
Abstract
Introduction
Over the past 20 years, the number of children in out-of-home care (OHC) has increased in Finland (Forsell et al., 2021). Approximately 19,000 children were in OHC in 2020 (Forsell et al., 2021). Population statistics and register data show that approximately 89,000 underaged children have at least one parent with a severe substance use problem (Raitasalo, 2024). This represents approximately 9% of all children and is consistent with similar estimates from other countries (Kraus et al., 2021; Ramstedt, 2019).
Several studies show that parental problematic substance use (PSU) is often a reason for placing small children in OHC (English et al., 2015; Heino et al., 2016). Raitasalo et al. (2014) found that in Finland 27% of children who had a mother with register entries related to alcohol problems and 13% with a father with these register entries had been placed in OHC at least once before their seventh birthday. As much as 57% of children with a mother with alcohol or drug problems were placed in OHC at this age. Among other children, the proportion was 1%.
PSU and other social problems have typically been associated with suburban areas dominated by multi-storey housing in Finland. For example, problems that have emerged in such suburbs built in the 1960s and 1970s have been associated with their remote location, difficulties in access to services and poor housing market status (Stjernberg, 2019). Rootlessness, social isolation, loneliness and youth problems have raised concerns and they have often been associated with PSU. In present-day Finland, social disorder is more common in neighbourhoods dominated by multi-storey housing, particularly in the suburbs built in the 1960s and 1970s, compared with low-rise neighbourhoods (Kemppainen, 2017). These observations are associated with differences in socioeconomic disadvantages between residential areas. As both somatic and psychological morbidity (Pickett & Pearl, 2001; Richardson et al., 2015) and mortality (Meijer et al., 2012) have been shown to be higher in deprived areas, the need for health and social services, including substance use and child welfare services, can be assumed to be higher.
The image of an association between social problems and substance use in the suburbs is strong despite a lack of generalisable scientific evidence. However, research evidence suggests that certain characteristics of disadvantaged neighbourhoods, such as low income level (Kunnas, 2013) and high unemployment rate (Karvonen & Rimpelä, 1997), are associated with harmful health habits, such as alcohol use. Ahern et al. (2008) found that a neighbourhood’s culture of alcohol use impacted an individual's propensity to drink. Another study showed that a one-percentage-point increase in the proportion of residents living in poverty was associated with 86% higher odds of binge drinking (Cerda et al., 2010). Still, living in disadvantaged neighbourhoods per se does not seem to increase the risk of PSU (Karimo, 2018; Karriker-Jaffe, 2011).
Many studies have shown the negative association between neighbourhood disadvantage and the well-being of children and families (Minh et al., 2017). In the US and Canadian contexts, OHC is more common in disadvantaged neighbourhoods (Esposito et al., 2013; Lery, 2009), but the parents’ socioeconomic characteristics have not been controlled for in these studies. Research is needed from more varied contexts and with more efforts on controlling for family characteristics.
Even if the adverse effects of parental PSU on children has been documented (Rossow et al., 2016), there is a lack of research on whether the association between parental PSU and outcomes such as children's OHC varies across neighbourhoods. For example, parental PSU could impair parental oversight, which may have different consequences in different neighbourhoods (Rankin & Quane, 2002). Alternatively, neighbourhood disadvantages may influence how child welfare services interpret the cases.
The aim of the present study was to shed light on the associations between neighbourhood characteristics, parental PSU and children's OHC. Using register data, we explore the spatial concentration of parental PSU and children's OHC in differnt kinds of urban areas.
We have two research questions: (1) Is the prevalence of parental PSU and children's OHC similar in different types of neighbourhoods? and (2) Is the association between parental PSU and children's OHC similar regardless of neighbourhood characteristics?
Methods
Study design
The data is retreived from Finnish administrative registers and covers all children born in Finland in 2002 (N = 55,007) and their biological parents. We restricted our scope to include children born and living for at least 1 year in cities participating in the governmental programme funding research and development in suburban neighbourhoods. A total of 14 Finnish cities with the largest population in 2019 were included. The children (n = 24,271) and their biological parents were followed from the child's birth until the child's first OHC episode (n = 1,008) or until the age of 18 years or a censored event [drop out from housing data (n = 107), moving away from the study area (n = 8,233)], whichever came first.
There were 145 children lost to follow-up during their first year and 23 children who had not lived with either biological parent for 1 year during the follow-up time. Information from mothers was available for all children; for 99% of the children, the father's records were available from the Population Register. The final data included information on 23,788 mothers and 23,242 fathers. We did not control for moving between or within cities.
The study used individual-level data from Finnish healthcare and social welfare registers (Sund, 2012), which include annual data on the whole population during the follow-up. First, the personal identity numbers (assigned to all Finnish residents at birth or upon residency) of children in the study population and their biological mothers were obtained from the Medical Birth Register. The Population Register was used to obtain the personal identity numbers of fathers. The Child Welfare Register was used to detect whether the children had been placed in OHC before their 18th birthday. To detect where the child and their parents lived, we compared the unique building codes and the dates of moving in and out of the specific building by utilising the Digital and Population Data Services Agency data.
Data obtained from Statistics Finland were used to measure the sociodemographic characteristics of neighbourhoods. The neighbourhood delimitation was based on administrative sub-divisions of the cities, and the average total population of the neighbourhoods was approximately 3,000 residents.
Different datasets were linked via personal identity numbers. The register keepers at the Finnish Institute for Health and Welfare (THL), the Social Insurance Institution of Finland and Statistics Finland carried out the data collection and linkages as well as anonymisation of the data. The study plan was approved by the Ethical Review Board of the Finnish Institute for Health and Welfare.
Measures
Outcome: out-of-home care (OHC)
Being placed in OHC by child protection services was defined as the first care episode during the follow-up from birth until the child's 18th birthday.
Exposure: parental problematic substance use
Parental PSU was detected using the Care Register for Health Care, the Care Register for Social Welfare, the Prescription Register and the Causes of Death Statistics. The parents were defined as having PSU if they had received any primary or secondary International Classification of Diseases [ICD]-10 diagnosis 1 (ICD, 2019) or a record of inpatient or specialised outpatient treatment related to alcohol or drug abuse or any register entry on purchases of medication for the treatment of alcohol or drug abuse (N07BB and N07BC according to the Anatomical Therapeutic Chemical Classification System, ATC) (WHO, 2024), or had died with a diagnosis related to PSU during the follow-up (Raitasalo et al. 2014). PSU was classified into the mother's PSU alone, the father's PSU alone and both parents’ PSU. Alcohol and drug abuse were combined into a single measure of PSU.
Covariates
Our analysis considered time-invariant and time-varying covariates. Time-invariant individual-level covariates included parents’ psychiatric disorders, education and financial difficulties. Parents were classified as having psychiatric disorders (PDs) if they, during the follow-up, had any primary or secondary ICD-10 diagnosis 2 or a record of inpatient treatment related to PDs (schizophrenia, schizotypal and delusional disorders, mood disorders, neurotic, stress-related and somatoform disorders, and adult personality and behaviour disorders) in the Care Register for Health Care or the Care Register of Social Welfare.
The parents’ education was obtained from the Register of Completed Education and Degrees and was used dichotomously: any recorded education after comprehensive school (i.e., any post-compulsory education) or not.
Financial difficulties in parents were defined as having received social assistance (a last-resort benefit) for more than 3 months per year for at least 3 years during the follow-up. These data were obtained from the Social Assistance Register. The prevalence of the outcome, exposure and the individual-level covariates are presented in Table 1.
The proportion and number of children with parents with PSU, PDs, no education after primary school and long-standing poverty (n = 24,271).
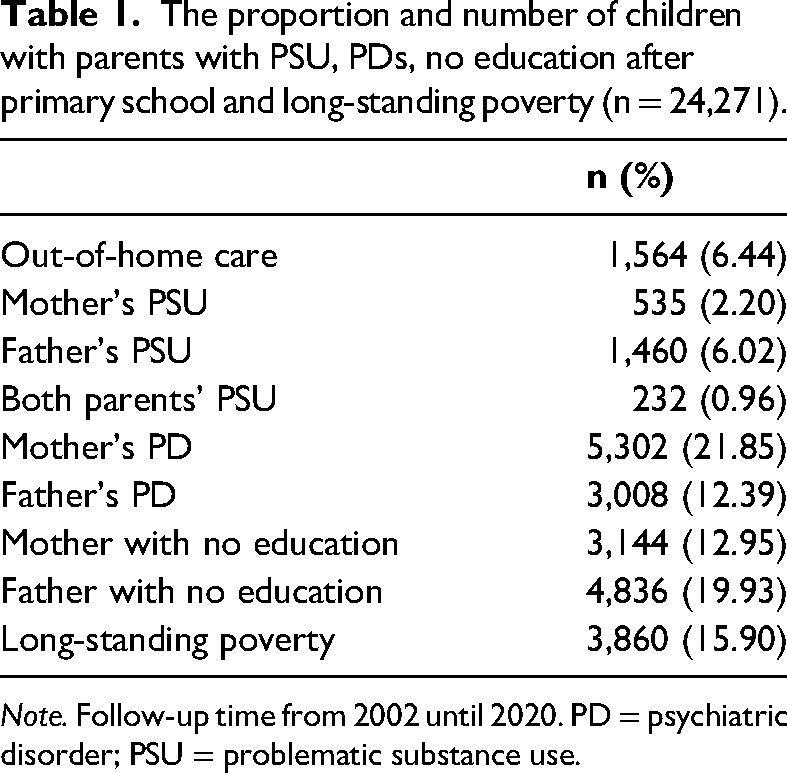
Note. Follow-up time from 2002 until 2020. PD = psychiatric disorder; PSU = problematic substance use.
Time-varying covariates related to neighbourhoods included the neighbourhood type, which was divided into city centres, suburbs and peri-urban areas. The delimitation of the city centres was based on the centre classification of the Finnish Environment Institute (Helminen, 2011). Suburbs were defined as inner or outer urban areas of the cities not belonging to the centres of the urban regions, based on the urbanicity classification of the Finnish Environment Institute (Helminen et al., 2020). Peri-urban areas are an intermediate category between urban and rural area types. The biggest proportion of children in our data lived in the suburbs (mean = 83.64%; range 81.93% in 2002 to 84.13% in 2009). In city centres, the corresponding figures were 8.07% (mean), ranging from 6.79% (in 2013) to 12.16% (in 2002), and in peri-urban areas, 8.29% (mean), ranging from 5.91% (in 2002) to 9.15% (in 2012).
The data included several time-varying sociodemographic characteristics of the neighbourhood population (proportion of inhabitants with low income, without employment, without secondary education, with an immigrant background and single-parent households). We used low income (the share of the population belonging to the lowest national quintile of equivalised disposable household income) as an indicator of socioeconomic deprivation in the neighbourhood. The different neighbourhood-level variables were mostly positively correlated with each other (Supplementary Table 1) and had similar associations with children's OHC (Supplementary Table 2) and parental PSU (Supplementary Table 3). As the share of the low-income population was equal each year at the national level (20%), we avoided the problem of effects due to a changing general level of the neighbourhood-level variable getting confounded with effects related to the ageing of the children.
In addition, we used the proportion of dwellings in multi-storey buildings in the neighbourhood to measure the type of urban design.
The proportions of low-income residents and dwellings in multi-storey buildings were measured each year from birth until the end of the follow-up, until the first OHC occurred or until censored. The mean proportion of low-income residents was 17.24%, ranging from 16.93% (in 2011) to 17.53% (in 2003 and 2019), and the mean proportion of dwellings in multi-story buildings was 53.22%, ranging from 50.64% (in 2013) to 59.64% (in 2002).
Statistical analysis
For descriptive purposes, cross-tabulation with chi-square tests were used. As we have data on the time of OHC and time-varying variables related to the residential area, multi-level Cox proportional hazards modelling with the PHREG procedure in SAS (SAS Institute, 2018) was used to assess the association of neighbourhood characteristics and parental PSU with children's OHC. The counting process method for time-dependent covariates (Powell & Bagnell, 2012), with separate lines for each time interval during which all covariates remain constant, was applied. To consider the different urban structures of our study cities and possible variation over the years in study variables, the municipality and the study year were adjusted for in the final analysis. In addition, living with the mother/father/both at the time of OHC episode was controlled for. The results are presented as hazard ratios (HR) and adjusted hazard ratios (AHR). The multi-level specification, with municipal sub-areas (Statistics Finland, 2023) as a higher level above the individual level, takes into account the clustering of observations into sub-areas in the estimation of standard errors for the individual- and area-level variables (Leyland & Groenewegen, 2020).
The interaction effects of area type and parental PSU as well as neighbourhood characteristics on a child's risk of being placed in OHC were analysed to see whether there were differences in the effects between different area types. Pearson correlations and analysis of variance were used in the supplementary analysis for correlations between area-level sociodemographic characteristics and descriptive analysis of children's living areas according to children's OHC episodes and parental PSU (Supplementary Tables 1–3).
Results
The associations between different neighbourhood types and children's OHC and parental PSU were estimated by looking at OHC episodes in the three different kinds of neighbourhoods (centres, suburbs, peri-urban areas) between 2002 and 2020. Table 2 shows that over the whole study period, OHC was most common in the suburbs, where 6.5% of children had been placed in OHC at least once during the follow-up. The corresponding figure was 5.7% in city centres and 4.8% in peri-urban areas. There were no major differences between city centres and suburban areas regarding the prevalence of parental PSU. However, PSU by fathers alone was somewhat more common in city centres (6.8%) than in suburbs (6.2%) and peri-urban areas (4.7%).
The prevalence of at least one episode of OHC and parental PSU in children born in 2002 before their 18th birthday according to area type.
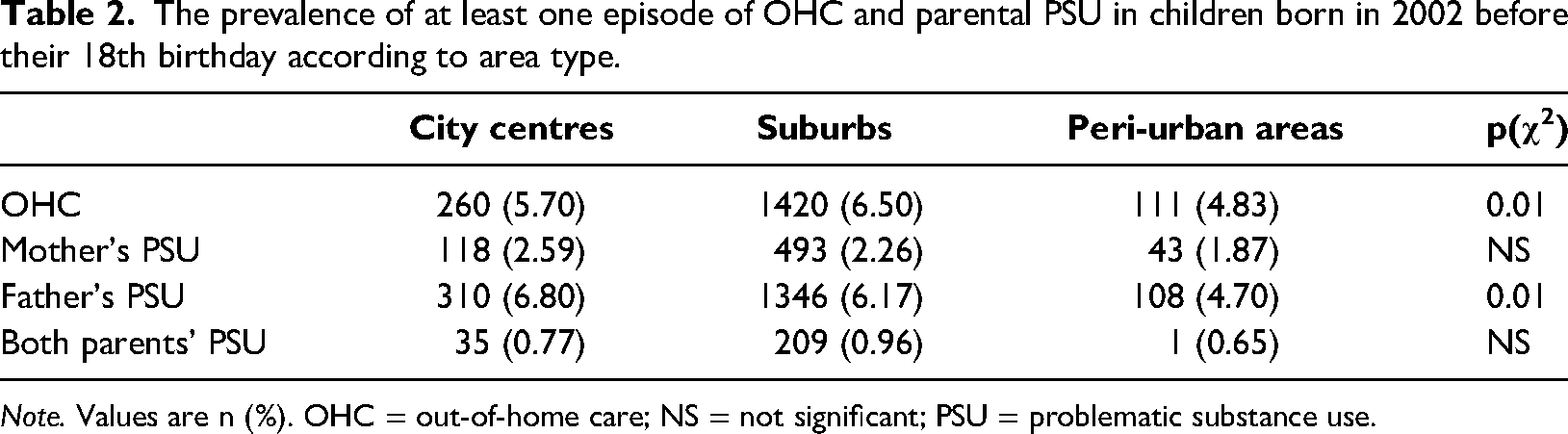
Note. Values are n (%). OHC = out-of-home care; NS = not significant; PSU = problematic substance use.
When looking at neighbourhood characteristics (Table 3), a similar picture is seen with children's OHC and parental PSU. The proportion of low-income residents was significantly higher (p < .0001) in city centres and suburbs than in peri-urban areas. Similarly, the proportion of dwellings in multi-storey buildings was lower in peri-urban areas than in other urban area types (p < .0001).
Mean prevalence of neighbourhood sociodemographic characteristics according to area type (2002–2020).

The results of the Cox regression analysis (Table 4) show that when other individual-level characteristics and area type were not adjusted for, the mother's PSU increased the child's risk of being placed into OHC (HR = 9.72, 95% confidence interval [CI] 7.92–11.93) compared with children with no parental PSU (Table 4, Model 1). The father's PSU had a smaller but statistically significant effect (HR = 3.42, 95% Cl 2.84–4.12). Both parents’ PSU increased the child's risk for OHC the most (HR = 42.79, 95% Cl 35.05–52.25). Adding parents’ PDs, education and the family's financial difficulties to the model considerably attenuated the effect of parents’ PSU. However, the effects remained statistically significant for all categories of parental PSU (Model 2). When the neighbourhood-level factors together with year and municipality were added (Model 3), the effect of parental PSU remained at a similar level than in Model 2 (mother: HR = 3.53, 95% Cl 2.80–4.46; father: HR = 1.38, 95% Cl 1.10–1.73; both parents: HR = 8.05, 95% Cl 6.38–10.16). The family's financial difficulties during the follow-up also increased the child's risk of OHC (HR = 4.29, 95% Cl 3.55–5.19) as well as parents’ PDs (mother: HR = 2.30, 95% Cl 1.98–2.68; father: HR = 1.44, 95% Cl 1.22–1.69). The mother's post-compulsory education decreased the child's risk of OHC (HR = 0.66, 95% Cl 0.57–0.77), whereas the father's education did not have a statistically significant effect. Finally, with all these adjustments, the child's risk of OHC was higher in the suburbs (HR = 1.76, 95% Cl 1.38–2.25) compared with city centres; peri-urban areas did not deviate from other types of neighbourhoods with this respect. The effect of the proportions of low-income residents and dwellings in multi-storey buildings in the neighbourhood were statistically non-significant.
Children's OHC according to individual-level characteristics, adjusted for area type, municipality and year (follow-up time from 2002 to 2020, from birth year until 18th birthday).
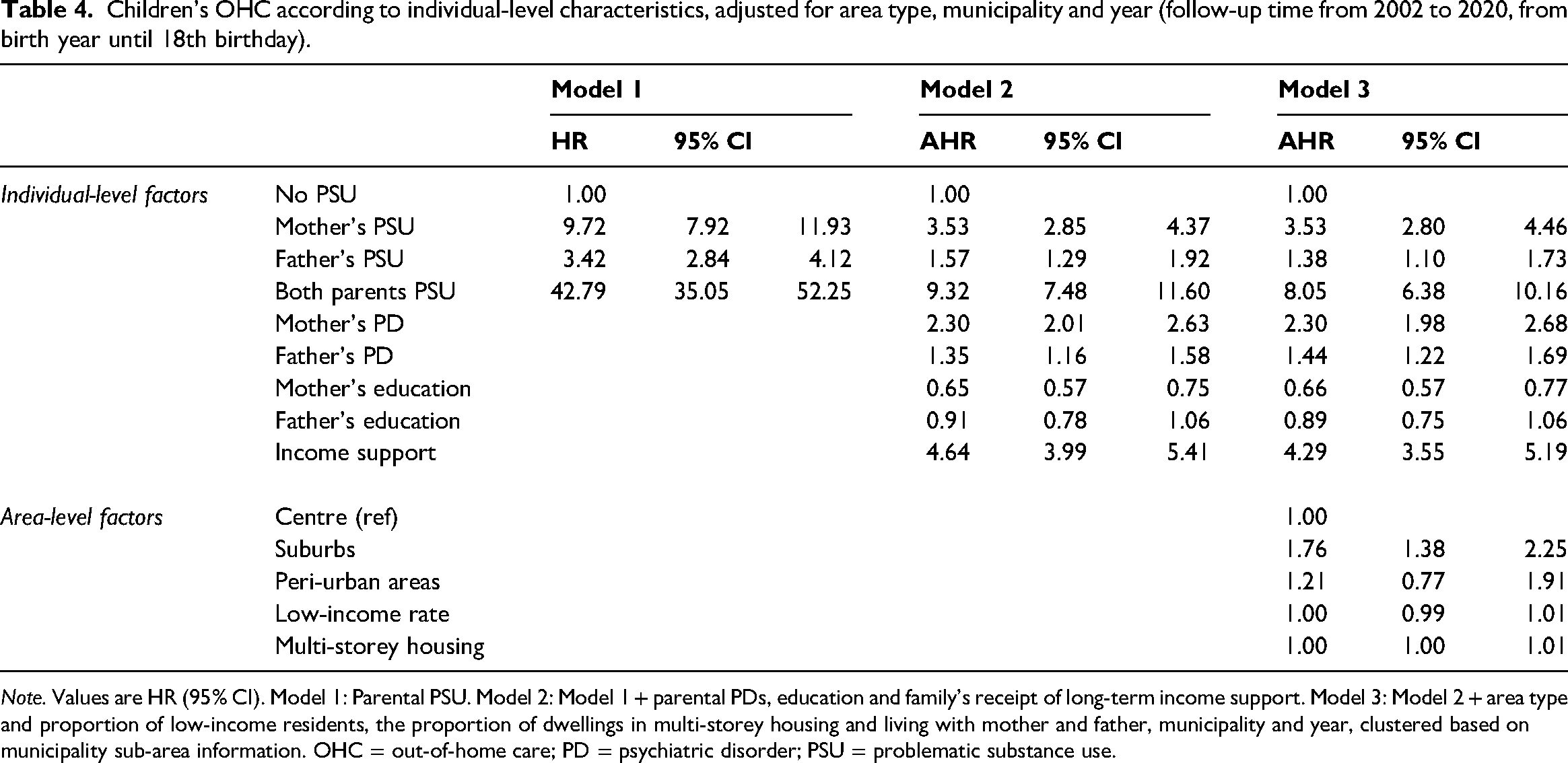
Note. Values are HR (95% CI). Model 1: Parental PSU. Model 2: Model 1 + parental PDs, education and family's receipt of long-term income support. Model 3: Model 2 + area type and proportion of low-income residents, the proportion of dwellings in multi-storey housing and living with mother and father, municipality and year, clustered based on municipality sub-area information. OHC = out-of-home care; PD = psychiatric disorder; PSU = problematic substance use.
To better understand how neighbourhood characteristics and parental PSU might be associated with children's risk of OHC, we elaborated on these effects in different areas. Interactions between (1) neighbourhood type and parental PSU, (2) the proportion of low-income residents and parental PSU, and (3) the proportion of multi-storey buildings and parental PSU were calculated. Table 5 shows that when adjusted for both individual and area-level variables, the interaction effect of parental PSU and neighbourhood type remained statistically significant (p = .015). The more detailed results showed that mother's PSU was associated with children's OHC only in suburban areas (p = .007, not shown in tables). The association between father's and both parents’ PSU and children's OHC was similar in all neighbourhood types when other parental problems and neighbourhood characteristics were also considered.
Interaction models in unadjusted and adjusted models, with children's OHC as the outcome.
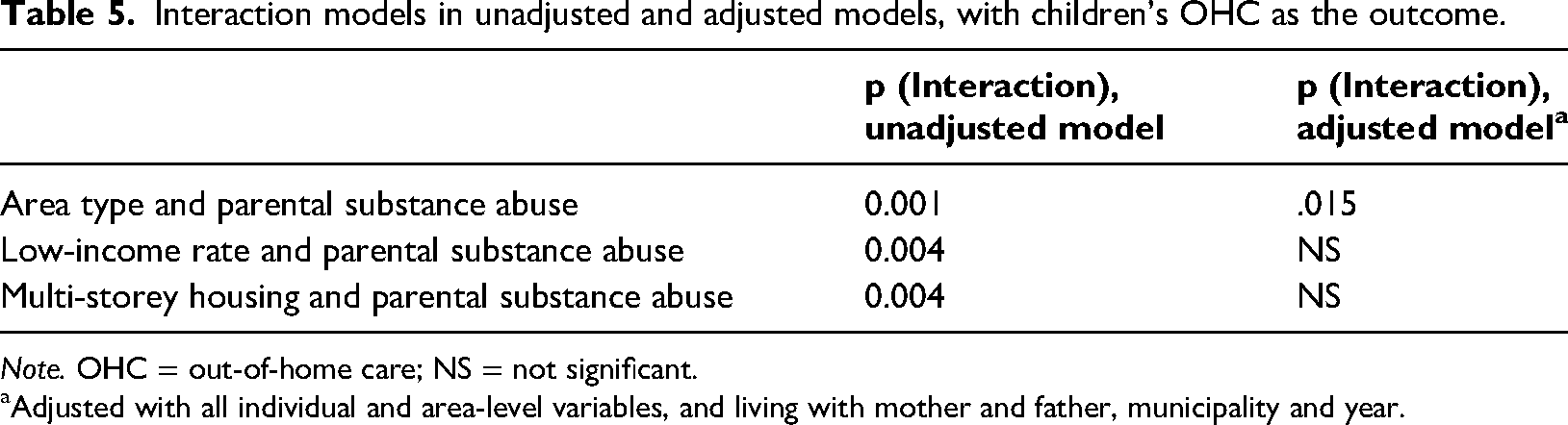
Note. OHC = out-of-home care; NS = not significant.
Adjusted with all individual and area-level variables, and living with mother and father, municipality and year.
Next, the analysis showed that the interaction between the proportion of low-income residents and parental PSU was statistically significant (p = 0.004) in the unadjusted model, specifically when the mother (p = 0.001) had a PSU problem. After adjustments, the effect attenuated to non-significant.
Finally, the interaction between the proportion of dwellings in multi-storey buildings and parental PSU was statistically significant (p = 0.004), the association being stronger if the mother had PSU in the unadjusted model. In addition, here the effect attenuated to non-significant after adjustments.
Discussion
Using population-level register data from 14 cities in Finland, we found that there were no major differences between city centres and suburban areas regarding the prevalence of parental PSU. However, children living in suburbs were more likely to be placed in OHC than children living in city centres or peri-urban areas. Having parents with PSU was associated with children's OHC before their 18th birthday, regardless of neighbourhood type or its characteristics. Still, the effect of a mother's PSU was more substantial in the suburbs. The proportions of low-income residents or those living in multi-storey buildings had no independent effect on the probability of placing children in OHC. Before adjustments, a higher proportion of low-income residents was associated with the child's risk of being placed into care, especially in suburbs and peri-urban areas, but the effect attenuated in the adjusted analysis.
The reasons for OHC are manifold, and can be related to the child, caregiver/parent, family or the context within which families live (English et al., 2015). Parents’ PSU, financial difficulties, health issues or other problematic behaviours, children's own problems and risky behaviours or difficulties in school attendance and studying, as well as family separation or the challenges of reconstituted families are among the most common reasons for placing children in OHC in Finland (Heino et al., 2016). The association between parental PSU and OHC is already established (Raitasalo et al., 2014; Sarkola et al., 2007). In this study, we found that there is spatial differentiation so that the risk of OHC, in general, is increased in suburbs regardless of parental PSU or other individual and area-level adversities. However, the effect of a mother's PSU is somewhat more substantial in the suburbs compared to other area types. The results reflect previous findings on the accumulation of adversities and deprivation in Finnish suburbs, which have been documented particularly concerning housing estates with large shares of rental housing (Kemppainen et al., 2018). In addition to financial difficulties, there may be, for example, PSU and health problems in families living in poor neighbourhoods (Halonen et al., 2012). Thus, children are exposed to accumulating adversities in their family and neighbourhood.
At least two possible mechanisms can be related to our findings. First, in deprived neighbourhoods, parents may need to make more effort to keep their children away from problematic behaviours, which may ultimately lead to OHC because of the child's own behaviour. For example, in the US context, parental control has been found to prevent delinquent behaviour, particularly in high-risk neighbourhoods, with some ethnic differences (Deutsch et al., 2012). PSU possibly weakens parental control over the child's behaviour, which may explain the stronger association between parental PSU and OHC in low-income neighbourhoods. Second, parents with PSU problems, and even more so if living in deprived neighbourhoods, may end up spending time with other people with similar problems, which may lead to worsening of problems also reflected in their children. This, again, may increase the probability that the children will be placed in OHC.
Our findings are in accordance with studies on alcohol-related harm. The so-called alcohol-harm paradox posits that people of low socioeconomic status (SES) tend to experience greater alcohol-related harm than those of high SES, even when alcohol consumption does not differ (Bloomfield, 2020). Similar associations have also been observed in studies on alcohol's harm to others (Laslett et al., 2012; Sundin et al., 2021). This line of reasoning could explain why children with parental PSU in more deprived areas more often experience problems that lead to child welfare measures than in wealthier areas.
Fewer protective factors may also explain the observed differences against family adversities in certain neighbourhoods. Previous literature shows that the neighbourhood’s social context appears essential for child and adolescent well-being (Sellström & Bremberg, 2006; Vyncke et al., 2013). For example, child maltreatment rates are lower in neighbourhoods with higher levels of positive social processes (e.g., collective efficacy, intergenerational disclosure, social networks) and lower levels of social and physical disorders (Molnar et al., 2016). If suburbs lack these neighbourhood-level protective factors, parental problems, including PSU, may have more harmful effects on children living in suburbs (Kemppainen, 2017). Unfortunately, our data did not include information on this. On the other hand, it may be that in the suburbs, personnel in daycare centres, schools, healthcare or child welfare services are more alert and conscious so that possible problems are more easily noticed and intervened.
The area-level differences in the availability of services for children and families should also be considered. Still, research on these kinds of inequalities between different kinds of urban areas is lacking. For example, in Finland there have been concerns that child-welfare services take the place of missing PSU and psychiatric services for adolescents and other specialised services for families. However, these services cannot replace one another but should instead be complementary and work together multi-professionally. Whether there is evidence of differentiation in the availability of services for adults and adolescents in different kinds of areas should be further studied as this kind of development may deepen segregation.
Strengths and limitations
A strength of our study is that the register data offer a possibility to study entire cohorts, hard-to-reach populations and complex phenomena at low costs and without the problems of response rates. The register data eliminate social desirability bias as it is based on diagnoses and evaluations made by professionals.
The main limitation is related to the underrepresentation of alcohol and drug abuse in the register data. Parents with PSU who have not used the treatment services included in the registers are not represented. Our data thus reach only the “tip of the iceberg” of the phenomenon; registers do not include data on persons with occasional abuse of substances or those who have not ended up in treatment (Gissler & Haukka, 2004; Pirkola et al., 2006). Thus, we do not know whether the effect of parents’ problematic substance use that has not led to use of services is similar to the effects found in this study.
Another limitation is that it was not possible to control for all relevant sociodemographic factors, such as the parent's employment status or income level. As we only had data on biological parents, we do not know whether the child was living in a family where a social parent, such as the mother's or father's new spouse, abuses substances. Finally, our data do not allow examining familial dysfunctions, such as child maltreatment and abuse, which also adversely affect children (Anda et al., 2006) and are related to placing children in OHC. Previous research has shown that children with parental PSU have a higher risk of different types of abuse and neglect (Walsh et al., 2003), which probably mediates the association between parental PSU and placing children in care. Many characteristics regarding the study areas – that cannot be measured using register data – may influence family adversities and children's risk of OHC.
Confusion over the direction of causation due to selection bias, that is, the non-random selection of people into neighbourhoods, is one of the most important methodological limitations for interpreting statistical associations between neighbourhood factors and health (e.g., Sampson et al., 2002). As the factors possibly affecting the selection into neighbourhoods and the children's OHC are not fully known or controlled for in this study, the associations between neighbourhood factors and OHC should not be considered as indications of causal effects.
Conclusion
There are several possible interpretations for our findings. Parental PSU may precede children ending up both living in disadvantaged neighbourhoods and OHC. On the other hand, parents’ financial difficulties may be behind all these. It is also possible that some mechanisms other than parental substance use problems mediate the association between neighbourhood characteristics and OHC. More research is needed to identify these possible mediators.
Our findings suggest that to prevent adverse living conditions that lead to OHC, accessible and effective interventions must be made available for families who experience PSU in all kinds of neighbourhoods, especially in suburbs with sociodemographic deprivation. As parental PSU is a complex problem that often is intertwined with other life challenges, such as financial difficulties and mental health problems, it is not sufficient to treat caregiver conditions such as PSU in isolation from other factors; instead, it is essential to provide services that increase positive, pro-social connections that may be lacking in the neighbourhood where the family lives.
Supplemental Material
sj-docx-1-nad-10.1177_14550725241270203 - Supplemental material for Children’s out-of-home placements: Associations with parental substance use and neighbourhood sociodemographics
Supplemental material, sj-docx-1-nad-10.1177_14550725241270203 for Children’s out-of-home placements: Associations with parental substance use and neighbourhood sociodemographics by Kirsimarja Raitasalo, Karoliina Karjalainen, Sanna Kärkkäinen and Timo M Kauppinen in Nordic Studies on Alcohol and Drugs
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Suburban development programme by the Finnish Ministry of the Environment,
Supplemental material
Supplemental material for this article is available online.
Correction (January 2025):
Since the original online publication, redundant text has been removed from page 545.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.