
Abstract
Keywords
Alcohol-related problems have been a priority for the healthcare system in many countries, especially high-income countries (World Health Organization, 2018). However, treatment-seeking among people with alcohol problems remains infrequent (Cunningham & Breslin, 2004), concerning less than 40% of alcohol-dependent individuals (World Health Organization, 2018). In Sweden, less than 6% of people with an alcohol problem sought professional help (The Swedish Government, 2011). Beside the lack of problem awareness, reasons for refraining from seeking help are stigma or shame and perceived barriers to treatment, for example unaffordability or lack of trust in the healthcare system (Probst et al., 2015). Recently, telephone helplines have emerged as a cost-effective alternative to overcome barriers for help seeking for several problems (Gates & Albertella, 2016). In fact, telephone counselling is sometimes preferred to face-to-face interactions because it is easily accessible, conveys a sense of trust and safety to clients, and preserves anonymity (Reese et al., 2006).
The Swedish National Alcohol Helpline (SAH) was established in 2007 as a nation-wide free-of-charge counselling service targeting hazardous and harmful alcohol users. Details about the helpline can be found on the corresponding website (http://alkohollinjen.se/). The usual counselling consists of multi-session motivational interviewing (MI) aiming at the modification of drinking patterns and at the reduction of alcohol use (Heinemans et al., 2014). In a follow-up of a client-based cohort there was a pronounced decline of the Alcohol Use Disorders Identification Test (AUDIT) score. Additionally this study found that almost 30% of callers were abstinent or consumed alcohol at a low-risk level after 12 months (Heinemans et al., 2014), suggesting a beneficial effect of the intervention. However, this type of “on demand” counselling is rather resource-intensive.
As an alternative to extended multi-session counselling, brief interventions have been used to reduce hazardous and harmful alcohol use in primary care settings (Kaner et al., 2018). Brief interventions consist of a short-duration (5–30 minutes) structured counselling session that is offered to individuals to reduce substance use, mainly smoking and alcohol, or other lifestyle choices (World Health Organization, 2019). Since brief interventions imply lower costs, they could be implemented on a larger scale, therefore increasing the reach of the target groups (World Health Organization, 2019).
Although the effectiveness of brief interventions in addressing problematic alcohol use has been established (O’Donnell et al., 2014), their superiority compared with extended counselling is still under debate, and they have not been studied in the context of telephone helplines. A recently published systematic review showed that brief interventions significantly reduce both frequency of binge episodes per week (95% CI of mean difference –0.14 to –0.02) and drinking days per week (95% CI of mean difference –0.23 to –0.04) compared with no treatment (Kaner et al., 2018). Also, no additional effect was found with either increased duration of counselling or extended treatment compared with brief intervention (Kaner et al., 2018; Moyer et al., 2002). In contrast, an earlier review found a stronger effect of brief multi-contact intervention compared with brief or very brief interventions (Jonas et al., 2012).
In 2015, a randomised controlled trial (RCT) was set up in order to compare the effectiveness of the two counselling models at the Swedish National Alcohol Helpline (SAH). The main hypothesis was that the effectiveness of the two counselling modes would not differ, thus making the brief intervention potentially more cost-effective compared with the multi-session intervention. The results at six-month follow-up have been reported (Safsten et al., 2019). This article presents results after 12 months of follow-up, focusing on both concurrent and sustained behavioural changes.
Methods
The protocol of the trial with details about study design and methods has been published elsewhere (Säfsten et al., 2017) and will only be summarised here.
Study design and participants
This study is a two-arm randomised controlled trial, described in detail previously (Säfsten et al., 2017). Participants were randomised with a 1:1 ratio to either brief, structured intervention or usual care with follow-up at six and 12 months. Callers were eligible if they were 18 years of age or older, were first-time callers or callers with a “wash-out” period of at least 12 months since their last contact with the helpline, and were classified as hazardous or harmful alcohol users at inception. Exclusion criteria were a history of severe alcohol dependence, psychiatric co-morbidity, illicit drug use, suicidal intentions, and acute health problems. The flow of participants is illustrated in Figure 1.
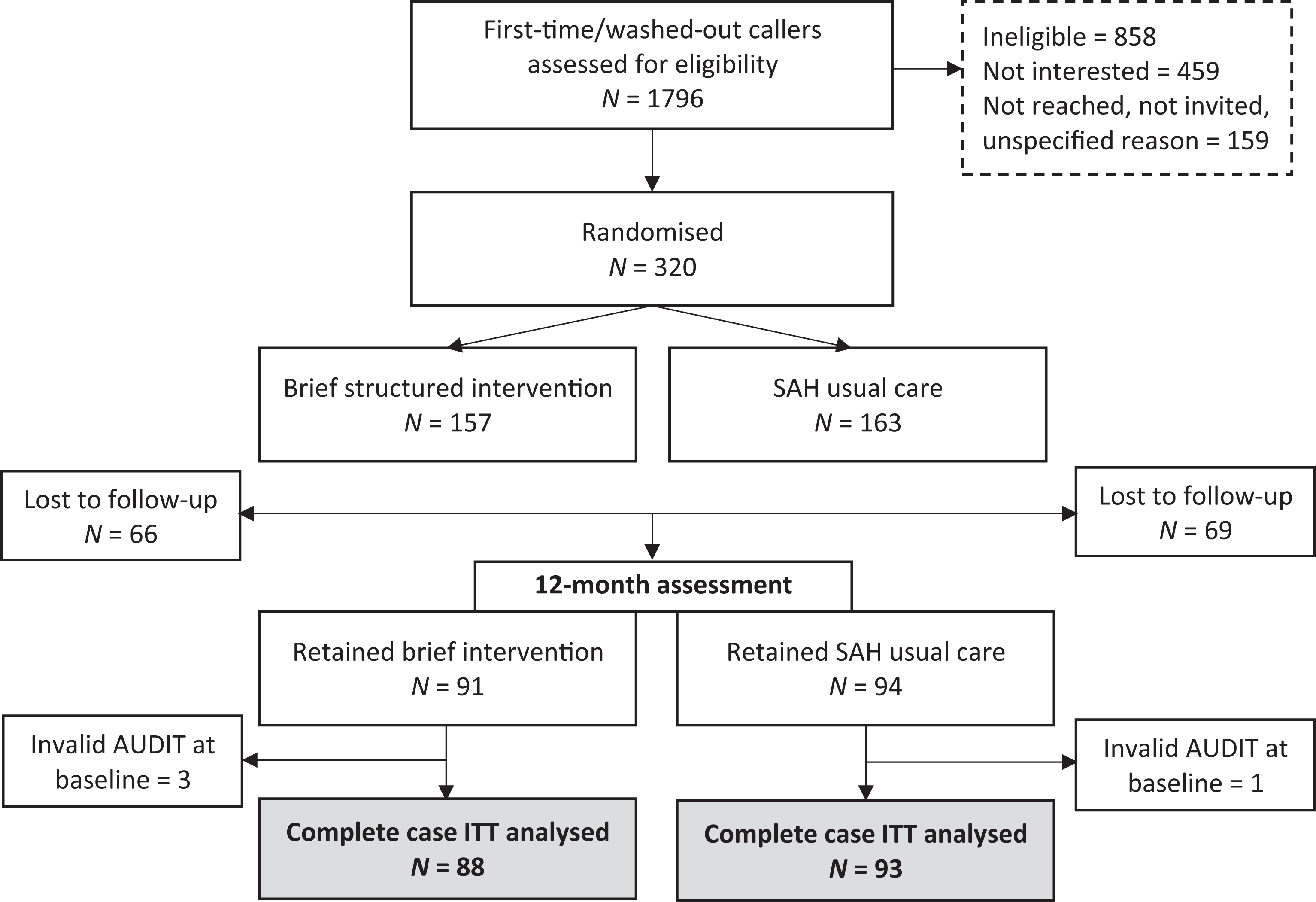
Flow of participant enrolment and follow-up.
Recruitment and randomisation
Clients who called the helpline between May 2015 and December 2017 were assessed for eligibility to participate in the trial. Eligible clients were informed about the study and asked about their interest in participating. Interested clients were contacted via telephone within a week from the first call by trained interviewers who were not involved in the counselling. During the call, interviewers (1) obtained verbal informed consent, (2) conducted the baseline interview, (3) opened a sequentially numbered, sealed envelope containing results of the randomisation algorithm and, (4) informed participants about the group allocation. The envelopes with group allocation were prepared in advance by a centrally located research coordinator, not part of the helpline’s staff.
Counsellors and participants were not blinded regarding the content of the intervention but were not aware of the study hypothesis or of the protocol of analysis.
Interventions
The brief structured intervention
The brief intervention consisted of a self-help booklet mailed to the participants, followed by a proactive call by a counsellor at the SAH. The self-help booklet contains a step-by-step guide based on cognitive behavioural therapy (CBT) to change alcohol use patterns. The booklet focusses on increasing motivation to change, initiating reflection, facilitating goal-setting and self-monitoring, as well as on providing suggestions to build resistance skills. Two weeks after receiving the booklet, participants were contacted by a counsellor who assessed its use, gave additional instructions, and discussed participants’ progress. After this proactive call, no additional contact was initiated by the helpline staff. However, participants could contact the SAH again if they needed. In this case usual counselling was provided.
Completion of the intervention was assessed by counsellors after the delivery of the proactive call. The counsellors recorded whether the intervention was (1) completed according to the protocol; or (2) completed with other content (i.e., usual motivational interview counselling), or (3) not completed.
The usual care
As part of usual care, telephone counselling was provided based on motivational interviewing with components of CBT. The counselling was intended to help participants to develop resistance skills, to promote motivation to change and to prevent relapse into the hazardous use of alcohol. Usual care had no standardised protocol. Counselling was based on the specific needs of each participant, including severity of alcohol problems and readiness to change. Clients and counsellors agreed on a counselling plan during the first call (including whether the following sessions should be client-activated or counsellor-activated). The number and duration of counselling sessions could vary but providing more than five sessions was very infrequent.
Data collection
Data were collected through structured interviews at baseline, six-month and 12-month follow-up via telephone. At baseline, information about demographics, i.e., sex, age, education, employment and living arrangements, and social support was collected. Information on alcohol use patterns was collected at all three time points. The baseline assessment was conducted prior to disclosure of treatment assignment. Likewise, outcome assessment at follow-up was conducted by interviewers blinded to the participants’ group allocation. Further details on methods of data collection can be found in previous publications (Safsten et al., 2019; Säfsten et al., 2017).
Outcome measures
We used the Alcohol Use Disorders Identification Test (AUDIT) to assess the alcohol use risk levels and derive the outcome variables. The instrument consists of 10 questions with a score of 0–4 for each question, yielding a total score ranging from 0 to 40; the higher the score, the more problematic the alcohol use (Berman et al., 2012). Risk levels were defined separately for men and women as described below (Berman et al., 2012): Low-risk use: score 0–7 men; 0–5 women Hazardous use: score 8–15 men; 6–13 women Harmful use: score 16–19 men; 14–17 women Probable dependence: score ≥ 20 men; ≥ 18 women
Additionally, some items of the AUDIT, composing the subscale known as AUDIT-C, were also used to assess frequency and quantity of drinking. The AUDIT-C consists of the first three questions of the AUDIT that yield a total score ranging from 0 to 12.
In this study, the primary outcome was defined as any shift to a lower AUDIT risk level (binary outcome), at 12-month follow-up compared with baseline. Five secondary outcomes were also derived including: (1) mean change in AUDIT score and (2) mean change in AUDIT-C score (3) change to “low-risk level”; (4) sustained risk level reduction throughout the whole follow-up, i.e., being in a lower risk level compared with baseline at both six-month and 12-month follow-up and (5) sustained low-risk level, i.e., being classified as low-risk user at both six-month and 12-month follow-up.
Statistical analysis
Baseline characteristics are presented as means and standard deviations (SD) for the continuous variable (age) and numbers and percentages for the categorical variables of the total sample and separately for each group of intervention. Baseline characteristics of participants lost to follow-up at 12-months are also reported.
The AUDIT score was analysed both as a continuous and as a binary variable (change to lower risk level and sustained change: yes/no). As the randomisation was expected to be successful, no confounder was controlled for, and all analyses were bivariate.
Analyses were conducted as intention to treat, e.g., participants were considered as exposed to the intervention that they were randomised to. The binary outcomes risk ratios (RR) and their 95% confidence intervals (CI) were estimated using the generalised linear models function with binomial family and logistic link using no improvement as reference category. For continuous outcomes linear regression models were used.
Due to a high level of missing information on the outcome within the two follow-up data points (42.7% attrition) where the assumption of missing completely at random (MCAR) could not be made, we compared the results obtained from simple pairwise deletion with results from multiple imputation of the outcome variable (AUDIT/AUDIT-C score) in line with recommendations for randomised control trials (Sainani, 2015). Since outcomes were assessed at two subsequent follow-up occasions, the method of choice was chained multiple imputation on multiple outcomes, as described by Azur et al. (2011). Further, the chained multiple imputation steps were ordered so that data for the first follow-up was imputed independently from the second follow-up. In line with recommendations from Graham et al. (2007), a large number of imputations was carried out (n = 100). The multiple imputation resulted in a sample of 311 participants out of 320 randomised individuals. Nine participants did not provide valid information for the starting variables that were used for the chain multiple imputation.
In order to further explore the entity of possible bias introduced by attrition we conducted some additional sensitivity analyses adjusting for potential confounders including sex, age, education, employment status and living arrangement, i.e., whether or not living alone.
All analyses were conducted with Stata 14.2
Results
Participant characteristics
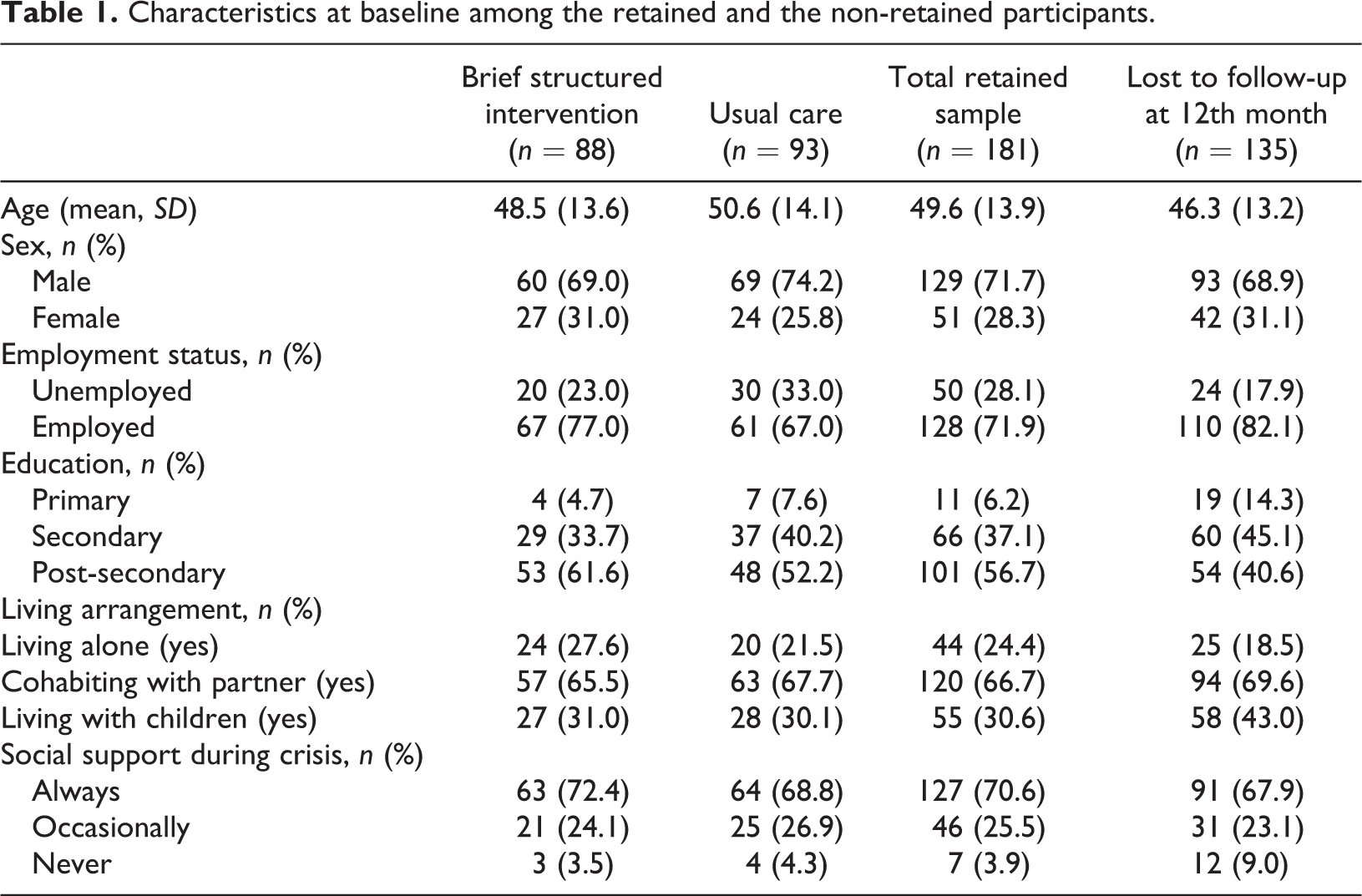
Table 1 presents the baseline characteristics of the analytical sample, separately for each experimental group, and the comparison between participants retained and those lost to follow-up after 12 months. Of 320 randomised participants four had AUDIT scores lower than hazardous use level, therefore they were excluded from the analyses; yielding the final sample size of 316 participants (Figure 1). After 12 months 135 participants (42.2%) were lost to follow-up, with similar attrition in the two groups (42.3% in usual care and 42.0% in the brief structured intervention). Participants lost to follow-up were younger than those retained; more often females; had lower education levels; were more often employed; and were more likely to have low social support (Table 1). The characteristics of participants lost to follow-up were similar between the two intervention arms (data not shown).
The 181 participants constituting the primary analytical sample had a mean age of 49.6 years; less than one third was female. Most participants were employed, had an educational level of high school or above and were living with a partner. Although the two experimental groups were well balanced at baseline as effect of random assignment (data not shown), at the 12-month assessment this was no longer the case, because of loss to follow-up. Compared with usual care, participants in the brief structured intervention were on average two years younger, and included more women (31% and 26% respectively); the proportion unemployed was lower by 10% and the proportion with education attainment beyond secondary school was higher (62% compared with 52% in the usual care group). In terms of living arrangements and social support, the two groups were similar (Table 1).
Characteristics at baseline among the retained and the non-retained participants.
Change of alcohol drinking habits at 12-month follow-up
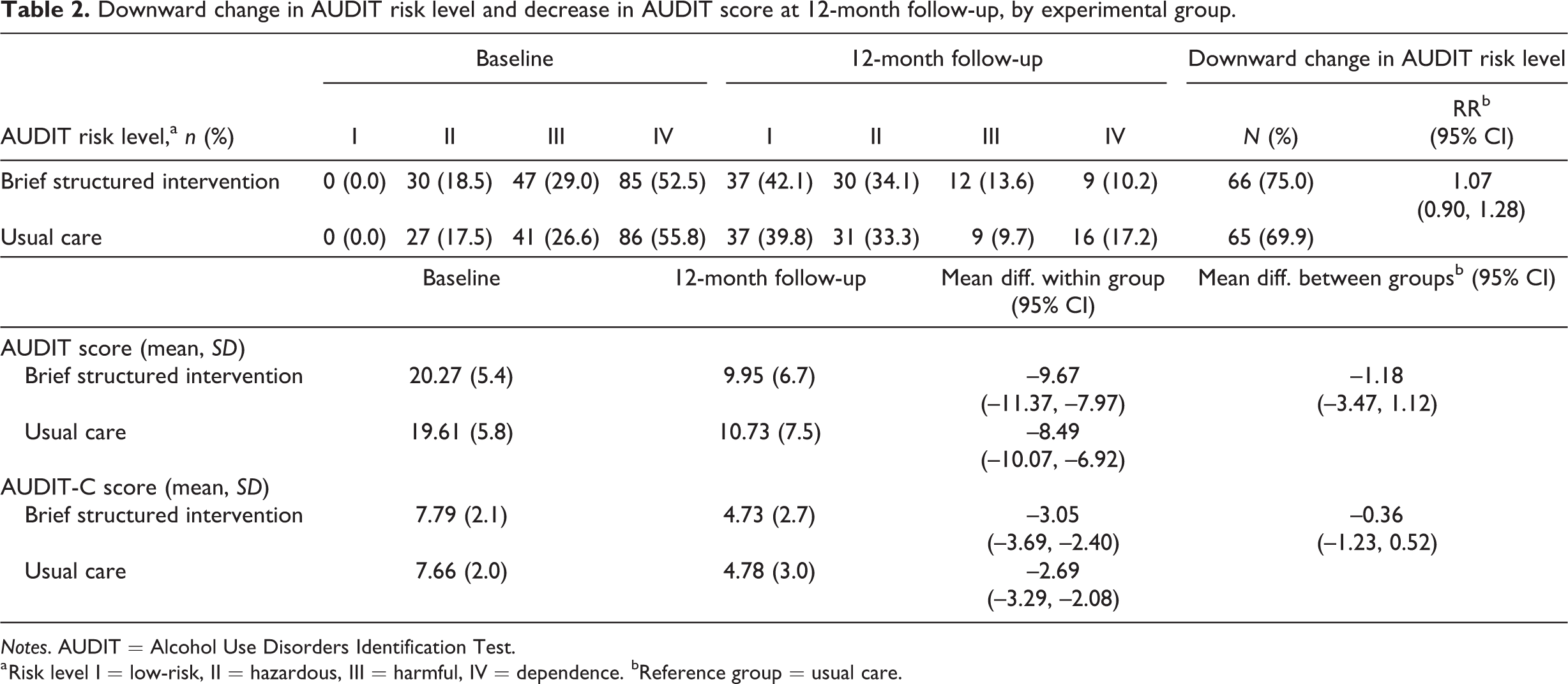
Twelve months after the intervention, 75% of the participants in the brief structured intervention and 70% of the participants in the usual care group shifted to a lower alcohol use risk level. About 42% and 40% in the two respective groups had shifted to low-risk level (level I). The mean AUDIT and AUDIT-C scores also decreased in a comparable fashion between the two groups (Table 2).
As a consequence, there was no difference between experimental groups in either the change to lower risk level (RR 1.07; CI 95% 0.90, 1.28) or the mean AUDIT score (for AUDIT score mean difference between groups –1.18, CI 95% –3.47, 1.12; for AUDIT-C score mean difference between groups –0.36, CI 95% –1.23, 0.52) (Table 2).
Downward change in AUDIT risk level and decrease in AUDIT score at 12-month follow-up, by experimental group.
Notes. AUDIT = Alcohol Use Disorders Identification Test.
a Risk level I = low-risk, II = hazardous, III = harmful, IV = dependence. bReference group = usual care.
Sustained risk level reduction
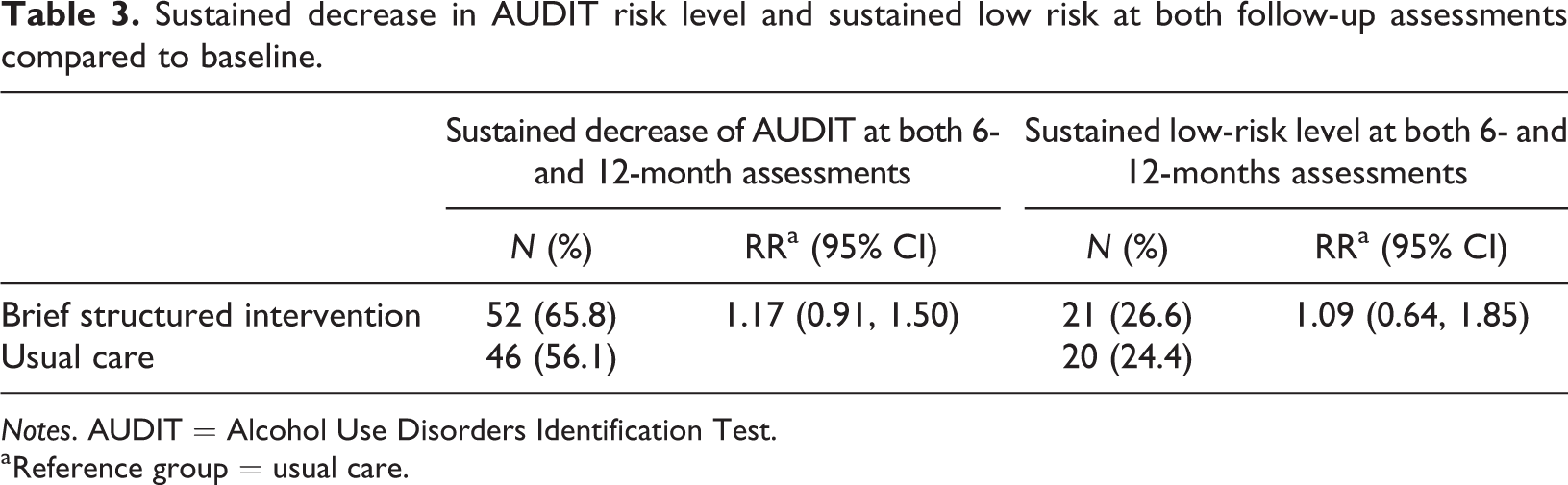
About 66% of participants in the brief structured intervention and 56% in the usual care group remained at a lower risk level at both follow-up times (six and 12 months) compared with baseline. The corresponding proportions remaining in the low-risk level were 27% in the brief structured intervention and 24% in the usual care group (Table 3).
Sustained decrease in AUDIT risk level and sustained low risk at both follow-up assessments compared to baseline.
Notes. AUDIT = Alcohol Use Disorders Identification Test.
a Reference group = usual care.
Sensitivity analyses
The sensitivity analyses adjusting for potential confounders (sex, age, education, employment status and living arrangements) yielded estimates that did not appreciably differ from the unadjusted (data not shown).
The results from imputed data indicated that the estimates of effect size (RRs and mean score differences between groups) were generally slightly larger than in the available case analysis (Table 4). However, the precision was not significantly affected.
Comparison between estimates obtained through multiple imputation for missing outcome variable and available case analysis.
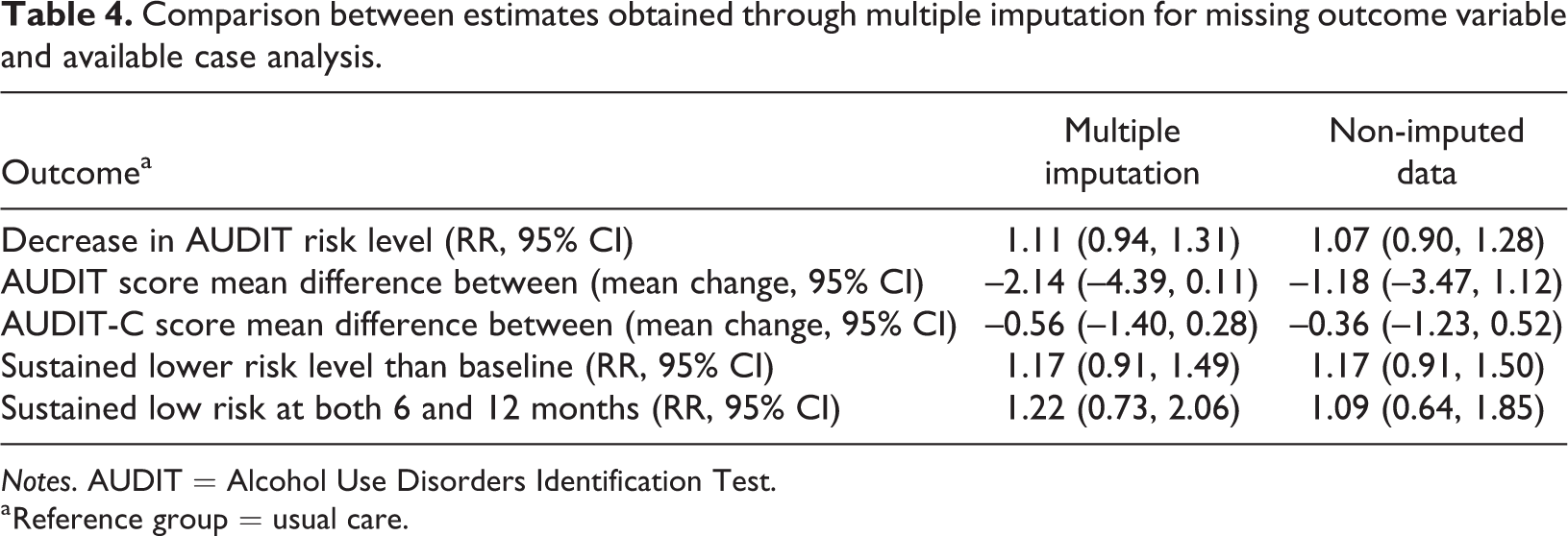
Notes. AUDIT = Alcohol Use Disorders Identification Test.
a Reference group = usual care.
Discussion
This experimental study is the first to explore the effectiveness of brief and extended counselling within the frame of a telephone alcohol helpline. We did not find evidence that a brief structured intervention or multi-session motivational interviewing presented important differences in promoting changes of alcohol drinking behaviour among callers to the Swedish Alcohol Helpline (SAH). This was true for a variety of outcomes including sustained change over one year. Both interventions were equally and consistently associated with a change of alcohol use among the participants in this study, where more than 70% of the participants reported a lower-risk drinking level at follow-up compared with inception, and more than 40% shifted to low-risk alcohol use. In addition, more than 50% of those reporting a risk level decrease maintained this profile, and at least one out of five becoming a low-risk alcohol user sustained this drinking pattern throughout one year.
Our findings are generally in line with those of previous studies. A systematic review of interactive telephone counselling treatment on alcohol or illicit drug uses found an overall positive effect of counselling of minimal intensity compared with other types of interventions. This review also suggested that the effect of counselling treatments was long-term (Gates & Albertella, 2016). A randomised trial conducted among adult harmful drinkers compared the effectiveness of usual care with counselling for alcohol problems (multi-session counselling based on motivational interview) (Nadkarni et al., 2017). Behavioural changes at both three and 12 months among drinkers receiving the counselling were very similar to those found in the present study (Nadkarni et al., 2017). In a study conducted in the UK among patients in primary care using brief advice and brief counselling, Kaner et al. (2013) found a proportion of hazardous and harmful alcohol users shifting to low-risk level after 12 months of about 35%, which compares well with that found in this study (40–42%).
This study also adds to the evidence that brief structured and multi-session counselling may be similarly effective in changing alcohol use even in settings different from telephone services. In the aforementioned study conducted by Kaner et al. in a primary care setting, three interventions with increasing intensity of counselling were compared, with equivalent results (Kaner et al., 2013). In a randomised controlled trial in Australia based on a telephone helpline, a brief intervention including a self-help manual was compared with an intensive cognitive behavioural therapy (CBT). A similar proportion of participants in the two groups shifted to a low-risk alcohol use level (Shakeshaft et al., 2002). Several other studies also failed to detect a difference between brief interventions using self-help materials and more intensive multi-session counselling in promoting behavioural changes concerning alcohol use (Group, 1996; Senft et al., 1997).
However, other studies presented contrasting findings. For instance, a randomised controlled trial among German adults with alcohol use disorders showed the superiority of multi-session counselling compared with self-help materials (Bischof et al., 2008). Motivation to change in the target group can explain this discrepancy. In fact, in the German study, participants were screened and recruited from general practices, while callers of a helpline are individuals who autonomously took the step of seeking help for their alcohol use.
The similar effectiveness of the two interventions found in the study is likely to be explained by this high motivation, predicting behavioural change even with minimal support. However, we cannot exclude that the low statistical power of the study due to the small sample size may have prevented the detection of weak effects. Using the final analytical sample, the study had only about 12% power to detect as statistically significant an RR of 1.07 for the main outcome.
Strengths and limitations
The randomised controlled trial design minimises bias due to confounding in this study. Attrition was similar in the two experimental groups, thus indicating low potential for selection bias, as also indirectly supported by the sensitivity analyses.
Some limitations of this study should also be acknowledged. In behavioural interventions, blindness cannot be achieved at all levels. However, in this study the baseline assessment was conducted before randomisation, and the outcome assessment at follow-up involved staff blinded to the treatment allocation. The selected sample of participants in this study imposes caution about the generalisability of the results. While participants in this study were largely representative of the clients calling the SAH (Safsten et al., 2019) they presented a more problematic alcohol use than could be expected from the general population prevalence. Motivation to change was probably higher in this sample than in a general population of problematic drinkers. Finally, participants agreeing to be randomised are more likely to judge the two counselling models as similarly suitable for their needs. The limited analytical sample prevented the detection of small effects. Finally, the risk of contamination cannot be excluded, because the clients in the brief structured intervention were not discouraged from further calling the helpline due to ethical concerns. However, the average number and the duration of sessions were substantially higher in the usual care group, indicating a good preservation of the original treatment plan.
Conclusion
In the context of telephone helplines, brief counselling coupled with self-help aids did not differ from extended counselling in promoting long-term change in alcohol use. This suggests that such brief interventions may be used as an alternative or complementary treatment in telephone counselling, and that their cost-effectiveness should be investigated.
Footnotes
Ethics approval and participant consent
Ethical approval was granted by the Ethical Review Board of the Stockholm region (DNR 2014/1732-31/5). Written information was available on the website (![]() ). As the data were collected via telephone, verbal informed consent was registered in a survey form by interviewers. The trial was registered with ID: ISRCTN13160878; date applied 21/11/2015; date assigned 18/01/2016.
). As the data were collected via telephone, verbal informed consent was registered in a survey form by interviewers. The trial was registered with ID: ISRCTN13160878; date applied 21/11/2015; date assigned 18/01/2016.
Availability of data and material
The data that support the findings of this study are available on request from the authors. The data are not publicly available due to containing information that could compromise the privacy of research participants.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Public Health Agency of Sweden (grant No. 05576-2014-6.2) and by SRA Systembolagets råd för alkoholforskning (grant No. 4-5/2018).