
Abstract
Keywords
Problematic parental substance use (PPSU) has been shown to have a significant impact not only on childhood experiences but also on outcomes in adolescence and adulthood (Brummer et al., 2021; Raitasalo & Holmila, 2017; Ramstedt et al., 2022; Velleman & Templeton, 2016). But what role does family structure play in this association? Is it better for a child to live in a family with both parents, including the parent with substance use problems, or to live only with the parent who does not have substance use problems? These types of questions take as their starting point different perspectives on the relative importance of family separation versus PPSU.
PPSU and other family problems often co-occur. Families with PPSU have a higher risk of parental separation and parental mental health problems, as well as more frequent economic problems, compared to families without PPSU (Frederiksen et al., 2022; Holst et al., 2020; Jääskeläinen et al., 2016; Kuppens et al., 2020; Waldron et al., 2013). Family environments and parenting styles vary, but research has shown that tension, conflicts and harsh parenting are more frequent when PPSU is also present (Templeton et al., 2009; Velleman & Templeton, 2007, 2016). Children are at increased risk of traumatic memories if the childhood was characterised by a dysfunctional family environment with tension and conflicts (Haugland et al., 2021; Järvinen, 2015). Thus, PPSU and its effect on the family as a whole should be seen as an interplay between PPSU and other family problems.
Difficulties extend outside the family environment, as children from families with PPSU more often experience problems at school (Johnson et al., 2017; Ramstedt et al., 2022), poorer academic outcomes (Berg et al., 2016; Brook, 2010) and a higher risk of mental disorders, substance use problems, hospitalisations and criminality (Brummer et al., 2021; Christoffersen & Soothill, 2003; Park & Schepp, 2015; Smith & Wilson, 2016). Prior studies have explored differences in life circumstances as well as in the level of family-related problems among families with PPSU. Jääskeläinen et al. (2016) identified five different types of families based on PPSU, the gender of the parent, the type of substance and family status: the drinking father; the absent drinking father; the drinking mother; the drug-using mother; and broken families. However, this study did not explore the association between family type (for instance, families with a drinking father versus an absent drinking father) and different outcomes in the child's later youth or adulthood (Jääskeläinen et al., 2016). A Danish study found that parental alcohol problems were associated with a higher odds of internalising problems among high school and vocational school students and that the association was not stronger if the young person lived with the parent with alcohol problems (Pisinger et al., 2016). This study, however, did not investigate the direct link between cohabitation and problems in youth and only looked at one outcome, internalising mental health problems.
Children from separated or divorced families are at an increased risk of some of the same consequences as children who have experienced PPSU, such as problematic use of substances (Hope et al., 1998; Sadler et al., 2017; Waldron et al., 2014), anxiety or depression (Otowa et al., 2014; Strohschein, 2005) and overall poor physical health (Bzostek & Beck, 2011). Research has found that while children of divorced or separated parents experience more internalising and externalising problems, as well as lower self-esteem, it may not be the divorce in itself that is the crucial element but whether stressful circumstances are present in the time before, during and after the divorce (Amato, 2000; Strohschein, 2005; van Dijk et al., 2020).
Given that children with PPSU more often experience family separation compared with children without PPSU, the question is, how do these two risk factors interplay? Prior studies have, on the one hand, shown that parental separation and divorce can have quite a considerable long-term impact, such as increasing the risk of mental health problems (Chase-Lansdale et al., 1995; Strohschein, 2005) and problematic use of substances (Hope et al., 1998). Sadler et al. (2017) explored the associations between paternal alcohol problems, separation and academic performance and concluded that separation was more strongly associated with high school non-completion than parental alcohol problems. A substantial number of studies have investigated whether PPSU or parental divorce/separation more strongly predicts outcomes such as substance use, sexual debut and quality of interpersonal relationships with parents (McCutcheon et al., 2018; Waldron et al., 2014; Windle & Windle, 2018). An Australian study based on a sample of children of twins concluded that early substance involvement was primarily predicted by parental separation and that parental dependence on alcohol and cannabis, including genetic risks, were not predictive in most models (Waldron et al., 2014).
The critique of using two-parent households as the gold standard for healthy child development has raised awareness of how new types of non-traditional family structures are becoming more prevalent (Ford-Gilboe, 2000; Shaw et al., 2019). Amato (2000) argues that the rising divorce rate was one of the most dramatic changes in family life during the 20th century. In Denmark, the divorce rate was 1%–2% at the end of the 19th century, but, 100 years later, the rate had risen to 44% (Vallgårda, 2021). This increase means a greater social acceptance of divorce and family separation in Denmark, and researchers have argued that adults thrive and children develop just as well in a variety of family structures (Amato, 2000). This topic could be explored further by comparing societies with high and low divorce rates and examining if the consequences of a divorce are different for children in societies with a higher acceptance of divorce. At the same time, divorce and separation can be a solution to a dysfunctional home environment, and a critique of the existing research has pointed at how the quality of family life before parental divorce has not been taken into account (Strohschein, 2005).
As mentioned, young people and adults with PPSU are at higher risk of adverse academic, labour market, legal, and physical and mental health outcomes compared with their peers. Prior research on the impact of the family structure has primarily focused on single outcomes. The present study, however, investigated a broader spectrum of adverse outcomes: school/work problems; hospitalisation; mental health problems; and criminality.
Aim of the study
The aim of the present study was to investigate the association between childhood family structures, including the presence or absence of PPSU, and adverse outcomes during adolescence/young adulthood. Family structures included information about whether the child lived with both parents during all 15 years of childhood, PPSU and the number of years of living with the parent with problematic substance use. Outcomes were not being in education, employment or training (NEET), hospital admissions, mental disorders and criminality.
Three different hypotheses were formed: (1) living with both parents during childhood would protect against adverse outcomes; (2) PPSU would increase the risk of adverse outcomes; and (3) the longer a child or young person lived with the parent with the problematic substance use during childhood and adolescence, the higher the odds of adverse outcomes would be.
Methods
This study used data from two national surveys to define the sample and parts of the measure of PPSU (described below). The survey data were linked with nationwide register data on both the young people and their parents from the time of the youth's birth up to 2015/2018. The register data were used to define parts of the measure of PPSU, the family structures and the outcome variables.
Procedure and sample
In 2014 and 2015, two national surveys (YouthMap surveys) were conducted in Denmark among youth aged 15–25 years (Pedersen et al., 2017). The focus of the surveys was on youth well-being, psychological, social, behavioural and physical problems and resources, as well as the use of different substances. Of the initial random sample of 10,414 young persons, 5,755 participated, giving a response rate of 55.3% (Table 1).
Demographic characteristics of the sample and the participants.
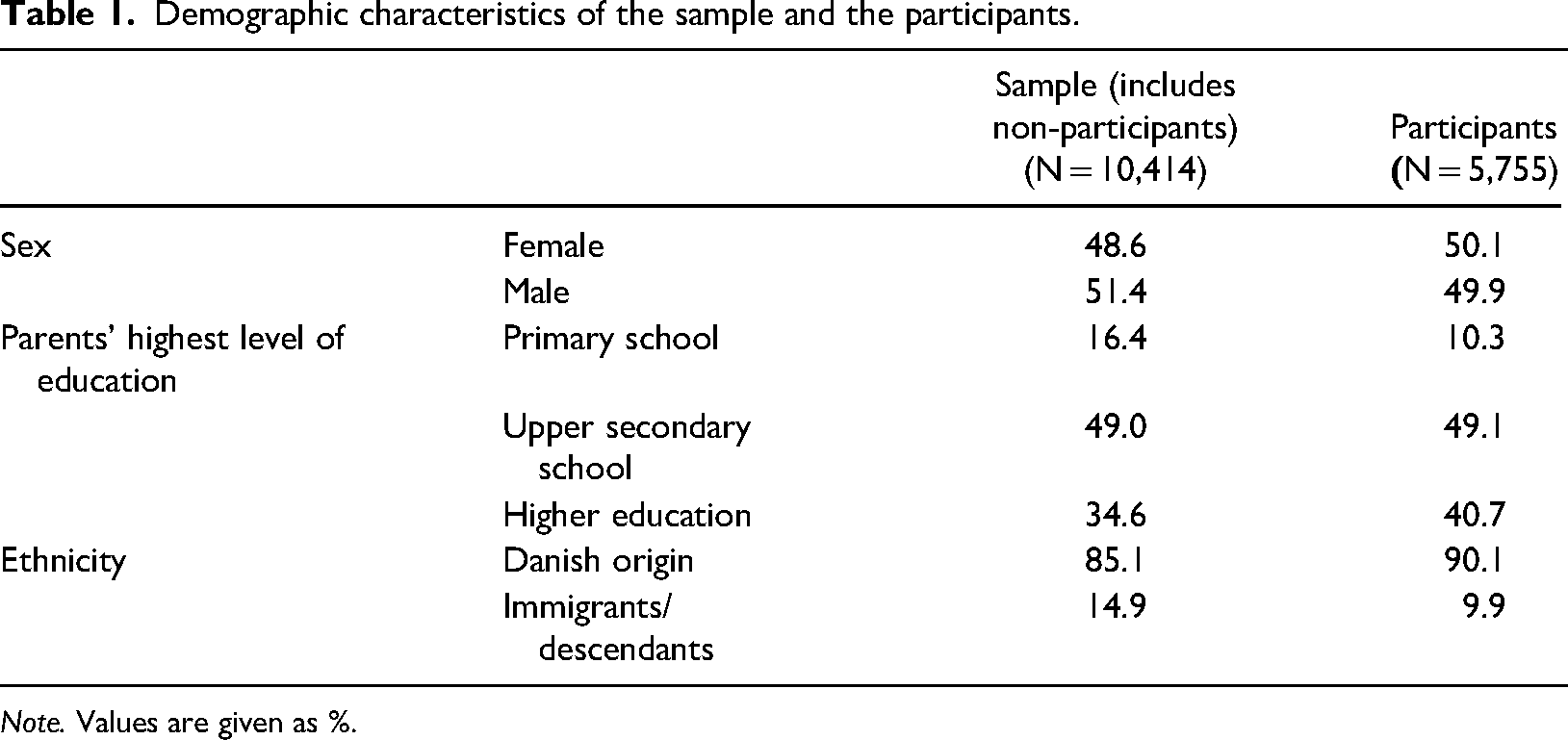
Note. Values are given as %.
The study population for the present study included the 9,770 young people from the survey samples who were also registered in the Danish Civil Registration System (Pedersen, 2011). The remaining 644 young people with missing register data about family structure during childhood were mostly immigrants and likely with their parents in another country. The Danish Civil Registration System was used to identify the parents of the study population, as well as the family structure (living with both parents or not) and years of living with each parent in the first 15 years of the young people's lives.
Exposure
PPSU
The measure of PPSU was a combination of self-reported and register-based PPSU. Participants in the two surveys were asked whether their parents had misused alcohol or drugs. The sub-question “Which parent?” (response options: “Father”, “Mother”, “Both”, “Do not want to answer”, “Don’t know”) identified the respective parent(s) with problematic substance use. Register-based PPSU was defined based on whether a parent had a substance-related contact in a hospital, criminal justice, prescription, alcohol and drug treatment, or cause of death register (from 1989 – or the year the register was established if it was after 1989 – until 2015; see Table 1 in Supplementary material). For further information, see Frederiksen et al. (2021) and Frederiksen et al. (2022). Out of the study population of 9,770 young people, 1,884 (19.3%) were identified as having PPSU, either by survey or register data. By using the different data sources, it was possible to capture different types of youth and families. The self-reports gave insight into families that had not been in contact with the different services (such as alcohol or drug treatment, mental health services, etc.) even though severe parental alcohol or drug problems may have been present (Ramstedt et al., 2022). Many people never seek help for their alcohol or drug problems (Oleski et al., 2010), and self-reports are an important source to identify these individuals. On the other hand, survey studies only give information about the participants, and survey non-participants have been shown to have higher levels of different problems compared with participants (Frederiksen et al., 2021; Gundgaard et al., 2007). Registers can provide information about non-participants, and register-based studies have other advantages, including large study populations, wide population coverage, as well as access to historical data.
Family structures
Data from the Danish Civil Registration System identified which parent the child lived with during each year, from birth up to and including the child's 15th birthday (Pedersen, 2011). Using this information, five family structures with varying durations of living with a parent with problematic substance use were defined as follows: (1) living with both parents all 15 years, without PPSU (“Both/−PPSU”); (2) living with both parents all 15 years, with PPSU (“Both/+ PPSU”); (3) not living with both parents, without PPSU (“Not both/−PPSU”); (4) not living with both parents, with PPSU, living 0–4 years (“brief period”) with the parent with problematic substance use (“Not both/ + PPSU, brief”); and (5) not living with both parents, with PPSU, living 5–15 years (“long period”) with the parent with problematic substance use (“Not both/ + PPSU, long”).
The distinction between “brief” and “long” periods of living with the parent with substance use (groups 4 and 5) was made based on the median number of years (median = 4) living with the parent with substance use in families where the parents did not live together all 15 years of the young person's childhood.
Outcome variables
Adverse outcomes included NEET, hospital admissions, criminal convictions except traffic offences and mental disorders. Outcomes were identified during the ages of 15–20 years.
Not in education, employment or training
Information on the receipt of social benefits, work and education was obtained from Danish registers on personal labour market affiliation (Petersson et al., 2011). Social benefits included unemployment benefits and early retirement but not leave benefits such as State Education Support or parental leave. The category NEET was defined as receiving social benefits at the age of 20 years. In the primary analysis, the variable was dichotomised (Not NEET/NEET). In a secondary analysis, the group not included in NEET was further investigated using two subgroups: (1) working and (2) enrolled in education. Each variable was dichotomised (Not working/Working; Not in education/In education).
Hospitalisations
The National Patient Register (NPR) (Lynge et al., 2011) contains records of admissions to all hospitals in Denmark, both private and public, and covers inpatient, outpatient, and acute and emergency care. In the first analysis, hospital admissions from the ages of 15–20 years were dichotomised (No hospitalisations/Hospitalisations). In a secondary analysis, the specific cause of the admission was included in order to distinguish whether the admission was related to health problems (illness as the cause), mental problems (indicated by suicide attempts) or social problems (indicated by violence). The following causes of admissions were included: (1) illness (without any external cause); (2) accident; (3) violence; (4) suicide attempt; and (5) “other cause” (Schmidt et al., 2015). Each was dichotomised in the analysis.
Diagnoses of mental disorders
Information on the young people's diagnoses of mental disorders during the ages of 15–20 years was drawn from the Psychiatric Central Register (PCR) (Mors et al., 2011; Sahl Andersen et al., 2011). The PCR covers all hospital-based psychiatric care in Denmark, similar to the NPR. The first analysis investigated the odds of any diagnosis of mental disorders, and the outcome was dichotomised (No mental disorder/Mental disorder). Subsequent analyses examined different types of diagnoses using the following three subgroups, which were constructed based on prevalence using International Classification of Diseases (ICD-10) codes (World Health Organization, 2004): anxiety disorders (F4-diagnosis); behavioural and emotional disorders with onset usually occurring in childhood and adolescence (F9-diagnosis); and “other disorders” (all other F-diagnoses). The subgroups were each dichotomised (No diagnosis/One or more diagnoses), and an individual could be included in one or more of the subgroups if they had been diagnosed with more than one type of disorder during the ages of 15–20 years.
Criminality
Criminality was defined as any registration of a conviction in the Danish Central Crime Register during the ages of 15–20 years (Ravn, 2001). Traffic offences were excluded. In the first analysis, criminality was dichotomised (No criminality/Criminality). Secondary analyses included information on the type of crime: property crimes (e.g., burglary); drug-related crimes (e.g., possession and distribution); and “other offences”. Each was dichotomised (No/Yes).
Ethics
The invitations to participate in the two YouthMap surveys included a description of the purpose of the study, information about voluntary participation and a statement that all confidentiality and privacy requirements were met. Participants indicated their informed consent by completing the survey. The two survey studies as well as the present study were registered with the Danish Data Protection Agency.
Statistical analysis
A descriptive analysis examined the distribution of the different family structures and the outcomes. Next, the associations between family structure and four adverse outcomes (i.e., receipt of social benefits, hospitalisation, mental disorders and criminal conviction) were investigated using binary logistic regression models, with young males living with both parents without PPSU as the reference group. Pairwise comparisons were performed between structure 1 (“Living with both parents/without PPSU”) and the four other structures. The analyses included an interaction between gender and the respective family structure, based on research showing gender differences in outcomes, such as education, mental health problems and criminality (Camenius & Sandman, 2021; Chesney-Lind & Chagnon, 2016; Pekkarinen, 2012). In the analysis, odds ratios (OR), p-values and 95% confidence intervals (CI) were reported. In a post-estimation analysis, the adjusted risk difference (ARD) was calculated for each type of family structure to report an absolute risk measure.
In the second part of the analysis, logistic regression models investigated the four outcomes in more detail. The relationship between family structure and odds of being employed or enrolled in education was analysed. In the area of health consequences, hospital admissions were divided into four categories based on the reason for the contact, and the relationships with the different family structures were analysed. Subgroups of mental disorder diagnoses were analysed to shed light on whether some family structures were associated with an increased risk of particular diagnoses. Different types of criminalities were analysed to determine whether different family structures were associated with an increased risk of conviction for different reasons.
All analyses controlled for ethnicity (Danish origin vs. immigrants/descendants), parents’ highest level of education (primary education only vs. any additional education), parental mental disorder (any record in the PCR except F10–F19 diagnoses, which were included in the PPSU measure) and parental receipt of social benefits (≥3 consecutive years vs. <3 consecutive years). These variables have to be taken into account, as previous research has found them to be important confounders when investigating outcomes such as NEET, hospitalisation, mental health problems and criminality (Bachman et al., 2011; Balsa, 2008; Chesney-Lind & Chagnon, 2016; Leis & Mendelson, 2010; Mock-Muñoz de Luna et al., 2019; Povlsen et al., 2018; Weissman et al., 2016; Yu, 2018). Parental mental disorders and receipt of social benefits (including unemployment benefits and early retirement but not State Education Support or parental leave) were measured in the years after the birth of the child. Being on social benefits indicates not only a long period of unemployment, but also an economic disadvantageous situation. Information on parents’ employment status was obtained from Danish registers on personal labour market affiliation (Petersson et al., 2011). The analyses were conducted with STATA 16 (StataCorp., 2019).
Results
Distribution of types of families and outcomes
The distribution of family structures was as follows: 4,273 young people (43.7%) in Both/−PPSU; 471 (4.8%) in Both/+PPSU; 3,613 (37.0%) in Not both/−PPSU; 717 (7.3%) in Not both/+PPSU, brief; and, lastly, 696 (7.1%) in Not both/+PPSU, long.
Concerning the outcomes, 436 (4.5%) of the young persons were in the category NEET when they were aged 20 years, and 6,811 (69.7%) had one or more hospital admissions during the ages of 15–20 years. Between the ages of 15–20 years, 887 (9.1%) had a mental disorder diagnosis and 1,114 (11.4%) young people were convicted of one or more crimes.
Association between family structures and adverse outcomes in young adulthood
The relationship between family structure, including years living with a parent with problematic substance use, and the study outcomes is illustrated in Table 2. Both/−PPSU was used as the reference group, and the analysis explored whether young people from the other family structures had increased odds of the different adverse outcomes.
Family structures and ORs for adverse outcomes at age 15–20 years from a logistic regression using “Both/ PPSU” as the reference group (n = 9,770).
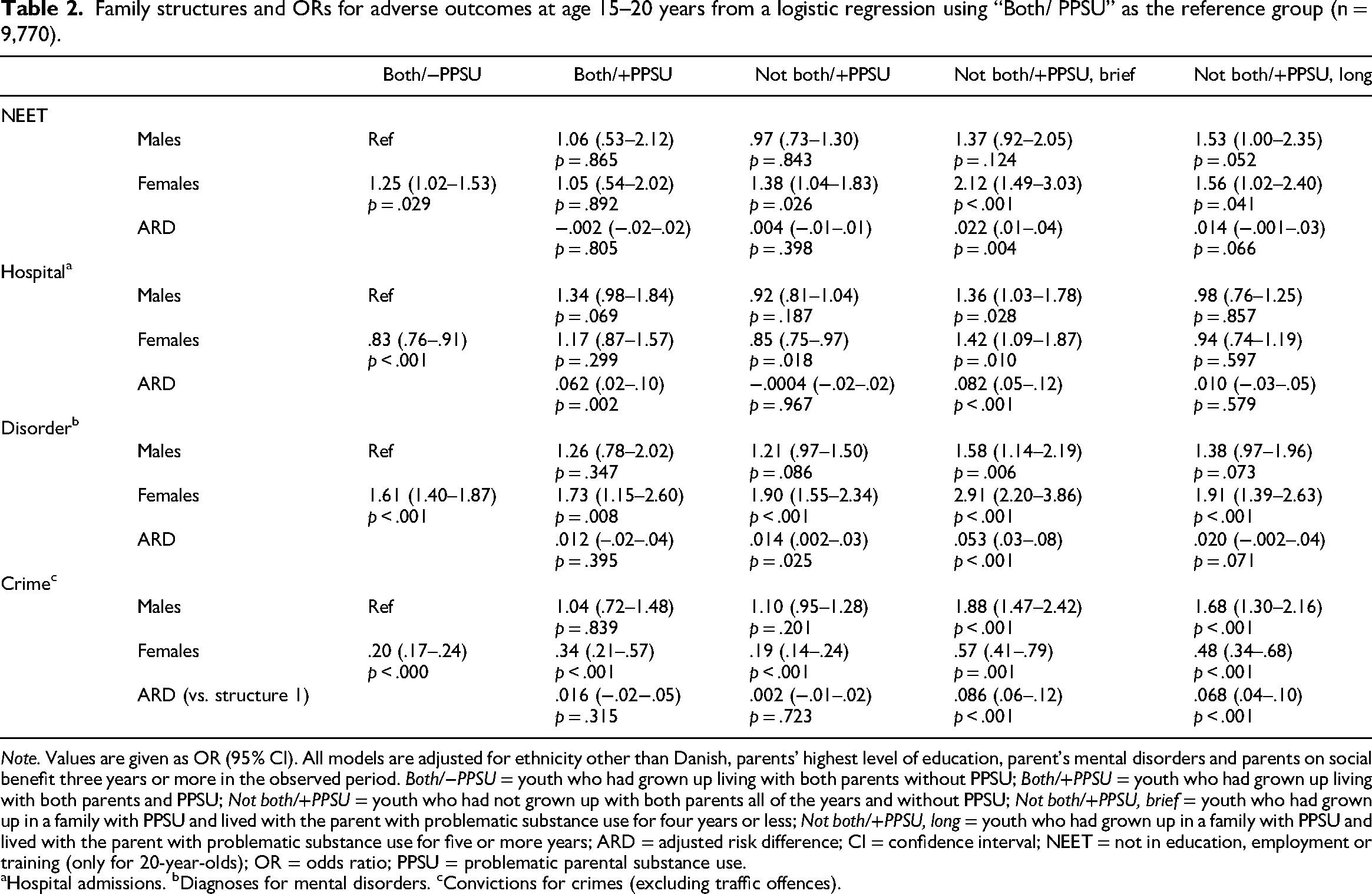
Note. Values are given as OR (95% CI). All models are adjusted for ethnicity other than Danish, parents’ highest level of education, parent's mental disorders and parents on social benefit three years or more in the observed period. Both/−PPSU = youth who had grown up living with both parents without PPSU; Both/+PPSU = youth who had grown up living with both parents and PPSU; Not both/+PPSU = youth who had not grown up with both parents all of the years and without PPSU; Not both/+PPSU, brief = youth who had grown up in a family with PPSU and lived with the parent with problematic substance use for four years or less; Not both/+PPSU, long = youth who had grown up in a family with PPSU and lived with the parent with problematic substance use for five or more years; ARD = adjusted risk difference; CI = confidence interval; NEET = not in education, employment or training (only for 20-year-olds); OR = odds ratio; PPSU = problematic parental substance use.
Hospital admissions. bDiagnoses for mental disorders. cConvictions for crimes (excluding traffic offences).
Young males had the same odds of NEET irrespective of family structure, but young females had higher odds of NEET if they came from a family structure where they had not been living with both parents (both with and without PPSU). Girls from family structure 4 (“Not living together with both parents/with PPSU, 0–4 years”) had twice the odds (OR = 2.12; p < .001; 95% CI = 1.49–3.03) of NEET compared with boys from family structure 1 (“Living with both parents/without PPSU”), and taking the ARD into account, this was the only group with a significant difference in relation to the risk of NEET (ARD = 0.022; p = .004; 95% CI = .01–.04).
The risk of hospitalisation did not significantly differ between the different family structures with one exception: young individuals, both male and female, from family structure 4 (“Not living together with both parents/with PPSU, 0–4 years”) had significantly higher odds (males: OR = 1.36; p = .028; 95% CI = 1.03–1.78; females: OR = 1.42; p = .010; 95% CI = 1.09–1.87) of hospitalisation compared with males from family structure 1. The ARD was also significant (ARD = .082; p < .001; 95% CI = .048–.117).
Among young males, only those living in family structure 4 (“Not living together with both parents/with PPSU, 0–4 years”) had a significantly higher odds of a mental disorder compared with the reference group (OR = 1.58; p = .006, 95% CI = 1.14–2.19). In general, young females had higher odds of mental disorders compared with the reference group of young males from family structure 1 (“Living with both parents without PPSU”), but taking the ARD into account, the differences persisted for females from structure 3 (“Not living with both parents/without PPSU”: ARD = .014; p = .025; 95% CI = .002–.026) and structure 4 (“Not living with both parents/with PPSU, 0–4 years”: ARD = .053; p < .001; 95% CI = .029–078).
The odds of being convicted of a crime were significantly higher for young males from the two types of family structures in which the parents did not live together and in which there was PPSU: structure 4 (“Not living with both parents/with PPSU, 0–4 years”: OR = 1.88; p < .001; 95% CI = 1.47–2.42) and structure 5 (“Not living with both parents/with PPSU, 5–15 years”: OR = 1.68; p < .001; 95% CI = 1.30–2.16). The ARD was also significant for both family structures (structure 4: ARD = .086; p < .001; 95% CI = .057–.115; structure 5: ARD = .068; p < .001; 95% CI = .040–.95). Females in all types of family structures had significantly lower odds of being convicted compared with the reference group.
Social benefits, education and employment
Compared to the reference group (Both/−PPSU), young people living with both parents and experiencing PPSU (Both/+PPSU) and young people not living with both parents and not experiencing PPSU (Not both/−PPSU) did not have a significantly different odds of being enrolled in education. But the odds were significantly lower for young persons from Not both/+PPSU, brief (OR = .67; p < .001) and from Not both/+PPSU, long (OR = .64; p < .001) (Table 3). The odds of being employed were not significantly different for the young people from the different types of families.
Logistic regression for being in education or working when 20 years old, comparing the five family structures (n = 9,770).
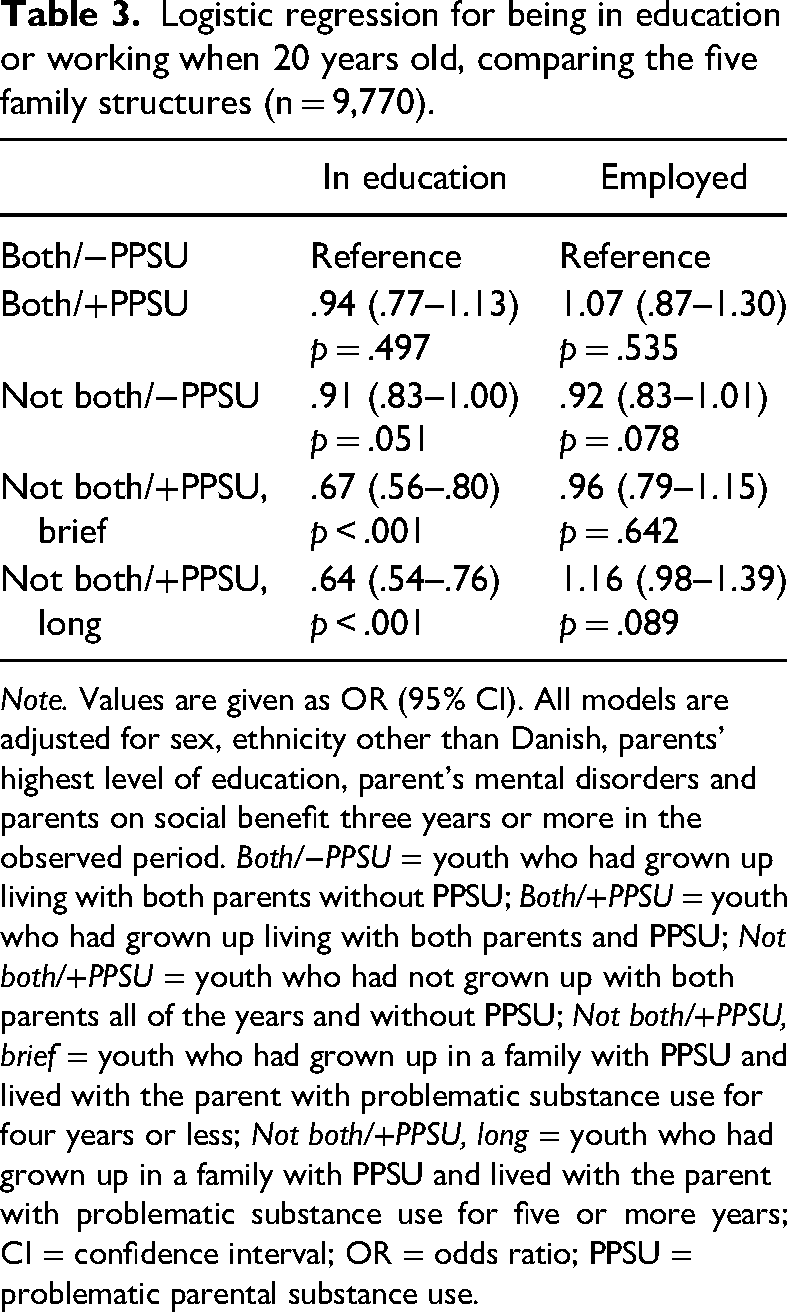
Note. Values are given as OR (95% CI). All models are adjusted for sex, ethnicity other than Danish, parents’ highest level of education, parent's mental disorders and parents on social benefit three years or more in the observed period. Both/−PPSU = youth who had grown up living with both parents without PPSU; Both/+PPSU = youth who had grown up living with both parents and PPSU; Not both/+PPSU = youth who had not grown up with both parents all of the years and without PPSU; Not both/+PPSU, brief = youth who had grown up in a family with PPSU and lived with the parent with problematic substance use for four years or less; Not both/+PPSU, long = youth who had grown up in a family with PPSU and lived with the parent with problematic substance use for five or more years; CI = confidence interval; OR = odds ratio; PPSU = problematic parental substance use.
Causes of hospital admission
A total of 6,811 young people had one or more hospital admissions during the ages of 15–20 years (Table 4). Accidents were the most frequent cause of hospital admission, as 4,177 young people had one or more accident-related admissions (4,177/6,811, 61.3%). Illness was the second most frequent cause of admission (1,815/6,811, 26.7%). The remaining causes of hospitalisation were violence, suicide attempts and “others” (1,514/6,811, 22.2%) (Table 4).
Logistic regression for the cause of hospital admission during the ages of 15–20 years comparing the five family structures (n = 9,770).
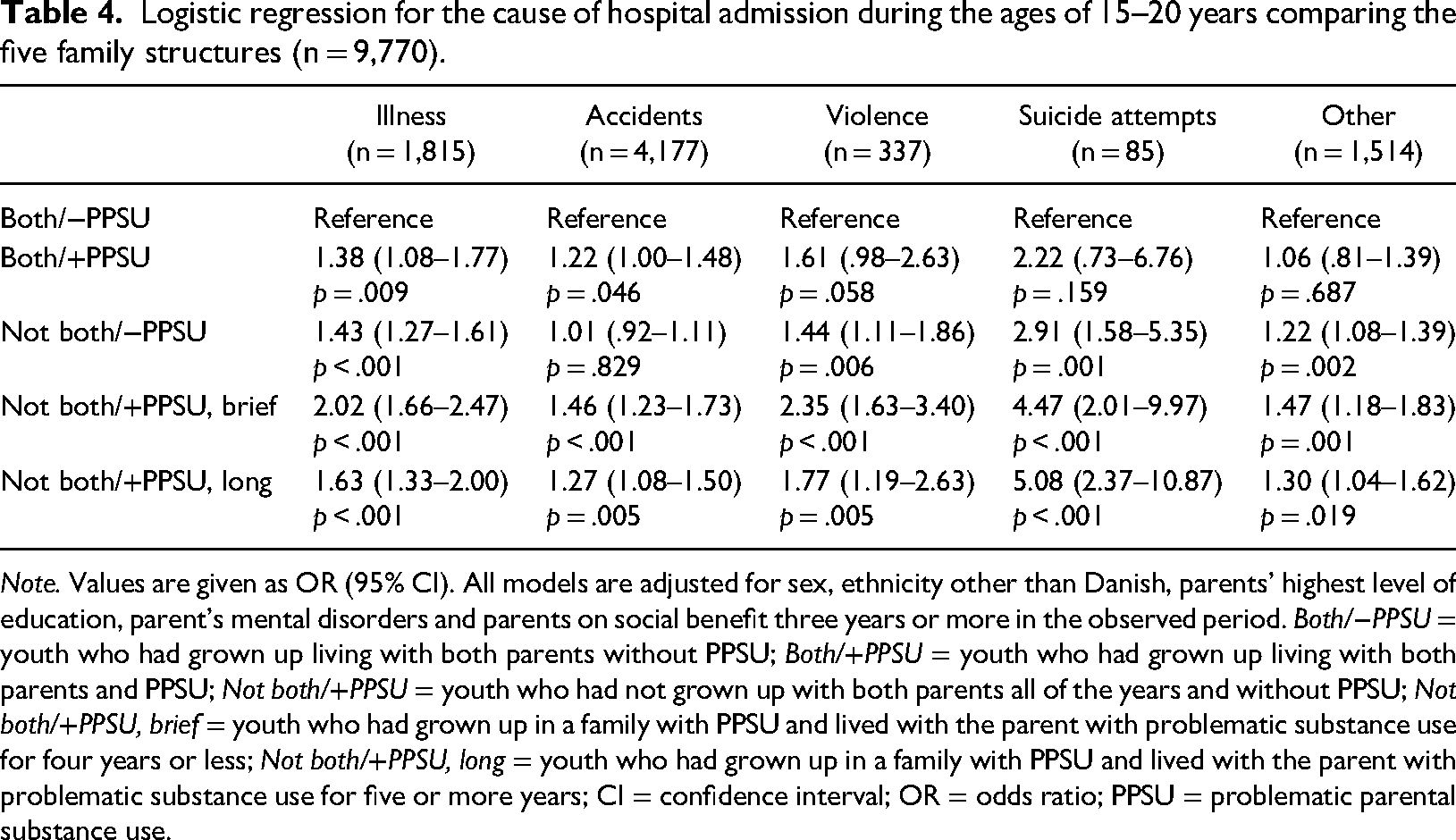
Note. Values are given as OR (95% CI). All models are adjusted for sex, ethnicity other than Danish, parents’ highest level of education, parent's mental disorders and parents on social benefit three years or more in the observed period. Both/−PPSU = youth who had grown up living with both parents without PPSU; Both/+PPSU = youth who had grown up living with both parents and PPSU; Not both/+PPSU = youth who had not grown up with both parents all of the years and without PPSU; Not both/+PPSU, brief = youth who had grown up in a family with PPSU and lived with the parent with problematic substance use for four years or less; Not both/+PPSU, long = youth who had grown up in a family with PPSU and lived with the parent with problematic substance use for five or more years; CI = confidence interval; OR = odds ratio; PPSU = problematic parental substance use.
Compared to young persons from Both/−PPSU families, the odds of hospitalisation due to illness were higher for young persons from Both/+PPSU (OR = 1.38; p = .009), Not both/−PPSU (OR = 1.43; p < .001), Not both/+PPSU, brief (OR = 2.0; p < .001) and Not both/+PPSU, long (OR = 1.63; p < .001) families. The odds of accident-related admissions were significantly higher among persons from Both/+PPSU (OR = 1.22; p = .046), Not both/+PPSU, brief (OR = 1.46; p < .001) and Not both/+PPSU, long (OR = 1.27; p = .005) families compared with young persons from Both/−PPSU families. There were also higher odds of hospitalisations due to violence and suicide attempts among young people not living with both parents, with the highest increased odds among the two PPSU families (“Not both/+PPSU, brief/long”).
Types of diagnoses of mental disorders
A total of 887 young people received a mental disorder diagnosis between the ages of 15–20 years. Primary or secondary F4-diagnoses for “anxiety, dissociative, stress-related, somatoform and other nonpsychotic mental disorders” were the most frequent (358/887, 40.4%), followed by F9-diagnoses (primary or secondary) for “behavioural and emotional disorders with onset usually occurring in childhood and adolescence” (240/887, 27.1%). Diagnoses of “Other” disorders primarily consisted of F3-diagnoses for “mood (affective) disorders” and Z0-diagnoses for “persons encountering health services for examinations” (“other” diagnoses in total 594/887, 67.0%) (Table 5).
Logistic regression for types of mental disorders during the ages of 15–20 years, comparing the five family structures (n = 9,770).
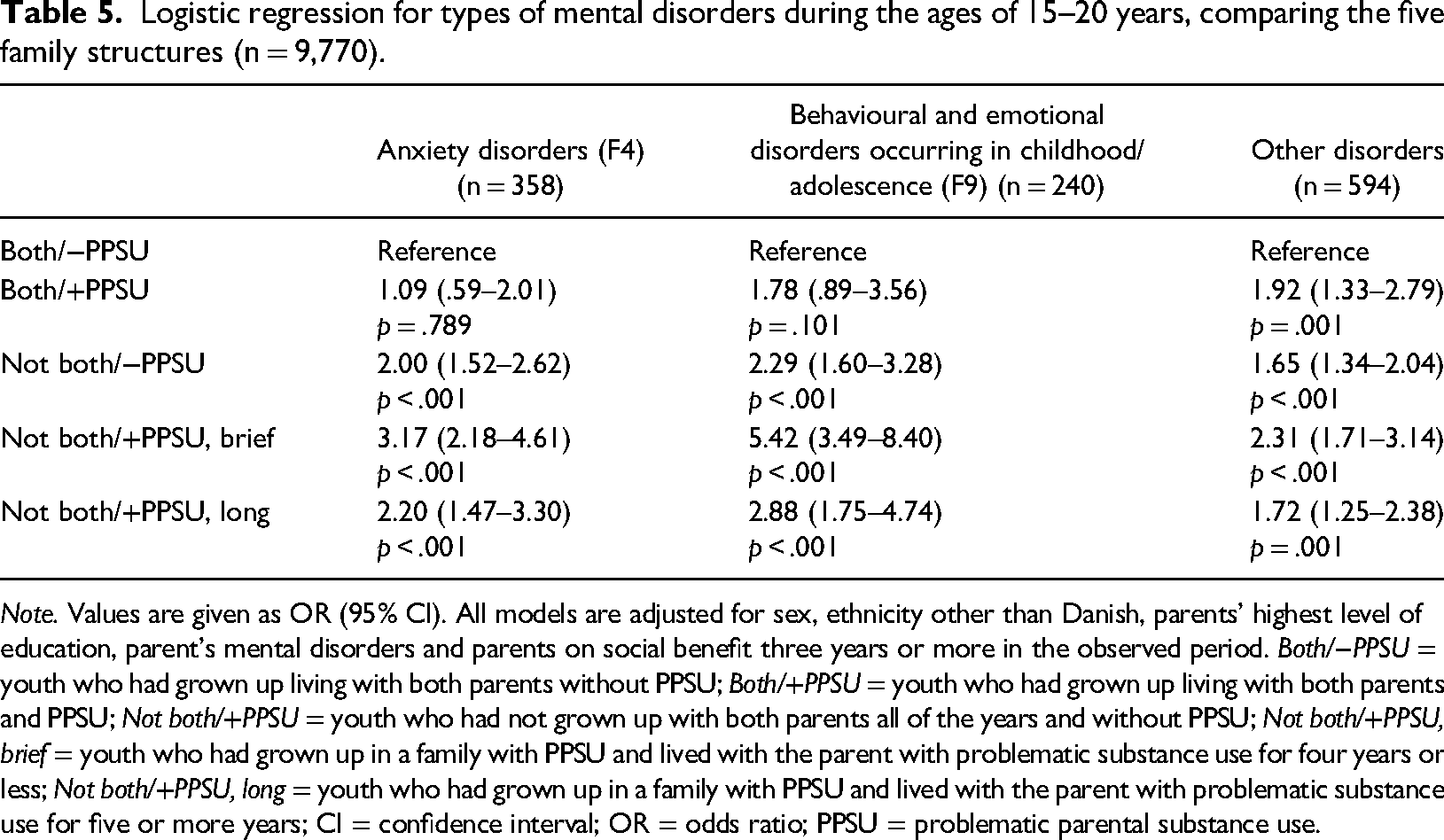
Note. Values are given as OR (95% CI). All models are adjusted for sex, ethnicity other than Danish, parents’ highest level of education, parent's mental disorders and parents on social benefit three years or more in the observed period. Both/−PPSU = youth who had grown up living with both parents without PPSU; Both/+PPSU = youth who had grown up living with both parents and PPSU; Not both/+PPSU = youth who had not grown up with both parents all of the years and without PPSU; Not both/+PPSU, brief = youth who had grown up in a family with PPSU and lived with the parent with problematic substance use for four years or less; Not both/+PPSU, long = youth who had grown up in a family with PPSU and lived with the parent with problematic substance use for five or more years; CI = confidence interval; OR = odds ratio; PPSU = problematic parental substance use.
Young people from the three family structures where the child did not live with both parents had a higher odds of a diagnosis of anxiety disorder compared to young people who lived with both parents and did not experience PPSU, with the highest odds among young people from Not both/+PPSU, brief (OR = 3.17; p < .001), which was also the group with the highest odds of having a diagnosis of childhood and adolescent behavioural and emotional disorder (OR = 5.42; p < .001) and other diagnoses (OR = 2.31; p < .001) (Table 5).
Types of criminality
Property crimes (n = 527, 22.4%) were the most common type of crime for which the young people were convicted, followed by drug-related crimes, including possession (n = 260, 11.0%). A final category of “other” offences accounted for 28.6% (n = 674) of the convictions (Table 6).
Logistic regression for types for criminality during the ages of 15–20 years, comparing the five family structures (n = 9,770).
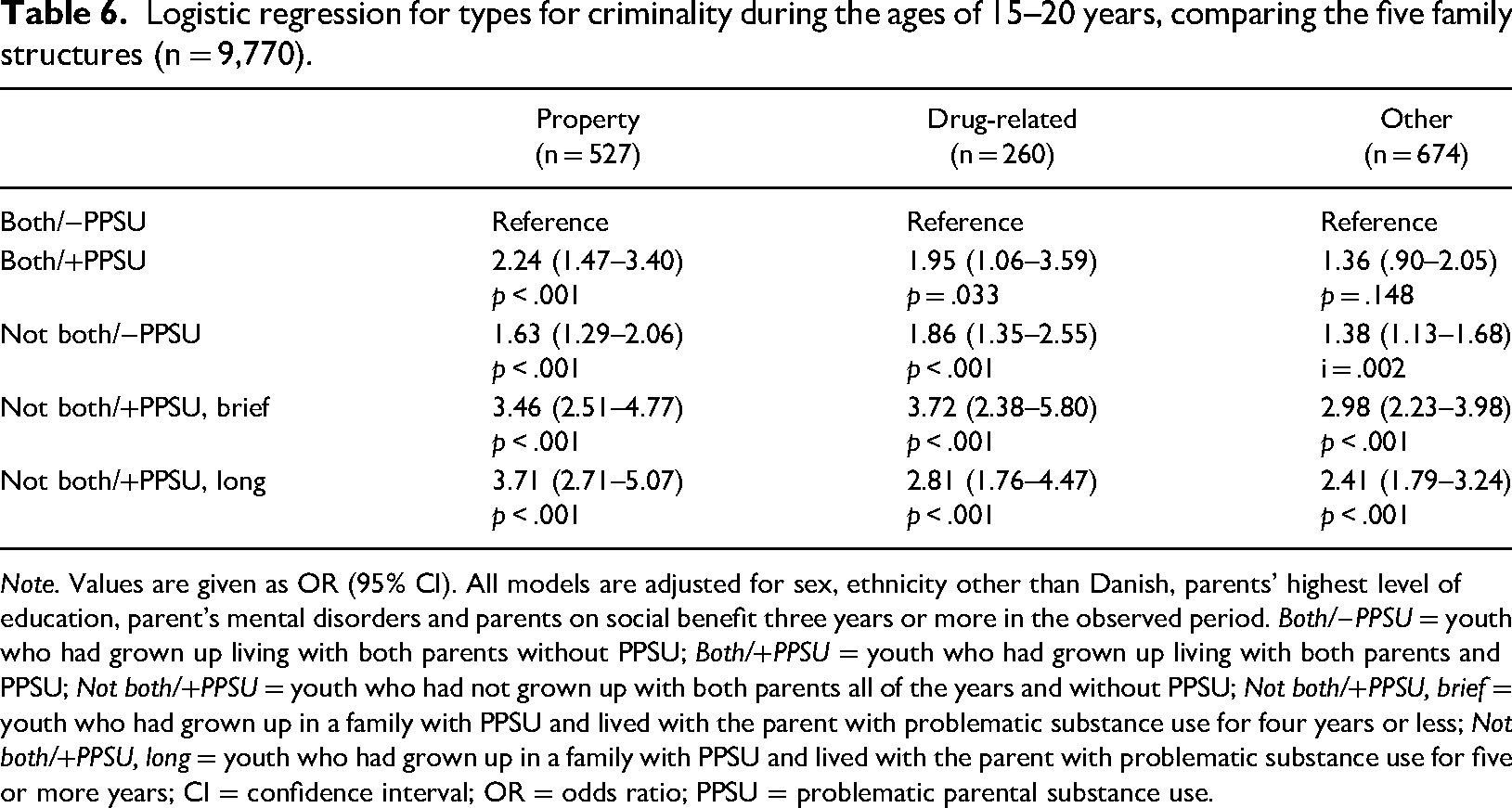
Note. Values are given as OR (95% CI). All models are adjusted for sex, ethnicity other than Danish, parents’ highest level of education, parent's mental disorders and parents on social benefit three years or more in the observed period. Both/−PPSU = youth who had grown up living with both parents without PPSU; Both/+PPSU = youth who had grown up living with both parents and PPSU; Not both/+PPSU = youth who had not grown up with both parents all of the years and without PPSU; Not both/+PPSU, brief = youth who had grown up in a family with PPSU and lived with the parent with problematic substance use for four years or less; Not both/+PPSU, long = youth who had grown up in a family with PPSU and lived with the parent with problematic substance use for five or more years; CI = confidence interval; OR = odds ratio; PPSU = problematic parental substance use.
The odds of conviction for the different offences were higher among all the other groups when comparing each group with Both/−PPSU (except “Other” crimes among young people from Both/+PPSU). The highest odds of conviction were among young people not living with both parents and with PPSU.
Discussion
We hypothesised that living with both parents during childhood would protect against adverse outcomes such as NEET, physical problems (hospital admissions), mental disorders and criminality. This was supported by the analysis, which showed higher odds of adverse outcomes for young persons from families where the parents did not live together all 15 years of the young person's childhood. We hypothesised that PPSU would increase the odds of adverse outcomes, which was partly supported by the analysis, as young people not living with both parents and who experienced PPSU had higher odds of NEET, hospital admissions, mental disorders and criminality. However, young people living with both parents with PPSU only had higher odds of a few outcomes (illness, accidents, other disorders and property crime) compared with peers living with both parents without PPSU. This could indicate that PPSU primarily increases the likelihood of different adverse outcomes if it is present in families with other problems and conflicts leading to separation/divorce. But, as the present study did not include qualitative information about family dysfunction, this is only conjecture.
The hypothesis that living with a parent with problematic substance use for longer periods during childhood would be associated with worse outcomes was not supported by the results. Compared with the reference group, the highest odds of different adverse outcomes were observed among young people from Not both/+PPSU, brief families, not among young people from Not both/+PPSU, long families. Furthermore, the secondary analysis showed that young people from Not both/+PPSU, brief families had higher odds of not being employed or enrolled in education, having an accident-related hospitalisation, having a diagnosis of an anxiety disorder, as well as other kinds of diagnoses of mental disorders, and being convicted of property, drug-related and other crimes compared to the reference group, Both/−PPSU. First, it is important to recognise the limitation of the measure, which indicates years living with the parent and not necessarily with PPSU (discussed further in the section “Limitations”). Second, an explanation for the significantly higher odds of adverse outcomes among this group of young people could be the early timing of a break between the two parents. There is some evidence that the risk of adverse outcomes is higher for young people who experienced parental divorce in childhood compared with those who experienced parental divorce later (Hope et al., 1998), but other studies have not supported this finding (Amato, 2000; Strohschein, 2005). Another explanation could be the level of family dysfunction and the severity of substance use, which are variables not included in this study. Higher levels of family dysfunction and more severe substance use may contribute to a decision to separate shortly after the child's birth. Thus, the level of family functioning during childhood may be more important than whether the child lives with the parent (Amato, 2000; van Dijk et al., 2020). In families with a lot of conflict and problems, the parent with problematic substance use may still have an important impact on the child, even though they do not live together. This is supported by studies demonstrating that parental problems have an effect on externalising behaviours over time and that family functioning mediates the relationship (Finan et al., 2015; Park & Schepp, 2015). The importance of taking the parent-child relationship, disruptive social changes and family conflict into account in the analysis was also demonstrated by an Icelandic study, which showed that the higher risk of adolescent cigarette and alcohol use among those with parental divorce was explained by the family environment (Kristjansson et al., 2009). Furthermore, it is likely that it is instability in the family structure, and not the structure itself, that is associated with adverse outcomes (Bzostek & Beck, 2011; Shaw et al., 2019). In this way, the children are not only experiencing PPSU and parental separation but also high levels of conflict and family dysfunction. Different studies of adverse childhood experiences (ACEs) have shown how ACEs not only affect the children's physical and mental health but also the risk of negative life course outcomes (Hansen et al., 2021; Hughes et al., 2019; Shin et al., 2018).
However, in some contexts, the family structure may have the opposite impact. For instance, Shaw et al. (2019) studied justice-involved children in Florida and found a lower risk of past-30-day opioid misuse among children living in single-parent households compared with those in two-parent and grandparent-only households.
Other factors that could be important when examining the adverse outcomes in young adulthood include the type (alcohol vs. illicit drugs) and severity of parental substance use. Kuppens et al. (2020) conducted a meta-analysis of the longitudinal relationship between PPSU and child well-being (including studies from North America, Europe, Australia, Asia and South America) and concluded that alcohol use (both dependent and not) was as harmful as tobacco use, while parental drug use had the strongest effect on child well-being. In the present study, information about substance type was only available for some of the measures (e.g., drug vs. alcohol-related diseases or disorders), but this could be a relevant aspect to incorporate in future analysis.
In the present study, we expected to find a positive association between years living with the parent with problematic substance use and adverse outcomes. Instead, the results indicated how PPSU in families where the parents did not live together early in the young person's childhood influenced the situation in young adulthood. In a prior study based on the same population, we identified the following four groups of families with different levels of family and parental problems, including PPSU (Frederiksen et al., 2022): (1) families with a low level of problems; (2) families with primary PPSU as a problem; (3) families with primary long-term unemployment (and not PPSU) as a problem; and, lastly, (4) families with a high level of problems including PPSU. The study investigated associations between family type and school outcomes, including the grade point average from the final examination in mandatory school. In the present study, the aim was to investigate PPSU as a separate risk factor in more detail to determine whether greater exposure to the parent with problematic substance use was associated with poorer outcomes for the child. But this seems not to be the whole picture, and other factors also contribute.
Limitations
As mentioned in the “Methods” section, the measure of PPSU only captured if the parent had problematic substance use at a point during the young person's life before the surveys were conducted. The measure of living with (or apart from) the parent with problematic substance use during childhood was based on register data indicating whether the parent and child lived together each year and does not necessarily indicate the number of years living with PPSU. That is, this does not mean that the parent was necessarily using substances during the exact years when the child was living with the parent. The survey data did not include information about the duration of PPSU. For instance, a young person may have lived together with their father all 15 years, and the father started having obvious problems with drinking when the young person was 10 years old. In addition, some alcohol-related diagnoses may not coincide with the time of drinking, such as alcohol-related liver disease, which may only occur after many years of heavy drinking.
Another limitation is a lack of information about family dysfunction, family relations and conflicts. The surveys did cover some aspects of these issues (e.g., questions about parental support and conflict), but survey data would only provide information about the participants and not the non-participants, a group which is more likely to have experienced severe PPSU (Frederiksen et al., 2021).
Implications
The study showed how PPSU can be associated with adverse outcomes, especially in combination with other problems, such as early parental divorce and a brief period of living with the parent with problematic substance use. Further investigations of young people from different kinds of family structures are needed to clarify if it is the level of family dysfunction which is the dominant factor; however, this was not a part of the present study. When social welfare and healthcare professionals are in contact with young people, it is important that they not only consider PPSU, but also the interplay with family environment, dysfunction and relations and how this affects the well-being of the young individuals. In the same way, it is important to be in dialogue with parents who enter alcohol and drug treatment about how children are affected by PPSU (Selbekk, 2019). The evaluation of tools to support this dialogue could be an interesting subject for future research, not only to facilitate the discussion with the children involved and other family members, but also to focus on the impact of the substance use problems on the family. Some methods have already been developed, such as the five-step method by Copello et al. (2010), by which counsellors can provide relevant information, discuss social support and facilitate contact with other sources of specialist help. Another method is Community Reinforcement and Family Training (CRAFT) (Smith & Meyers, 2004), which is a programme that teaches family members to change their own behaviour and target problems in different aspects of their lives in ways that encourage the individual with problematic substance use to seek treatment or to reduce their substance use.
Furthermore, when PPSU is detected, preventive interventions should direct attention towards decreasing the risk of NEET and mental disorders, as well as the risk of criminality. The higher odds of hospital admissions among young people with PPSU also suggest that hospitals could be an appropriate setting to conduct screenings for PPSU to ensure these young people receive proper help.
Conclusion
The odds of adverse outcomes in young adulthood were lowest among young people living with both parents without PPSU. The highest odds of adverse economic, health, mental health and criminal justice problems were found among young people not living with both parents and living with a parent with problematic substance use for 0–4 years. These results demonstrate the importance of considering the interaction between different aspects of family structure and PPSU when considering long-term outcomes for children.
Supplemental Material
sj-docx-1-nad-10.1177_14550725221143177 - Supplemental material for Problematic parental substance use, childhood family structures and adverse outcomes in young adulthood
Supplemental material, sj-docx-1-nad-10.1177_14550725221143177 for Problematic parental substance use, childhood family structures and adverse outcomes in young adulthood by Kirsten Søndergaard Frederiksen, Morten Hesse and Mads Uffe Pedersen in Nordic Studies on Alcohol and Drugs
Footnotes
Acknowledgements
The authors wish to thank Julie Brummer, who assisted with the proofreading of the manuscript and with valuable comments and suggestions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by a block grant under the Danish budget law to finance the Centre for Alcohol and Drug Research, and a PhD scholarship granted to KSF.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.