
Abstract
Keywords
Substance use and substance use disorders (SUDs) among young people are one of the major global risk factors today for negative health outcomes (Degenhardt et al., 2018; NIDA, 2020; NIDA, 2020; Schulte & Hser, 2014). In addition to physical and mental health consequences, SUDs have been strongly associated with negative behavioural consequences such as violence victimisation and perpetration, low educational attainment and delinquency (Cafferky et al., 2018; Deas, 2006; Green et al., 2016; Pedersen et al., 2018; van Ours & Williams, 2009). These important consequences call for efforts to reduce SUDs among adolescents and young adults. One way to reduce adolescent SUDs is evidence-based treatments for adolescent SUDs, which have demonstrated positive outcomes in adolescents (Tanner-Smith et al., 2013; Winters et al., 2018), and in many studies these treatment gains are sustained over time (Winters et al., 2018). However, the effect of treatment and the level of recovery may be influenced by a number of different factors, including age, sex, parental support, family circumstances, ethnic minority status, co-morbidity with mental disorders and adverse experiences (Bachrach & Chung, 2021; Brunelle et al., 2013; Green et al., 2020).
The association between adverse experiences and treatment outcomes
Adverse experiences typically refer to potentially traumatic events in childhood and adolescence, such as physical abuse, sexual abuse and neglect. Among patients in treatment for drug use disorders, approximately half report at least one type of childhood abuse or neglect (Anderberg & Dahlberg, 2016; Garner et al., 2014; Huang et al., 2012; Lotzin et al., 2016). In comparison, a recent meta-analytic study of child maltreatment experiences in the general population showed that the overall prevalence of self-reported child maltreatment was in the range of 12%–36%, depending of the type of maltreatment (Stoltenborgh et al., 2015). More than other types of adverse events, experiences of child maltreatment have been linked to a range of negative consequences and have been shown to have far-reaching negative effects on individuals’ development and well-being (Buckingham & Daniolos, 2013; Carr et al., 2020; Felitti et al., 1998; Reading, 2006; Zielinski, 2009). In light of the detrimental consequences of adverse childhood experiences, researchers have stressed the importance of taking adverse childhood experiences into account as influencers of SUD treatment effects (Brents et al., 2015; Funk et al., 2003; Najavits & Hien, 2013). An increasing number of studies have examined the effect of adverse experiences in childhood and adolescence on SUD treatment outcomes (Derefinko et al., 2019; Funk et al., 2003; Hyman et al., 2008; Karsberg et al., 2021; Shane et al., 2006), and although results are mixed (Garner et al., 2014), there are strong indications that stressful experiences in childhood and adolescence are important influencing factors for treatment outcomes. However, how and to what extent adverse experiences affect individuals after drug use treatment is less clear.
Measuring treatment trajectories
The majority of research on treatments for SUDs has focused on the extent to which interventions reduce drug consumption, with one or more indicators of substance use as the primary outcomes. However, as argued by multiple researchers, the recovery trajectories and outcomes after treatment should not be measured and described by abstinence and treatment adherence alone (Garner et al., 2014; Hser & Anglin, 2011; Hser et al., 2007). Treatment represents only one of the paths to recovery. In recent years, conceptualisations of the term “recovery” have shifted to emphasise the broader biopsychosocial process of improvement that is related to, but not only determined by, substance use (Dodge et al., 2010; DuPont et al., 2015). There appears to be increasing consensus that recovery means more than just a reduction in substance use. Rather, it involves achieving benefits in a wide range of life areas, such as personal relationships, housing, health, employment and offending (DuPont et al., 2015; McQuaid et al., 2018). As such, factors are often addressed and targeted in treatment for SUDs, it seems relevant to define and measure these factors as treatment outcomes.
Treatment outcomes: not being employed or in education or training (NEET) and mental health
Employment and mental health have been emphasised as important indicators for recovery after treatment for SUDs (Martinelli et al., 2020; McLees et al., 2015). Research has shown that employment can prevent relapse after treatment (Henkel, 2011; McLellan et al., 2005; Pasareanu et al., 2015). Employment has both economic and non-economic benefits for recovering individuals, as it provides economic stability and is also a gateway into a productive social network (Laudet et al., 2002; Leukefeld et al., 2007; Walton et al., 2003). Besides the positive influence on reducing the substance use, studies have demonstrated additional benefits of employment, such as a reduction in homelessness, criminality, infectious diseases, as well as mental and physical health (Leukefeld et al., 2007; McLellan et al., 2005; Walton et al., 2003). Conversely, NEET is associated with lower personal and social well-being (Baggio et al., 2015). NEET youth report poorer health and lower social trust and activity (Nordenmark et al., 2015) as well as higher odds of depression and lower life-satisfaction (Minh et al., 2020). Mental health problems have also been positively associated with the risk of relapse after treatment for SUDs (Bradizza et al., 2006; Brunelle et al., 2013). Mental health and well-being are fundamental in everyday life and have a far-reaching impact on an individual's perception of quality of life (Rajmil et al., 2009). Patients with mental health issues often have lower levels of functioning (Pedersen et al., 2018; Winters et al., 2018), and those with dual diagnoses have an elevated risk of complications, such as relapse (Bradizza et al., 2006), elevated hospitalisation rates and shorter life expectancy (Lotzin et al., 2016; Tanner-Smith et al., 2013). Since employment and mental health are important factors for overall recovery and societal functioning after treatment, we sought to examine whether adverse events would have an impact on these outcomes after treatment for SUDs.
The present study
The present study examined three adverse experiences in childhood and adolescence as potential predictors for NEET and acute mental health problems two years after enrolment for SUD treatment. The research question for the present study was “Are past adverse experiences (i.e., physical abuse, sexual abuse and parental SUP) predictors of NEET and acute contact to psychiatric services two years after SUD treatment after controlling for treatment response (i.e., abstinence) and a range of other potentially influential factors (i.e., age, sex, ethnicity, treatment condition)?”
Based on previous findings that associate child maltreatment experiences with negative psychiatric effects and lower employment rates, we expected to find that exposure to the adverse experiences would be positively associated with both NEET and acute contact to psychiatric services two years after treatment.
Methods
Setting and participants
The participants were drawn from two sources: (1) a four-arm randomised controlled clinical (RCT) trial (Pedersen et al., 2021) that examined the effects of a 12-session motivational enhancement and cognitive behavioural therapy (CBT)-based intervention; and (2) a post-trial phase of the RCT, when treatment components were implemented in day-to-day practice. Initially, there were 778 young people from these sources. However, we excluded 198 following a criterion of minimal exposure to treatment. The minimum level of exposure was defined as attending at least three treatment sessions. This decision was made as the analyses focused on examining recovery beyond treatment exposure. Thus, the final sample in the present study consisted of 580 adolescents and early adults aged 15–25 years receiving treatment for problematic drug use.
Participants for both the RCT and post-trial stage were eligible if they were aged 15–25 years and had contacted the treatment centre with the intention of entering treatment for their drug use disorder. Patients were excluded from the RCT if they sought treatment for an opioid use disorder, had known active psychotic disorders, known cognitive deficits and/or were otherwise deemed not safe to participate (e.g., had recently engaged in violent actions against staff).
Ethics
The study was conducted in accordance with the Declaration of Helsinki and approved by the Danish Data Protection Agency and the Regional Committee for Medical and Health Research Ethics for the Central Denmark Region. The study protocol was sent to the regional ethics committee of the Capital Region of Denmark (No. 1-10-72-177-14). In Denmark, parents or caretakers of youth aged below 18 years have to provide informed consent for children's participation in health scientific research. However, the Ethics Committee for Medical and Health Research Ethics can dispense from explicit parental signed informed consent for research involving youth aged 15–17 years, depending on the aim of the study, the study design and the potential harm of the study. For the present study, such exemption was given. For adolescents aged 15–17 years, parents were informed about both the treatment and the research project and in accordance with the ethical approval, consent was implied. All participants signed an informed consent form.
Procedures
In total, 53 counsellors received training in one of the four treatment conditions in the RCT, and 46 provided treatment to one or more patients during the study. The training took place over two four-day workshops, and all counsellors received supervision throughout the study on a regular basis. The training and supervision were carried out by two Danish psychologists specialised in SUD treatment and with substantial experience with motivational interviewing (MI) and CBT. Between September 2014 and May 2016, patients were invited to participate in the RCT. In the RCT, patients were randomised to one of four treatment conditions: (1) standard (MI and CBT); (2) standard + reminders; (3) standard + vouchers + low-intensity aftercare; and (4) standard + reminders + vouchers + low-intensity aftercare) based on age, gender and use of cannabis and other illicit drugs in the last 30 days. In the post-trial phase lasting from May 2016 to October 2017, all eligible patients were asked if they would consent to the use of their assessment data for research purposes and quality assurance. In the post-trial phase, participants received the treatment condition that included both reminders, vouchers and low-intensity aftercare, but in a less strict version than in the RCT.
Treatment conditions
Patients in all four treatment conditions were offered 12 treatment sessions of 50–60 min each. The standard condition followed a manualised treatment with a combination of CBT and MI (Pedersen et al., 2021; Socialstyrelsen, 2020). In the other three treatment conditions, participants also received vouchers for attendance, reminders of sessions, or both vouchers and reminders (Socialstyrelsen, 2020). In the first three sessions for all conditions, the main focus was establishing treatment aims, which were centred around substance use, but also included aims for social network, communication, living situation, education/employment and coping skills. In the following nine sessions, the treatment aims were the focus in sessions and therefore not only substance use, but also a range of related factors were targeted in the treatment.
Measures
All patients were assessed using the YouthMap assessment form (Pedersen et al., 2016) during the first counselling session of the RCT. The YouthMap assessment form is a comprehensive assessment tool, tailored for young people in treatment for SUDs. The YouthMap covers background information, current substance use, past and current behavioural and mental problems, victimisation experiences, peer and family relations, and a range of other relevant behavioural and psychosocial measures. In addition, during the treatment course, participants were assessed in all sessions with the well-being and outcome monitoring (WOM) screening tool (Frederiksen et al., 2019). WOM is a nine-item routine outcome monitoring tool inspired by the feedback informed treatment system (Miller et al., 2015), which monitors substance use, well-being, and everyday function level. All responses were entered into a secure web-based interface by the involved counsellors.
Lifetime exposure to adverse events
To measure exposure to sexual abuse, physical abuse and parental SUP, three items from the YouthMap survey were selected: (1) “Have you ever been the victim of sexual abuse?”; (2) “Have you ever been the victim of physical abuse?”; and (3) “Does one or both of your parents have (or has one or both of your parents had) a substance abuse problem, with the exception of cigarettes?” All items were dichotomised (yes/no).
Treatment response
Treatment response was measured as drug use abstinence at the last treatment session attended via the WOM measure as a binary variable.
Register-based outcomes
Denmark has population and healthcare registers with individual-level data on the entire population. These register data can be linked to survey participants and non-participants through a personal identification number (Thygesen et al., 2011). Different registers were used to obtain the following two outcomes of interest: (1) NEET status in the second year after treatment enrolment; and (2) acute contact to psychiatric services within the two years after treatment enrolment.
For NEET, we extracted data from The Employment Classification Module, which contains the primary source of income in a given year (Petersson et al., 2011). Participants who were not registered as having an income based on employment or education in the second year after treatment were categorised as being NEET. Adolescents aged 15 and 16 years (n = 26) were excluded from the NEET dataset since most individuals in this age group are not yet registered in the employment classification module. In addition, most individuals who are aged 15–16 years will be registered as active students in the mandatory public school regardless of their rate of attendance or academic performance, and therefore the register data referring to education among 15–16-year-olds were not considered good indicators of NEET status. Therefore, the analyses predicting NEET were based on 554 participants.
Acute contacts to psychiatric services were extracted from the mental health services section of the National Patient Register (Lynge et al., 2011). In the present study, we defined acute contact to psychiatric services as non-scheduled contact to psychiatric hospital departments and psychiatric referrals after hospital admissions. All acute contacts within two years after treatment enrolment for each participant were included. The reason for not including contacts by appointment (i.e., outpatient treatment) was that this type of contact may actually indicate positive social functioning through planned and preventive help-seeking.
Statistical analyses
After obtaining descriptive statistics, the main analyses consisted of separate multivariate logistic regressions to predict each outcome: NEET and acute psychiatric contacts. Both NEET and acute psychiatric contacts were dichotomised (i.e., NEET yes/no, any acute contacts to psychiatric health services in the two years following treatment enrolment (yes/no). In all models, the main predictor variables were three types of adverse experiences (i.e., physical abuse, sexual abuse and parental SUP). Treatment response was examined as a potential confounder in the relationship between adverse experiences and the two outcomes. Since studies have shown that factors such as sex (Hser et al., 2003), ethnic minority status (Lewis et al., 2018; Mitchell et al., 2008) and age (Anderson et al., 2007) may play a great role in relation to SUD treatment outcomes, we also controlled for the effect of these factors. Sex (boys = 0; girls = 1) and ethnic minority status (participant or one or both parents born in Denmark = 0; participant or both parents born abroad = 1) were dummy coded. In addition, based on the variety of treatment components that the study participants have received, the potential effect of the different treatment conditions was controlled for in our analyses (i.e., the four RCT groups and the post-trial phase). The predictors and control variables were entered individually in univariate analyses and together in multivariate analyses. Additional follow-up analyses were conducted to investigate a potential dose-response effect of accumulated events by using the number of adverse experiences (1, 2 or 3) as independent categories predicting each outcome.
Effect sizes for the multivariate analyses are reported as adjusted odds ratios (AORs). All analyses were conducted with Stata in a secure server of Statistics Denmark, the national census bureau, due to the handling of sensitive register data.
Results
Participants’ baseline characteristics
Baseline participant characteristics of the analysed sample are shown in Table 1. The majority were men. Over half of the participants reported that at least one of their parents had a SUP. Further, 75% (n = 436) had been exposed to at least one of the three adverse experiences, of which the most common was parental SUP (see Table 1).
Descriptive statistics for the full sample (N = 580).
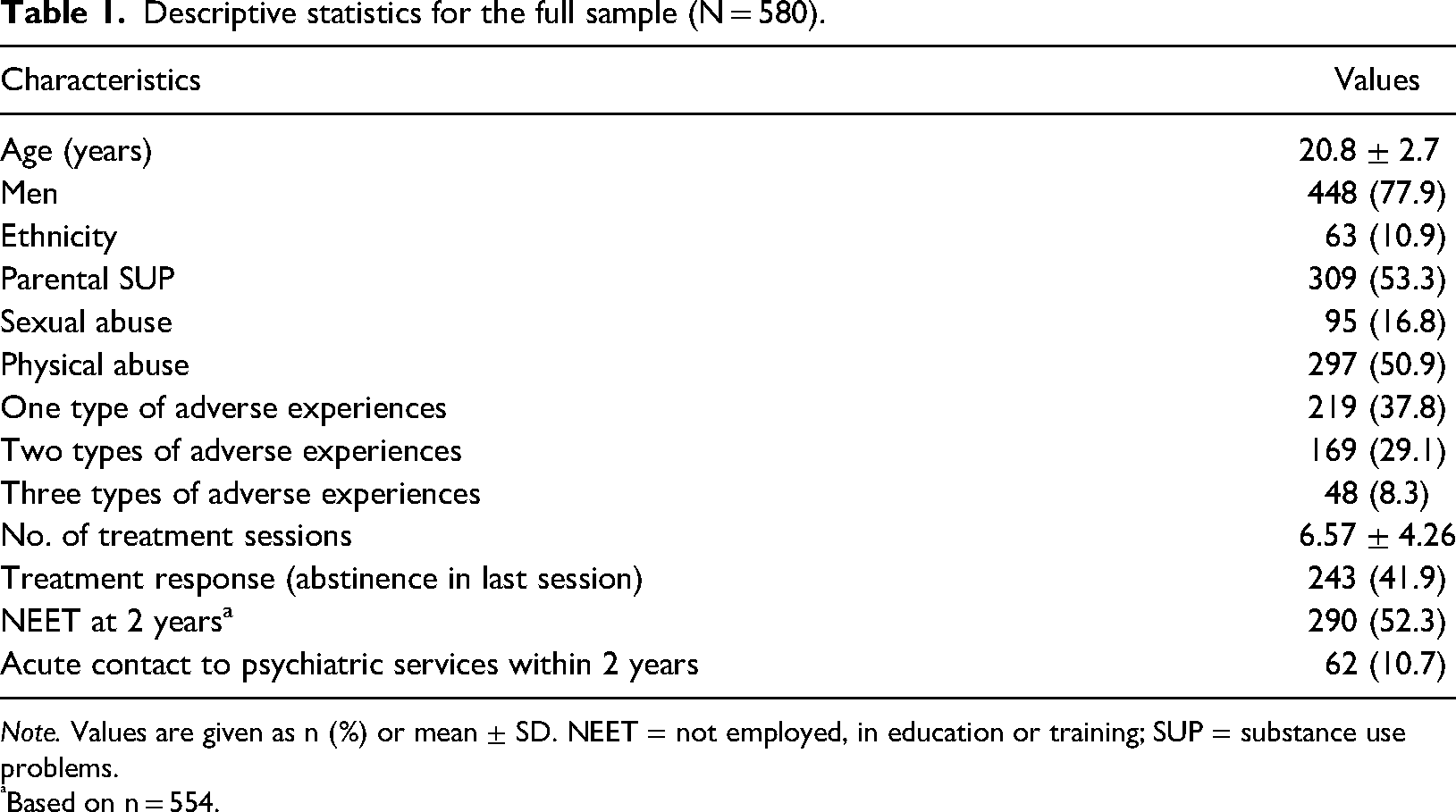
Note. Values are given as n (%) or mean ± SD. NEET = not employed, in education or training; SUP = substance use problems.
Based on n = 554.
Prediction of NEET
A total of 284 (51%) participants were NEET at some point in the two years after starting treatment. After controlling for demographic variables, treatment response and treatment conditions, only parental SUP, exposure to physical abuse and leaving treatment as non-abstinent (i.e., no treatment response) predicted NEET after starting treatment. Demographic variables, the treatment conditions and exposure to sexual abuse were not significant predictors of NEET. See Table 2 for all the parameter estimates.
Univariate and multivariate models predicting NEET (N = 554).
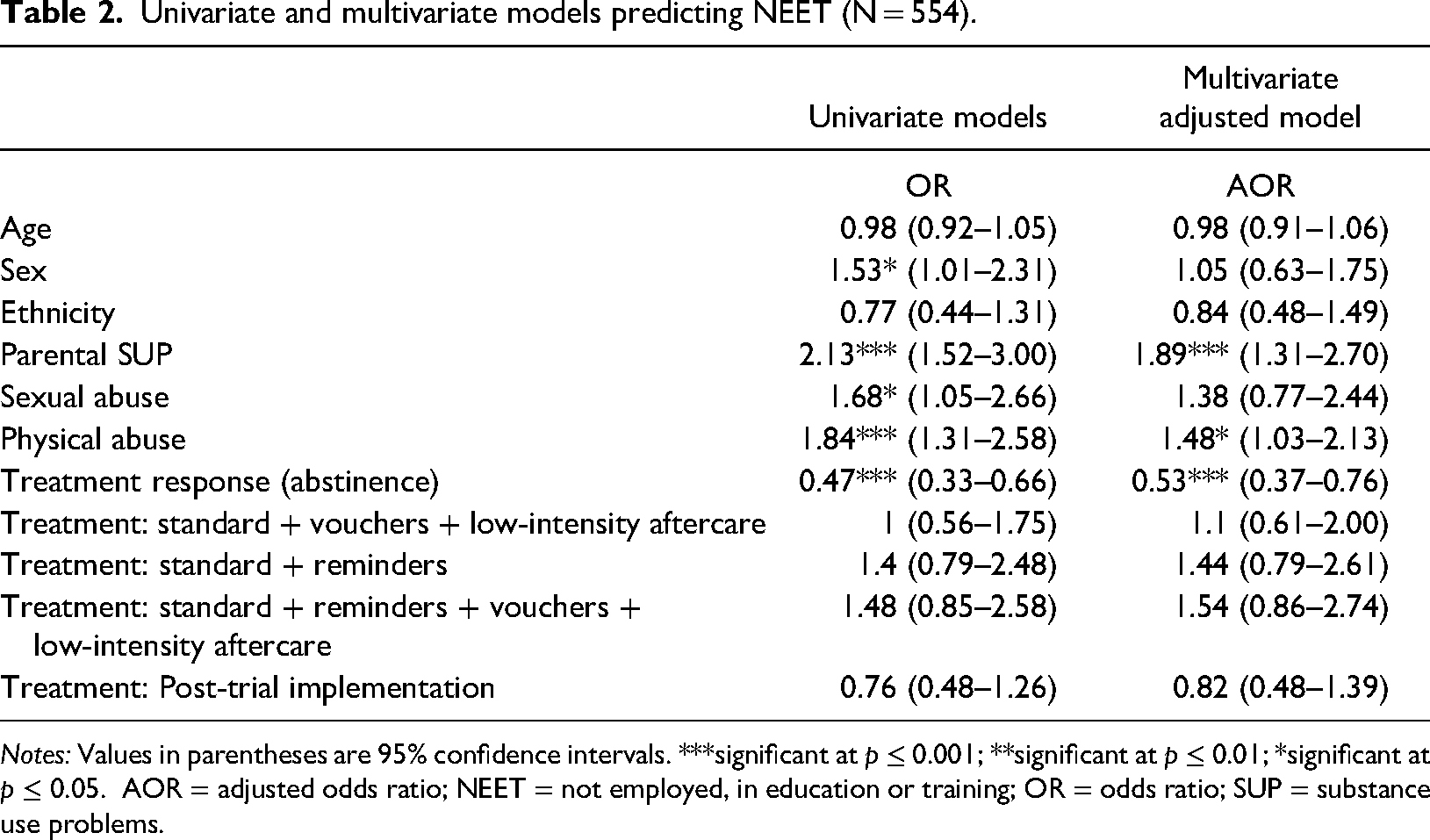
Notes: Values in parentheses are 95% confidence intervals. ***significant at p ≤ 0.001; **significant at p ≤ 0.01; *significant at p ≤ 0.05. AOR = adjusted odds ratio; NEET = not employed, in education or training; OR = odds ratio; SUP = substance use problems.
In the follow-up analyses, we found that experiencing at least one type of adverse experience predicted NEET status two years after starting treatment (AOR = 1.89, 95% CI 1.20–3.00, p = .006). However, the effect sizes were larger for exposure to two (AOR = 3.17, 95% CI 1.93–5.21, p < .001) and three types of adverse experiences (AOR = 3.14, 95% CI 1.47–6.70, p = .003). Thus, the magnitude of the effect was small for exposure to one of the adverse experiences, and moderate to being exposed to two or three types of adverse experiences. This may be interpreted as a dose-response effect with larger effects for exposure to more types of adverse experiences.
Prediction of acute contact to psychiatric services
A total of 62 (10.7%) participants had acute contacts with psychiatric services at least once within the two years after starting treatment. As shown in Table 3, the multivariate models showed that both sex and ethnic minority status were related to a higher likelihood of contacting psychiatric services. Neither age, treatment response, treatment conditions or exposure to any adverse experiences predicted acute contact to psychiatric services. We conducted exploratory analyses taking into account the effect of the number of adverse experience types predicting acute contact to psychiatric services. There were no significant effects in these analyses (AORs <1.94, all p > .10).
Prediction of acute contact to psychiatric health services (N = 580).
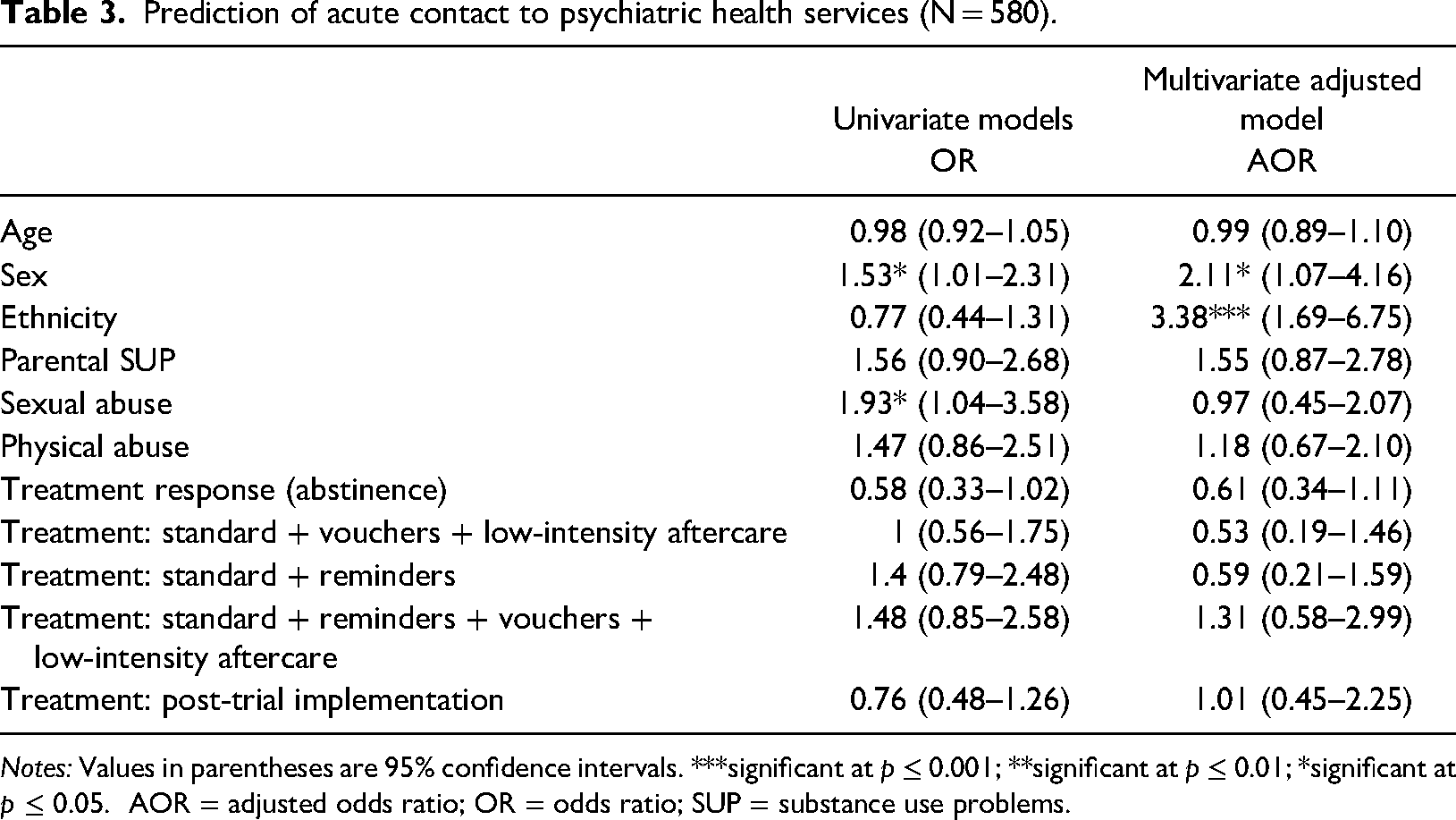
Notes: Values in parentheses are 95% confidence intervals. ***significant at p ≤ 0.001; **significant at p ≤ 0.01; *significant at p ≤ 0.05. AOR = adjusted odds ratio; OR = odds ratio; SUP = substance use problems.
Discussion
The aim of the present study was to examine three types of adverse experiences as potential predictors of NEET and poor mental health two years after SUD treatment enrolment. The analyses showed that more than half of the patients were NEET two years after treatment enrolment and one out of 10 contacted psychiatric services in an emergency at least once within the two years after starting treatment. The analyses that examined the impact of adverse experiences partially supported our hypotheses, since the adverse experiences predicted NEET two years after treatment enrolment, but not acute contact to psychiatric services. NEET was predicted by reported parental SUP, physical abuse and a greater number of adverse experiences as indicated by a dose-response effect relationship.
The association between physical abuse, parental SUP and NEET highlights the detrimental long-term effects of child maltreatment and neglect. The significant effects of adverse experiences were present even after controlling for the effect of treatment response and treatment condition. The association found is particularly noticeable since the measures of abuse and parental SUP used were broad and did not require any level of severity. Based on research indicating that abuse perpetrated by caregivers (i.e., high betrayal trauma) or abuse that continues for longer periods of time results in worse outcomes than abuse perpetrated by non-caregivers or single episodes of abuse (Delker et al., 2018; Edwards et al., 2012; Goldsmith et al., 2012; Springer et al., 2003), we could speculate that the association between adverse experiences and NEET would be even stronger for a population that only reported abuse experiences perpetrated by caregivers.
We also found a dose-response effect, which is in line with research establishing that the number of different types of child maltreatment experiences, also termed poly-victimisation, is crucial in the causal relationship between child maltreatment and negative social, behavioural and psychological outcomes (Brown et al., 1999; Cougle et al., 2010; Delker et al., 2018; Hyman et al., 2008; Springer et al., 2003).
The associations between adverse experiences and NEET in the present study underline the importance of looking beyond treatment and substance intake when assessing treatment outcomes and recovery trajectories. Although an individual may have changed a behavioural pattern such as drug use, the individual's overall behavioural and psychological profile and related challenges may still persist. Our findings underline that adolescents and early adults in SUD treatment with experiences of physical abuse, parental SUP and multiple adverse experiences may be in particular need of support in relation to enter and function in educational and employment systems.
It is worth noticing that we did not find an association between sexual abuse and NEET. Recent studies have examined the unique effects of physical and sexual abuse on negative outcomes including employment, but overall findings have been inconsistent. For example, in some studies, sexual abuse has been shown to be a stronger predictor for depressive disorders than physical abuse (Brown et al., 1999), anxiety (Cougle et al., 2010) and suicidal behaviour (Brown et al., 1999; Lopez-Castroman et al., 2013), whereas others have found physical abuse to be a stronger predictor of lifetime depressive disorders and poorer well-being than sexual abuse (Ney et al., 1994; Spatz Widom et al., 2007). Studies conclude that the time of onset, severity and duration is crucial for the effect of abuse experiences (Adams et al., 2018; Young et al., 2011). However, since we did not obtain these data, we could not explore these factors further. The variability in potential perpetrators may also have influenced our results. For instance, a number of unwanted sexual experiences perpetrated by peers or strangers (such as being fondled) may have been reported, and as such experiences are less likely to be associated to detrimental outcomes, this could explain the non-significant association between sexual abuse and NEET. In future studies, we would recommend more detailed measures of adverse treatment experiences and associated symptoms to entangle the effect of trauma severity.
Neither type nor number of adverse event types predicted acute contact to psychiatric services. This finding seems to contrast previous findings of associations between childhood trauma and higher rates of co-morbid psychiatric disorders, such as post-traumatic stress disorder (PTSD), personality disorders, major depressive disorder, anxiety disorders and suicide attempt in patients with diagnoses of SUD (Bernstein et al., 1998; Davies, 2009; Douglas et al., 2010). One explanation for our finding could be that the severity of adverse experiences probably varies considerably in the present study. Therefore, less severe experiences that are not associated with negative psychological reactions may have watered down the effect of the adverse experiences in the analyses. Another explanation is that a high proportion of individuals with a child maltreatment history who enter treatment for SUDs already have a psychiatric diagnosis. This could mean that although this patient group is more vulnerable psychologically, they are already a part of the established psychiatric treatment system and may therefore not be more in need of acute help after treatment compared to patients without a maltreatment history.
Two variables were significantly associated with contact to psychiatric services in the two years after treatment enrolment: ethnic minority status and sex (women). Past studies show that immigrants and refugees are more susceptible to mental illness because of potential mental health stressors, such as pre-migration experiences, intolerable memories, acculturation, lack of social support, unemployment and structural characteristics of the society that oppress or limit opportunities for ethnic minorities (Beiser, 2005; O’mahony & Donnelly, 2010). In addition, individuals of ethnic minority status are typically less prone to seek help in the public healthcare systems and encounter more system-level barriers to access regular mental health services (Leong & Kalibatseva, 2011; Scheppers et al., 2006). This could mean that, compared to the ethnic majority, the ethnic minority may receive less regular outpatient mental health services and therefore seek help only in more acute situations. Another potential partial explanation pertains to trauma symptoms and PTSD, which are more prevalent in ethnic minority individuals (Brewin et al., 2000; de Vries & Olff, 2009). Reductions in drug use and focusing on symptoms in SUD treatment could have worsened trauma-related symptoms such as sleep problems, depressive symptoms or anxiety symptoms that have been eased or suppressed by drug use. Therefore, there may be a higher need for acute psychiatric help after treatment for this particular group. From our data, we cannot interpret the reasons or acute symptoms triggering the contact of acute psychiatric services among individuals of ethnic minority status after SUD treatment, but it is a potential important focus point in the aftercare and follow-up treatment for this population.
To the best of our knowledge, this is the first study to find that adverse experiences in childhood and adolescence is a predictive factor for NEET after SUD treatment after controlling for treatment results. The results of the present study can be added to the rapidly increasing number of studies showing that adverse experiences in childhood and adolescence are important risk factors for SUD recovery trajectories, particularly occupational status (Najavits et al., 2020; Roberts et al., 2015; Simpson et al., 2017). Overall, the results call for a heightened focus on previous adverse experiences for adolescents and young adults who enter drug use treatment. However, as highlighted in a recent review of early childhood trauma, substance use and complex concurrent disorders among adolescents (Cabanis et al., 2021), there are hardly any guidelines for early identification of trauma in SUD populations, and existing SUD guidelines pay little attention to trauma among adolescents.
Limitations
A number of limitations are relevant when interpreting the results of this study. First, self-reports of adverse experiences have their limitations. Specifically, questions that are not behaviour-specific may be inaccurate since these questions assume that respondents categorise their experiences as abuse (Leong & Kalibatseva, 2011). It has been argued that people who have experienced physical or sexual abuse may not recognise what they experienced was against the law or may be reluctant to categorise their experiences as abuse (de Vries & Olff, 2009). This can lead to underreporting. However, underreporting may be more prevalent in surveys that examine the general population than in SUD treatment. Individuals in SUD treatment may be more prone to disclose victimisation experiences: first, because they are already in a developmental process in which they have recognised that they have a serious problem; and second, because that information could help their counsellor plan their treatment course. Due to the very high prevalence of adverse experiences in the present study, underreporting of these experiences do not seem to be an issue, but indeed more behaviour-specific measures are recommended. Further, as presented above, the measures of adverse experiences did not indicate severity of the event, the duration or the degree of psychological harm caused by the event (e.g., PTSD symptomatology). This means that less severe experiences, which were not perceived or experienced as harmful, may have been included in the analyses. The predictive effect of the adverse experiences may have been stronger if less severe experiences were excluded. It would therefore be very relevant to examine the effect dependent on different appraisals of experiences and symptom severity in future research studies. Further, it is a limitation that we do not know the relational nature of physical and sexual abuse experiences, which means that a broad range of abuse from caregivers, partners and peers could have been reported as sexual/physical abuse. Similar studies that examine differences in the specific effects of, for example, child maltreatment versus other abuse experiences would indeed be helpful.
Conclusion
The results of this study underscore the extent of employment and education challenges among adolescents and young adults after treatment for SUDs. More than half of the participants were not in education or employed two years after entering treatment for SUDs. Our findings suggests that adverse experiences such as parental SUP or physical abuse may be important predictors for unemployment after treatment. More research that includes more detailed measures of more adverse childhood experiences and a range of further social function outcomes, such as homelessness and criminality, would be very relevant to understand the full extent of the effect of adverse experiences for the social pathways after treatment. No association between adverse experiences and seeking acute help from psychiatric services in the two years after treatment was found.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article