
Abstract
There is a high prevalence of persons with alcohol problems in the Danish population (Demant & Krarup, 2013). It is estimated that 20% of the adult population are heavy drinkers, 14% have a harmful alcohol use, and 3% are dependent drinkers (Hansen et al., 2011). Thus, approximately 150,000 Danes are defined as dependent drinkers (Hansen et al., 2011). Despite the high number of persons with alcohol problems in Denmark, the proportion of persons in treatment for alcohol use disorder (AUD) is low (Schwarz et al., 2018) even though Danish public treatment is free of charge and individuals may choose to be anonymous. The treatment typically consists of psychosocial interventions such as motivational interviewing and cognitive behavioural therapy, and pharmacological treatment, when relevant. No referral is needed. Treatment follows clinical guidelines and is typically delivered during individual weekly or bi-weekly sessions. Every year, approximately 15,000 persons over the age of 15 years receive publicly financed treatment for AUD (Schwarz et al., 2018). This means that only around 10% of the dependent drinkers sought treatment. It has been found that misconceptions about AUD treatment (Mellinger et al., 2018) and sparse knowledge about the treatment offers (Finn et al., 2014), in addition to not knowing what specialist addiction services were available or what types of support could be accessed at particular services (Parkman et al., 2017), influence treatment-seeking. A finding also described in studies of individuals who have changed their drinking by themselves (Copeland, 1997).
Furthermore, several studies performed in both general and clinical populations have examined reasons for being reluctant towards AUD treatment. They have suggested a common barrier to treatment to being stigma, including personal feelings of embarrassment and shame as well as concern over societal judgment (Andreasson et al., 2013; Cunningham et al., 1993; Grant, 1997; Keyes et al., 2010; Mellinger et al., 2018; Saunders et al., 2006; Schober & Annis, 1996; Schomerus & Angermeyer, 2008; Small et al., 2010) and worries about anonymity, e.g., due to concerns about employers finding out about alcohol use problems via insurance reviews (Mellinger et al., 2018). Additional psychosocial factors associated with discarding professional help for addictive behaviour has also been mentioned; for instance, lower educational level, ethnic minority status (Fernandez-Artamendi et al., 2013), and logistical, i.e., financial, insurance, and transportation obstacles (Mellinger et al., 2018).
Other commonly described barriers are emotional factors, such as personal unwillingness to be treated, not recognising alcohol-related problems, denial, and not perceiving a need for treatment (minimisation of problem severity) (Cunningham & McCambridge, 2012; Cunningham et al., 1993; Mellinger et al., 2018; Parkman et al., 2017). A desire to manage alcohol problems without professional help (treatment delay or self-change attempts) (Cunningham et al., 1993; Saunders et al., 2006) and needing help with other health or social issues before being able to address a drinking problem (Parkman et al., 2017) have also been found to be important barriers. Negative attitude towards treatment and lack of confidence in the treatment system and its effectiveness are other recognised obstructions (Grant, 1997; Parkman et al., 2017). Zero-tolerance, i.e., the requirement of absolute abstinence promoted by traditional programmes, may also hinder individuals who want to reduce the risks associated with heavy drinking, but do not want to quit drinking completely (Marlatt & Witkiewitz, 2002). This has, in particular, been seen in the young age group (18–34 years) and has been shown to function as a hurdle to seeking treatment (Finn et al., 2014).
Likelihood of treatment-seeking for problematic alcohol use can probably not be fully understood if attention is not paid to why the individual drinks alcohol in the first place. Thus, alcohol culture in society, including alcohol use in sub-groups, is also of importance (Rehm & Room, 2017) and needs to be taken into consideration when interpreting findings in the field, including what is perceived as problematic alcohol use and what is not (Emiliussen et al., 2017). In Denmark, the vast majority of the population drinks alcohol on a regular basis (European Commission, 2010) and alcohol is considered to be a natural part of daily life and, in particular, of social gatherings (Elmeland, 2015), in addition to being associated with masculinity (Emiliussen & Morrison, 2017). Factors such as peer pressure, enjoyment, masking pain, and a desire to drink are also reported to impact alcohol use (Yamarthi & Kannuri, 2019).
In order to increase the likelihood that individuals suffering from AUD seek treatment, it has often been proposed that hospitals may be effective platforms for identifying individuals who drink in a harmful way and recommending them to seeking treatment for AUD when needed (Babor et al., 2007). However, a series of attempts to implement systematic use of Screening, Brief Intervention, and Referral to Treatment (SBIRT) (Babor et al., 2007) in hospital settings has not been highly effective in leading patients suffering from AUD to seeking specialised AUD treatment (Glass et al., 2015; Nygaard & Aasland, 2011; Schwarz et al., 2018; Sivertsen et al., 2021; Watson et al., 2015). Thus, SBIRT seems to be effective primarily for patients suffering from heavy use rather than AUD. Even studies investigating the impact of outreach visits, where therapists from the AUD clinic talked to the patients at the hospitals, did not identify a large effect on treatment-seeking (Schwarz et al., 2018; Watson et al., 2015).
So far, however, no one has particularly studied how hospitalised patients, who suffer from AUD but have not sought treatment for their AUD, perceive their own drinking and the possibility of treatment-seeking. Thus, the attitude among the major target group for SBIRT interventions at hospitals is under-investigated. From a public health and clinical perspective, it is important to understand the reasons of the non-treatment-seeking population for not seeking treatment in order to explain the discouraging outcome of SBIRT so far, and in order develop acceptable and more useful interventions. To understand these phenomena more fully and gain insight into how people with alcohol dependence perceive treatment, research with a qualitative approach is required (Finn et al., 2014; Room, 2005).
Aims
This qualitative study aimed to investigate the reasons why individuals, identified at mental health and somatic hospitals, who suffer from AUD, have never sought treatment.
Methods
The present study is a qualitative study based on semi-structured individual interviews.
Recruitment
Recruitment for the study was conducted by the second author at somatic and mental health hospitals. The author was present at each ward for a period of time and recruited participants among somatic as well as psychiatric in- and outpatients. We made use of purposive sampling, including all patients who were willing to participate in the study and lived up to the inclusion criteria. Inclusion criteria for participants were 18+ years of age, native Danish speaking, assessed by the means of an Alcohol Use Disorder Identification Test (AUDIT) and scoring above 15 (indicating alcohol dependence), or assessed by the clinical staff using (International Statistical Classification of Diseases and Related Health Problems 10th edition (ICD-10); World Health Organization [WHO], 1992) as diagnosed with severe alcohol dependence. The final inclusion criterion was that the participant had never sought treatment for AUD.
One participant was recruited at the Department of Medical Gastrointestinal Diseases at Odense University Hospital. The screening for alcohol dependence was performed by the second author using an AUDIT, and the score was above 15. Two participants were recruited at the Gastro Unit, Surgical and Medical Division at Hvidovre Hospital. Three participants were recruited at the Mental Health Services in the Capital Region of Denmark. The participants were identified by the clinical staff at the hospitals; they had assessed them by the means of ICD-10 and diagnosed them as suffering from severe alcohol dependence. Patients were also recruited from general practice, but although initially agreeing to participate, they eventually declined participation.
Sample
In total, the sample thus consisted of six participants: two women and four men. Their average age was 58 years (range 41–74 years); the women were younger than the men. One of the participants was living together with a partner, the rest were living alone (as single, divorced, or widowed). Five of the participants had children and two of them had grandchildren. The participants had different education levels; varying from unskilled to trained doctor. One of the participants was working, the rest were not (due to retirement, early retirement, or unemployment). All of the participants had been using alcohol excessively for many years and were considered to be suffering from severe dependence by the staff of the hospital units. Besides that, they were suffering from liver cirrhosis, pancreas problems, schizophrenia, and bipolar disorder, and these illnesses were the reasons for their hospitalisation.
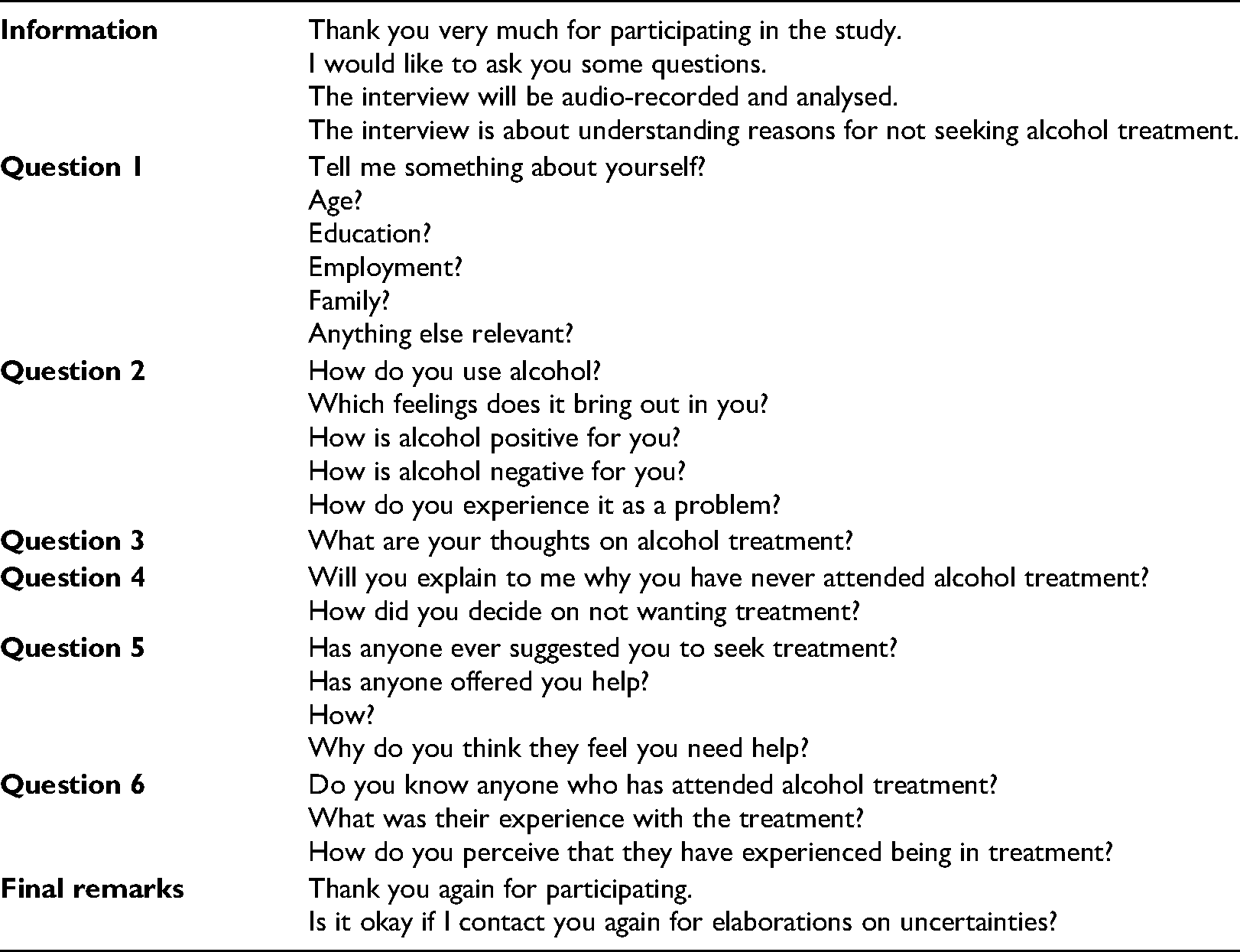
Data collection
After screening/assessment, eligible participants were approached by the second author, who holds a Master’s of Public Health and a PhD and has no experience of heavy alcohol use nor AUD herself or within her network. Neither did she have any work experience from the addiction field and had thus no pre-assumptions about AUD or treatment. After receiving verbal and written information about the study, the participants signed a consent form. The interviews were conducted by means of semi-structured, open-ended, and follow-up questions. The questions were formulated in an interview guide, which can be seen in Appendix 1. The participants were asked to describe their use of alcohol throughout their life as well as their perspectives on not seeking AUD treatment. The six interviews took place at the hospitals, but the participants had the opportunity to suggest other places. The interviews lasted between 18 and 62 minutes and had a mean duration of 36 minutes. They were audio-recorded and transcribed anonymously in full length. The given names of the participants were changed and specific information such as name of workplace and the like, was omitted. Data are securely stored.
Data analysis
According to the cognition researcher Bruner (1986), thinking takes form in two fundamentally different ways: paradigmatic thinking, which is expressed by logical arguments, and narrative thinking, which happens when people strive to understand, explain, and create coherence between incidents and experiences (Mattingly, 1991). A narrative approach will be applied to the present study, where the focus will be on how the individual makes sense of his or her actions.
Applying a health behaviour theory or conceptual framework such as the health belief model (HBM) can also be useful in understanding why a troubling number of persons with alcohol dependence do not seek treatment services. In brief, the HBM suggests that health behaviour is determined by an individual's assessment of threat (perceived susceptibility and severity), costs (perceived barriers), as well as perceived benefits. While several factors at different levels of influence can determine help-seeking behaviour, the HBM, which is a model of individual health behaviour, provides an appropriate lens to understand under-utilisation of alcohol treatment services among alcohol-dependent individuals, given that many efforts aimed at encouraging help-seeking focus on influencing behaviour at the individual level (Nutbeam & Harris, 2004).
The first four participants revealed narratives that were rather alike. As interviews five and six also presented similar narratives, we consider that data saturation was achieved. During the analysis, the transcribed interviews were read closely and repeatedly by two of the authors of this paper; first individually and thereafter discussed in detail. The analysis was constructed by first defining the basic logic of each narrative: what conception of alcohol use and treatment it reflected. The narratives were then categorised according to how they described alcohol use during life and by what they presented as the key to not seeking treatment. Eventually, composite stories were constructed, using parts of several original narratives. Mishler has called this method “constructing the told from multiple tellings” (Mishler, 1995). Often several categories of composite stories can be identified, and in the present material two composite stories were found. The narratives were then analysed in terms of the HBM, i.e., the individual's assessment of threat, costs, and benefits in relation to drinking and treatment-seeking and, with inspiration from Hänninen and Koski-Jännes, in terms of the emotional, explanatory, and moral meanings (Hanninen & Koski-Jannes, 1999). The emotional meaning refers to goals and what is considered of importance to the individual. The explanatory aspect of a narrative refers to causality and how events are linked. The way the events are explained, however, also has moral implications, since the explanation may allocate responsibility for the events.
Results
All participants were screened positive for alcohol dependence. They had all been drinking extensively throughout most of their lives, and in all cases their network had expressed concern. Nevertheless, none of them had ever sought or even considered seeking treatment for AUD, even though they all knew that the treatment system existed, and they all considered specialised, free, public treatment a good offer for people in need. A few participants had participated in a very small number of self-help meetings (Alcoholics Anonymous, AA). Two prominent narrative forms were recognised in the material, i.e., rather similar descriptions of how alcohol was a natural part of life and why treatment was not considered an option. The two stories are presented below.
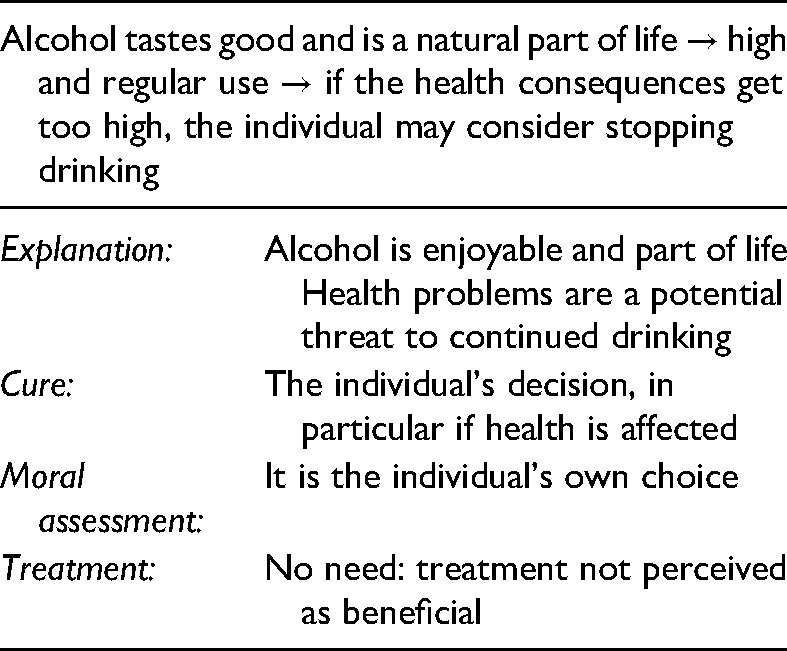
The “alcohol adds to the quality of my life and treatment is not for me” story
The first prominent story described how drinking alcohol had always been part of life since adolescence. Drinking was associated with quality of life. Drinking did not take place during working hours, but during lunch breaks and after hours. Drinking alone or with peers constituted the normal way of living for the individual. The drinking was described as quiet and calm: It has always been steady drinking with all too many beers every day. Only beer. I have never drunk spirits. (Peter, 67 years old)
Although the drinking often took place when the individual was alone, it was not hidden to the surroundings nor was it a secret. Alcohol was simply considered to be a natural part of life – just as natural as breathing, eating, relaxing, and watching television – and associated with a good life. The constant high intake of alcohol, however, raised concern among family and friends. The concern was expressed and did not lead to conflicts. Rather, the individual acknowledged it and felt comforted by the concern from others, but the concern did not lead to stopping or to decreased drinking, i.e., it was not perceived as a threat or cost. Neither did it lead to treatment-seeking: I feel that they are in their right to say that (recommend treatment), but I am, as I said, I am 41 years old, I can … I can decide for myself if I need treatment or if I should not seek treatment. But of course, it means something when your close ones think that I should seek treatment. (Marianne, 41 years old)
The individual expressed satisfaction with his or her current drinking and felt convinced that the drinking would continue if he or she felt like it. Thus, drinking alcohol was perceived positively as a quality of life, i.e., as a benefit in itself. The individual was convinced that, if needed, he or she would be able to stop drinking. One individual had recently completely stopped drinking because of health problems due to drinking, but regarded the decision to be temporary and a private decision that did not involve treatment.
The reason why specialised treatment was not considered an option in this composite story was described as it is just not for me: Of course I know what treatment is and so on, but I have always considered that it is not something I need. (Peter, 67 years old)
The individual would rather rely on his or her own ability to reduce his or her intake of alcohol if deemed necessary and rely on support from family. In the moral sense, the individual took full responsibility for drinking in this story: I am perfectly aware of the health consequences, I have … eh … I know that and, and, and … I am prepared that it's probably also going to hit me sooner or later. (Marianne, 41 years old)
The story's emotional, explanatory, and moral meanings are summarised in Table 1.
The “alcohol adds to the quality of my life and treatment is not for me” story.
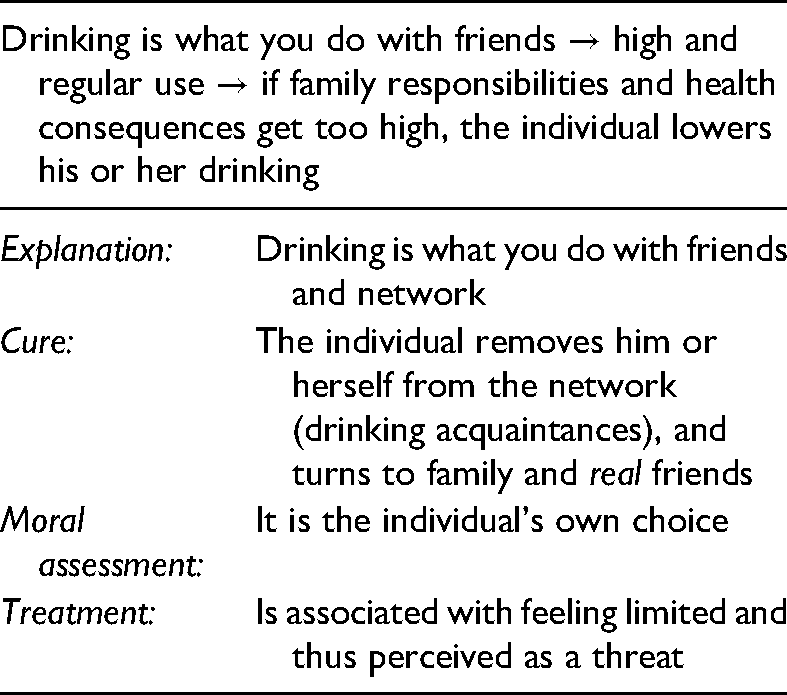
The “drinking with friends” story
The other condensed story from the material is the story about how excessive drinking is closely related to interacting with the social surroundings. Within this narrative, drinking was considered a social event; something you do with friends, colleagues, or drinking acquaintances. Therefore, decreasing drinking would mean removing yourself from your network. Drinking was described as so intertwined with being social that being social did not seem possible if drinking was not part of it, and drinking was thus perceived positively as being beneficial overall. Reduced drinking would be costly since it might lead to loneliness. Similar to the narrative above, this story also involved receiving concern from significant others and even concern from drinking acquaintances, and the concern was also described as having led to increased awareness of the alcohol intake. However, in particular, responsibilities for children and grandchildren led to decisions about lowering or stopping drinking, at least for a while: All of a sudden, I sat there with Maria, my second daughter, and thought: I don't want to do it (the drinking) anymore, it does not work. (Henrik, 65 years old)
Treatment was, however, neither in this story considered a relevant option. Instead, alternative coping strategies for lowering and controlling the alcohol intake were described. These strategies included only drinking on specific days (in contrast to every day), eating more, spending more time alone rather than with friends. Talking with professionals and receiving advice about how to cope or receiving therapy was not aligned with a feeling of autonomy, i.e., it was thus perceived as a threat for the individual's perception of feeling independent. Treatment was associated with restraints and limitations, and even noted as being degrading for the individual: It is degrading for one-self to – in treatment. All too many seek treatment for almost anything, right … (seeking treatment) is just like, like getting handcuffed, you cannot really move as you use to, as you feel like, but there is someone watching you all the time. (Henrik, 65 years old)
The individual would rather rely on his or her ability to reduce the intake of alcohol or turn to family and close friends for support. In the moral sense, besides the individual taking full responsibility for drinking within this narrative, he or she also acknowledged the potential need for support. The story's emotional, explanatory, and moral meanings can be seen in Table 2.
The “drinking with friends” story.
Health belief model
The individual's assessment of threat, costs, and benefits in relation to drinking and treatment-seeking was strikingly similar in the two identified prominent stories. Drinking was perceived as a natural part of the culture and of social settings, and drinking problems were perceived as being a personal matter. Mental and, in particular, physical health consequences were in both stories considered as prominent reasons for striving for control over the alcohol use, and even for stopping drinking for a while. Direct concern from close friends and near family members was a facilitating factor in the respect that it made the individual feel loved and also feel responsible: It started to become less and less meaningful to me as I became older, you cannot sit on a bench until four or five in the afternoon when you have a family to provide for. (Henrik, 65 years old)
The possibility of seeking treatment was, however, not an option in any of the stories, and the reasons were that treatment-seeking was seen as hampering the individual's autonomy or simply not necessary: It was my choice and my assessment that I did not want anything to do with that (…) I have always considered it something I did not need (…) I don't feel the need to enter professional treatment to get rid of the alcohol. (Peter, 67 years old)
Thus, since treatment was perceived as unnecessary and even a threat, in particular to the individual's autonomy, none of the individuals wanted to receive professional help to curb their alcohol use; instead, they all wanted to reach their goals independently. All the participants claimed full responsibility for taking this decision.
Discussion
The present study confirms the findings of prior studies hinting that hospitalised patients suffering from AUD may not be ready to or interested in considering specialised treatment for their drinking problems (Watson et al., 2015). In the present study, we found that the narratives told by the six patients, identified at hospitals as suffering from severe AUD, but who nevertheless had never sought treatment, were strikingly alike regarding: (1) their perspectives on alcohol use, (2) their attempts to gain control over their alcohol use, (3) their perceptions of health-related issues as well as relatives and relations as facilitators in obtaining what they were striving for, (4) their conceptions of alcohol treatment not being an attractive or relevant offer for them, (5) their feelings towards wanting to deal with their alcohol (non-)issues independently.
We found that the participants felt that alcohol was perceived as a natural part of life that added to their quality of life, or as an important aspect of social settings, in spite of the fact that the drinking was indeed heavy and even classified as dependent use by the hospital staff. This finding is in line with a qualitative study on service provision for alcohol-related health issues by Haighton et al. (2016), where the social element in drinking was found to be a barrier to changing due to concerns about losing the positive aspects of drinking. In addition, the participants in the present study had all been drinking for many years, little by little escalating their alcohol use to becoming excessive, and not all of them wanted to stop drinking altogether. This finding is corroborated by other studies, describing how the most common goal for changing problematic drinking is moderation (Emiliussen et al., 2019; Fucito & Hanrahan, 2015), just as it is a frequently reported reason for not seeking treatment (Probst et al., 2015).
The participants in the present study were not, however, hostile towards treatment-seeking, nor unknowing about the possibilities, and did not report that they considered treatment-seeking stigmatising. In fact, treatment was described in rather positive terms, and the participants had heard of the treatment offers from friends and family. However, there were two major reasons for not seeking AUD treatment imbedded in the stories told by the participants.
The first reason was the fact that the participants did not believe that alcohol treatment was a relevant offer for them. Not because of stigma or shame, rather they just felt that they would likely not benefit. This is similar to a 10-year study of factors associated with alcohol treatment use and non-use, where Chartier et al. (2016), found that barriers related to predisposing beliefs and fears about treatment as well as perceptions about treatment need increased during the 10-year period. They saw that the most commonly endorsed reason for not seeking help was related to the respondents’ (lack of) perception of treatment need. According to their findings, this reason represented four out of the five top reported barriers and increased during the decade. Also in a latent class analysis of perceived barriers to treatment for alcohol problems, Schuler et al. (2015) found that 33% of the participants believed that the problem would get better by itself, whilst 21% reported that their drinking problem was not serious enough for them to seek treatment for it. Furthermore, in a study about gender, acculturation, and other barriers to alcohol treatment utilisation among Latinos, Zemore et al. (2009) found that most individuals who avoided treatment did so because they did not believe they had a problem. In that study, the most commonly perceived barriers were that the treatment would not help or that the individual would not be understood. This finding was confirmed in a study of preferences and barriers to AUD treatment in alcohol-related cirrhosis performed by Mellinger et al. (2018), where the authors identified not wanting treatment as a key barrier to treatment-seeking, since about half of the participants in the study did not consider treatment as being necessary.
In the present study, the second reason for not seeking treatment was that the participants wanted to deal with their alcohol overuse issue themselves (if they felt that it even was an issue), not involving professional help. In fact, treatment was considered to tamper with a feeling of freedom and autonomy. This finding, again, has also been described in other studies. In their latent class analysis of perceived barriers to treatment for alcohol problems, Schuler et al. (2015) found the most frequently endorsed barrier to be the attitudinal belief among the participants that they would deal with the alcohol issue themselves. Forty-two per cent believed that they would be strong enough to handle it alone. In a study on barriers to help-seeking among American Indians with alcohol dependence, Venner et al. (2012) found personal barriers to be the most commonly cited. Here, 64% of the participants reported a barrier in this category, not believing that outside help was needed. In their study about reasons not to seek alcohol treatment, Probst et al. (2015) found the most frequent reason for not seeking treatment to be lack of problem awareness, which 55.3% of the participants responded. The participants did not consider their drinking to be a problem, nor did they feel that help was needed, and 20.9% of them stated wanting to cope alone as a reason for not seeking treatment. Mellinger et al. (2018) also noted that confidence in one's ability to remain abstinent from alcohol without treatment was an emergent theme. Findings from a qualitative study by O’Donnell et al. (2020) about patient experiences of alcohol screening and advice in primary care, suggest that patients use self-monitoring techniques in particular (which they perceived as learned through experience rather than based on clinical advice) to control their drinking. This is in line with findings from the study by Fucito and Hanrahan (2015), where participants used behavioural strategies to reduce drinking, e.g., changing their social environment, limiting how much alcohol they purchased, using controlled drinking strategies, staying busy, and changing their routines.
Although this was not a specific topic of the interviews performed within the present study, the stories also indicated two major groups of facilitating factors towards change of excessive alcohol use. The first factor seemed to be health-related issues; a finding also in line with several other studies, which found that facilitators to help-seeking included concerns about the risk of fatal illness (Chartier et al., 2016; Gilburt et al., 2015; Haighton et al., 2016; Mellinger et al., 2018; Naughton et al., 2012). Also in a qualitative study on patient experiences of alcohol screening and advice in primary care by O’Donnell et al. (2020), it was found that especially patients experiencing co-occurring health conditions saw alcohol advice as a valuable component of preventative healthcare.
The second facilitating factor towards rehabilitation seemed to be relatives and relations. This finding corroborates those of the study by Mellinger et al. (2018), where family and relationships were the most frequently cited motivation for change. Also in the qualitative study by O’Donnell et al. (2020), family, friendship, and relationships were identified as influencing drinking practices in multiple ways, from immediate practical concerns, such as needing to be sober to be able to parent younger children, to more long-term parenting ambitions, such as wanting to be a positive role model. In the qualitative studies by Haighton et al. (2016), and by Emiliussen et al. (2016), it was also found that facilitators to seeking help included motivation from significant people; thus, it seems that pressure from family and friends can build an impetus to change drinking behaviour. In addition, a narrative study on recovery from addictive behaviours by Hänninen and Koski-Jännes (1999) found that reasons for wanting to change (but maybe not succeeding) included spousal issues, becoming unemployed, and self-value problems.
We had assumed we would find structural reasons for not seeking treatment, such as lack of access to or knowledge about treatment offers, which would have tied in with findings from other studies (May et al., 2019). However, we did not recognise any such reasons in the stories told by the participants, who were all well-informed about public AUD treatment being a free offer. In addition, we had assumed we would find stigma and shame to be prominent reasons for not seeking AUD treatment as this would have supported findings from other studies. According to a recent review, stigma is the most prevalent barrier to AUD treatment-seeking (May et al., 2019). However, in the present study, the participants did not feel that their alcohol use was serious enough to require treatment; thus, they did not feel the need to hide it. These findings indicate that we may need to rethink the communication effort towards the non-treatment-seeking population. It seems that information about AUD treatment aimed at non-treatment-seekers, focusing on decreasing stigma attached to treatment-seeking and how it is possible to easily get in contact with the treatment system, may, in fact, not always be targeting a non-treatment-seeking population and may not be perceived as relevant. Instead, it seemed that health and family-related issues may act as facilitators for habit change and could therefore be an area where information and feedback were relevant as well as needed. This is supported by findings from the study by Fucito and Hanrahan (2015), where most participants reported that they did not relate to general health promotion campaigns but indicated that personalised health information would be motivating.
Since it seems that significant others are of crucial importance when it comes to signalling when reduction of alcohol use is needed, it points to the importance of implementing support for others to a larger extent in the treatment system. Of such methods, Community Reinforcement and Family Training (CRAFT) (Sisson & Azrin, 1986) is the only one with any evidence to support that it increases the likelihood of the person suffering from AUD actually seeking treatment. CRAFT is aimed at training significant others to become involved in the problem drinkers’ choice of treatment, helping significant others to handle situations between themselves and the problem drinkers, and finally helping significant others to develop specific strategies to take proper care of themselves in risk situations. This might be a possible way to reach a larger proportion of those in need of treatment.
Autonomy and viewing alcohol as a completely natural part of life that “had always been there”, both in relation to quality of life and in social settings, characterised the description of alcohol use by the participants in the present study, and in that respect, they described themselves within the narrative pattern of cultural drinkers (Nielsen, 2003). None of the participants described their alcohol as self-medication, as a reaction to other problems, or as a way of coping with something else. Rather, heavy alcohol use seemed to be part of their identity as described by Eriksen and Hoeck (2021). Considering the focus on autonomy and quality of life in the stories, identified in the present study, it can be hypothesised that in order to make treatment an attractive option, treatment interventions should not emphasise abstinence per se as the only possible treatment goal. Instead, interventions such as “guided self-change” might be attractive (Probst et al., 2015), at least as a first step towards change. Such a brief cognitive behavioural motivational intervention is designed to support patients in the process of becoming aware of and dealing with their alcohol use issues (Saladin & Santa Ana, 2004), comprising personal goal setting, self-monitoring of drinking behaviour, analysis of drinking situations, and learning alternative coping skills (Witkiewitz & Marlatt, 2011). Internet-based treatment may be another way to lower barriers to treatment-seeking and increase access to evidence-based treatment for individuals suffering from AUD (Andersson, 2016; Davies et al., 2019; Rogers et al., 2017). The potential benefits of such offers include ease of access and capacity to reach a wide range of users in a cost-efficient manner (Andersson, 2018).
Also, for people who suffer from a mild AUD and who are at increased risk but do not (yet) perceive a treatment need, primary care continuous monitoring and assessment of alcohol use to prevent AUD and physical health consequences may be relevant (Probst et al., 2015). Indeed, the present study indicates that such interventions are well-perceived rather than producing resistance, in spite of the fact that the interventions may not lead to treatment-seeking. Tailored screening, e.g., according to age (Haighton et al., 2016), gender (Venner et al., 2012), and culture (Venner et al., 2012; Zemore et al., 2009) could also be considered. The present study adds to the little insight into why SBIRT interventions at hospitals do not work as efficiently as hypothesised (Schwarz et al., 2018).
Strengths and limitations
It is a strength that we have recruited participants suffering from AUD, who have never sought AUD treatment, from both physical and psychiatric settings. Respondents were also recruited from the general practitioner's office but they chose to withdraw from the study prior to the interviews taking place. Therefore, it may be a limitation that only six respondents ended up participating in the study. However, in a trend report, Crouch and McKenzie (2016) argue that analytic, inductive, and exploratory studies are best conducted with a small number of participants to facilitate the interviewer's connection to the interviewee and enhance the validity of in-depth interviews. Further, in an experiment with data saturation and variability, Guest et al. (2016) found that the basic elements for meta themes occurred within the first six interviews. Their experiment suggests that a sample of six interviews might be sufficient to enable the development of meaningful themes and useful interpretations. Despite the limitations stemming from the small sample size, it is our hope that this study can serve as a basis for further research and discussion within the area.
Conclusions
This study has examined people who suffer from AUD and do not seek treatment’s reasons for not doing so. The investigation indicated that the participants felt that alcohol added to their quality of life and that they enjoyed using it in social settings. In addition, it seemed that there were two major groups of facilitating factors towards rehabilitation: (1) health-related issues, (2) relatives and relations. Finally, two major reasons for not seeking AUD treatment appeared: (1) that the participants neglected their problematic alcohol use and did not believe that alcohol treatment was a relevant offer for them, and (2) the fact that the participants wanted to deal with their alcohol overuse issue themselves and not involve professional help.
It is important to consider ways in which the existing treatment system is not meeting the needs of individuals who would benefit from services. Hearing directly from such individuals has the potential to be instructive. We encourage future research in the field to take into account the findings from the present and similar qualitative studies on patient-perceived barriers to treatment-seeking.
Research ethics and patient consent
The study was conducted according to current ethical standards. The protocol was presented for and approved by the Scientific Research Ethics Committee of the Region of Southern Denmark. The Danish Data Protection Agency gave permission to collect and store data (ID number 3499, record number 19/21386). The participants signed a consent form after receiving verbal and written information about the study.
Footnotes
Acknowledgements
The authors wish to thank the patients and staff at the Department of Medical Gastrointestinal Diseases at Odense University Hospital; the Gastro Unit, Surgical and Medical Division at Hvidovre Hospital; and the Mental Health Services in the Capital Region of Denmark. Especially, the authors wish to thank Professor Ulrik Becker and Associate Professor Bjarne Lühr Hansen for recruitment efforts.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was financially supported by the Psychiatric Research Foundation of the Region of Southern Denmark.
Appendix 1. Interview guide.
|
|
Thank you very much for participating in the study. |
| I would like to ask you some questions. | |
| The interview will be audio-recorded and analysed. | |
| The interview is about understanding reasons for not seeking alcohol treatment. | |
|
|
Tell me something about yourself? |
| Age? | |
| Education? | |
| Employment? | |
| Family? | |
| Anything else relevant? | |
|
|
How do you use alcohol? |
| Which feelings does it bring out in you? | |
| How is alcohol positive for you? | |
| How is alcohol negative for you? | |
| How do you experience it as a problem? | |
|
|
What are your thoughts on alcohol treatment? |
|
|
Will you explain to me why you have never attended alcohol treatment? |
| How did you decide on not wanting treatment? | |
|
|
Has anyone ever suggested you to seek treatment? |
| Has anyone offered you help? | |
| How? | |
| Why do you think they feel you need help? | |
|
|
Do you know anyone who has attended alcohol treatment? |
| What was their experience with the treatment? | |
| How do you perceive that they have experienced being in treatment? | |
|
|
Thank you again for participating. |
| Is it okay if I contact you again for elaborations on uncertainties? |