
Abstract
Few researchers have explored Canadian migrants’ experiences of mental health and service access. We interviewed 10 migrants to Canada from a local settlement organization about mental health and services and 5 organization staff about their experiences supporting migrants’ mental health and service access. Our interviews with migrants revealed cultural perceptions of mental health and unmet service needs. Our focus group with staff indicated challenges experienced by migrants and the tension between their openness with mental health difficulties and stigmatization from their cultural communities. A call to restructure existing mental health support for this underserved population is needed.
Health and Well-Being
According to the World Health Organization (WHO), 1 health has been defined as “… a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.” Mental health is integral to overall health. 2 In 2018, the WHO described mental health specifically as “… a state of well-being in which an individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and is able to make a contribution to his or her community.” 2 General well-being is integral for meaningful contributions to one's personal and community life.
Migrant Mental Health
Unfortunately, difficulties with mental health are a growing global concern affecting approximately 1 in 5 individuals every year.3,4 North American research has also shown that 75% of all mental health challenges occur between childhood and the end of young adulthood and are highest among those in young adulthood.5,6 O’Connell et al. 6 found that the most frequently reported mental health concerns among young adults were substance dependency, attention deficit hyperactivity, and anxiety and depressive disorders. Mental health problems may be elevated during young adulthood, given that it is a period when individuals undergo many critical developmental changes as they transition from being a child to becoming an adult. 5 It is therefore vital to explore the experiences of young adult migrants, given that early adulthood is a developmental period during which mental health may be problematic.
While general research on mental health in adults has been growing, relatively fewer research studies focus on the mental health of immigrants, who have unique mental health concerns compared to nonimmigrants. Wood and Newbold 7 found depression, anxiety, and posttraumatic stress disorder were the most frequent diagnoses among immigrants to Canada. In a sample of immigrant women, O’Mahony and Donnelly 8 identified serious mental health illnesses, including schizophrenia, depression, and postmigration stress disorder, in addition to depression and anxiety being the most common mental health problems. Lasry 9 identified that anxiety levels were higher among Canadian immigrants than native-born Canadians, which may be associated with the stresses of the immigration process. A focus on immigrants’ mental health is essential, given that immigrants to Canada in particular comprise a growing proportion of the population. Canada has one of the highest immigrant admission rates compared to any other country when examined annually, at approximately 30%, 10 an increase from 21.9% 11 in 2017. Research on immigrant mental health highlights a need for social programming that is individualized and sensitive to the needs of newcomers.
Migration and Mental Health
Challenges associated with migration, such as limited employment opportunities, financial difficulties, and language barriers, may substantially impact immigrants, making them particularly vulnerable to new and continuing mental health challenges. Displacement (ie, relocating from their country of origin) is likely to impact mental health, mental health-seeking behavior, and successful treatment. 12 Mental health may be negatively influenced when immigrants live in low-income situations. 13 Immigration status and the uncertainties awaiting a final decision on residency status are also linked to poor mental health. Kim et al. 14 found that adolescents from families with undocumented newcomers were at an increased risk of experiencing anxiety compared to fully documented families. Immigrants’ unique mental health challenges merit further empirical attention.
Mental Health and Service Perceptions
Various social–environmental factors may negatively influence how migrants perceive their mental health and experience and utilize related health services. Findings across individual studies comparing immigrants’ self-reported mental health status compared to Canadian-born people have been mixed. Interestingly, in a systematic review, Vang et al. 15 concluded that results generally support the “healthy immigrant effect,” such that immigrants’ mental health appears to be better than native Canadians’ mental health. This effect typically occurs through the migration screening process, whereby immigrants are less likely to declare conditions or disabilities and more likely to report good health. 16 This effect may relate to heightened experiences of fear and stress during the intake process. Following the migration process, how the treatment is offered to migrants compared to native residents may differ once a mental health challenge has been identified. Research has shown that care providers were more inclined to offer medication as the primary way of managing the problem and less likely to encourage psychotherapy, which was the opposite for their native-born counterparts. 17 Because too few health professionals are fluent in multiple languages, it is especially challenging for immigrants to receive proper care for mental health symptoms. 12 Health care providers who lack cultural sensitivity training in addition to limited ethno–racial-focused programs 18 may further challenge immigrants’ uptake of available supports.
Social and Financial Stressors
Separation of the family through strict immigration processes may leave migrants feeling isolated in finding or receiving help. 19 The emotional stress associated with migrating from one country to another can negatively impact one's perceived sustainability after migrating. Bamgbose Pederson et al 20 conducted focus groups with black immigrant women, soliciting their mental health perspectives. Participants reported that the loss of financial security and status after migrating to North America was related to increased feelings of not being welcome in their new country. These challenges further suggest the need for improvements not only in personalized support and services for immigrants, but also societal-level changes in attitudes toward immigrants.
Stigma
Internalized negative stereotypes of visible minorities may also create barriers to understanding and managing mental health and accessing services. Samuel 21 interviewed African-American male adolescents about their mental health experiences. Participants understood their mental health challenges resulting from unequal treatment experiences through racism, prejudice, and discrimination. It is plausible that societal-level experiences of stigma and stereotypes may be internalized, creating distress and feelings of helplessness. Mantovani et al 22 examined the experiences of women of African descent to explore the ways that stigma played a role in mental health service utilization. The findings revealed that this group held particular beliefs about the origin of their symptoms, which led to the underutilization of services and societal-level stigma and resulting in active self-silencing to align with the community's expectations. 22 Research has also shown that, among Asian immigrants, culture played an essential role in their service utilization by associating their illness with supernatural power or by asserting that another individual caused it through “magical means” 23 (p217). Salami et al. 24 interviewed service providers at various immigrant-serving agencies in Alberta to explore their observations of the most influential contributors to immigrants’ mental health service access and utilization. The results revealed internalized stigma related to mental illness, community understandings of mental health, and ambiguity regarding the potential negative implications of maneuvering daily life with a mental illness.
Cultural influences are important sources of socialization, with implications for how people interpret their life experiences. O’Mahony and Donnelly 8 interviewed immigrants from 3 cultural backgrounds. They found that their families often encouraged them to hide their illnesses out of fear of rejection from their cultural community, which exacerbated symptoms when they were ready to go against their family or community and address the problem. Cultural stigma strongly affects whether immigrants believed they should access professional services for their mental health. 12 Even when migrants recognize worsening mental health, cultural views of the issue being a family problem that they should not raise with anyone outside of the family, including friends and care providers, ultimately influence their help-seeking behaviors. 19
Research Aims
Although some empirical attention has been given to help-seeking trends among migrants, gaps remain in our understanding of how one's culture facilitates or impedes help-seeking behavior. This study aimed to understand young adult migrants’ perspectives on mental health and service accessibility and utilization.
We addressed 4 research questions in this study: (1) What are young adult immigrants’ mental health help-seeking experiences? (2) How do young adult migrants interpret the influence of their cultural socialization and upbringing on mental health support-seeking and access? (3) What other social factors influence how migrants seek and access mental health support? (4) What do migrants and support staff recommend to address identified challenges?
Theoretical Framework
Similar to O’Mahony and Donnelly, 8 we used Kleinman's explanatory model 25 from project conceptualization to data analysis and interpretation throughout the study. This model has been used to examine how beliefs based on culture, values, and knowledge explain how an individual interprets, understands, and copes with illness. 25 According to Waite and Killian, 26 this model highlights compromising and bargaining between a person's cultural norms and Western culture's ideas of illness treatment.
Method
Research Design
We conducted a qualitative research study, incorporating an interpretivist framework to explore the perspectives and experiences of our participants. We adhered to Braun and Clarke's27,28 thematic analysis, a six-step qualitative process comprised of data familiarization, development of preliminary codes, initial theme development, review of potential themes, finalization of themes, and development of the report.
Researcher Positionality
The first author is of Jamaican descent, and both of her parents were born and raised in Jamaica. Her parents had migrated to Canada 27 years ago with extended family members at the time of data collection. The first author belongs to the House of God-Seventh Day denomination. The second author is of Filipino, British, and French descent. At the time of data collection, her mother had migrated to Canada from the Philippines over 40 years ago on her own; her father was Canadian-born. The second author is Roman Catholic. The third author is of Persian descent, and both of her parents were born and raised in Iran. She migrated to Canada with her family in 1988 and, at the time of data collection, her parents had passed away. The third author's family practices Zoroastrian religion based on 3 principles: Good Thoughts, Good Words, and Good Deeds.
Setting and Recruitment
We recruited participants at a local, multi-service agency supporting the diverse needs of immigrants and refugees through settlement and integration services. This organization was situated in a region home to a large and growing population of immigrants. The organization provided settlement, counseling, English language training, newcomer childcare, and employment support for anyone who identifies as an immigrant.
We used a convenience sampling method to recruit Canadian immigrants and support staff, who we interviewed about their experiences of the phenomenon of interest. The inclusion criteria for migrant participants were as follows: (a) young adults who had migrated to Canada within the past 10 years, (b) either experienced a decline in their mental wellness within the past year or were interested in sharing their cultural perspectives on mental health, and (c) had basic oral English communication skills. The organization's executive director compiled a list of immigrant clients who met our study inclusion criteria. Our recruitment strategy was focused on migrants in early adulthood because of our empirical interest in understanding the mental health experiences of immigrants in a developmental period where mental health difficulties may be particularly high. The inclusion criteria for support staff participants were that they: (a) were employed at the local newcomer organization for at least 6 months and (b) had basic oral English communication skills.
Our sample of 10 migrant participants was appropriately suited to address our research question. Existing literature suggests no agreement about a minimum number of participants (eg, Levitt et al 29 ). We focused on the appropriateness of our sample size based on how the data allowed us to achieve our study goals. Our migrant sample size permitted us to portray the phenomenon of interest within the qualitative tradition appropriately. We were pleased to have 10 migrant participants dialogue with a Canadian-born researcher who did not share our migrant participants’ disclosed ethnic backgrounds or religious affiliations. Given the history of marginalization of this disadvantaged group, we were grateful for our participants’ involvement.
The first author scheduled 3 research visits to the organization to conduct the individual interviews. On interview days, the first 10 migrants from the list present at the center were verbally informed by the organization staff about the study and subsequently provided with further details by the primary researcher and invited to participate. Support staff participants were informed about the study by an email that was sent out to all staff through email with study recruitment details.
Participants
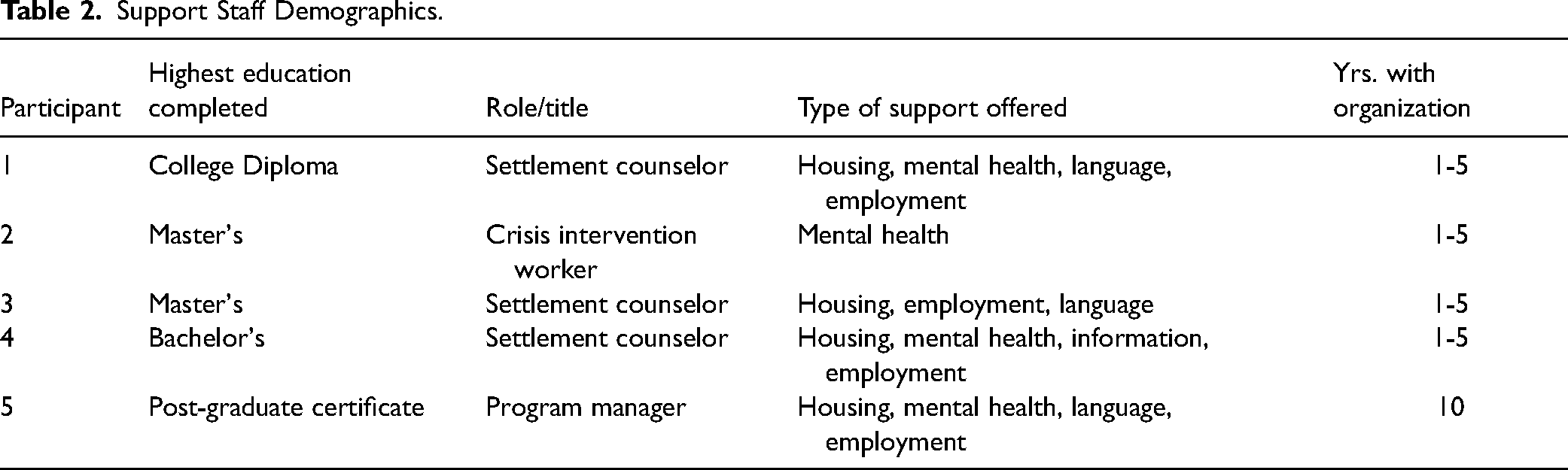
Ten migrants to Canada and 5 support staff participated in the present study. Migrants included young adults between the ages of 18 to 30 years who had migrated to Canada within the past 10 years. Migrant participants reported that they had either been experiencing a decline in their mental well-being within the previous 12 months or were interested in sharing their cultural views on mental health. They were required to have basic oral English communication skills. Migrant participants were members of various racial and ethnic groups, including (but not limited to) Hispanic/Latino, East Asian, and Middle Eastern backgrounds. All migrant participants identified as first-generation immigrants to Canada. See Table 1 for migrant demographic characteristics. Support staff who had worked at the organization for at least 6 months were invited to participate in the focus group. Support staff participants were required to have basic oral English communication skills. Support staff participants had extensive experience working with migrants; they reported working with a significant number of Canadian migrants at the organization (eg, “1000 + ,” “100/month”). See Table 2 for additional support staff demographic characteristics.
Immigrant Demographics.
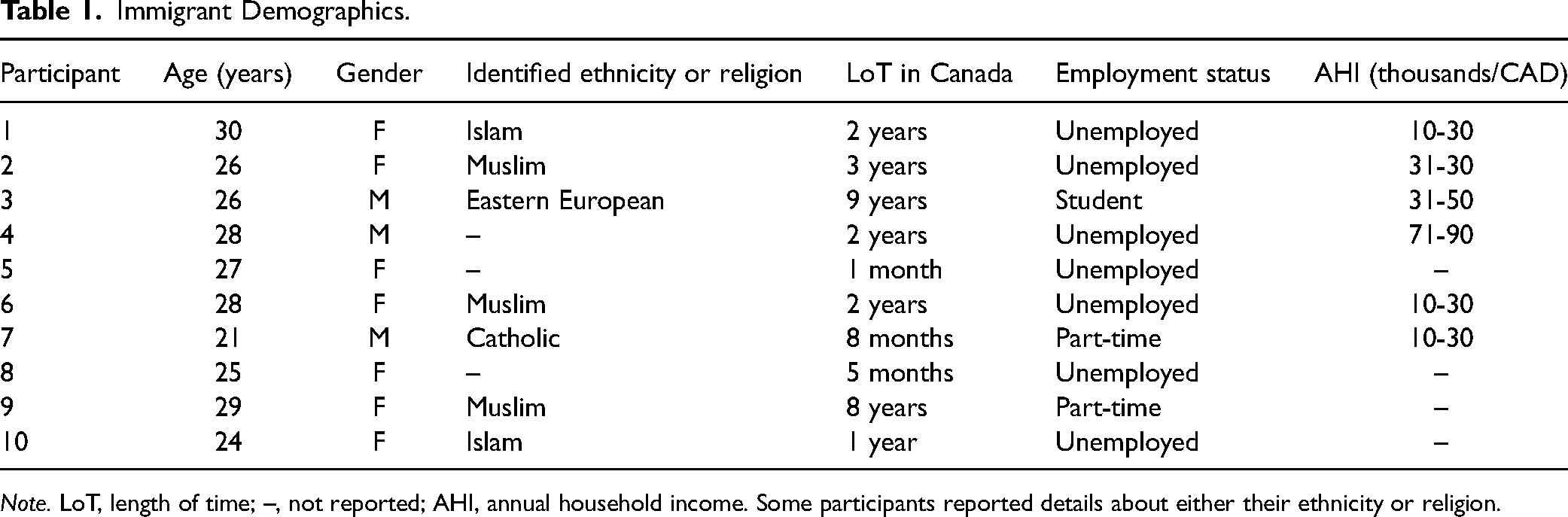
Note. LoT, length of time; –, not reported; AHI, annual household income. Some participants reported details about either their ethnicity or religion.
Support Staff Demographics.
Procedure
We conducted individual interviews and a focus group to explore experiences of cultural and social barriers or facilitators related to mental health concerns and service utilization. The first and second authors developed the interview guides (see Supplemental Material for copies of each guide) and co-facilitated the focus group. The interview guide included a series of open-ended questions to facilitate dialogue directly influenced by questions posed by Salami et al. 24 These questions highlighted mental health experiences and facilitators or obstacles to accessing related supports. 24 Interview questions focused on culture, immigration, displacement, mental health services, and stigma. Participants were encouraged to share what they were comfortable with regarding their culture and how various social factors affected their mental health experiences and concerns.
The first author conducted all one-on-one migrant interviews (no support staff from the organization was present) and the first and second authors co-facilitated the support staff focus group. The migrant interviews were approximately 30 min in length, and the focus group was approximately 60 min in length. All interviews were audio-recorded. The primary researcher listened to each recording and transcribed the narratives into written form. We obtained written consent from all migrant and support staff participants before data collection (see Supplemental Material for copies of the consent forms). We received ethics clearance for this research at Brock University in December 2018 (File # 18-088).
Data Analysis
We used an inductive approach (ie, the researcher relies on data from participants to create broad themes regarding the phenomenon) to understand migrant perspectives.27,28,30 Within this study, the researcher did not derive the themes before collecting data and analyzing each participant's narratives. Using thematic analysis,27,28 we identified patterns within the data.
We developed the themes by following Braun and Clarke's27, 28 thematic analysis steps. The analysis includes (a) data familiarization (ie, reading and re-reading the transcripts), (b) initial code development (ie, noting words or phrases while reviewing the transcripts), (c) examining the data for themes (ie, grouping codes together to develop higher-level categories), (d) reviewing potential themes (ie, reviewing potential themes and ensuring consistency across codes within each theme and subtheme), (e) naming themes (ie, determining appropriate theme titles consistent with the data included within each theme and subtheme), and (f) producing the report (ie, developing the data report substantiated by quotes that highlight various components of the analysis).
We used NVivo 12 software to organize the data while the primary researcher conducted a step-by-step analysis of the narratives expressed by the immigrants and support staff. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Trustworthiness of the Data
We established the methodological rigor of the data.31,32 We used thick descriptions as the narratives of experiences and accounts provided by migrants and support staff reflected the experiences of these populations and their perspectives on the topic. Next, we achieved prolonged engagement with the topic through the collective experiences of the organization's director (third author), primary researcher (first author), and graduate supervisor (second author). The authors’ combined research interests and service experiences with immigrant mental wellness were critical in informing the data analytic process. We achieved theme agreement by having regular discussions throughout the entire analytic process. The first and second authors held weekly meetings during the initial code development and theme development stages of the analyses. Preliminary and final summaries of the themes were shared with the third author, who provided input on the analysis. Finally, we considered the negative case analysis by identifying disparities across the narratives between and across participants throughout the study. Throughout our preliminary analysis, we further explored some of the interviews in which there appeared to be dissonance with what the other participants had described. As we proceeded through the advanced stages of our analysis, we integrated all seemingly contradictory findings into separate subthemes within an overarching theme. It is worth noting that because the organization's executive director (third author) was involved in supporting the recruitment process (ie, compiled a list of immigrant clients who met inclusion criteria, sent support staff an email informing them about the study and recruitment details), this should be considered when interpreting our findings.
Results
Immigrants and support staff described various perspectives and experiences about mental health and service utilization. Both groups described the influence of how cultural experiences shaped their perceptions and interactions with help-seeking supports.
Migrant Themes
Immigrants highlighted how cultural experiences influenced their perceptions of mental health and service utilization. Our analysis of the migrant interviews revealed the following themes: (a) perspectives of mental health and factors that negatively affect it (research question 1), (b) when to seek professional help, if at all (research question 2), and (c) expectations and experiences of help-seeking (research questions 2, 3, and 4).
Perspectives of Mental Health and Stressors That Negatively Affect It
Immigrants held various culturally rooted beliefs regarding mental health challenges. They also described external influences on mental health, including living in war-torn countries and assimilating to a new country.
Culturally Informed Understandings of Mental Health
Migrants described their perceptions of mental health. Some migrants expressed that those with mental health challenges were born “psycho” or “crazy” (immigrants 1 and 2) and were “cursed.” Immigrant 2 described the segregation of people experiencing mental health challenges. He stated, “… you are sick and uh like [others] don’t accept you in that group. They don’t want you to be with them because … you have this problem” (Migrant 2). Immigrants mentioned that mental health challenges were hidden from nonfamily members. For example, Immigrant 3 stated, “Uh like you can keep [it] in your family only, not outside …” Immigrant 8 described her family's negative perceptions of mental health when she expressed her decision to pursue a psychology degree. She explained: “Like when I decided to study psychology, all of my family like even my family said, ‘So you want to study crazy people? You want to go to the hospital to see those, those crazy people?’” (Immigrant 8). Interestingly, Immigrant 8's family expected that she would “be like them” if she worked with people who had mental health challenges.
External Stressors on Mental Health
Migrants described influential external factors that negatively affected their mental health. For example, participants described the experience of war. Immigrant 10 discussed the distress resulting from living in a war-stricken country, saying, “You have a lot of war … and that is our culture … There's a lot of wars and bomb blasts so every day we are scared on how to go.” Immigrant 10's description of the imminent fears associated with living in a war-torn country was their focus relative to mental health.
When leaving their home countries, most immigrants expressed the difficulties associated with moving to a new country and attempting to assimilate into their new cultural surroundings. Immigrant 2 acknowledged these hardships and their impacts on mental health: “Because of the war, we move to Turkey. I live there to for two years and then I move to Canada because I wanted like [a] safe place for my kid, my child, but I became depressed and alone.” Immigrant 2 moved to Canada with her child to live in a “safe place”; however, she experienced isolation and depression as a result.
When to Seek Professional Help, If At All
Immigrants described difficulties regarding the decisions to seek intervention for mental health challenges. Some participants minimized the severity of mental health difficulties, and others suggested that clinical intervention was only necessary for extreme situations. Some participants suggested intervention was never warranted.
Minimizing the Potential Seriousness of Symptoms
Immigrants articulated that mental health challenges and associated symptoms were temporary and that they would “grow out of it” (Immigrants 3, 5, and 6). Participants reported that anxiety and depression symptoms did not require clinical intervention. Immigrant 4 stated: I was worried little bit and maybe [my depression] last for one month maybe … And I rather to deal with it myself because I didn’t see—I knew that was going to pass. The period, the period will pass, and I will feel relief and I didn’t find I need to go to doctor or something.
Some participants expressed that addressing anxious or sad feelings was minimized compared to their reality of having lived in a war-torn country where they prioritized the safety of their loved ones. Participants paid relatively little attention to mental health until it limited their ability to work or their family responsibilities. One migrant participant spoke of the cultural taboo surrounding mental health in his community and expressed his perspectives on normalizing poor mental health in terms of stress: “You have stress, everybody has the stress, it's okay. Take multivitamins, melatonin, you will be okay don’t worry …” (Immigrant 7).
Intervention is Only for Severe Mental Health Challenges
Immigrants expressed that people should only access clinical mental health interventions if their mental health poses a “big problem” (Immigrants 5, 6, and 9). Strategies to manage “big problems” included meditation and finding a personal outlet, such as a hobby. All immigrants described the importance of knowing when a mental health challenge became “big.” Immigrant 5 mentioned, … if I will have kinda like big problems like big depression ya sure I will go but if I just have little bit anxiety or like if I’m sad I just like can handle by myself like try to meditate, think positive [or] read something.
However, when probed further, participants did not elaborate on the distinction between a “big problem” and less serious issues.
Immigrant 6 commented on the differences between service utilization in their country of origin compared to Canada: In my country, goes to severe problems and then we go to the doctor but in here, if you face small problems or small stress, we can go to the doctor, but in there, not like that. If we have severe problem about mental health, we can get medicine free in here.
Professional Intervention for Mental Health Challenges is Unnecessary
When immigrants referred to mental health challenges as “small problems” (Immigrants 6 and 9), they described only discussing mental health with family and close friends. Immigrant 7 commented on how mental health difficulties are kept secret within the family unit, stating, They don’t accept it like even [if] I want to [go to] the counselor, like my family, they don’t tell my relatives. For my neighbors, they don’t talk like they keep it like a secret, like they don’t tell on us that you made it to the doctors, or you have a problem, like they don’t talk about this.
Immigrant 6 described a family who hid their daughter with depression from others and did not take her to mental health professionals for treatment: “… they have one daughter, and I think she has depression, and they didn’t take her to the counselor or the doctor. They just stay in the home, give her medicine, and don’t talk about her, like they don’t show us to her.” Some participants explained that they received support from their family and friends during times when they experienced a decline in their mental health. Immigrant 2 commented on an experience stating, “I have friends here, of course, they help me, and sometimes I call my mother. She helps me a lot and my sisters also are helping me, so I know how to manage that time.”
Immigrants managed their mental health issues without intervention because of fears regarding the stigma of mental health challenges and accessing support. Participants mentioned the negative connotations of mental health challenges and accessing support for these experiences. For example, Immigrant 6 said, “If they can uh like open talk about it, it's like a stigma on them, on their reputation or something like that it's like kinda you weak, like weaknesses …”
Instead, participants described strategies such as distracting themselves with hobbies and praying to God to rid themselves of these symptoms. Participants discussed alternative interventions to alleviate mental health challenges rather than seeking clinical intervention. Non-medical interventions were common in narratives among Muslim participants in our sample. For example, Immigrant 2, who was Muslim, stated: … you have to pray, and we say like make wishes to manage uh the time. Yes, like that … my religion as Muslim you have … like … If you are feeling depression and then you have to do uh like to believe that God and pray. Like have to pray and make wishes and he can be treated, and God will treat you.
Expectations and Experiences of Help-Seeking
Immigrants referred to their initial help-seeking expectations in Canada before and after arriving. They also described their experiences accessing available supports.
Perceptions of the Canadian Mental Health Care System
Immigrants discussed general positive perspectives of Canada's mental health care system. They articulated that people in Canada cared about residents more than professionals in their country of origin based on their perceptions from the media (eg, television). One participant attributed the affordability of services in Canada compared to their country of origin to the government and professionals caring more about citizens and their health: So out here they more care about people, they more care about your health and they don’t really care about money here. It's very different because you get more services here than back home… Actually, Canada, they care about those stuff, mental health and I would say they more care about people like this out here than back home. (Immigrant 3)
Regarding the differences between Canada and other countries, some immigrants also stated that services were easy to find in Canada compared to their country of origin. Specifically, they discussed the accessibility of resources through other supports and the media within Canada. Immigrant 6 stated, “I can just walk into a walk-in clinic and ask for information or some other places that I can ask for information that are there for those services, so I think it's pretty easy here. … They care about that stuff out here.”
While mental health services were considered available, immigrants commented on the financial costs of accessing supports. Immigrant 3 said, “Because can you imagine it for the people who do not really have money, [mental health services are a] lot of money for them so sometimes they have to do extra stuff to get the money.” Immigrant 3 went on to suggest that “The government should help.”
Through various media outlets (eg, television and radio), participants believed that diagnosis was common in Canada, professionals were more accepting of mental health issues, and people were encouraged to access services once they experienced mental health challenges. One migrant compared his perception of the prevalence of Canadians with mental health difficulties compared to Ukrainians with similar challenges: “What I noticed in Canada, it's much more people with mental illness, officially mental issues than in Ukraine. I don’t know what the consequences are or what's the connection between this but that's what it is” (Immigrant 4).
Experiences Accessing Services
Participants described both positive and negative experiences with service access. Participants expressed their satisfaction with their support from people in their social networks. Few immigrants felt supported by their families when expressing their desire to seek intervention in Canada.
Immigrant 10 spoke about his mother, saying that she “always support me. She would say if I want, then go and if you feel really bad. I don’t have a lot of friends and you feel very bad, go to doctor. So, I would go to the doctor.”
Most participants described positive experiences with Canadian healthcare providers after migrating to Canada. Immigrants believed that professionals addressed their concerns wholly and appropriately. For example, Immigrant 9 had a chronic illness and discussed her experiences meeting with various doctors and specialists to receive the necessary support. She stated: I just go to the doctor and I ask him because I already take the medication, so they just wrote me a prescription. After that, I have seizure recently uh so he told me that you should go to the specialist and we will decide whatever he will do for you. That's it. (Immigrant 9)
Participants also described language difficulties as a barrier to service access. Immigrant 8 described her initial unfamiliarity with mental health services when she arrived in Canada. She suggested that immigrants who are less fluent in English may have more difficulties finding out about appropriate supports: Yeah, maybe I tell people about these services because many people they don’t know. Like me at the beginning, when I came many services here, I don’t know about it. Just sometimes by accident I know or some of my friends they told me about it but it's easier maybe for me because my language is better than others but it's very hard or difficult or maybe some people, they will never know about it because they don’t have the language.
Relatedly, Immigrant 7 articulated that she would be more likely to access services with a professional who speaks her native language: “If I know that there's someone who speaks Arabic and can help me, I will see more.”
Support Staff Themes
Support staff described their experiences supporting migrant clients with their mental health needs. Our analysis revealed 2 themes: (a) immigration status, financial constraints, and mental health (research questions 3 and 4) and (b) immigrant attitudes toward mental health and service utilization (research question 3).
Immigration Status, Financial Constraints, and Mental Health
Support staff described immigrants’ anxieties while waiting to hear news from the government regarding permanent residency or citizenship. They stated that government assistance was inadequate, leaving immigrants with relatively little money to afford mental health supports if required.
Stress Associated With Undocumented Status
Support staff described their newcomer clients’ feelings of anxiousness, worry, and fear regarding whether they would become permanent residents and, if so, when it would happen. Support staff recalled meetings in which immigrants directly linked undocumented status and mental health. For example, Support Staff 2 said: Some of them are still waiting for the papers. Even if they are not refugees, other refugees, like refugees in protection, are still waiting for the PR [permanent residency] so a lot of people are waiting, making them anxious about it no matter how you speak to them. Immigration status also plays a role in the type of services they can access. So that is actually important because those programs out there are for everyone but actually just for selected people.
Other support staff agreed that having documented status provided immigrants with opportunities for settlement into Canadian society by accessing supports, such as reduced academic tuition rates and increased government-funded services.
Restricted Finances
When asked about pressures affecting mental health challenges, support staff recognized that some immigrants were eligible for financial assistance from limited sources through Canadian government assistance programs. A discussion around the consequences of the negative intersection of economic status, waitlists, and service efficiency began with Support Staff 2 stating: We refer them to services, but do they help them? … [Migrants] cannot wait for six years to get good service so, very limited services and it is creating tension on the family who are newcomers, very small houses, no support, no family support. I believe that mental health is an issue but what is really affecting them is loss of the day. It's holistic.
Financial assistance covered necessities and left little additional money for other needs. Support staff suggested that troublesome financial discussions and uncertainty of residency status were significant concerns for immigrants and impacted mental health. Other support staff indicated that immigrants could not pay out-of-pocket for services and supports, which may negatively affect their mental health and the mental health of their families. For example, one support staff said, “They can only get money from [government program], which does not cover expenses, and on top of that, they are waiting, which affects their mental health and their children's mental health” (Support Staff 5). Support Staff 4 also discussed the impact of financial constraints on mental health: I want to talk about the other end. The service provider. I think the hardest barrier is in a financial piece … not all health services are provided for free so even though I put my kids’ wants first and foremost, the resources are limited. They need to be referred and also the prices are so high … so how do you imagine an immigrant family can afford that? They try so hard, but they can’t.
Support Staff 4 went on to describe the cost of services, saying, “One session for CBT [cognitive behavioral therapy] is $200–500 so how do you imagine an immigrant family can afford that?” Support staff described the need for increased government-funded supports for this population to aid in the settlement process.
Migrant Attitudes Toward Mental Health and Service Utilization
Support staff expressed tension between immigrants’ openness with mental health challenges and acknowledging their existence. Participants discussed the stigma immigrants experienced from within their cultural communities. Finally, they described the difficulties communicating with service providers due to language barriers and the inaccessibility of interpretation supports.
Perceptions of Mental Health
Support staff shared their perceptions of immigrants’ cultural beliefs about mental health. They described migrant narratives that mental health challenges were fictional and did not require the person to access support. When support staff were asked why immigrants believed that mental health was not real, one support staff replied, “They may not believe it or supported, or it may conflict with their cultural beliefs and what a parent's role is and their support may not be like they are back home for them” (Support Staff 5). Support staff also stated that many cultures do not have a term for mental health, which made the topic more difficult to explain to clients. Support Staff 4 also stated that help-seeking words may have a negative connotation: “Well, I think that even in some cultures and languages, there isn’t a word for mental health and there isn’t a word to translate it to them even. Talking about support in Arabic may be a negative thing.”
Intra-Cultural Stigmatization
Support staff acknowledged immigrants’ feelings of wanting to access mental health supports but being fearful of what others in their cultural networks would think and how they would be treated. One support staff explained their experiences hearing about culture and stigmatization by saying: … we are all human beings and there are some common ways that [people] react and deal with mental health. We see resistance from certain cultural backgrounds, not really specific to certain cultures but it's basically really common there. More like people based on their own stigma and cultural practice and also fear because mental health definitely means different things for different people. (Support Staff 5)
Participants also discussed the role of religion on attitudes toward service access. Support Staff 4 reflected on an experience with mainly Arabic clients, stating: I also think because I work with mostly Arabs, the religion plays a role in the mental health. You know many of them have commitment to something and they have a tool in which they use to overcome mental health issues and things like that. Many times, for them it can be stigma or if you can focus on religion [thus] resulting in the issues that they have.
Interpretation Services and Cultural Understanding
Support staff explained barriers and facilitators that impacted immigrants’ abilities to access services necessary to promote mental health. Participants described language and cultural barriers. They explained that many mental health professionals often did not speak the same language as immigrants, and immigrants did not have the money to pay for a translator. For example, Support Staff 5 shared an experience of a migrant accessing supports in Canada: There are no interpretation services. [The professionals] keep telling [the immigrants] to bring somebody, but we cannot bring somebody, you have to provide them, and I have to fight for them. Many of my clients do things without knowing what it is. They went into the surgery and because they were embarrassed to say they don’t understand, they just did it.
Support staff noted that feeling comfortable to share experiences in a judgment-free environment facilitated mental health service utilization among their clients. Support staff stated that understanding the client's needs and referring them to an appropriate service was easier when they shared similar cultural backgrounds. A few of the support staff agreed that sharing culture enhanced the services they could provide to immigrants. Alternatively, there were also positive experiences from native-born Canadians who did not share cultural backgrounds, providing a different perspective. Support staff 2 stated, “So, in my experience, I was born and raised in Canada and a lot of my clients have voiced that they like that because they can speak to me about issues that are stigmatized within their own culture …”
Immigrant and Support Staff Recommendations
Participants described various interwoven recommendations for addressing some of the challenges associated with improving mental health help-seeking and increasing support uptake (research question 4). Participants focused on service accessibility, commenting on the lack of bilingual healthcare professionals. Migrants and support staff also described challenges with the affordability of available services and supports. Participants from both groups recommended that more government-funded support be increased for this population to help improve the settlement process.
Discussion
Migrant and support staff participants in our sample described various perspectives regarding mental health, help-seeking behaviors, and available supports. Both groups described challenges related to perceptions of poor mental health and if and when to seek professional support. Support staff uniquely explained issues on immigration status that our migrant participants did not describe. Perhaps expectedly, support staff in our sample described their experiences from a help-seeking standpoint, which differed from the vantage point of migrants coming to Canada and their perspectives about mental health and Canadian supports.
Migrants
Immigrants discussed their cultural beliefs regarding the origins of mental health challenges. According to Kleinman's 33 model, people from different cultures have various views regarding the reason for their symptoms, which impact their course of action. Research has shown that one's culture and socioeconomic status may influence a person's decisions about accessing mental health services.7,12 Some immigrants in our sample believed that mental health difficulties were the result of a curse or were chosen by God. These findings closely align with Fung and Wong, 23 (p217) who found that mental health challenges were associated with “magical means” from a spirit-type individual. As several immigrants considered themselves refugees escaping war-ridden countries, some participants understandably prioritized physical safety over mental wellness. Therefore, our findings suggest that additional attention to mental health among immigrants fleeing war-torn countries is critical in newcomer settlement services.
Immigrants in our sample had difficulties expressing whether mental health challenges in fact existed, as well as whether and how to determine when seeking intervention was appropriate. Some participants challenged the legitimacy of mental health challenges. Participants deemphasized mental health challenges, referring to them as temporary and minor. Findings from our sample contrast with research highlighting the increased prevalence of mental health challenges in newcomer groups, especially depression, and anxiety.7,8 Unfortunately, undiagnosed or mistreated symptoms may facilitate experiences of chronic, worsening conditions. Perhaps Newbold and Simone's 16 (p53) findings whereby immigrants were more likely to report good health and ignore their chronic conditions when migrating to their new country (ie, “healthy immigrant effect”) came through in our newcomer participants’ narratives.
Regarding disclosing mental health difficulties, immigrants in the present study stated that these challenges should only be discussed with immediate family members. According to Kleinman's model, 25 the decision to seek medical intervention depends on the person's social community, past experiences of illness, and cultural belief system. These findings were consistent with qualitative studies by O’Mahony et al 12 and Yorke et al, 19 who found that a fear of experiencing intra-group stigma deterred immigrants from accessing support. Immigrants likely require a safe environment to establish trust and openly share their experiences.
Expectations and experiences of help-seeking in Canada were also important themes. Immigrants in our sample believed that Canadian organizations provided greater support to people and that professionals addressed issues holistically compared to their home countries. Comparatively, immigrants faced financial insecurity and other circumstances that disproved these beliefs. This finding is consistent with Miranda and colleagues, 34 who highlighted the experiences of black women and found that the inaccessibility of support related to increased mental health challenges, unemployment, and uninsured statuses. In the present study, participants described positive experiences with Canadian healthcare providers once they had migrated to Canada. These findings contrast with research indicating that immigrants felt that they did not receive quality care and adequate attention for their mental health challenges. 12 Immigrants also discussed being offered prescription medications over psychotherapy, opposite from their native-born counterparts. 16 These findings are consistent with McSweeney's 35 application of Kleinman's explanatory model, 25 which found that each person interpreted illness uniquely depending on their environment, past experiences, and ethnicity or culture.
Support Staff
Although our focus group was relatively small, support staff discussed various factors that contributed to immigrants’ mental health challenges. They described a connection between immigrants’ stress, anxiety, undocumented citizen status, and limited available finances. These findings were consistent with Kim et al, 14 who investigated the influence of culture on stressors for immigrant children and noted that these youth were at an increased risk of developing anxious feelings compared to fully documented families.
Support staff indicated that immigrants were conflicted about acknowledging mental health challenges and experiencing stigmatization from their cultural communities. Support staff suggested that people from certain cultures might not believe that mental health concerns exist, and if they accept this Western ideology, they are stigmatized.8,36 Support staff participants discussed that stigma is one of the greatest barriers to the help-seeking behaviors of immigrants they support. Salami et al 24 found that cultural understandings of mental health may create impediments to immigrants’ symptom acceptance. This information appears to be a critical first step in supporting this population: supporting immigrants by providing them with mental health education and teaching them how to identify when they are experiencing mental health challenges to begin an important dialogue.
Immigrant and Support Staff Recommendations
Participants had several recommendations to improve mental health service access among immigrants. Newcomer mental health services with bilingual staff may create an opportunity for immigrants to be comfortable expressing potentially difficult and personal topics. This may be especially important given the intra-cultural stigma toward mental health among various cultures. Finally, participants recommended additional government funding to appropriately serve and support the mental health of immigrants to Canada.
Limitations
There were several limitations to this study. Immigrants and support staff were invited to participate if they were available on the researcher's scheduled interview days. As such, we likely missed important participant voices. Authentic community engagement is critical in research with disenfranchised communities, including migrants to Canada. The organization's executive director's involvement in our participant recruitment strategy is also worth noting. We consider the executive director's passion for research on settlement issues and its impact on policy changes as a major strength of our study and demonstration of research relationship trust building. At the same time, it may be worth considering her involvement in our recruitment process (ie, support with study advertising) when interpreting our findings.
Additionally, participants represented multiple cultures and religious orientations in the present study. Relatedly, not all migrant participants disclosed their cultural or religious orientations, making the connections between cultural conceptions of mental health and service access even more tentative. Based on the available demographic data, our sample was comprised of culturally diverse participants. Understanding the connection between mental health beliefs and behaviors and specific cultural or religious orientations remains essential for future research. Our findings shed light on potential individual differences in mental health perceptions, including the influence of culture and other integrated factors (eg, age, upbringing, mental health experiences, and family perceptions about mental health and wellness). Future research might focus specifically on selected cultures, which may provide deeper insight into the unique experiences of immigrants from specific cultural orientations.
While we did not collect discrete mental health condition data from migrant participants, this information would have provided further contextual information about the participants in the present study. Descriptively, we could have further clarified our question about migrant participants’ ethnicity. In our demographic survey, we asked participants to indicate their ethnicity as an open-ended question. Some participants described their ethnic backgrounds, whereas others included their religion.
Support staff participants described stresses associated with undocumented immigration status. Although we did not collect immigration status as part of our demographic survey, this information may have provided further insight into migrant participants’ mental wellness at the time of the study. Future researchers might consider examining the influence of immigration status on immigrants’ experiences of mental health.
We excluded participants with limited oral English skills. Perhaps providing participants with the option of submitting oral or written answers in their native language to be later translated and transcribed for analysis may have offered additional immigrants an opportunity to express their narratives. The researchers were female and did not belong to the cultural or religious groups represented in the study. Different cultural and religious orientations may have influenced how participants shared their stories.
Conclusion
This study adds to previous research on migrants’ experiences of mental health and service access. Through this study, immigrants and support staff revealed that culture and other social factors facilitate and hinder help-seeking behavior and mental health service utilization. Participants provided thoughtful insights into the challenges associated with relocating to Canada in addition to recommendations to improve service access upon newcomer arrival. Future research with additional participants is needed to explore innovative ways to best support the unique needs of this underserved population. Findings from this relatively small convenience sample may be used to inform the future delivery of effective and holistic care to immigrants to Canada and their families.
Supplemental Material
sj-docx-1-joh-10.1177_27551938231156032 - Supplemental material for Understanding the Mental Health Perspectives and Experiences of Migrants to Canada
Supplemental material, sj-docx-1-joh-10.1177_27551938231156032 for Understanding the Mental Health Perspectives and Experiences of Migrants to Canada by Brittany Davy, Priscilla Burnham Riosa and Effat Ghassemi in International Journal of Social Determinants of Health and Health Services
Footnotes
Authors’ Note
Brittany Davy conducted this research as a graduate student in the Department of Applied Disability Studies. Brittany is currently a PhD candidate in Health and Society at McMaster University, Ontario, Canada. Priscilla Burnham Riosa is an associate professor in the Department of Applied Disability Studies at Brock University, Ontario, Canada. Effat Ghassemi is the Executive Director at the Newcomer Centre of Peel, Ontario, Canada.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.