
Abstract
Aims:
To examine differences in help-seeking for mental health problems among migrants and non-migrants in Norway and to consider the role of symptom severity, acknowledgement of a mental health problem and region of origin.
Methods:
We used data from a cross-sectional, online Norwegian Country Public Health Survey conducted in 2021. A total of 32,126 people, aged 18+ years, were included in the analyses, of which 8% were migrants. Around 60% of these were from countries within the European Economic Area, associated countries or the UK, USA, Canada, Australia and New Zealand (EEA+).
Results:
Migrants from non-EEA+ countries showed higher odds of having sought professional mental health help than non-migrants, but this difference attenuated when controlling for sociodemographic factors, psychological distress and self-reported depression. An interaction revealed that at higher, but not lower, levels of psychological distress, non-EEA+ migrants had significantly lower odds of having sought help. Moreover, a stratified analysis indicated that this applied only to those without self-reported depression.
Conclusions:
At high levels of psychological distress, people from non-EEA+ regions living in Norway may not be getting professional support for mental health problems to the same extent as EEA+ migrants and non-migrants. This may especially be the case for those who do not perceive their symptoms as a mental health problem. Consequently, improving the ability to recognise mental health problems may be a possible avenue for reducing the treatment gap for migrants with high symptom levels, though longitudinal studies would be required to confirm this.
Introduction
Migration can be a challenging experience even for the most resourceful people. Migrants can face post-migration stressors such as disadvantages in the labour market, higher rates of poverty and difficult experiences pre- and during migration, which may impact their mental health [1]. Reports in Norway, for example, find higher rates of mental health problems among migrants compared with the majority population, though rates vary by country of origin and reason for migration [2]. Furthermore, the literature consistently observes a mismatch between the number of people with a migrant background who report mental health problems and those who get help from formal health services, such as a doctor, psychologist or other health personnel. This seems to apply to forcibly displaced as well as voluntary migrants [3 –5], particularly those who are newly arrived [6].
Someone’s ability or decision to seek help is impacted by a variety of different factors including both systemic and social factors, as well as individual factors like evaluated need (to what extent someone’s symptoms indicate they may benefit from professional help) and personal beliefs around mental health [7]. Among non-migrant populations, greater symptom severity can increase the likelihood of someone seeking help for mental health problems [8]. Many people do not seek help until their condition severely affects their functioning [9]. In other cases, symptom severity may lead to less willingness to seek help, due to internalised stigma, such as among those with severe depression [10]. Whether the relationship between symptom severity and help-seeking differs for migrants and non-migrants is unclear. One study finds that among refugee men, more severe symptoms may lead to lower rates of help-seeking [3], but research on migrants in general is limited.
A person’s evaluated need for professional help may also relate to mental health literacy; the ability to read, write and utilise health information to make informed decisions across various settings, such as at home, within the community and in healthcare facilities [11]. This might play an important role in help-seeking among people with a migrant background [12,13]. It is important to note that high or low mental health literacy is defined by the dominant model in the relevant cultural context. Culture may influence our understanding of what health and illness are, what causes them and how they ought to be managed [14]. As such, people from more culturally distant countries may not recognise or consider their symptoms as a mental health problem, or as something that could benefit from professional psychological treatment. A study among Somalis in Norway, for example, found that some participants conceptualised depression as a result of spiritual possession, stress as a result of social isolation and/or past trauma [15]. Similarly, another Norwegian study found that Syrian migrants appear hesitant to use the term depression to describe a vignette character displaying symptoms in line with ICD-10 major depression [16]. Thus, when looking at help-seeking, it is important to consider whether a person recognises or acknowledges that they have a mental health problem in line with the dominant model in the country. The relationship between recognition of a mental health problem and help-seeking may also differ for migrants compared with non-migrants, owing to the likelihood of experiencing greater barriers to care [17].
The current study investigates help-seeking for mental health problems among migrants and non-migrants, specifically examining the role of both symptom severity and acknowledgement of a common mental health problem in line with the dominant model in Norway. Given the high prevalence and recurring nature of depression [18] we use self-reported depression in the last 12 months as a measure of acknowledgement of a mental health problem that could benefit from professional help. High levels of psychological distress are often indicative of depression [19]. Further, in this study, we distinguish between migrants from European Economic Area or associated countries, UK, USA, Canada, Australia and New Zealand (EEA+) and migrants from non-EEA+ countries. People from countries outside of EEA+ countries tend to report higher rates of psychological distress [20]. Yet, they may be more likely to understand mental health differently from the dominant models in Europe [21] and, thus, may seek help to a lesser extent despite experiencing a high level of symptoms.
Our research questions are:
Do migrants have lower odds of seeking professional help for mental health problems than their non-migrant counterparts, even after controlling for symptom level (current psychological distress) and recognition of a mental health problem (self-reported depression)?
Does the relationship between help-seeking and symptom level differ for migrants and non-migrants?
Does the relationship between help-seeking and recognition of a mental health problem differ for migrants and non-migrants?
Does the relationship between help-seeking and symptom severity depend on recognition of a mental health problem and does this differ for migrants and non-migrants?
Materials and methods
Data source and procedure
We utilised data from a cross-sectional, online Norwegian Country Public Health Survey (NCPHS) conducted in 2021 in Vestfold and Telemark, which at the time of data collection was one county in the South of Norway (redivided into two counties in 2024). The aim of NCPHS is to give an overview of the health and quality of life of inhabitants in the county in relation to community characteristics. The study population was randomly drawn from the population register and inclusion criteria were being aged 18+ years, registered as resident in Vestfold and Telemark and having a personal identification number. This number is assigned at birth to Norwegian-born individuals and to all long-term residents from six months after registering migration to Norway. Migrants with a temporary identification number were excluded, as well as individuals living in institutions.
Invitations to participate in the survey were sent out to 90,211 individuals via email and SMS. Participation was voluntary and those who responded had to provide digital proof of identity. A total of 34,148 individuals participated, yielding a response rate of 37.9%.
Variables
Sought professional help
Participants were asked if they had sought help from a doctor, psychologist or other health personnel due to mental health problems in the last 12 months (yes/no).
Current psychological distress
The Hopkins symptom checklist five-items scale (HSCL-5), shortened from the HSCL-25 item scale, is a brief instrument for assessing symptoms of anxiety and depression [22]. It includes two items representing anxiety (e.g. feeling fearful) and three representing depression (e.g. feeling hopeless about the future). Participants were asked to rate how, on a scale of 1 (not at all) to 4 (extremely), bothered they were by each symptom in the past week. Reliability in the current sample was very high (α=0.91). A mean score was calculated for all participants responding to at least four items, where a higher score indicates a higher symptom level.
Depression <12 months
Determined by the question: ‘Have you had depression in the last 12 months?’ (yes/no).
Migrant group
Participants were asked ‘Are you, or at least one of your parents, born abroad?’ (yes/no). Those who responded no were categorised as non-migrants. Those who answered positively were asked to indicate their own, and their mother and father’s, country of birth. We used this information to identify migrants (those born abroad, with two foreign-born parents). This is a standard definition used by Statistics Norway [23]. Migrants were further divided into two groups, based on their own country of birth: those born within the EEA or associated countries, or the UK, USA, Canada, Australia and New Zealand (EEA+), and all other countries (non-EEA+). Individuals who indicated that they, or their parent(s), were born abroad, but did not report their own or both parents’ country of origin were excluded in this study (n=263). We also excluded individuals who were born in Norway with migrant parent(s) or who were born abroad with Norwegian parent(s)) (n=1635).
Sex
Extracted from the Norwegian Population register during sampling: man/woman.
Age group
Age was extracted from the Norwegian Population Register during sampling and grouped into 18–24, 25–34, 35–44, 45–54, 55–64, 65+ years.
Partnership status
Participants were asked to indicate whether they were married, cohabiting or single.
Educational attainment
Measured with the question: What is your highest level of completed education? Responses were grouped as: ⩽compulsory education, upper secondary education, lower tertiary education (e.g. Bachelor’s degree) and upper tertiary education (e.g. Masters/PhD).
Employment status
Participants were asked to indicate their employment or life situation. Responses were grouped into: working (employed/self-employed), student/compulsory military or civil service, retired (including early retirement) or otherwise out of the workforce (sickness absence, unemployed, disability pension, homemaker, etc).
Missing data
Since sought professional help was our dependent variable, we excluded individuals who did not respond to this question (n=114). Less than 1% of the remaining data was missing and less than 5% of individuals had at least one missing value. We therefore imputed the remaining data with the mode for the categorical variables and the mean for current psychological distress.
Analyses
To investigate differences in the characteristics of the sample by migrant group, we conducted chi-square tests and a Kruskal–Wallis test. We centred current psychological distress to ease interpretation in the main analyses. Bivariate logistic regression analyses were conducted for each covariate before adjusting for all significant sociodemographic variables to determine whether there were differences in the odds of help-seeking across migrant group. Current psychological distress was added to the model, followed by depression <12 months. In separate analyses, we tested for an interaction between migrant group and a) current psychological distress and b) depression <12 months. Finally, we stratified the sample by depression <12 months and tested for an interaction between migrant group and current psychological distress. We calculated and plotted marginal predicted probabilities to visualise interactions. Analyses were conducted in STATA version 18.
Results
The final sample consisted of 32,126 individuals. Table I shows the characteristics of the sample by migrant group. Only around 7% of the sample were migrants and 60% were from EEA+ countries. There were significant differences across the migrant groups on all variables except sex.
Characteristics of the study sample by migrant group, n (%).
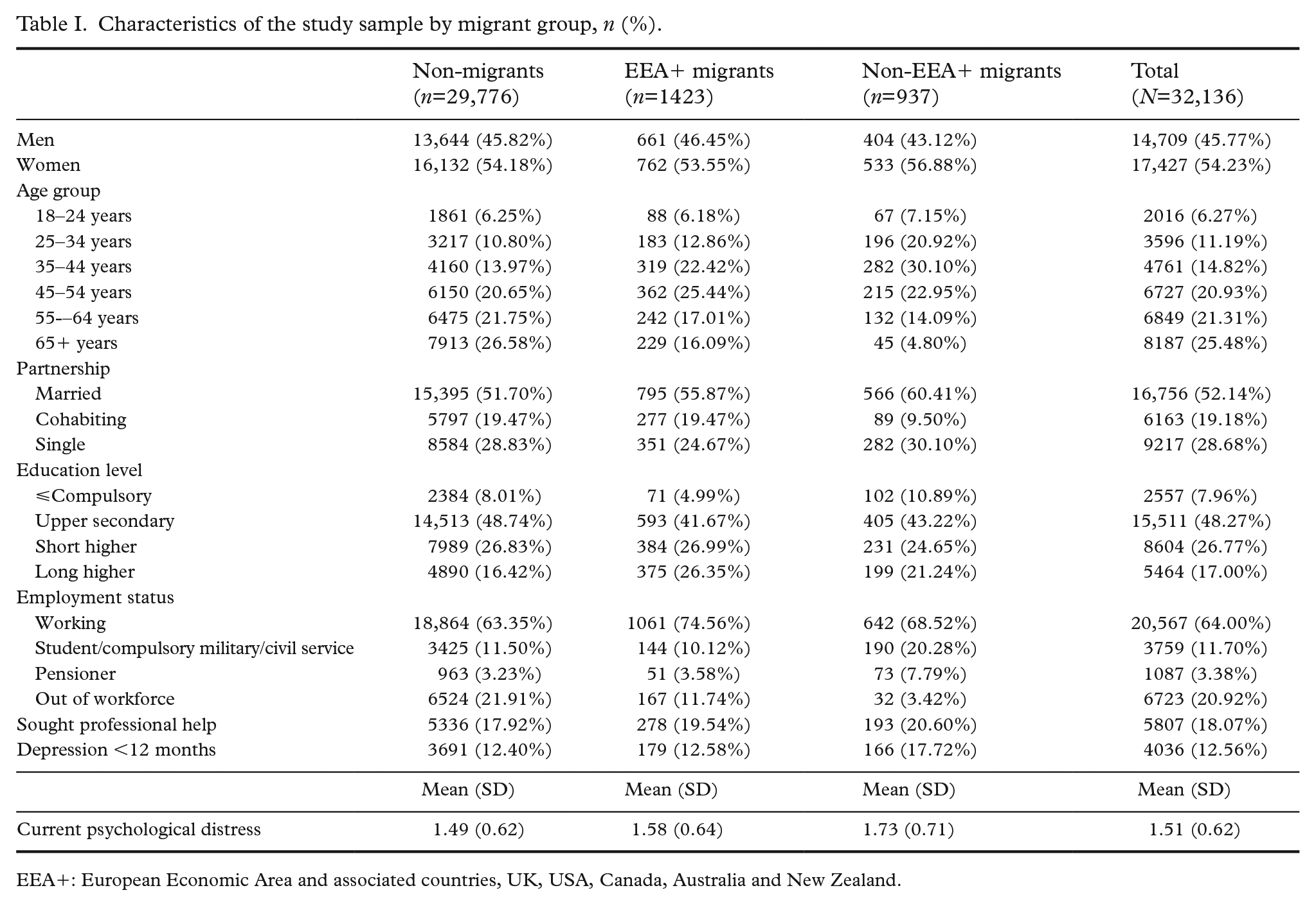
EEA+: European Economic Area and associated countries, UK, USA, Canada, Australia and New Zealand.
Although non-EEA+ migrants had higher odds of seeking professional help for mental health problems to a greater extent than non-migrants (Table II, bivariate models), after adjusting for sociodemographic variables, this difference was not significant (model 1). When adjusting for current psychological distress, non-EEA+ migrants but not EEA+ migrants had lower odds of help-seeking (model 2) than non-migrants. Adding depression <12 months to the model (model 3), however, rendered the differences between the groups insignificant.
Odds ratios (OR) and 95% confidence intervals (CI) for help-seeking.
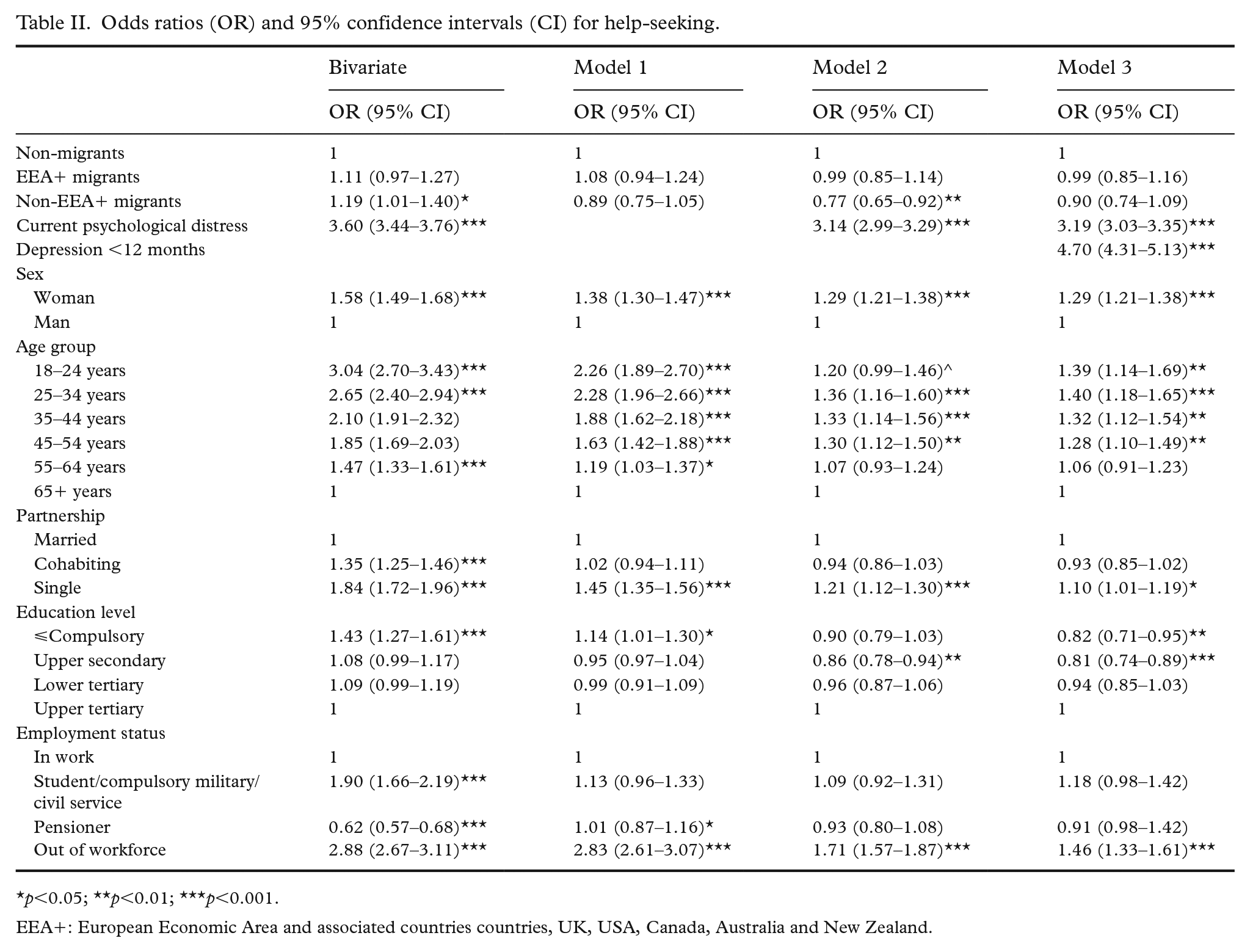
p<0.05; **p<0.01; ***p<0.001.
EEA+: European Economic Area and associated countries countries, UK, USA, Canada, Australia and New Zealand.
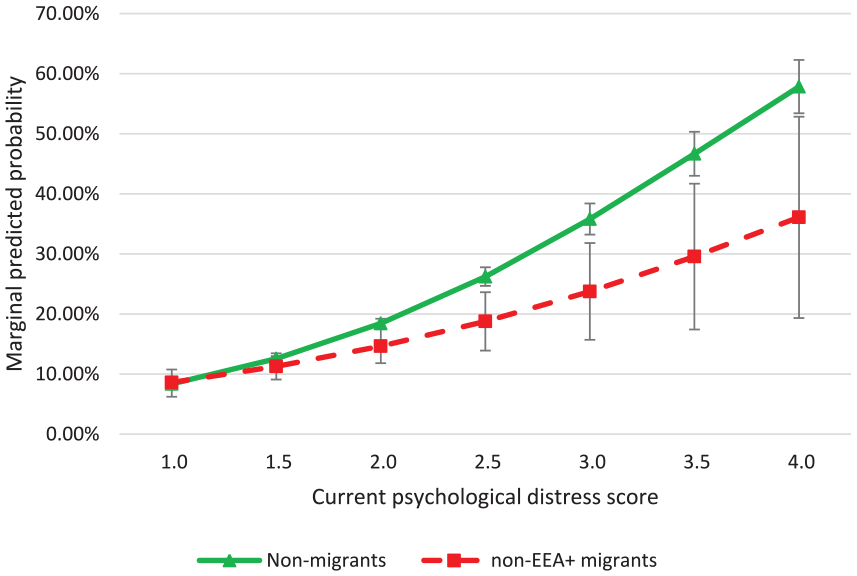
Table III shows the results of the interaction analyses. In model 1, there was a significant interaction between migrant group and current psychological distress for non-EEA+ migrants. We calculated and plotted marginal predicted probabilities for non-migrants and non-EEA+ migrants to visualise this interaction (Figure 1). For those with low levels of current psychological distress, there was no significant difference in the predicted probability of help-seeking, but as levels of distress increased, the predicted probability of seeking help increased more rapidly for non-migrants compared with non-EEA+ migrants. Among those with the highest level of current psychological distress, 30.1% of non-EEA+ migrants had sought help compared with 49.2% of non-migrants.
Adjusted odds ratios (OR) and 95% confidence intervals (CI) for help-seeking with interaction effects. a
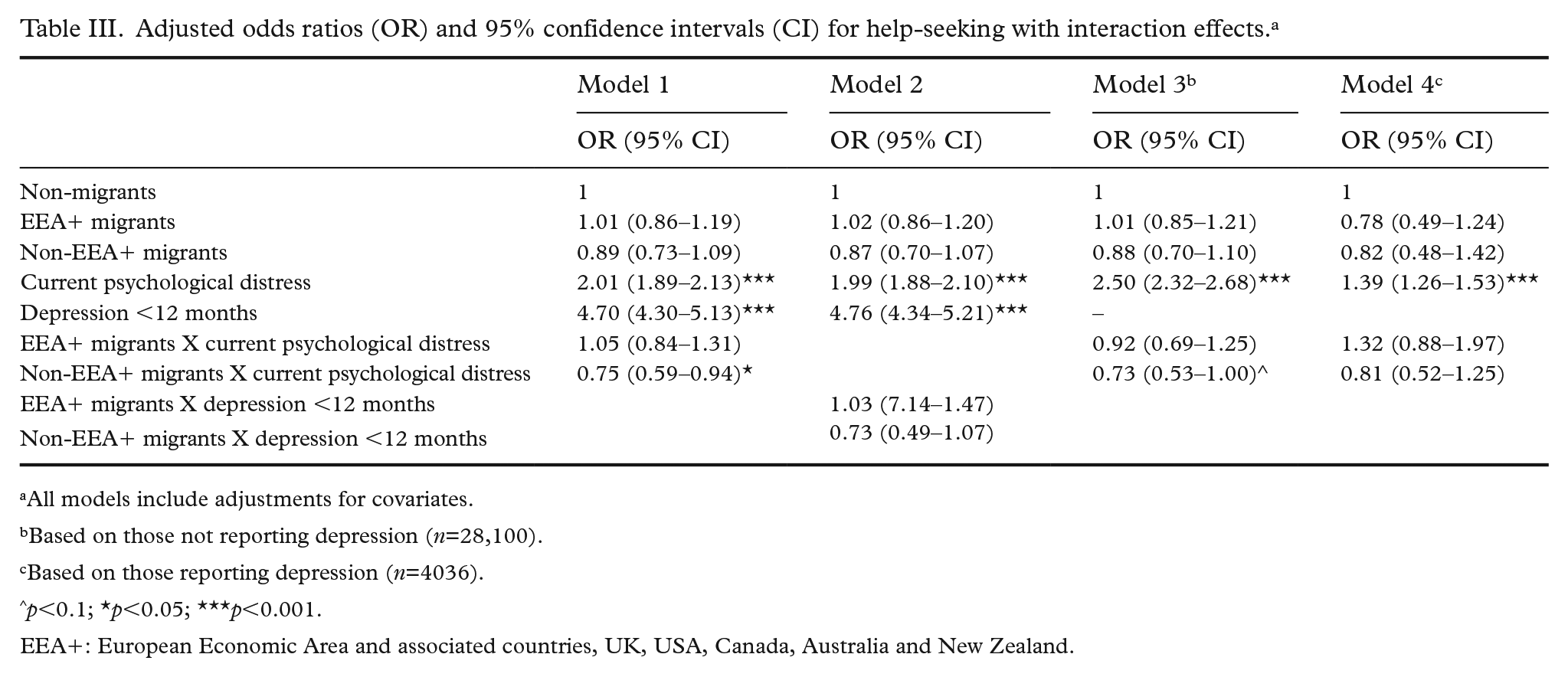
All models include adjustments for covariates.
Based on those not reporting depression (n=28,100).
Based on those reporting depression (n=4036).
p<0.1; *p<0.05; ***p<0.001.
EEA+: European Economic Area and associated countries, UK, USA, Canada, Australia and New Zealand.
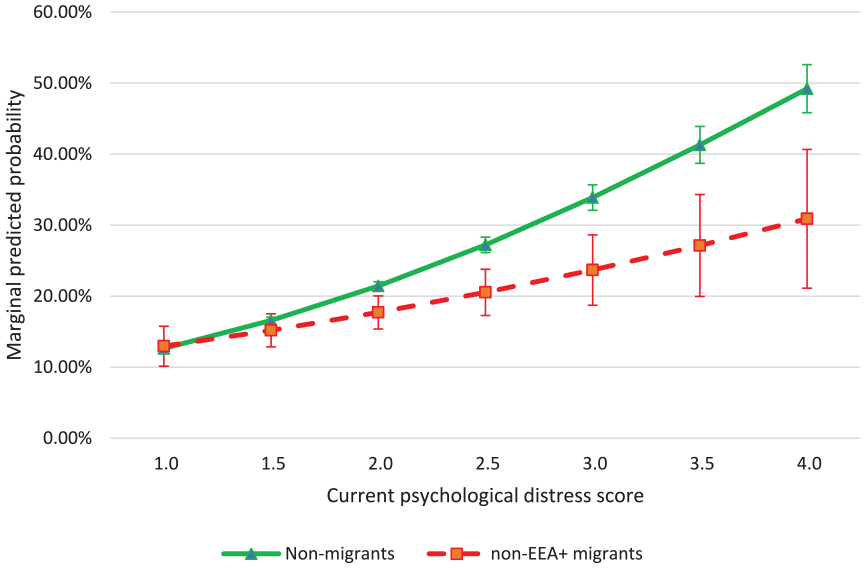
Marginal predicted probabilities (%) of having sought professional help by current psychological distress score and migrant group.
We found no significant interaction between depression <12 months and migrant group (model 2).
When we stratified by self-reported depression, we found no differences in the relationship between current psychological distress and help-seeking across migrant group for individuals who reported depression (model 4).
Yet, there was a tendency for a weaker relationship between current psychological distress and help-seeking for non-EEA+ migrants compared with non-migrants among those who did not report depression (model 3). Plotting marginal probabilities showed that the predicted probability of seeking help again increased more rapidly for non-migrants compared with non-EEA+ migrants (Figure 2). Among those with the highest level of current psychological distress but no self-reported depression, only 36.1% of non-EEA+ migrants had sought help compared with 57.9% of non-migrants, a difference of almost 22%.
Marginal predicted probabilities (%) of having sought professional help by current psychological distress score and migrant group among those without self-reported depression <12 months.
Discussion
The present study investigated help-seeking for mental health problems among migrants compared with non-migrants and found that non-EEA+ migrants have higher odds than, and EEA+ migrants the same odds as, non-migrants of having sought help from a doctor, psychologist or other health personnel owing to mental health problems in the last 12 months. This difference, however, attenuated after accounting for sociodemographics, psychological distress and self-reported depression. This finding is surprising given that studies of mental healthcare service use in Norway show that migrants in general, with few exceptions, are underrepresented [6,24,25]. However, in register studies, we capture only migrants using public services. Participants could be using private healthcare services in Norway or (digital) healthcare services in their home country. Previous research suggests some migrants may organise healthcare visits whilst visiting their home country [26,27]. Future research should consider alternative sources of help, both professional and non-professional, that migrants may use.
Another explanation for our findings is that the study sample is not representative of migrants in general. Indeed, the survey was offered only in Norwegian. We can therefore assume a high level of language proficiency among most participants. Our migrant sample more often had tertiary education and were in employment than the non-migrant sample. More than 70% had been in Norway for at least 10 years. High language proficiency, long length of stay, higher education and employment are all likely to be associated with a better understanding of, and ability to navigate, the health system, which can ultimately facilitate access to health services [28]. Migrants participating in this study may therefore be more able to seek help when required than migrants not participating. Thus, our findings do not apply to those with fewer resources or different levels of integration.
Although there were no overall differences in help-seeking between the groups, we found that non-migrants with a high symptom level had a significantly higher marginal predicted probability of having sought help than non-EEA+ migrants. The difference in probability of help-seeking between these two groups increased with increasing symptom level, suggesting that symptom severity plays a larger role in help-seeking for non-migrants than for non-EEA-migrants. Symptom severity may lead to higher levels of internalised stigma, which in turn may lead to lower levels of help-seeking. This has been observed among the majority population (10), but our findings might suggest it applies to a greater extent to migrants from non-EEA+ countries. This fits with research suggesting high levels of stigma surrounding mental health among many migrant groups from non-EEA+ countries [12,21], since group norms may be internalised. Future studies should examine variations in stigma, both anticipated and internalised, among groups of people from different world regions to test this.
Notably, when stratifying the sample by self-reported depression, we also found a tendency for a weaker relationship between psychological distress and help-seeking among those who did not report (and therefore did not recognise) depression but not for those who did recognise depression. This might suggest that the lower level of help-seeking among non-EEA+ migrants with a high level of symptoms is in part due to not perceiving the symptoms as a mental health problem. Qualitative studies have documented different understandings of depression among various migrant groups compared with the dominant model in Norway [15,16]. Together, this may suggest that there is a need to improve the recognition of mental health problems among non-EEA+ migrants. Longitudinal studies from the majority population suggest that mental health literacy predicts help-seeking [29]. There is, however, a lack of research on mental health literacy interventions and the effect on help-seeking among migrants, despite the considerable evidence of lower levels of health literacy among migrants in general [30].
It should be noted that this study uses a cross-sectional design. We therefore cannot be sure that the difference in findings for those who did and did not report depression is because those who recognised their symptoms as depression sought help. It is plausible that those who sought help because of their symptoms would later identify their symptoms as depression. There are, to our knowledge, no relevant longitudinal studies on symptom severity and recognition among migrants. Further, our psychological distress measure was related to the previous week, while help-seeking and self-reported depression was based on the last year. Since we do not know how long the distress has lasted, help-seeking could be low among those with more recent problems. Migrants, particularly non-EEA+ migrants, are thought to delay or avoid help-seeking due to a number of systemic, interpersonal and individual barriers [4,5,21]. It is possible that help-seeking would be slightly higher among those who have experienced psychological distress over a longer time period.
Help-seeking may also vary considerably within our broad categories of migrants, particularly for non-EEA+ migrants, where dominant models of mental health are likely to vary substantially more. Unfortunately, it is challenging to conduct robust research and draw conclusions on relatively small groups of people from more specific countries or regions. The relationships between current psychological distress and help-seeking could also vary within groups, depending on the person’s gender, age or education level. Future research could consider an intersectional approach.
Finally, HSCL-5 can be indicative of symptoms of both depression and anxiety [19]. Participants were not asked whether they had experienced anxiety in the previous 12 months. If anxiety is more common among non-migrants than non-EEA+ migrants, it could potentially explain the differences between these groups in the relationship between psychological stress and help-seeking among those without self-reported (and therefore recognised) depression in line with the dominant model in Norway.
Conclusion
The positive association between mental health symptom severity and help-seeking is weaker for migrants from non-EEA+ countries than for non-migrants. There may be a mental health treatment gap between non-migrants and non-EEA+ migrants at high levels of psychological distress, especially when a mental health problem is not recognised. Given that we found this gap among a relatively resourceful sample of migrants, we can assume the true gap is far greater. This treatment gap needs to be addressed to ensure equity in mental health care.
Footnotes
Acknowledgements
The authors express their gratitude to everyone involved in data collection for the Norwegian Country Public Health Survey, Vestfold and Telemark and to the team at the Norwegian Institute of Public Health who prepared the data file for the current research.
Data availability
Data used in this study may be available upon request from the Norwegian Institute of Public Health and after permission from the necessary ethical boards.
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Ethical approval for this study was granted by the Regional Committee for Medical and Health Research Ethics, South East Norway (REK: 409177).
Consent to participate
All participants provided consent for their data to be used for research purposes.