
Abstract
Objective:
The patient’s free choice of treatment goals for alcohol use disorder (AUD) is predictive for treatment outcome. Presently there is limited knowledge of whether the age at onset of AUD influences the choice of goal for treatment. The present study investigates whether there are differences in choice of treatment goal between patients with very late onset alcohol use disorder (VLO AUD ≥ 60 years) and those having early or mid-age onset of AUD (EMO AUD < 60 years).
Method:
Participants were 341 persons, voluntarily enrolled in the Elderly Study, who were seeking treatment for AUD in outpatient centres for alcohol treatment in Denmark. Data regarding thoughts about abstinence, alcohol use in the last 90 days, motivation for treatment and psychiatric diagnosis were collected via questionnaires. A logistics regression was used to analyse the data.
Results:
32.1% of the participants with VLO AUD chose temporary abstinence goals, compared to 18.2% of the patients with earlier-onset AUD (p = 0.024). Further, 10.7% of participants with VLO AUD chose total abstinence goals compared to 31.3% of participants with early or mid-age onset AUD (p = 0.002).
Conclusion:
There are significant differences in choice of goal between participants with very late onset AUD and early or mid-age onset AUD. Individuals with very late onset alcohol use disorder tend to choose temporary abstinence over any other treatment goal whereas, in general, individuals with early onset alcohol use disorder choose permanent abstinence over other treatment goals.
Today, there is a growing emphasis on involving patients in their own treatment as a key to health behaviour change and improved self-management of chronic conditions such as addiction (Hibbard, Mahoney, Stock, & Tusler, 2007; Hibbard, Stockard, Mahoney, & Tusler, 2004). Treatment goals are an important factor in predicting treatment outcome (Adamson, Heather, Morton, & Raistrick, 2010). Overall, abstinence as a goal in treatment for alcohol use disorder (AUD) seems to lead to the largest proportion of patients with successful outcomes (Dunn & Strain, 2013), where relatively fewer patients seem to be successful in treatment with controlled drinking goals (Meyer, Wapp, Strik, & Moggi, 2014). Although patients’ goals for treatment may change during the course of treatment for AUD (Haug, Castro, Eggli, & Schaub, 2018; Meyer et al., 2014), most patients seem to strive for controlled drinking goals (Haug et al., 2018; Haug, Eggli, & Schaub, 2017), particularly in the early stages of treatment. In the mid-1980s Orford and Keddie (1986) showed that self-selected goals were predictive for positive treatment outcome. Overall, treatment goals are, however, still a debated area (Kiluk, Fitzmaurice, Strain, & Weiss, 2018) and one of the central questions is whether the patient can and should choose their own goals, and whether they can do so freely (Emiliussen & Wagoner, 2012).
Alcohol problems are present in all age groups. The number of older adults with alcohol problems is rising (Bjork, Vinther-Larsen, & Thygesen, 2006; Hvidtfeldt, Vinther-Larsen, Bjork, Thygesen, & Grønbæk, 2006a, 2006b). Also, in Denmark, the proportion of older adults in the treatment-seeking population is increasing (B. Nielsen, Nielsen, Lolk, & Andersen, 2010). Some older adults have had an alcohol problem since they were young or middle aged and may have been in treatment before. Others have experienced a very late onset of their alcohol use disorder (VLO AUD), i.e., after the age of 60 years (Wetterling, Veltrup, John, & Driessen, 2003). While there is some literature on “late onset” of AUD, often defined by an age criterion of 45 years, VLO AUD is an understudied field (Emiliussen, Nielsen, & Andersen, 2017). We hardly know anything about the profiles of those who present with VLO AUD, or what they aim for in treatment. So far, studies on treatment goals have been performed primarily on middle-aged patients (Meyer et al., 2014; Orford & Keddie, 1986). Due to the very late onset of their drinking problems, their treatment goals may differ from older adult treatment-seeking individuals, who have been suffering from AUD for a larger part of their adult lives. For instance, VLO AUD has been found to be a milder and more narrowly defined psychiatric problem (Van Montfoort-De Rave, De Weert-Van Oene, Beurmanjer, & Koekkoek, 2017), than AUD with an onset at other ages. Very late onset AUD is also associated with less socially unacceptable symptoms, and persons with VLO AUD also have higher education, income and life satisfaction levels than those with earlier onset AUD (Schonfeld & Dupree, 1991; Wetterling et al., 2003). In sum, VLO AUD patients seem to have a large degree of psychological and social resources available. Thus, it is to be expected that individuals with VLO AUD will differ from those with earlier onset of an AUD in their choice of goals for alcohol treatment. It may also be expected that the seemingly larger amount of resources in the VLO AUD subgroup affects the patients’ motivation, self-efficacy and trust enabling them to lower or quit their drinking. However, Kelly and Greene (2014) has shown that among young individuals the significance of self-efficacy’s predictive ability may be moderated by the individual’s motivation to enact the behavior in the relation between motivation and self-efficacy.
Aim
The present study investigates whether there are differences in choice of alcohol treatment goal between patients experiencing VLO AUD (≥60 years) and those having experienced early or mid-age onset of AUD (EMO AUD < 60 years).
Materials and method
Data were gathered from the Danish participants in an international multi-site randomised controlled study between January 2014 and May 2016: the Elderly Study. The study compared two brief interventions for individuals over the age of 60 years with AUD (Andersen et al., 2015; A. S. Nielsen et al., 2016). Inclusion criteria for the Elderly Study were age (≥60 years), presenting an alcohol use disorder according to the DSM-5 (NIAAA, 2016), and passing a comprehension quiz based on 10 questions pertaining to the implications of participating in the study, e.g., knowing that it is voluntary to participate. Exclusion criteria were current psychotic symptoms, severe depression, manic episodes, bipolar disorder, or if the patient had suicidal thoughts/behaviour, used illicit opioids and/or stimulants, had participated in other types of alcohol treatment within the last 30 days, or had a legally authorised representative (Andersen et al., 2015).
Participants
All 341 Danish participants in the Elderly Study were voluntarily seeking treatment for their alcohol problem in outpatient centres for alcohol treatment in Odense, Aarhus, and Copenhagen, Denmark. They are divided into two groups: the group of individuals with very late onset alcohol use disorder (VLO AUD) includes participants who declared that they had experienced two or more symptoms of an AUD (DSM-5) after they reached the age of 60 years (n = 56). The second group, with an onset of AUD before the age of 60 years (EMO AUD), consists of 205 participants. The remaining 80 participants could not remember when they first experienced symptoms of alcohol use disorder and were treated as missing data. This latter group with missing data did not differ from the other two groups in relation to age and gender distribution (data not shown in the tables).
Data on treatment goals
On the “Thoughts about alcohol abstinence scale” the participants were asked to indicate their goals for treatment. The questionnaire has been utilised in a series of studies (Dunn & Strain, 2013; Hall, Havassy, & Wasserman, 1991; Ramo, Delucchi, Hall, Liu, & Prochaska, 2013). The goals were presented in Danish in the following sequence: I really don’t have a clear goal in mind. I want to use alcohol in a controlled manner – to be in control of how often I use and how much I use. I want to be totally abstinent from all alcohol use for a period of time, after which I will make a new decision about whether or not I will drink alcohol again in any way. I don’t want using alcohol to be a habit for me anymore, but I would like to, occasionally, use alcohol when I really have an urge. I want to quit using alcohol once and for all, even though I realise I may slip up and use alcohol once in a while. I want to quit using alcohol once and for all, to be totally abstinent, and never use alcohol ever again for the rest of my life. None of the above applies exactly to me. My own goal is:…
In the analysis of the present study, participants choosing statements 2 and 4 were grouped together, as these were considered to aim for controlled drinking goals. Participants choosing statements 5 and 6 were grouped together, as these were considered to be abstinence goals. Participants choosing statement 3 constituted a group for themselves. Participants choosing statements 1 and 7 were excluded as they were considered ambivalent about their choice of goal for treatment. A total of seven participants chose either statement 1 or 7, and they belonged to the EMO AUD group. The excluded participants were four men and three women with an age mean of 65.1 years (SD 4.1); 28.6% were married (a little lower than the included participants); one was still working while the rest were retired. Other than that, they did not vary from the included participants. Excluding these participants from the analysis is unlikely to have affected the statistical calculations.
Further questionnaires
The data in the present study were collected upon the patients’ entering treatment (Baseline and before randomisation). The questionnaires utilised were Form90 (Miller, 1996), Motivation: Importance, Confidence, Readiness Rulers Worksheet (Rollnick, Butler, & Stott, 1997), MINI International Neuropsychiatric Interview 5th edition (Sheehan et al., 1998), and Thoughts about alcohol abstinence (Hall et al., 1991). All questionnaires were completed by the participants supervised by an interviewer. The questionnaires are briefly described below.
Form90 is a calendar-based questionnaire measuring the participants’ use of alcohol in standard drinks/units (12 grams of alcohol) (Miller, 1996). Form90 maps the alcohol use in the last 90 days leading up to the day of the interview.
Importance, Confidence, Readiness Rulers describes various aspects of change. By means of a Likert scale, the following aspects were measured: (1) How important is it for you to change your drinking? (2) How confident are you that, if you decided to make a change in your drinking, you can actually do it? (3) How ready are you to change your alcohol drinking? (Rollnick et al., 1997). The participants were asked to give their here-and-now assessment of each question from zero to ten (0 = not at all, 10 = completely) at the baseline interviews.
MINI International Neuropsychiatric Interview 5th edition screens for psychiatric disorders. One question was added in the MINI section on alcohol asking the participant to indicate their age when they had first experienced two or more alcohol-related symptoms.
Statistical analysis
Descriptive analysis included gender, age, marital status, employment, degree of education, and number of treatment sessions in the past.
Potential differences between EMO AUD and VLO AUD were examined with Pearson’s chi2 and Wilcoxon rank-sum test (univariate analyses). A logistic regression was applied to examine the significant differences between EMO and VLO AUD in the previous univariate analyses. We chose to include the variables with a significant level at <0.10 from the univariate analyses in a logistics regression, to investigate these variables’ influence at EMO and VLO AUD. This means that we performed the logistics analysis adjusted for current age, previous treatment history, retirement status, and being married or living with a spouse for the last 25 years.
All data were accumulated in a REDCap database, stored by OPEN (Odense Patient Data Explorative Network, Odense, Denmark) and analysed using Stata 14 SE statistical software (StataCorp LP, College Station, Texas). The level of statistical significance was determined at p < 0.05.
Results
When dividing the group into individuals with early to mid-age onset alcohol use disorder (EMO AUD) (< 60 years) (n = 205) and very late onset of alcohol use disorder (VLO AUD) (≥ 60 years) (n = 56), 55% of the VLO AUD group were men, compared to 63% in the EMO AUD group (NS) (Table 1). The mean age for the individuals with EMO AUD was 64.3 years (SD 3.6) compared to 68.5 years (SD 4.5) for VLO AUD (p < 0.001) (Table 1). The two groups differed in several ways: (1) their work/retirement status: 57.1% of EMO AUD were retired, whereas almost all VLO AUD were retired – 87.5% (p < 0.001). (2) duration of marital status/living with a spouse for more than 25 years: 70.8% of patients with VLO AUD had been married or living with a spouse for at least 25 years or more, compared to only 47.1% of the patients with EMO AUD (p = 0.004). (3) The treatment history: 71.2% of patients with EMO AUD had been in treatment at least once before, compared to only 42.9% of the VLO AUD (p < 0.001) (see Table 1).
Demographics and baseline data.
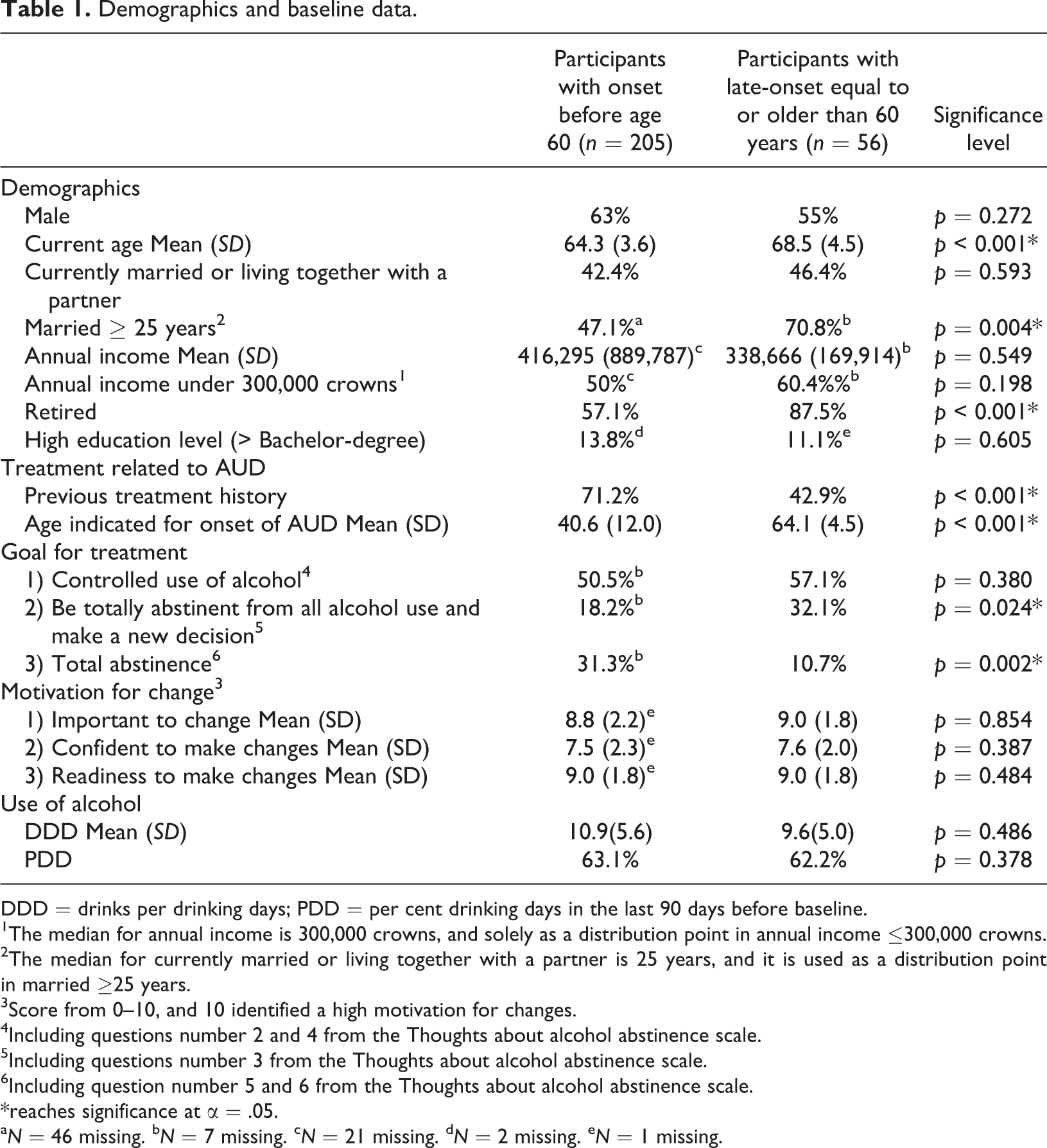
DDD = drinks per drinking days; PDD = per cent drinking days in the last 90 days before baseline.
1The median for annual income is 300,000 crowns, and solely as a distribution point in annual income ≤300,000 crowns.
2The median for currently married or living together with a partner is 25 years, and it is used as a distribution point in married ≥25 years.
3Score from 0–10, and 10 identified a high motivation for changes.
4Including questions number 2 and 4 from the Thoughts about alcohol abstinence scale.
5Including questions number 3 from the Thoughts about alcohol abstinence scale.
6Including question number 5 and 6 from the Thoughts about alcohol abstinence scale.
*reaches significance at α = .05.
aN = 46 missing. bN = 7 missing. cN = 21 missing. dN = 2 missing. eN = 1 missing.
The two groups differed in their choice of treatment goals. Almost a third of the participants with VLO AUD chose “I want to be totally abstinent from all alcohol for a period of time, after which I will make a new decision about whether or not I will use alcohol again in any way” (temporary abstinence), compared to only 18.2% of the patients with EMO AUD (p = 0.024). Only 10.7% of those with VLO AUD aimed for complete abstinence in the long run (permanent abstinence) compared to 31.1% of the participants with EMO AUD (p = 0.002) (Table 1).
No difference was seen in relation to alcohol use (number of drinks per drinking day) during the last 90 days before baseline. Nor were there any differences in the participants’ perceived importance, self-confidence and readiness for change of the problematic drinking behaviour.
Patients with VLO AUD were more likely to choose temporary abstinence as a goal for treatment OR = 2.7 CI (1.1 – 6.2) (p < 0.05), and less likely to choose permanent abstinence, OR = 0.1 CI (0.1–0.5) (p < 0.001), compared to patients with EMO AUD. The ORs increased when adjusting for current age, previous treatment history, retirement and being married or living with a spouse for the last 25 years (Table 2).
Prediction of the choice of treatment goals, and adjusted for current age, previous treatment history, married, and retired, in participants experiencing of early-onset (n = 205) or late-onset (n = 56).
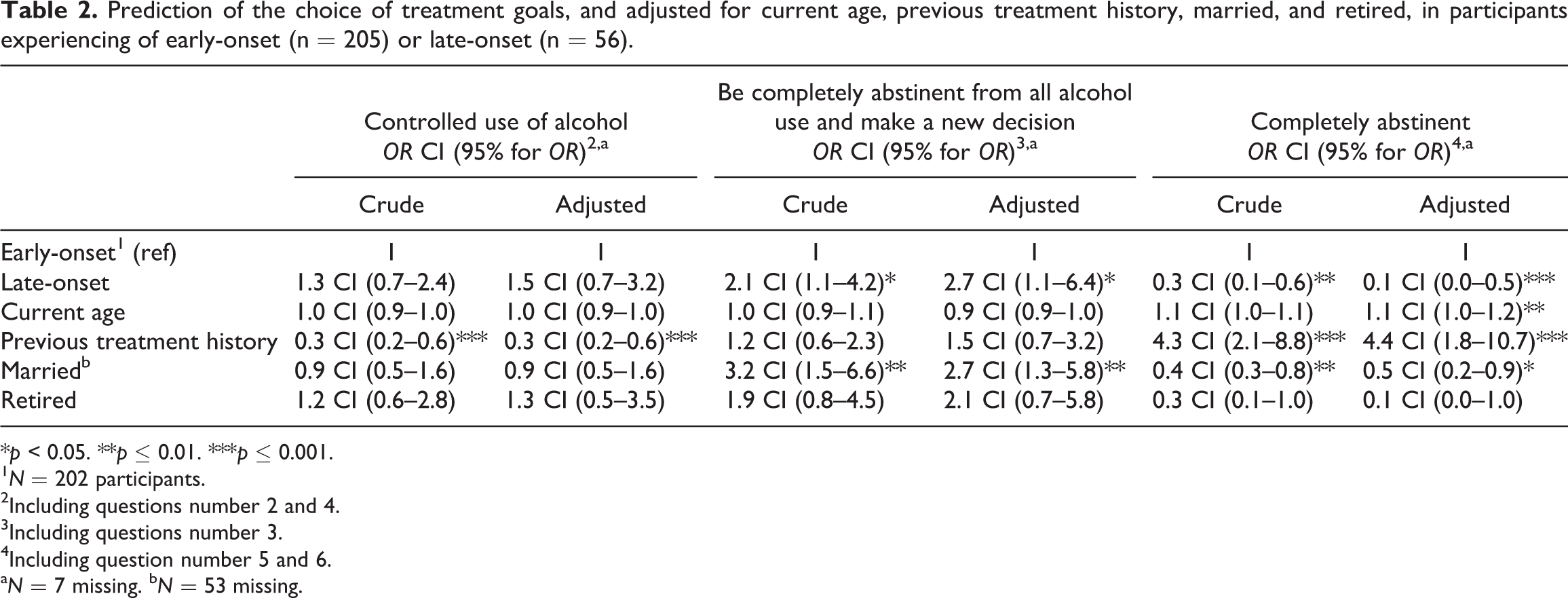
*p < 0.05. **p ≤ 0.01. ***p ≤ 0.001.
1N = 202 participants.
2Including questions number 2 and 4.
3Including questions number 3.
4Including question number 5 and 6.
aN = 7 missing. bN = 53 missing.
Interestingly, patients with a history of prior treatment affected the probability to choose permanent abstinence, irrespective of having EMO AUD or VLO AUD (OR 4.4, p ≤ 0.001).
Discussion
The present study compared treatment-seeking older adults with very late onset of AUD (≥60 years) and those with earlier onset of AUD in order to investigate whether the two groups strove for different outcomes from treatment. We found that individuals with VLO AUD were more likely to aim for temporary abstinence, while individuals with EMO AUD were more likely to aim for permanent abstinence goals. There were no differences between the groups regarding the proportion, at treatment start, aimed particularly for controlled drinking as the goal of treatment.
There is a lack of consensus regarding whether or not a goal of controlled drinking leads to successful treatment outcomes (Adamson & Sellman, 2001). Although it has been the topic of some (academic) debate whether controlled drinking should serve as a goal in alcohol treatment (Marlatt, 2001a, 2001b; Owen, 2001a, 2001b), in practice, “controlled drinking” has long been accepted as a treatment goal alongside a goal of temporary or permanent abstinence within the public-funded alcohol treatment centres in Denmark (Elmeland, 2015).
Studies have found that people who prefer controlled drinking goals are also those who have less heavy drinking problems (Booth, Dale, & Ansari, 1984; Hodgins, Leigh, Milne, & Gerrish, 1997; Pachman, Foy, & Van Erd, 1978). The individuals experiencing VLO AUD have, in fact, developed a problem that is substantial enough for them to seek treatment in a relatively short timeframe.
Qualitative research suggests that patients with VLO AUD often enter treatment based on encouragement/pressure from family (Emiliussen, Andersen, & Nielsen, 2017a). The “abstinent now, new decision later” goal seems to go hand in hand with this finding, as it makes sense for those who felt pressured into treatment, to make a short-term commitment. The same qualitative investigation found that the participants engage in a continuous process of valuation and devaluation of treatment. The findings in the present article support these findings, as the “abstinent now, make a new decision later” almost seems to be an operationalisation of this behaviour.
Our results indicate that being married is associated with the desire to abstain from alcohol for a limited period only. Previous research has indicated that older adult individuals living in congregate care settings want to maintain their habitual use of alcohol and do not think of it as a problem (Burruss, Sacco, & Smith, 2014). Further, it has been found that family pressure can be instrumental in an older adult seeking treatment (Emiliussen, Andersen, et al., 2017a). Therefore, the wish to maintain the habitual use of alcohol, and pressure from the family, might function as intrinsic and extrinsic motivation to achieve a “normal” use of alcohol. Hence, being married increases the likelihood of controlled drinking.
Qualitative research has also suggested that there are different trajectories into VLO AUD (Emiliussen, Andersen, & Nielsen, 2017b). Our findings indicate that individuals with VLO AUD show characteristics different from individuals with EMO AUD. They could be likely to prefer returning to that unproblematic controlled use rather than complete abstinence. The reason may be to avoid stigmatisation and taboo as a non-drinking adult is considered outside the norm in Denmark (Elmeland, 2015; Glass, Kristjansson, & Bucholz, 2013).
A more general notion can be made, namely that individuals who do not have a history of prior treatment aim for controlled drinking goals. This notion supports the literature (Haug et al., 2018; Haug et al., 2017) which finds that patients, in general, aim for controlled drinking. If, however, prior treatment has not led to the ability to control their drinking, the patients may adjust to the situation and/or resign and aim for permanent abstinence instead.
The relation between alcohol use, consequences, motivation and commitment to change is very complex. Our study points to differences between people with VLO AUD and EMO AUD. These differences may be related to the fact that people suffering from EMO AUD have had a long time to experience the consequences of overuse of alcohol. That means that those with a longer-lasting alcohol use disorder may have experienced more negative consequences and, hence, are more likely to choose total abstinence. Oppositely, people with VLO AUD may find it easier to cut back on drinking instead of stopping completely. However, with increasing age, even small consequences may be more visible and may motivate people to cut down.
The groupings used in the analysis for the present study are slightly different from the groupings used by Dunn and Strain (2013) who grouped them as follows: statements 3, 5 and 6 as abstinence goals and statements 2 and 4 as non-abstinence goals. They excluded participants choosing 1 and 7. We have counted those choosing statement 3 as a separate group as these participants were considered ambivalent.
The present study has some limitations. There may be a recall bias in relation to the participants trying to remember when they developed AUD symptoms for the first time. Further, the participants in this study were seeking treatment. This means that they are not a random group. Additionally, the sample is Danish and it is uncertain whether the results can be generalised beyond this particular alcohol culture and treatment system. As the analyses in the present article are based on subsamples, there is a risk of low statistical power, and the results should be seen in this light. A major strength of the present study is the number of participants (n = 261), which is considerably large. This lends power to our conclusions.
Conclusion
Individuals with very late onset alcohol use disorder (VLO AUD) tend to choose temporary abstinence over any other treatment goal whereas, in general, individuals with early onset alcohol use disorder (EO AUD) choose permanent abstinence over other treatment goals. Further, previous treatment attempts lead participants to choose permanent abstinence goals. In practice, therapists should take into account AUD trajectories and onset, when making the treatment goal the subject of discussion.
Footnotes
Acknowledgements
We would like to thank the staff in the Alcohol Treatment Centres in Odense, Aarhus and Copenhagen, who have supported the execution of the Elderly Study. We also extend our thanks to Odense Patient Data Explorative Network (OPEN).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We extend our thanks to the Lundbeck Foundation, the University of Southern Denmark and the Region of Southern Denmark who have given unconditional funding for the present study.