al., 2003; Danielsson et al., 2010; ESPAD Group, 2016a; Hingson & Zha, 2009; Kuntsche et al., 2013). At present, alcohol is the leading risk factor for premature mortality and disability-adjusted life years (DALYs) among individuals aged 15–24 years globally (ESPAD Group, 2016a). Consequently, public health researchers and policymakers have followed adolescent alcohol consumption with intensified interest (Bye & Rossow, 2010; ESPAD Group, 2020). Recently, adolescent substance use has also become a global health priority, as declared in the World Health Organization's (WHO) ‘global strategy to reduce harmful use of alcohol’ (Møller et al., 2019).
Despite the concern, several recent studies have documented a generally decreasing trend in alcohol consumption among European adolescents since the year 2000 (De Looze et al., 2019; Kraus et al., 2015). Indeed, in the Nordic countries of Finland, Iceland, Norway and Sweden, substantial reductions in the prevalence of lifetime alcohol use of approximately 15 percentage points have been observed between 1995 and 2015, with Denmark lagging somewhat behind (ESPAD Group, 2016a; Raitasalo et al., 2021). This decline continued between 2015 and 2019 in Finland, Norway and Sweden, and stagnated in Iceland, whereas the prevalence of lifetime alcohol use remained at a higher level in Denmark (ESPAD Group, 2020).
The decline in youth drinking is not only apparent in European and Nordic countries, it has also been found in other western countries (Pape et al., 2018; Raitasalo et al., 2021; Raninen et al., 2022; Vashishtha et al., 2020). Several hypotheses have been proposed to explain the emergence of this decline and have been tested empirically. These include that the decline is a result of the digital age, stricter parenting or new attitudes towards school, health and substances (Pape et al., 2018; Raitasalo et al., 2021). However, many questions remain unanswered.
Whereas discussions over the cause of the decline in youth drinking continue, other research has begun to investigate the implications of the decline in youth drinking and to ask whether alcohol-related consequences have declined in concert with the decline in consumption. There are many approaches to conceptualising and assessing alcohol-related consequences. Generally, these outcomes can be divided into acute or long-term consequences. For adolescents, looking at acute consequences in terms of, for example, intoxication, violence, criminality, injuries, conflicts with family, friends or school, etc. may be more relevant than long-term consequences, such as alcoholic liver cirrhosis and alcoholic cardiomyopathy, which take years of heavy consumption to manifest. Several studies have documented that, for the most part, acute alcohol-related consequences have indeed declined along with decreasing consumption among adolescents (Bye & Rossow, 2010; Møller et al., 2019; O’Donnell et al., 2017; Svensson & Landberg, 2013; Thor et al., 2017; Trefan et al., 2019). For example, decreasing trends in alcohol-related hospital emergency (Trefan et al., 2019) and injury admissions (O’Donnell et al., 2017) have been reported in past decades among adolescents in Wales and England. In addition, Thor and colleagues (Thor et al., 2017) have demonstrated decreasing trends since 2019 among Swedish adolescents regarding self-reported alcohol-related consequences, including problems with parents or teachers, victimisation by robbery or theft, and trouble with the police. However, more research is needed to determine whether the decline in alcohol-related consequences is a result solely of a decline in the number of drinkers in the population (non-drinkers are, by definition, not at risk of alcohol-related consequences), or whether there is also a decline in alcohol-related consequences among drinkers.
Current research has begun to focus on whether the association between consumption and alcohol-related consequences has remained constant, even while population-level consumption declines. The “normalisation/denormalisation” hypothesis suggests that because youth drinking is declining in general, heavy drinking in adolescence has become a rarer and more extreme (denormalised) behaviour among a more deviant and risk-prone group of young people (Moan et al., 2021). This, in turn, strengthens the association between heavy drinking and alcohol-related consequences (Moan et al., 2021; Pape et al., 2018; Thor et al., 2017). Thor and colleagues (Thor et al., 2017) did not find support for the (de)normalisation theory of a stronger association between consumption and related consequences during periods of low consumption. Nor did they find a weaker association in periods of a higher prevalence of consumption in their study of Swedish adolescents between 1995 and 2012. However, more recently, Moan and colleagues (2021) did find partial support for the strengthening of the association between heavy episodic drinking (HED) and alcohol-related violence among Norwegian and Icelandic youth, but not among Swedish youth.
Moreover, it is not clear whether a decline in alcohol-related consequences can be attributed solely to the decrease in adolescents’ drinking. That is, other factors may also play a role. Today's youth have been characterised by researchers and commentators as “Generation Sensible” (Holmes et al., 2022) so that, in addition to a decline in alcohol consumption, decreases have also been found for other risk behaviours, such as smoking, sexual activity and criminality (Lewycka et al., 2018; Svensson & Oberwittler, 2021). It could therefore be suggested that the driving mechanisms behind the decline in alcohol-related consequences may not be solely a decline in alcohol consumption, but could also possibly be part of a wider societal trend of decreasing engagement in risk-seeking behaviour among youth.
The aims of the present study were as follows: (1) to investigate whether self-reported acute alcohol-related consequences among adolescents in the Nordic countries have declined in concert with the decline in alcohol consumption between 2007 and 2015; (2) to investigate the strength of the relationship between alcohol consumption and self-reported acute alcohol-related consequences over the study period; and (3) to investigate whether the decline in self-reported acute alcohol-related consequences can be attributed to the decline in alcohol consumption.
Method
Data
Data for the present study are from the European School Project on Alcohol and Other Drugs (ESPAD). The project is a collaborative effort of independent research teams in 35 European countries with the overall aim to collect repeated comparable cross-sectional data on substance use among students in Europe aged 15–16 years (www.espad.org). The data collection began with the first wave in 1995; subsequent survey waves have been conducted every 4 years (i.e., 1999, 2003, 2007, 2011, 2015 and 2019).
The target population of ESPAD is defined as students enrolled in regular, vocational or academic studies who turned 16 years old in the calendar year of the specific survey year and were present in the classroom on the day that the survey was conducted. In all countries, the students completed the self-administered questionnaire anonymously in a classroom setting. The data collection methods are largely comparable across countries, although slight deviations may have occurred in relation to time of data collection (http://www.espad.org/reports-documents).
In the present study, data from Denmark, Finland, Iceland, Norway and Sweden are used from the survey waves in 2007, 2011 and 2015. The number of respondents in each of the three waves varied between 877 and 4,988 across countries. In all survey waves, data were collected by paper-and-pencil self-administered questionnaires. Data from the other survey waves (including 2019) were not included in the present study due do comparability issues for the relevant questions (e.g., different reference periods, question formulations and response categories). In each wave, all five countries followed their respective data protection legislation when gathering the data. Detailed information on the design and methodology, as well as on legal and ethical approvals, is provided in detail elsewhere (ESPAD Group, 2016b; Hibell et al., 2009, 2012).
Measures
Alcohol consumption
Students who reported drinking at least once during the last 12 months were considered current drinkers. The frequency of alcohol use in the last 12 months was assessed by the following question: “On how many occasions (if any) have you had any alcoholic beverage to drink during the last 12 months?” The response categories were: “0”, “1–2”, “3–5”, “6–9”, “10–19”, “20–39” and “40 or more” occasions. Also included was a question on HED, i.e., consuming at least five standard drinks (equal to 12 g of pure alcohol in all five countries) on one occasion within the last 30 days (response categories: “yes” vs. “no”). However, in the Finnish questionnaire, HED was defined as at least six standard drinks on one occasion. The variable volume of pure alcohol at the last drinking occasion was assessed by the following five beverage-specific questions: “If you drank beer/wine/spirits/alcopops/cider on the last day that last day you drank any alcohol, how much did you drink?” The response categories for beer, alcopops and cider were: “I never drink beer/alcopops/cider”, “I did not drink beer/alcopops/cider on the last day that I drank alcohol” (0 cL), “<50 cL”, “50–100 cL”, “101–200 cL” and “>200 cL”. The response categories for wine were: “I never drink wine”, “I did not drink wine on the last day that I drank alcohol”, “<20 cL”, “20–40 cL”, “41–74 cL” and “>74 cL”. For spirits, the response categories were: “I never drink spirits”, “I did not drink spirits on the last day that I drank alcohol”, “<8 cL”, “8–15 cL”, “16–24 cL” and “>24 cL”. The volume of pure alcohol at the last drinking occasion was calculated as the sum of all alcohol consumed (midpoint values of centilitres and converted to centilitres of pure alcohol).
Self-reported acute alcohol-related consequences
Variables on self-reported acute alcohol-related consequences were derived from a checklist of various situations that could occur under the influence of alcohol. The checklist included 10 situations in 2007 and 2011, and 14 situations in 2015. In 2007 and 2011, the question on alcohol-related consequences was: “Because of your own alcohol use, how often during the last 12 months have you experienced the following?” In 2015, the question was revised slightly: “While under the influence of alcohol, how often during the last 12 months have you experienced the following? 1 ” Three alcohol-related consequences were selected for the present study because questions on these consequence items were asked the most similarly in all three survey waves. For the purposes of this research, we shall call these items “Self-reported acute alcohol-related consequences”. They are: (1) accident or injury; (2) victimised by robbery or theft; and (3) trouble with the police. The response categories were as follows: “0 times”, “1–2 times”, “3–5 times”, “6–9 times”, “10–19 times”, “20–39 times” and “40 times or more”. Answers were dichotomised as “yes, at least once” versus “no”. These responses were then summed into an index, the result of which was then again dichotomised into at least one alcohol-related consequence reported by the respondent versus none. For more detailed information on the questions and response categories in the 2007, 2011 and 2015 survey waves, please see http://www.espad.org/reports-documents.
Statistical analyses
Descriptive statistics (percentages and means) for each country and study year were calculated to describe the main variables of the study samples. These results are also presented for all countries combined. The analyses were conducted by drinking status: all students; current drinkers; and students who had engaged in HED within the last 30 days, respectively. The Cochran–Armitage trend test was applied to examine trends in categorical alcohol use indicators over time, and the Jonckheere–Terpstra test was used to determine presence of trends in volume of pure alcohol at the last drinking occasion.
Multiple logistic regression models (adjusted for gender) were used to examine the association between HED within the last 30 days and having experienced at least one self-reported acute alcohol-related consequence among current drinkers during the last 12 months in 2007, 2011 and 2015, respectively. Logistic regression models were also used to examine the association between survey year and having experienced at least one self-reported acute alcohol-related consequence in the last 12 months among current drinkers. In these regressions, model 1 displayed crude associations, model 2 was further adjusted for gender and HED within the last 30 days, model 3 was further adjusted for consumed alcohol volume on the last drinking occasion and model 4 was further adjusted for frequency of alcohol intake. Results are presented as odds ratios (OR) with 95% confidence intervals (CI) for each country and the total combined dataset, adjusted for country. All reported p-values were two-sided. Data were analysed using SAS version 9.4.
Results
Table 1 describes the survey data by country and survey year. It is noticeable that the number of respondents is substantially lower in Denmark than in the other four countries for all three survey waves. The overall number of respondents in the Nordic countries decreased from 16,036 students in 2007 to 13,517 students in 2015. The school participation rate varied across countries; in all waves, the rate was markedly lower in Denmark and Norway than in the other three Nordic countries.
Description of study sales by country (2007–2015).
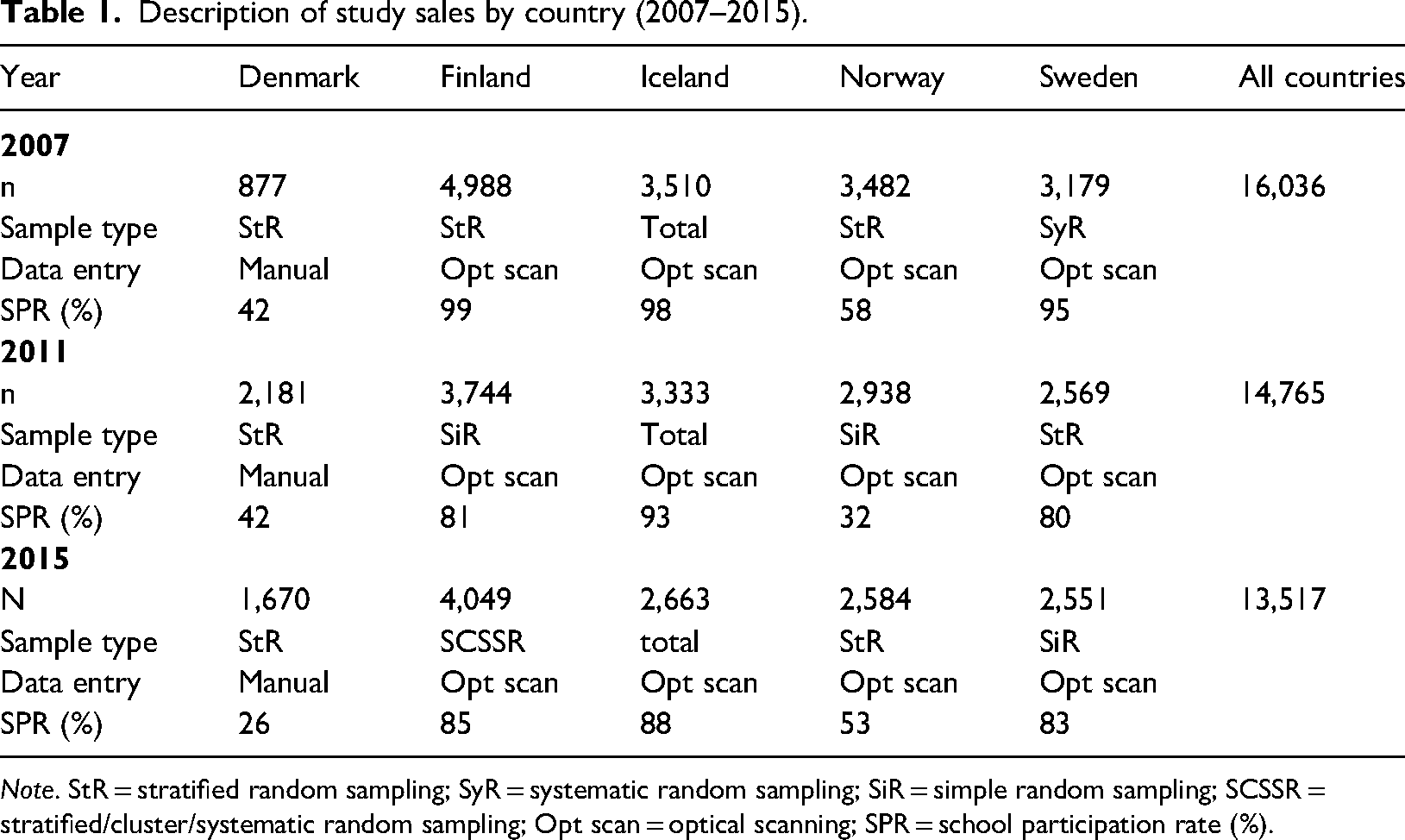
Note. StR = stratified random sampling; SyR = systematic random sampling; SiR = simple random sampling; SCSSR = stratified/cluster/systematic random sampling; Opt scan = optical scanning; SPR = school participation rate (%).
The prevalence of current drinking and HED in the last 30 days was substantially higher in Denmark than in the other Nordic countries (Table 2). The prevalence estimates for both indicators declined from 2007 to 2015 in all Nordic countries (Table 2), most markedly in Iceland, Norway and Sweden, and only modestly and without statistical significance (p-value for trend: .1951) in Denmark. The volume of pure alcohol consumed on last drinking occasion declined in Iceland, Norway and Sweden between 2007 and 2015 (all p-values for trend: < .0001) but increased in Denmark and Finland between 2007 and 2011, and remained at the same level in Denmark in 2015 but fell again in Finland.
Trends in alcohol use by country (2007–2015) among all students (percentages and means).
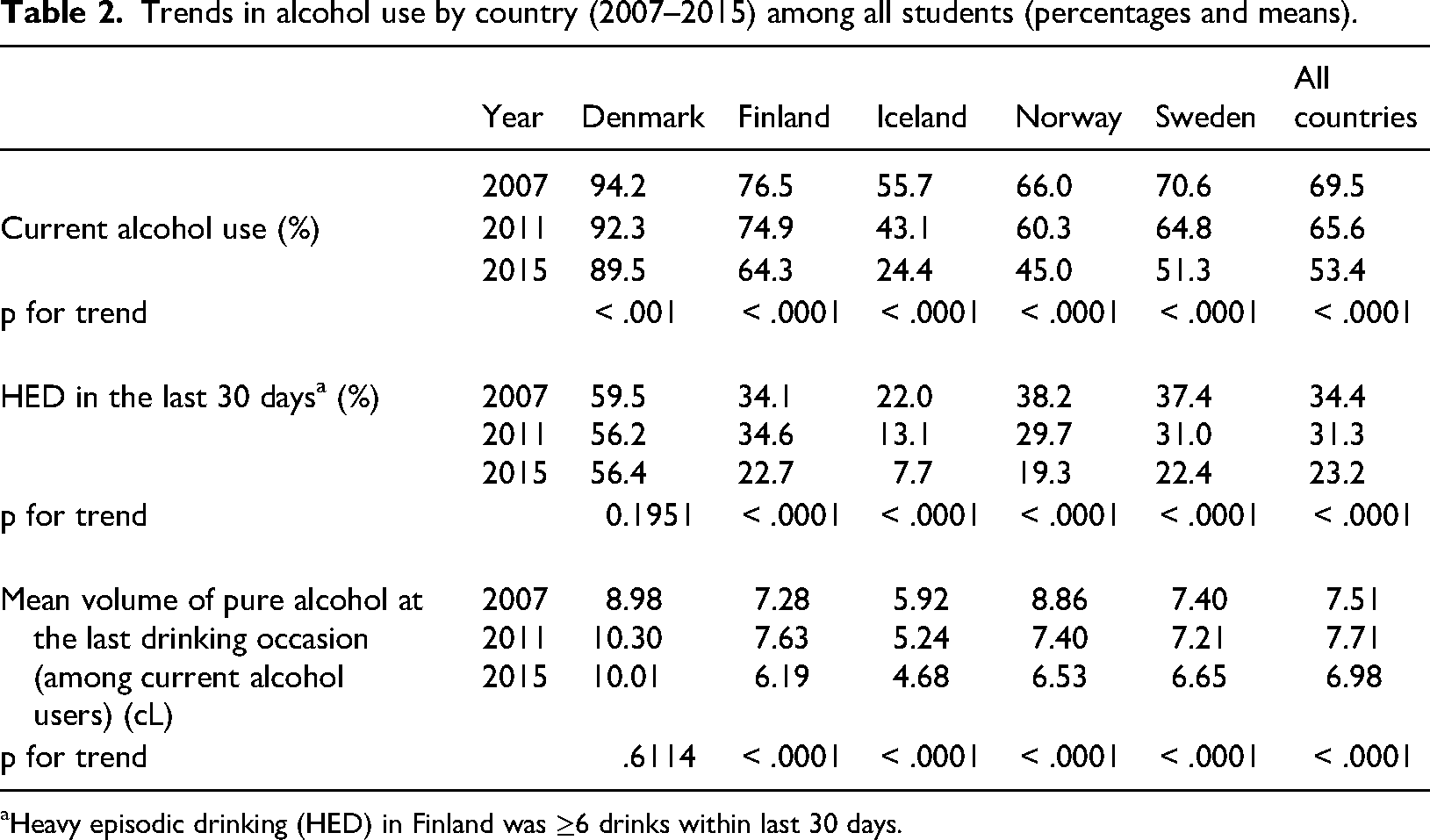
Heavy episodic drinking (HED) in Finland was ≥6 drinks within last 30 days.
Figures 1 to 3 display the prevalence of students who reported experiencing at least one of three acute alcohol-related consequences by drinking variable. When the entire student population (drinkers as well as non-drinkers) was considered to be the denominator (Figure 1), the overall prevalence of experiencing at least one consequence in the Nordic countries (combined) declined from 17.6% in 2007 to 10.4% in 2015 (p for trend: < .0001). The decline was marked in Iceland, Norway and Sweden, where a consistent fall in current drinkers, HED and volume of drinking has been observed. In Denmark, where only a modest decline in the prevalence of current drinkers and HED was observed (p for trend: .0240), the prevalence of experiencing at least one acute alcohol-related consequence increased from 12.2% in 2011 to 14.8% in 2015. In Finland the prevalence of experiencing at least one acute alcohol-related consequence was highest in 2011 (20.5%). The prevalence of reporting at least one consequence increased in all countries as the denominator changed from the entire population (Figure 1) to only current drinkers (students who consumed alcohol in the last 12 months) (Figure 2). Here the prevalence of experiencing at least one acute alcohol consequence declined in Norway and Iceland, but in Sweden the prevalence was relatively constant at approximately 19%–20% in all years, and in Finland the highest prevalence was still seen in 2011 (27.0%). When pooled together, a decline is observed in all countries (p for trend: < .0001).
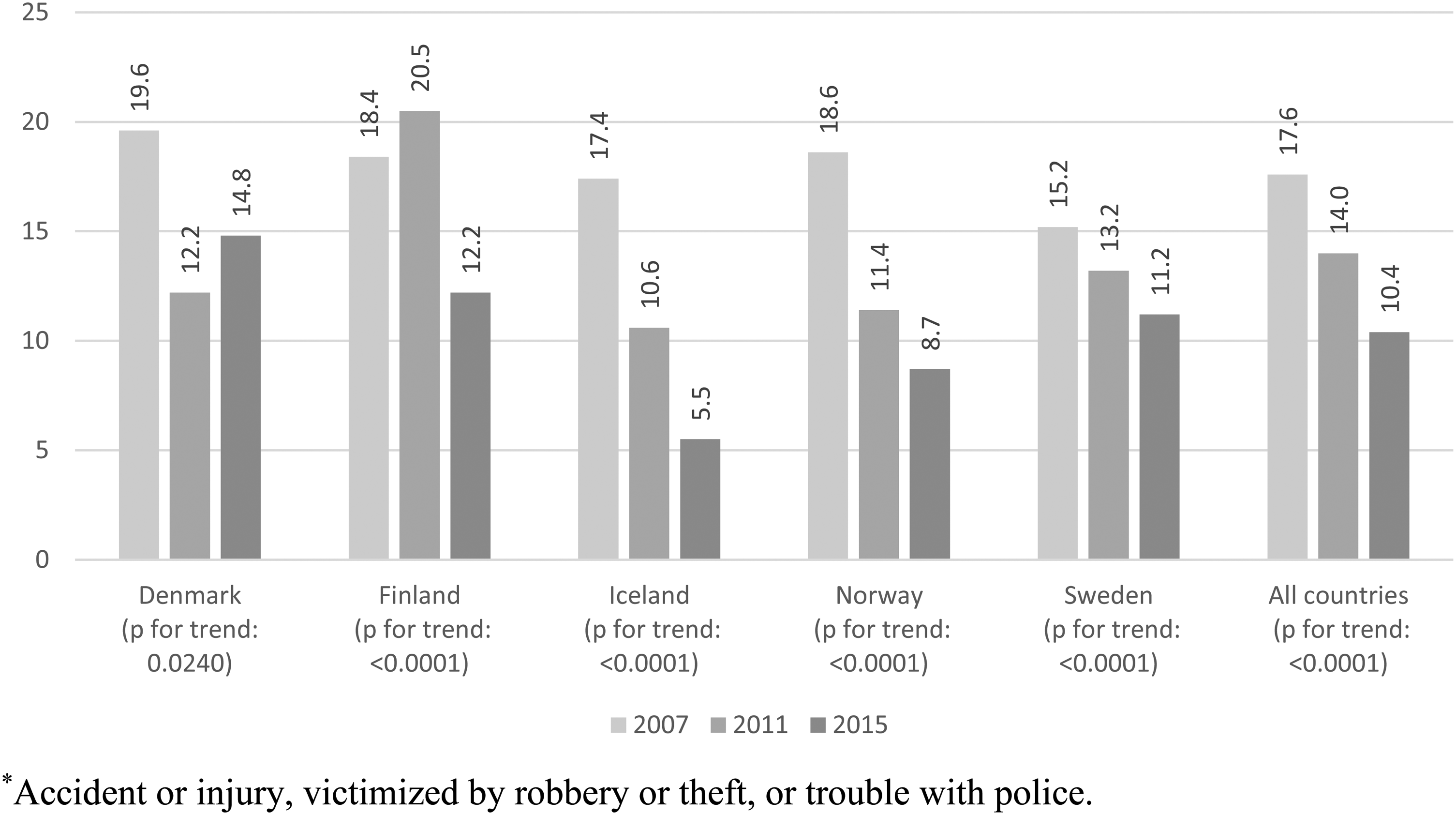
Prevalence of experiencing at least one self-reported acute alcohol-related consequence* among all students, during the last 12 months (2007–2015), percentages. *Accident or injury, victimised by robbery or theft, or trouble with police.
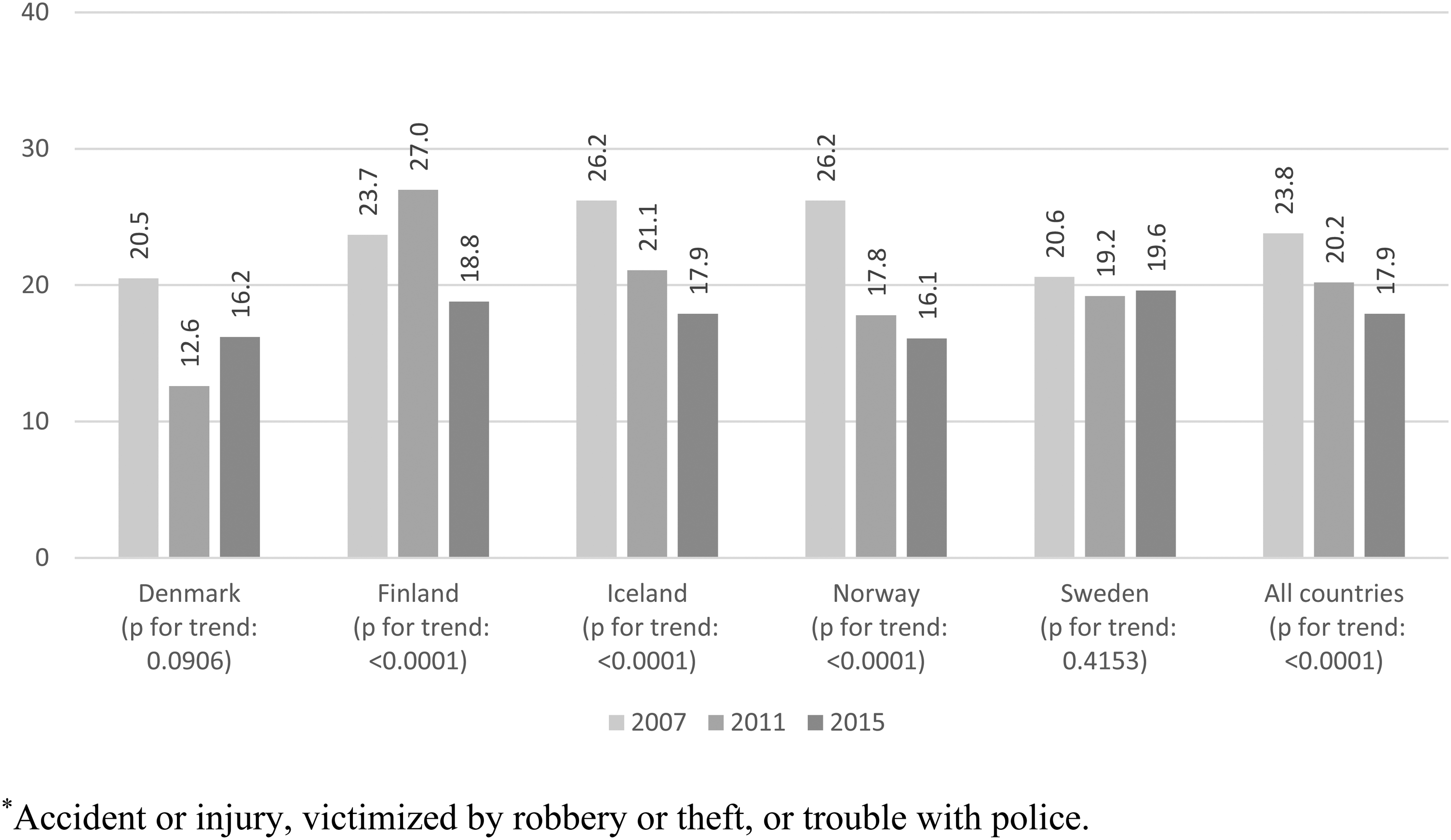
Prevalence of experiencing at least one self-reported acute alcohol-related consequence* among current drinkers, during the last 12 months (2007–2015), percentages. *Accident or injury, victimised by robbery or theft, or trouble with police.
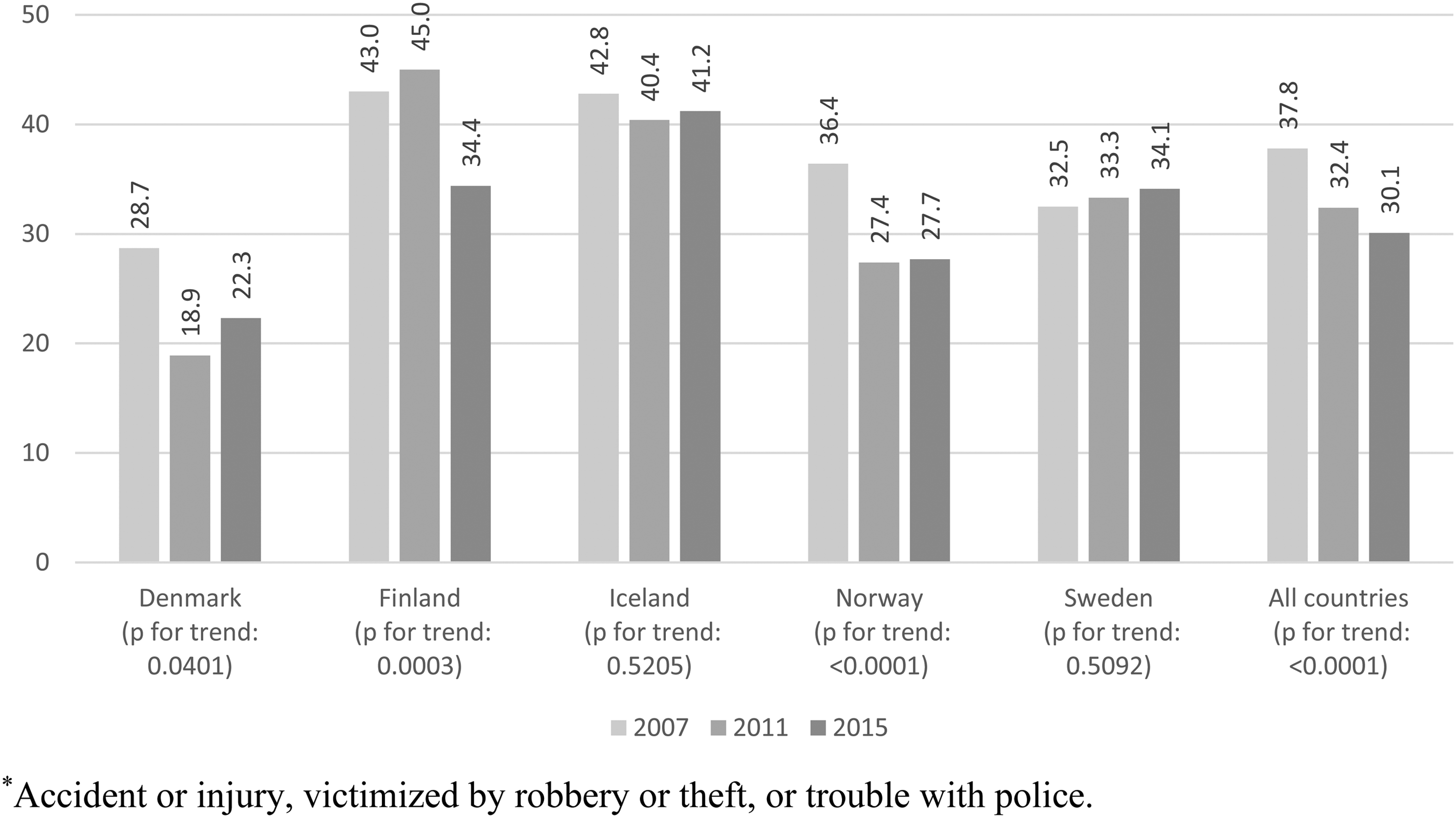
Prevalence of experiencing at least one self-reported acute alcohol-related consequence*, among heavy episodic drinkers within the last 30 days, during the last 12 months (2007–2015), percentages. *Accident or injury, victimised by robbery or theft, or trouble with police.
When the denominator was changed to those who had reported HED within the last 30 days, the prevalence of reporting at least one acute alcohol-related consequence increased further, especially in Iceland, where the prevalence of HED also dropped dramatically and is at a much lower level than the rest of the Nordic countries in all years (Figure 3). On the other hand, the change of denominator from current drinkers to heavy drinkers only modestly increased the prevalence of experiencing acute alcohol-related consequences in Denmark, where more than half of the population in all years engaged in HED. The prevalence of experiencing at least one alcohol-related consequence among those who reported HED was also relatively high in Finland in all years, although the prevalence of HED was at the same level as in Sweden and Norway in all years. A decrease in the prevalence of acute alcohol-related consequence over the years, when HED was the denominator, was only seen when all countries were combined (p for trend: < .0001). In Iceland and Sweden, the prevalence was relatively constant over the years (at approximately 41% and 33%, respectively); in Denmark and Finland, the same pattern were seen as in Figures 1 and 2; and in Norway, a sharp decline from 36.4% in 2007 to 27.4% in 2011 and 27.7% in 2015 was observed (p for trend: < .0001). Sensitivity analyses of the three individual acute alcohol-related consequences showed similar results (presented in Supplementary Table S1).
Table 3 shows the results of multiple logistic regression that examined the association between HED within the last 30 days and self-reported acute alcohol-related consequences in 2007, 2011 and 2015. This analysis was undertaken to determine whether there was an increase in the magnitude of this association over time. There was no strong tendency towards a strengthening of the association between 2007 and 2015 across the Nordic countries, except in Iceland, where alcohol consumption also declined most markedly from an OR of 4.13 (95% CI = 3.33–5.13) in 2007 to an OR of 9.00 (95% CI = 5.73–14.14) in 2015. In Norway and Sweden, the strength of association was relatively similar between 2007 and 2015. In Finland, the strength of association decreased from an OR of 8.64 (95% CI = 7.18–10.40) in 2007 to an OR of 5.20 (95% CI = 4.19–6.45) in 2015. In Denmark, the association was strongest in 2011 (OR = 8.68, 95% CI = 5.44–13.86).
Results from multiple logistic regression models showing the association between HED within the last 30 days and having experienced at least one self-reported acute alcohol-related consequence a during the last 12 months in 2007, 2011 and 2015.

Note. Gender-adjusted odds ratios (OR) with 95% confidence intervals (CI).
Accident or injury, victimised by robbery or theft, trouble with police.
Multiple logistic regression was employed to study the relationship between the decline in self-reported acute alcohol-related consequences between 2007 and 2015, while adjusting stepwise for each alcohol consumption variable (Table 4). The decreasing value in the ORs varied from country to country. Model 1 showed the crude results of the association of survey year to self-reported acute alcohol-related consequences without gender or alcohol variables. Except for Finland in 2011, all countries had ORs less than 1 in 2011 and 2015, indicating a decline in reported self-reported acute alcohol-related consequences. However, the OR for Sweden was close to 1 in both 2011 and 2015 and was not statistically significant different from the reference group (i.e., 2007). Model 2 was adjusted additionally for gender and HED within the last 30 days. The ORs displayed the same pattern as in model 1, but for Finland the OR in 2015 was no longer significant. Model 3 was further adjusted for volume of pure alcohol consumed on the last drinking occasion and for frequency of consumption during the past 12 months. The same basic pattern could be found again. However, after including frequency of consumption in the past 12 months and thus controlling for three different drinking variables (model 4), only in Norway did the ORs for 2015 show a significant decrease in alcohol-related consequences compared to 2007.
Odds ratios and 95% confidence intervals of multiple regression with having experienced at least one self-reported acute alcohol-related consequencea during the last 12 months regressed on survey year, controlling for gender, HED, alcohol volume from last occasion for survey years 2007–2015.
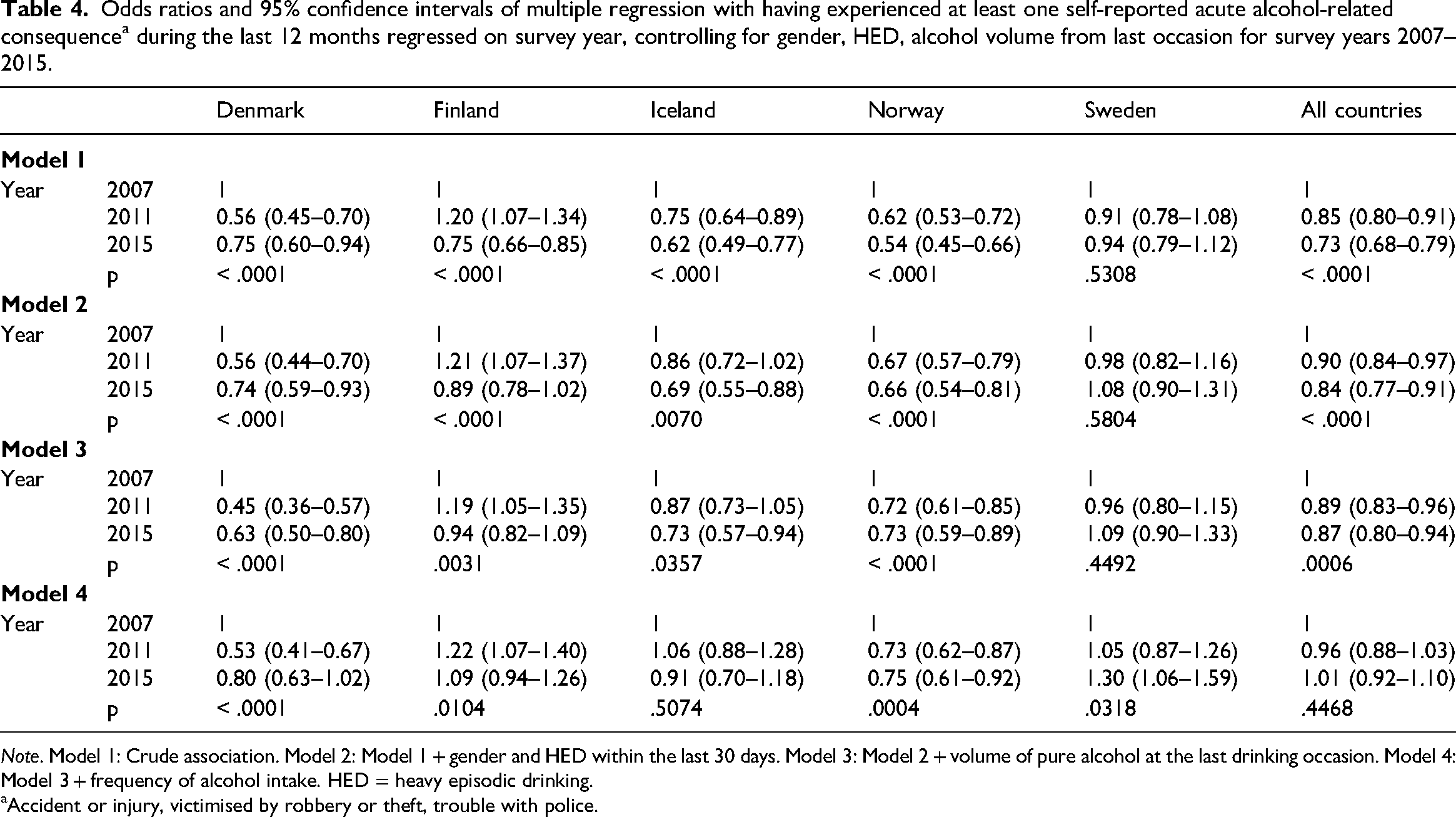
Note. Model 1: Crude association. Model 2: Model 1 + gender and HED within the last 30 days. Model 3: Model 2 + volume of pure alcohol at the last drinking occasion. Model 4: Model 3 + frequency of alcohol intake. HED = heavy episodic drinking.
Accident or injury, victimised by robbery or theft, trouble with police.
When all countries were combined, we found significant reductions in the reporting of self-reported acute alcohol-related consequences across the survey years. This is seen by the ORs below 1 for all subsequent years and in models 1, 2 and 3. However, in model 4, for all countries combined and adjusted for country, gender and all drinking variables, the ORs for 2011 and 2015 were no longer significantly lower (compared to year 2007). This indicates that the decline in alcohol-related consequences can be attributed to the decline in alcohol consumption between 2007 and 2015.
Discussion
The present paper has analysed survey data from three waves (2007, 2011, 2015) of the ESPAD project to examine whether the previously confirmed decrease in youth drinking has been accompanied by a similar decrease in the reporting of self-reported acute alcohol-related consequences (here measured as a sum index of experiencing the following at least once within the last 12 months: (1) accident or injury; (2) victimised by robbery or theft; or (3) trouble with the police).
First, our data have demonstrated and confirmed, once again, the previously reported reduction in alcohol consumption among students aged 15 and 16 years in the Nordic countries (De Looze et al., 2019; ESPAD Group, 2020; Hibell et al., 2012; Kraus et al., 2015). However, for Denmark, only the number of current drinkers decreased significantly, whereas HED and volume of pure alcohol at last drinking occasion were similar between 2007 and 2015. Our examination of reporting at least one self-reported acute alcohol-related consequence among all students, current drinkers and students who engaged in HED, respectively, showed a decline when the total Nordic youth population was combined. However, the trends did vary by country. For example, a slight uptick in Finland and a downtick in Denmark in 2011 were observed when all students, current drinkers and students who engaged in HED were used as the denominator. In Sweden, the decline was only observed when all students were the denominator, and the prevalence remained relatively constant when current drinkers and students who engaged in HED were the denominator. In Iceland and Norway, the prevalence of reporting at least one acute alcohol-related consequence declined over the years when all students and current drinkers were the denominator but remained relatively constant in Iceland throughout all years. The prevalence was also constant between 2011 and 2015 in Norway when students who engaged in HED were the denominator.
The associations between HED and the reporting of at least one self-reported acute alcohol-related consequence were similar between 2007 and 2015 in Sweden and Norway, became stronger over time in Iceland, became weaker over time in Finland and were strongest in 2011 in Denmark.
Since Iceland has experienced the largest decline in youth drinking over the past 20 years, we speculate that those represented in the Icelandic HED group in the later survey years may be a special “hard core” subpopulation of young people, who, characterised by greater risk-taking, would therefore be at greater risk of experiencing self-reported acute alcohol-related consequences. This hypothesis is in agreement with previous studies, which have suggested that the relationship between alcohol consumption and deviant behaviour is stronger in populations where heavy drinking is less prevalent (i.e., the denormalisation theory) (Moan et al., 2021). Hence, our results could possibly explain the stronger association between HED and alcohol-related consequences in 2015 compared to 2007 in Iceland. For Norway and Sweden, however, we found no tendency towards a strengthening of the association between HED and self-reported acute alcohol-related consequences to accompany the general decline in drinking.
Finally, we found an overall decline in self-reported acute alcohol-related consequences between 2007 and 2015 in the combined sample of the Nordic countries. However, when all alcohol consumption variables were included in our analyses, the prevalence of experiencing at least one self-reported acute alcohol-related consequence was no longer statistically significantly lower in 2015 compared to 2007. This indicates that the decline in alcohol consumption can indeed explain the decline in self-reported acute alcohol-related consequences in the Nordic countries. The only exception was Norway, where the prevalence of reporting at least one self-reported acute alcohol-related consequence did significantly decline between 2007 and 2015, even after adjustment for all alcohol consumption variables. This finding in Norway could suggest that the decline in drinking alone might not be the only driving mechanism leading to the decline in self-reported acute alcohol-related consequences. One could speculate whether the drinking setting or environment has changed over the same period, e.g., if young people in Norway are drinking at home more often or under adult observation, this could create a safer drinking environment with lower risk of accident or injury, being victimised by robbery or theft, and experiencing troubles with the police. Unfortunately, we do not have any information on drinking settings in the ESPAD data. Thus, we were unable to find any strong indication of the decline in self-reported acute alcohol-related consequences as being part of a wider societal trend that is creating a less risk-seeking generation of youth (Holmes et al., 2022; Lewycka et al., 2018). This is an area that needs further investigation with other data sources.
Strengths and limitations
It is a strength that our analyses not only investigated this relationship among the Nordic countries in total, but also offered an opportunity to examine individual associations and trends in each country. However, some methodological limitations require attention. An obvious limitation was that due to changes in formulation and variations in inclusion/exclusion of questions regarding alcohol-related consequences over the three survey waves, we were only able to include the following three alcohol-related consequences: (1) accident or injury; (2) victimised by robbery or theft; and (3) trouble with the police. We chose to make a sum index of the three items dichotomised into at least one alcohol-related consequence reported by the respondent versus none, although the consequences were very different in nature and, as a sum, do not cover all types of acute alcohol-related consequences. As sensitivity analyses, we have therefore also presented results for (1) accident or injury, (2) victimised by robbery or theft, and (3) trouble with the police individually. By dichotomising the outcome, we were also not able to look at dose-response effects in terms of experiencing the respective consequences more than one time.
Another limitation of our study was the revision of the questions about self-reported acute alcohol-related consequences in 2015. Upon inspection of the back-translation of the 2015 questionnaire, the question regarding whether students had been under the influence of alcohol when they had experienced an alcohol-related consequence differed slightly (in Sweden, the wording was “while being intoxicated by alcohol” instead of “while being under the influence of alcohol”). The lack of unanimity across countries in the trend of declining rates of self-reported acute alcohol-related consequences during our study period might be attributable in part to country-specific variations in the translation of the master ESPAD questionnaire.
An advantage of our study was that the investigated self-reported acute alcohol-related consequences were diverse in nature, which allowed for an examination of a variety of aspects of alcohol-related consequences. However, it could have been relevant to include even more types of consequences, but we were limited by the availability of measures common to all countries in all survey years. Also, for simplification of the analysis, all types of consequences were grouped together, which could have blurred differences between the consequences. Sensitivity analyses for each self-reported acute alcohol-related consequence variable separately, however, showed similar results (Supplementary Table S1).
As the ESPAD surveys were cross-sectional, data on measures of alcohol consumption and alcohol-related consequences were collected simultaneously. Therefore, we were only able to examine associations and could not establish timing or an ordering of how the factors were related. In addition, the variables had varying time frames, which might have affected the associations. The self-reported acute alcohol-related consequences were asked within a 12-month time frame, whereas HED was asked for the last 30 days, and consumed volume of pure alcohol was reported at the last drinking occasion. Thus, we cannot rule out that some students might have changed their drinking behaviour (e.g., quit HED) as a result of having experienced a self-reported acute alcohol-related consequence. If so, this would lead to differential misclassification and may, to some extent, underestimate the association between HED and the alcohol-related consequences in the present study.
School participation rates varied between countries and across survey years, with a lower rate in Denmark than in the other four countries for all three study waves. Low school participation rates, however, may not necessarily lead to biased estimates. A simulation study of school non-response in surveys on students’ substance use found that lower school participation rates did not largely affect the validity of prevalence estimates (Thrul et al., 2016). Moreover, the proportion of students present in the participating school classes was high in the Nordic countries while the number of students who refused to complete the questionnaire was very low (ESPAD Group, 2016b; Hibell et al., 2009, 2012).
Conclusions
In the five Nordic countries, we found an overall decline in alcohol use and self-reported acute alcohol-related consequences among adolescents aged 15–16 years between 2007 and 2015 in the combined sample of the Nordic countries, but with differences between the individual countries. We found marked differences in the prevalence of reporting acute alcohol-related consequences between 2007 and 2015 among all students, current drinkers and heavy episodic drinkers in the Nordic countries. Furthermore, we found no support for the denormalisation theory of a strengthening of the alcohol-consequences association with declining drinking among adolescents, except in Iceland.
Supplemental Material
sj-docx-1-nad-10.1177_14550725241229016 - Supplemental material for Implications of the decline in adolescent drinking on the experience of alcohol-related consequences in the Nordic countries: A study based on data from the ESPAD project
Supplemental material, sj-docx-1-nad-10.1177_14550725241229016 for Implications of the decline in adolescent drinking on the experience of alcohol-related consequences in the Nordic countries: A study based on data from the ESPAD project by Ola Ekholm, Veronica Pisinger, Heidi Amalie Rosendahl Jensen and Kim Bloomfield in Nordic Studies on Alcohol and Drugs
Footnotes
Acknowledgements
We thank our fellow NOS project members and the anonymous reviewers for their useful comments on previous drafts of this manuscript.
Data statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This publication is a product of a Nordic research collaboration project entitled “Twenty years later: Explanations and consequences of the decline in adolescents’ drinking in the Nordic countries”, which has been funded in part by a grant (Decision Number 328792) from The Joint Committee for Nordic Research Councils in the Humanities and Social Sciences (NOS-HS). This partial funding supported scientific meetings, including travel and accommodation, to promote the collaborative process during the project.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.