
Abstract
Aims:
(i) To examine whether mean consumption and prevalence of at-risk drinking are highly correlated across samples of older adults, and (ii) to explore whether sociodemographic and health characteristics of alcohol use differ across countries.
Method:
Cross-sectional surveys were conducted in four European countries, Norway, Denmark, Belgium, and Portugal, applying identical data collection methods and survey instruments in general population samples of older adults aged 60 to 75 years. Alcohol consumption was measured as units of alcohol per week, which provided the basis for categorising the two outcome measures: abstention (0 units/week) and at-risk drinking (8+ units/week). Cross-tabulations and logistic regression models were estimated to examine associations between sociodemographic and health characteristics on the one hand and alcohol abstention and at-risk drinking on the other.
Results:
Prevalence of abstention was highest in Portugal and lowest in Denmark, whereas at-risk drinking was more prevalent in Denmark and Belgium compared to Norway and Portugal. Among country- and gender-specific samples of drinkers, there was a strong positive correlation between mean consumption and prevalence of at-risk drinkers. Female gender characterised abstention, whereas male gender characterised at-risk drinking in all four countries. Other sociodemographic characteristics and indicators of health and wellbeing were differently associated with abstention and at-risk drinking across the four countries.
Conclusions:
A strong regularity in the distribution of alcohol consumption was observed in the samples of older adults. Gender was the only common factor associated with drinking behaviour across the four countries.
Alcohol use is among the highest-ranking risk factors for premature death and loss of healthy life years (Lim et al., 2013). In Europe, people live longer, and hence an increasing proportion of the population falls into the category “older adults” (Lutz et al., 2008). Along with this demographic shift is an enhanced research interest in various aspects of health and related risk factors in this population group, including alcohol use (Galluzzo et al., 2012). In comparison to younger adults, older adults are more susceptible to the negative effects of alcohol (Adams & Jones, 1998; Squeglia et al., 2014). This age differential in susceptibility is mainly due to the biological changes, the various health challenges, and the widespread use of psychotropic and other prescription drugs that are typically associated with ageing (Anderson et al., 2012; Galluzzo et al., 2012). More specifically, older people have, in general, less body fluid and slower liver function, implying less dose tolerance (Anderson et al., 2012). Moreover, older adults are more likely to suffer impaired balance, sight, and cognition, which deteriorate further under the influence of alcohol (Adams & Jones, 1998; Hartikainen et al., 2007; Squeglia et al., 2014; Woolcott et al., 2009).
Over the past few decades, alcohol use among older people increased in several countries, including Spain, the United States, Norway, and Sweden (Anderson et al., 2012; Breslow et al., 2017; Bye & Østhus, 2012; Hallgren et al., 2009). Considering the elevated susceptibility to harms from alcohol with increasing age, the increase in alcohol consumption among older adults has fuelled concerns regarding health consequences (Anderson et al., 2012). While the current cohort of older adults is more diverse with regard to health and social characteristics than earlier cohorts (Kuerbis et al., 2016), relatively little research has focused specifically on such diversity in older adulthood and alcohol use (Kuerbis et al., 2016). In the present study, we examine alcohol use across four European countries and in relation to various demographic and health characteristics, applying available survey data from a project on sexual health among older adults.
The four European countries studied included Belgium, Denmark, Norway and Portugal. These countries are relatively similar with regard to population size (range 5.3–11.4 million) and life expectancy at birth (81–82.5 years), and they are all high income countries, although with large variation in gross national income per capita (The World Bank, 2020). However, these countries differ in several ways regarding alcohol consumption that are of interest for the current study among older adults. First, according to data from 2016 (World Health Organization, 2018), the proportion of abstainers in the adult population varies, being highest in Portugal (31%) and lowest in Norway (21%). Alcohol per capita consumption (APC), which is measured in litres pure alcohol per inhabitant aged 15 years and older, varies also to some extent, and it is higher in Portugal (12.3), Belgium (12.1) and Denmark (10.4) compared to Norway (7.5). Consequently, total alcohol consumption per drinker is considerably higher in Portugal (17.8 litres) than in Norway (9.4 litres), leaving Belgium and Denmark in between (15.9 and 13.9 litres, respectively). Second, studies have suggested that birth cohorts who were in their early 20s during a period of high population drinking, developed heavier drinking habits than other cohorts into older age (Kerr et al., 2009). In the 1960s and 1970s, when today’s 60- and 70-year-olds were in their early adult years, the level of alcohol consumption varied markedly in these four European countries. Recorded alcohol per capita (15+) consumption was lowest in Norway (around 5 litres) and highest in Portugal (between 15 and 20 litres), with Belgium and Denmark in between (World Health Organization, 2018). Thus, the variation in current abstention rates and levels of alcohol consumption in the general population, as well as the large differences in population drinking half a century ago across these four European countries, may be reflected in the current drinking behaviour among older adults in these countries.
Two aspects of alcohol use are of particular interest in this respect: alcohol abstinence and at-risk drinking, that is, consumption exceeding low-risk drinking guidelines (Sacco, 2016). Alcohol abstinence is typically more prevalent in old age, although the prevalence rates of lifetime abstention and former drinkers vary considerably across studies and between countries and religious affiliations (Gell et al., 2014; Nuevo et al., 2015). Some people stop drinking due to poor health (“sick quitters”), and more frequently so in old age (Huth et al., 2007). Drinking typically occurs in social settings; with family, friends or colleagues (Mäkelä et al., 2012), and abstinence may therefore to some extent reflect a smaller social network or/and few social occasions when coming to old age.
Among drinkers, a consistent and strong pattern is found in the distribution of consumption (Sherk et al., 2017; Skog, 1985); that is, the mean consumption is strongly correlated with the proportion of heavy drinkers (i.e., those exceeding a given threshold), and hence, the higher the mean consumption, the higher the prevalence of heavy drinkers. This is reported from general population samples of adults and of adolescents (Brunborg et al., 2014; Norström & Svensson, 2014; Rossow & Clausen, 2013; Rossow et al., 2014; Skog, 1985). There seem, however, to be few, if any, studies that have examined this issue in samples of older adults.
In general population samples, alcohol use tends to vary along demographic, health and social characteristics. Men are more often current drinkers and are more likely to drink high volumes compared to women, although this gender differential varies by age and across countries (Wilsnack et al., 2009). Overall, the gender ratio in alcohol use seems to have decreased over time and is smaller in younger as compared to older cohorts (Slade et al., 2016). Moreover, people resident in urban areas drink more than those in rural areas (Dixon & Chartier, 2016); and there is some evidence that those in higher socioeconomic status (SES) groups tend to drink more than those in lower SES groups. Health characteristics are also associated with alcohol use; alcohol abstainers tend to report poorer mental and physical health than drinkers (Stranges et al., 2006), and they tend to be less satisfied with life (Massin & Kopp, 2014). Such patterns of socioeconomic and health variation in alcohol consumption are to some extent found also in studies of older adults. For instance, among older adults, consumption is higher among men than among women, and higher among those with high, as compared to low, SES (Jensen et al., 2018; Nuevo et al., 2015; Sacco, 2016), and there seems to be a positive correlation between alcohol consumption and good health (Nuevo et al., 2015). However, such sociodemographic and health differences in drinking behaviour may well vary between countries and drinking cultures.
Against this backdrop, the purpose of this study was to examine the prevalence and sociodemographic and health characteristics of alcohol abstention and at-risk drinking among older adults across four European countries with different alcohol consumption levels and to explore whether distributional patterns that have previously been reported in the general adult population apply also to older adults. More specifically, we aimed to (i) examine whether mean consumption and prevalence of at-risk drinking are highly correlated across samples of older adults, and (ii) explore whether sociodemographic and health characteristics of alcohol use differ across countries.
Methods
Participants, recruitment and procedure
On behalf of the Department of Psychology at the University of Oslo, Norway, the marketing research company IPSOS conducted a multinational survey on sexual health and ageing in probability samples of the population aged 60–75 years in Norway, Denmark, Belgium, and Portugal. This age group is often referred to as young older adults. The data from this multinational survey were made available for the present study. IPSOS was responsible for data collection and data processing in all countries. Ethics approval was overseen by IPSOS in accordance with European standards.
The data collection was conducted in two phases from October to December 2016. The first phase was a recruitment interview by telephone in nationally representative samples of the population aged 60–75 years. In Norway, Denmark, and Belgium, nearly the whole population – and thus the entire target group for this survey – is accessible by telephone (landline and mobile phone numbers). This enabled IPSOS to draw random and representative gross samples of the target group, provided that the name, address and age of the person specified, corresponded to the telephone subscriber. Thus, the initial gross samples in these three countries were selected with the same quality as samples from national population registers.
In Portugal, a complete and updated telephone register did not exist. For this reason, IPSOS employed a frequently used procedure when recruiting for telephone surveys in Portugal: (1) telephone numbers were first randomly selected from fixed phone directories and IPSOS’s own database of phone numbers; (2) to obtain a distribution representative of the population, participants were selected by age and gender; and (3) due to illiteracy problems, participants who had not completed primary school (ISCED 1) were excluded from the sample. This method corresponds to the standard procedure for public opinion surveys in the country. The gross sample comprised in total 7,607 persons (1,865 in Norway, 2,000 in Denmark, 1,742 in Belgium, and 2,000 in Portugal).
In the second phase, those who accepted participation in the recruitment interview received a postal questionnaire for self-completion at home, including a Freepost envelope to return the completed questionnaire. This method was chosen on the basis of experiences from previous studies on topics that may be regarded as taboo or very private. The questionnaires were coded with a unique number, so that IPSOS could identify non-responders from their lists of recruited participants. Two reminders were sent successively to non-responders, starting one week after the questionnaire was received by the participant. In Portugal, it was decided after a discussion with IPSOS to deliver the reminders by phone. Upon completion of data collection, IPSOS provided an anonymised data file to the project’s principal investigators.
Except in Portugal, the recruitment exceeded all expectations, in the sense that relatively many were interested in the study, and agreed to participate. Unfortunately, among the 2,000 potential Portuguese participants, 502 persons could not be reached by phone. In the recruitment interview of the remaining 1,498 Portuguese individuals, a majority agreed to participate. However, 561 declined participation after having received the questionnaire. The net sample size was 1,270 in Norway, 1,045 in Denmark, 990 in Belgium, and 509 in Portugal. Thus, overall, the response rates were 68% in Norway, 52% in Denmark, 57% in Belgium and 26% in Portugal. The number of survey participants by country is presented in Table 1.
Characteristics of the samples regarding socio-demographics, health and wellbeing and alcohol use, by country.
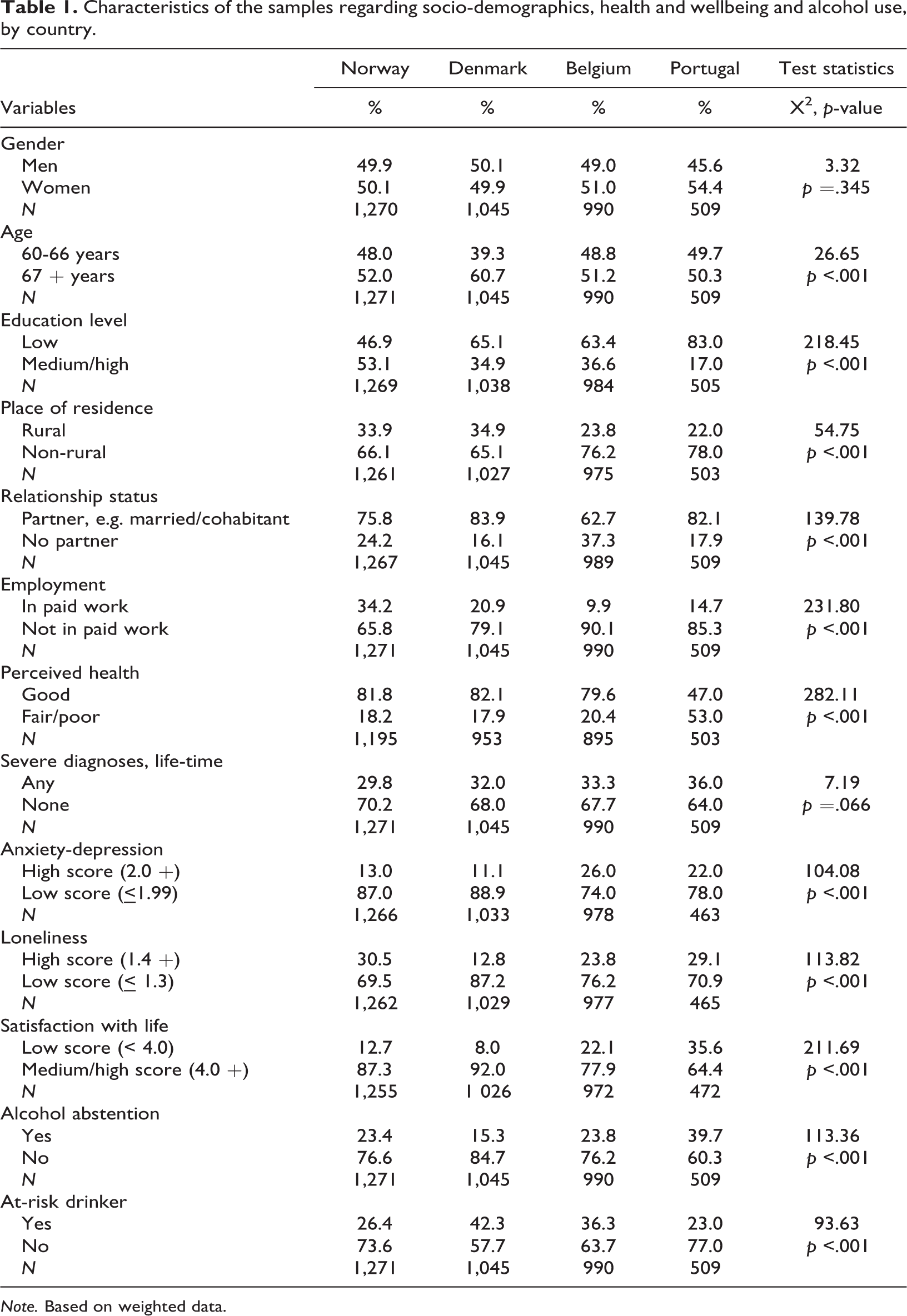
Note. Based on weighted data.
Survey questions
The questionnaire was developed in English and subsequently translated into local languages by the principal investigators and persons employed by IPSOS in each country. Most of the variables included in the questionnaire were selected from previous studies among the target group. An overview of the included survey questions is given elsewhere (Træen et al., 2019). The questionnaire took 20–30 minutes to complete.
Measures
Outcome variables
Alcohol consumption was assessed using a question from the Copenhagen Aging and Midlife Biobank (CAMB) study (Avlund et al., 2014): “On average, how many glasses of alcoholic beverages do you consume in a typical week?” One response category was “Do not drink alcohol”, and those indicating this response were categorised as abstainers. The other respondents were asked to state: Number of glasses of beer, Number of glasses of wine, Number of glasses of port wine, sherry etc., and Number of glasses of spirits, all in a typical week. No specifications were given regarding the volume for each beverage-specific glass. Missing observations were coded 0. The number of glasses of alcoholic beverages were summed across beverage categories and formed a continuous measure of weekly alcohol consumption, resembling units of alcohol per week. Those reporting 0 glasses of alcoholic beverages in a typical week were also categorised as abstainers. Those who reported alcohol consumption above the low-risk thresholds for the elderly (8+ drinks/week), according to guidelines (National Institute of Alcohol Abuse and Alcoholism, 2010) were categorised as at-risk drinkers. Thus, three outcome variables were applied in the analyses: the prevalence of abstainers, the number of alcohol units per week, and the prevalence of at-risk drinkers. The latter two were calculated among drinkers only, as there are good reasons, theoretically (Skog, 1985) and empirically (Sherk et al., 2017) to assume a positive correlation between mean consumption and prevalence of high consumption within the population of drinkers.
Explanatory variables
Gender was coded 1 = male, 2 = female, 3 = other (no participants gave this response).
Age was measured as a continuous variable and subsequently recoded into two age groups: 60–66 years and 67–75 years.
Level of education was assessed as the highest level of completed formal education. In three countries the response categories were 1 = primary school (6–8 years at school), 2 = lower secondary school (9–10 years at school), 3 = higher secondary school, high school (12–13 years at school), 4 = college, lower university level (bachelor’s degree level or similar), and 5 = higher university level (master’s degree, Ph.D. level or similar). In Belgium, additional response alternatives were added to mirror the education system structure in the country. To allow for cross-cultural comparisons in multivariate analyses, the variable was recoded into “Low/medium education” (including primary, lower secondary and higher secondary school) and “High education” (college, lower university and higher university level).
Urban–rural place of residence – “How would you describe the town or community where you live?” The response categories were 1 = rural (up to 5,000 inhabitants), 2 = small town (5,001–50,000 inhabitants), 3 = medium-sized city (50,001–200,000 inhabitants), 4 = suburb of a large-sized city (more than 200,000 people), 5 = downtown or in the central district of a large-sized city (more than 200,000 inhabitants), and 6 = other. Very few respondents (i.e., 1–2%) chose the latter category. For the present analyses, we recoded the variable into a dichotomous measure, separating those living in rural areas (Rural) and others (Non-rural, i.e., living in small towns or cities, and also including those who reported “other”).
Relationship status – “Do you currently have a steady/committed relationship with anybody? A steady/committed relationship also includes married/cohabiting persons.” The response categories were 1 = yes, 2 = no, and 3 = unsure. The 21 participants who were unsure about their relationship status were included in the “no” category.
Retirement status – Participants were asked “Are you currently…?: In paid work/employed, Retired from paid work, Looking after home or family, Doing unpaid or voluntary work, or Doing something else”. The option “Retired from paid work” (1 = yes, 0 = not ticked) was used in the present analyses.
General health status self-assessment was measured with the question “In general, would you say your health is…” and the response categories were 1 = excellent, 2 = very good, 3 = good, 4 = fair, and 5 = poor. We applied a dichotomous measure, separating those in the former three categories (termed “good”) from those in the latter two (termed “poor”).
Number of severe diagnoses was created from the question: “Has a doctor ever told you that you have any of the medical conditions listed below? Tick all that apply: heart attack/coronary artery disease, angina, other form of heart disease/stroke/diabetes, also known as high blood sugar/chronic lung disease (not including asthma)/Parkinson’s disease/epilepsy/If you are a man; prostate cancer? /If you are a woman; cancer in the uterus or ovaries?/If you are a woman; breast cancer?”. We applied a dichotomous measure separating those with one or several severe diagnoses (“1+”) from those with no such diagnoses (“0”).
Anxiety and depression scale – was assessed using the following items, originally from the Symptom Check List (SCL-25), and also included in the Common Mental Disorders Screening Questionnaire (CMD-SQ) (Søgaard & Bech, 2009): “During the past 4 weeks, how much were you bothered by: Feeling blue/Feelings of worthlessness/Thoughts about ending your life/Feelings of being trapped or caught/Feeling lonely/Blaming yourself for things, and Feeling suddenly scared for no reason/Nervousness or shakiness inside/Spells of terror or panic/Worrying too much”. The former six items constitute the SCL-6 depressive symptoms scale, and the latter four items constitute the SCL-4 anxiety symptoms scale. The response categories were 1 = not at all, 2 = a little, 3 = moderately, 4 = quite a bit, and 5 = extremely (Søgaard, 2009). The scale was then computed to determine the mean sum scores (Cronbach’s alpha = .87 for men and .88 for women), with higher scores indicating greater levels of anxiety and depression (theoretical range 1.0–5.0). Thus, this sum-score resembled the SCL-10 scale, although the latter applies four response categories covering the range from “not at all” to “extremely” (theoretical range 1.0–4.0) (Strand et al., 2003). For this reason, we applied a cut-off of 2.0, which is somewhat higher than the conventional cut-off of 1.85 to distinguish the majority with “few or no symptoms” of anxiety and depression from those with “moderate or severe symptoms” and high likelihood of a mental disorder (Strand et al., 2003).
The Satisfaction with Life Scale was also utilised (Diener et al., 1985). This scale consists of the following five items: “In most ways my life is close to my ideal”, “The conditions of my life are excellent”, “So far, I have gotten the important things I want in life”, “I am satisfied with my life”, and “If I could live my life over, I would change almost nothing”. The response categories ranged from 1 = strongly disagree, to 7 = strongly agree. The scale was then computed to discover the mean sum scores (Cronbach’s alpha = .90 for men and .91 for women), with higher scores indicating a greater satisfaction with life in general (theoretical range 1.0–7.0). A score of 4.0 represents the neutral point on the scale (Pavot & Diener, 2009). We dichotomised the scale and categorised those with a score below 4.0 as having “low satisfaction with life” (i.e., “extremely dissatisfied with life” or “slightly dissatisfied with life”; Pavot & Diener, 2009).
Loneliness scale was constructed from three of the items in the revised University of California, Los Angeles (UCLA) Loneliness Scale: “How often do you feel that you lack companionship?/How often do you feel left out?/How often do you feel isolated from others?” Response options were 1 = hardly ever, 2 = some of the time, and 3 = often. A mean from the sum of the scores was then constructed (Cronbach’s alpha = .78 for men, and .81 for women), and higher scores indicated more frequent feelings of loneliness (theoretical range 1.0–3.0). We dichotomised the scale with a cut-off close to the 75th percentile, and those who scored above 1.5 were categorised with a “high score” on the Loneliness Scale, and the others with a “low score”.
The distributions of explanatory variables and outcome variables by country are presented in Table 1.
Statistical analysis
Based on census data, weighting was used to match national samples to their respective population characteristics (age and gender) (DuMouchel & Duncan, 1983). To check for robustness, the analyses presented in this article were carried out on weighted and unweighted data.
The distribution of outcome measures and explanatory variables by country were described by cross-tabulation and Chi-square statistics. The relationship between the outcome variables and the explanatory variables was first examined bi-variately in cross-tabulations with estimates of crude odds ratios (ORs) within each country. Due to inter-correlation between explanatory variables, we explored the importance of sociodemographic and health characteristics for abstention and for at-risk drinking in each country in multivariate logistic regression analyses. Only explanatory variables that were statistically significantly associated with the outcome measures in the bi-variate analyses were entered into hierarchical logistic regression models, applying model fit criteria (log likelihood ratio), and the models were specified separately by country. Only the results from the final models are presented in Tables 3 and 4. All data analyses were performed using IBM SPSS 25.0 statistical software package.
Distribution of alcohol consumption by country and gender. Proportion abstainers among all respondents. Measures of central tendency and dispersion and proportion of at-risk drinkers among drinkers only.
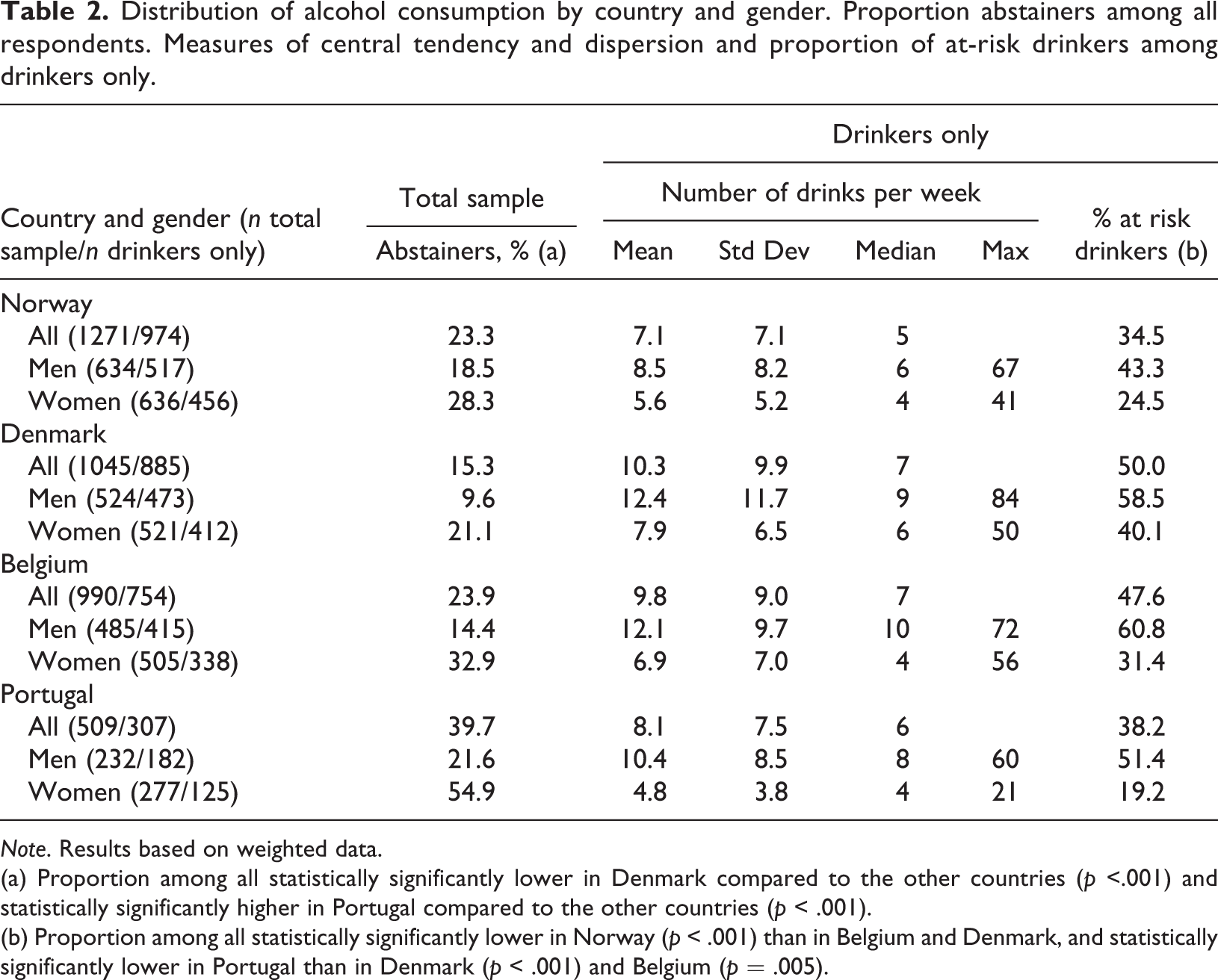
Note. Results based on weighted data.
(a) Proportion among all statistically significantly lower in Denmark compared to the other countries (p <.001) and statistically significantly higher in Portugal compared to the other countries (p < .001).
(b) Proportion among all statistically significantly lower in Norway (p < .001) than in Belgium and Denmark, and statistically significantly lower in Portugal than in Denmark (p < .001) and Belgium (p = .005).
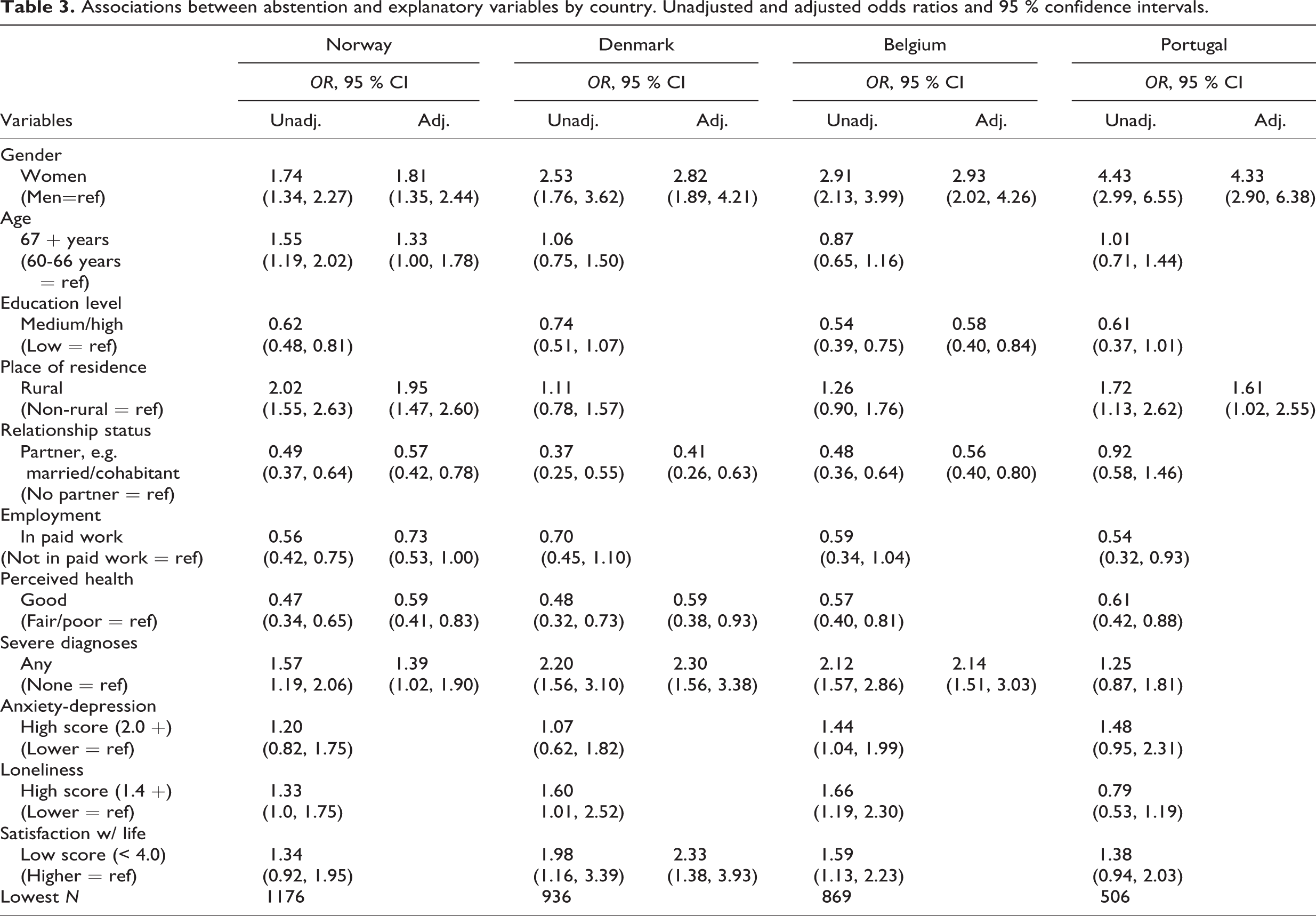
Associations between abstention and explanatory variables by country. Unadjusted and adjusted odds ratios and 95 % confidence intervals.
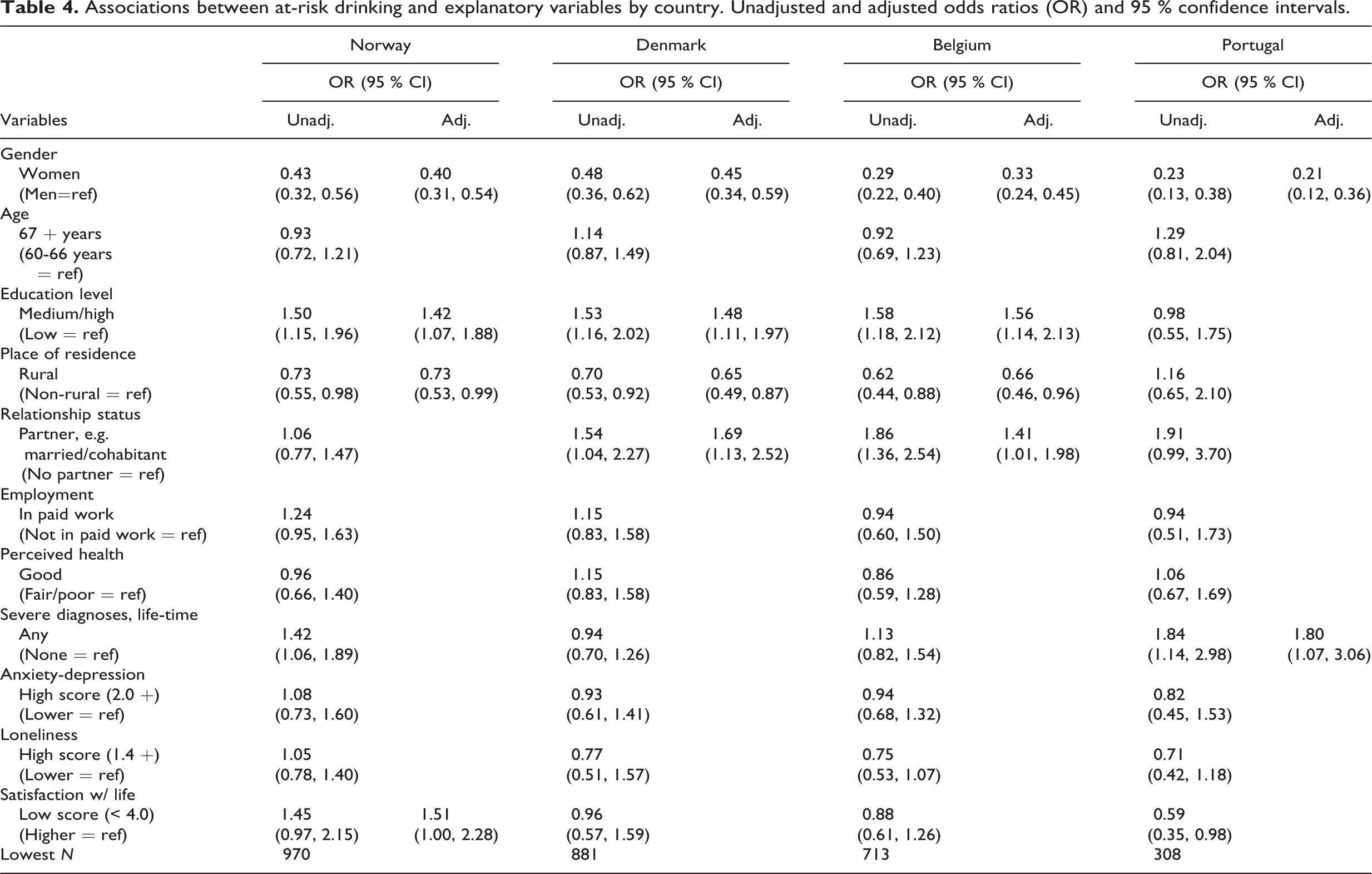
Associations between at-risk drinking and explanatory variables by country. Unadjusted and adjusted odds ratios (OR) and 95 % confidence intervals.
Results
The proportion of abstainers was, in comparison to the other countries, lowest in Denmark (15.3%, p < .001) and highest in Portugal (39.7%, p < .001), and systematically higher among women than among men (Table 1). The gender difference in proportion of abstainers differed by country and was statistically significantly smaller in Norway than in Portugal, as evident from non-overlapping confidence intervals (Table 3). Among drinkers, the mean weekly consumption was lowest in Norway compared to the other countries (p < .001), and highest in Denmark compared to the other countries (p < .001), whereas mean consumption in Portugal did not differ statistically significantly from that in the other countries (p = .102). In all countries, mean weekly consumption among drinkers was systematically higher among men than among women (p < .001 in all four countries), as was the dispersion of the distribution (Table 1). This pattern in mean consumption by country and gender was reflected in the proportion of at-risk drinkers (i.e., those consuming eight or more drinks per week) (Table 2). Again, the gender difference in mean consumption and prevalence of at-risk drinkers was smaller in the Nordic countries compared to Portugal (see Table 4 for ORs and confidence intervals). Across the eight gender-specific population samples, as described in Table 2, there was a strong positive correlation between mean consumption and prevalence of at-risk drinkers (Pearson’s r = 0.992, p < .001).
The likelihood of being an abstainer varied with sociodemographic characteristics, and indicators of health and social wellbeing in all four countries (see unadjusted ORs in Table 3). In multivariate analyses, the likelihood of abstention was elevated for females in all four countries, but to varying extents; the odds ratio was lowest in Norway and highest in Portugal (Table 3). Moreover, the importance of other explanatory variables varied across the countries. In three countries – Norway, Denmark and Belgium – one or several indicators of poor health were associated with alcohol abstention. These indicators were: perceived own health as fair/poor (one or several severe disease diagnoses), and low score on life satisfaction (Table 3). Having a steady partner decreased the likelihood of abstention in three countries (all but Portugal), having a medium/high education level lowered the likelihood in one country (Belgium), and rural place of residence increased the likelihood in two countries (Norway and Portugal) (Table 3).
Among drinkers, gender was a strong predictor for at-risk drinking. In all four countries, women were significantly less likely to be at-risk drinkers than men, and this association was stronger in Portugal compared to Denmark and Norway (Table 4). Having a medium/high level of education increased the likelihood of at-risk drinking in three countries (Norway, Denmark, and Belgium), as did non-rural residence in the same three countries. Having a steady partner increased the likelihood of at-risk drinking in two countries (Denmark and Belgium). Generally, the various indicators of health and wellbeing seemed to be of little importance for at-risk drinking, although with two exceptions: in Norway, at-risk drinking was elevated among those reporting low satisfaction with life; and in Portugal, at-risk drinking was elevated among those with one or more severe diagnoses (Table 4).
The presented results were based on weighted data. Re-running the analyses applying unweighted data, we found that in Norway, Denmark and Belgium, the estimates from weighted and unweighted data were very similar. In Portugal, the estimates differed somewhat between weighted and unweighted data, but also here, we obtained the same patterns of associations.
Discussion
This study showed that alcohol use among older adults varied considerably by gender and between four European countries, and among drinkers, the variation in prevalence of at-risk drinkers clearly reflected the variation in mean consumption. In all four countries, women were more often abstainers and less often at-risk drinkers, compared to men. Indicators of poor health were commonly associated with abstinence, but of little importance for at-risk drinking. Sociodemographic factors, including rural dwelling and high level of education, were associated with both abstinence and with at-risk drinking – although in opposite directions and to varying extents across countries.
Our findings corroborate the results of previous studies in several respects. The strong correlation between mean consumption and prevalence of at-risk drinkers is well in line with the extant literature, demonstrating a consistent distribution pattern of alcohol consumption and a systematic positive correlation between mean consumption and prevalence of high consumption across populations of drinkers (Brunborg et al., 2014; Norström & Svensson, 2014; Rossow et al., 2014; Sherk et al., 2017). The striking gender difference in abstention and at-risk drinking is well in line with meta-regression effects for similar age cohorts (Slade et al., 2016). The level of consumption in terms of alcohol units per week was of the same magnitude in the present study as compared to recent findings among the elderly in other European countries (Nuevo et al., 2015). The cross-country differences observed in our study do to some extent mirror those in the general population in these countries (World Health Organization, 2018); specifically the high proportion of abstainers in Portugal and the low mean consumption in Norway. On the other hand, in our sample of older adults, mean consumption and prevalence of at-risk drinkers among drinkers were of the same magnitude in Portugal and Norway. Taking into consideration that total consumption among all adult drinkers is currently almost twice as high in Portugal as compared to Norway, and that the difference was even larger half a century ago (World Health Organization, 2018), our findings did not corroborate those from previous studies in the USA, demonstrating that cohorts exposed to a wet society in their formative years were more likely do drink heavily in older age (Kerr et al., 2009).
When considering the substantial inter-country variation in abstention rates and indicators of at-risk or excessive drinking among older adults in other, mainly Eastern European countries (Nuevo et al., 2015), the inter-country variation observed in our study appears modest. A substantial inter-country variation in the proportion of hazardous drinkers was also found when comparing data from 17 European countries in the SHARE project (Bosque-Prous et al., 2017). However, the prevalence figures reported from the SHARE project were calculated from the total samples including abstainers, implying inflated inter-country variation.
The observed associations between indicators of poor health and alcohol abstinence have also previously been reported for older adults in Norway (Li et al., 2017) and Belgium (Hoeck & Van Hal, 2012), as well as in other countries (Sacco, 2016). A higher consumption with increasing education level or other indicators of SES is reported in several previous studies in the general population as well as among older people (Bosque-Prous et al., 2017; Holdsworth et al., 2017; Jensen et al., 2018; Li et al., 2019), and our findings are well in line with these previous observations.
Thus, the rates of abstinence and at-risk drinking and important predictors of these aspects of drinking behaviour among the elderly reported in the present study fit well into a growing epidemiological literature on alcohol consumption among older adults. The specific contribution of the present study is the cross-country comparison of these rates and associations. While there are indeed several publications providing fairly recent descriptions of the elderly’s alcohol use in many European countries (e.g., Bosque-Prous et al., 2017; Hallgren et al., 2009; Nuevo et al., 2015), they fail to obtain a comparative picture of the importance of various predictors across countries. A quite novel outcome of the present study is thus the finding of both common and country-specific predictors of alcohol use. We will discuss this in more detail in the following.
Comparing characteristics of alcohol use among older adults across the four countries, there were few commonalities and several differences. We found clear gender differences in abstention and at-risk drinking in all countries, as could be expected from previous studies (Nuevo et al., 2015; Sacco, 2016; Wilsnack et al., 2009). But, we also found that these gender differences varied by country, suggesting a north–south gradient among older adults; that is, larger gender differences in the south. However, data from the general adult populations in these four countries (World Health Organization, 2018) show very similar female:male ratios in abstention rates (around 2.4 in all countries) as well as alcohol consumption among drinkers (0.34 in all countries) (our calculations based on the WHO, 2018 data). In other words, a larger gender divide in alcohol use in Portugal compared to the Nordic countries was found only among older adults, not in the general populations. Across many countries, a narrowing of the gender gap in alcohol use is observed, with smaller gender differences in younger cohorts (Slade et al., 2016). It is suggested that this trend can be explained by changes over time in female gender role traditionality (Slade et al., 2016), as older cohorts to a larger extent uphold traditional gender roles (Seedat et al., 2009). Thus, our findings among older adults may possibly reflect the north–south gradient across European countries in values and attitudes towards gender equality (Arpino & Tavares, 2013).
Among the many inter-country differences with regard to characteristics of abstention and at-risk drinking, the most striking overall difference was that of Portugal compared to the other countries. This may to some extent be attributed to the smaller population sample and lower statistical power. However, it is noteworthy that in Portugal, abstention was more prevalent and to lesser extent associated with indicators of poor health and social wellbeing, as compared to the other countries. This may reflect that a “sick-quitter effect”, is of less importance when abstention is prevalent. Moreover, Portugal was an exception also with regard to the association between education level and at-risk drinking. While consumption was higher among those with medium or high education level in Norway, Denmark and Belgium, much in line with observations from general population surveys (Collins, 2016), this was not the case in Portugal, where a markedly higher proportion of the older adults had obtained only a low education level.
The findings of the present study add to the extant literature in several respects. First, the strong correlation between mean consumption and prevalence of at-risk drinking across samples of gender- and country-specific samples of drinkers is, to our knowledge, a novel finding in studies of older adults. Second, we found across the four European countries that female gender was the only common characteristic of abstention, and we found a north–south gradient in its relative importance. However, in the three countries with relatively low abstention rates, abstention was also characterised by one or several indicators of poor health and lack of partner. Third, with regard to at-risk drinking, we found that male gender was the only common characteristic across the four countries. With the exception of Portugal, at-risk drinking was also characterised by medium/high education level and non-rural area of residence, whereas there was no clear patterning in the importance of indicators of health and wellbeing across countries. Thus, even among relatively similar high-income countries in the western part of Europe, characteristics of abstainers or at-risk drinkers do not necessarily apply alike.
Study limitations
Several limitations of the present study should be noted. First, the sample was restricted to people in the age range 60 to 75 years (the so-called young-old age), and it seems likely that the findings are not generalisable to older age groups. Second, drinking pattern and heavy episodic drinking were not measured, and hence we lacked one important aspect of drinking behaviour and hazardous drinking in this survey. It should, however, in this respect be noted that heavy episodic drinking is, in general, quite infrequently reported among older adults. Third, we had only information about current drinking in a typical week, and hence we had no information about infrequent drinking, and we were not able to separate former drinkers and lifetime abstainers. As former drinkers may have stopped drinking for health reasons (so-called sick quitters), the association between health indicators and abstinence may well be reflected by such a mechanism (Stockwell et al., 2016), but we did not have data to examine this to any further extent. Fourth, the reported number of drinks on a typical week is likely downward biased, due to under-reporting and poor understanding of standard drinks units (Mongan & Long, 2015). Finally, no data were available on non-respondents, and it is therefore difficult to assess how non-response may have impacted the results. However, it is possible that sexually inactive ageing men and women were less likely to participate in this study, which, again, may have impacted sample representativeness in other respects, including health, relationship status and alcohol use. Non-response was particularly large in Portugal, leaving a small net sample of respondents with less statistical power to detect associations compared to the other countries.
Conclusions
Two aspects of drinking behaviour among older adults – non-drinking and at-risk drinking –varied in prevalence and with regard to several sociodemographic and health characteristics across four western European countries. Gender was the only common factor associated with drinking behaviour. Female gender characterised abstention, whereas male gender characterised at-risk drinking. Other sociodemographic characteristics and indicators of health and wellbeing were differently associated with abstention and at-risk drinking across the four countries, suggesting limited transfer value of individual characteristics of drinking behaviour across countries, even within the same world region. However, among the country- and gender-specific samples of drinkers, a strong positive correlation was observed between mean consumption and prevalence of at-risk drinking, suggesting that a strong regularity in the distribution of alcohol consumption applies also to older adults. Further studies are needed to broaden the epidemiological literature on alcohol use among older adults, particularly to better understand what influences drinking behaviour and how drinking impacts health and welfare in this population group.
Footnotes
Availability of data
The data used for the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Norwegian Research Council under the grant number 250637.