
Abstract
Introduction:
Globally, between the ages of 10 and 19, 15% of teenagers have mental health issues, according to the World Health Organization (WHO). Mental health issues in schools lead to dropouts, poor academic performance, social isolation, and increased substance misuse. Various strategies, including universal screening and raising mental health literacy, have been implemented. However, constraints like limited resources and inadequate training hinder effective management. Therefore, this paper aimed to explore student access to and utilisation of the school health system for mental health challenges, and to identify key barriers to its effectiveness from the perspective of students and staff in Mapanzure Masvingo District.
Methods:
A mixed-method survey was used with interviews and questionnaires to gather information from key informants and 62 randomly selected students. The key informants were purposively sampled, including two nurses, two teachers, three health masters, and two administrators. Quantitative data was analysed in Excel and SPSS and presented as tables and graphs, while the qualitative data was recorded, transcribed verbatim, coded, and thematically analysed.
Results:
The study found a high prevalence of self-reported mental health symptoms among students, including attention deficit (62.9%) and low self-esteem (72.6%). This high burden of need contrasted sharply with utilisation of the school health system was low (40.3%), primarily due to a lack of student awareness. This indicates a significant gap between system provision and student access. Key informants identified health clubs and guidance counselling as core components of the system, but their effectiveness was hampered by major barriers like poverty and substance abuse.
Conclusion:
It can be concluded that students are experiencing mental health issues, and key informants generally view school health systems as helpful. However, there are certain obstacles, such as poverty and substance use and abuse hindering implementation and optimal functioning of school health systems. These results may help create a supportive and inclusive environment that values student health and emotional wellbeing that can lead to improved academic outcomes and positive life for students.
Introduction
The global prevalence of mental health challenges among children and adolescents has become a significant concern, with the World Health Organization (WHO) estimating that up to 20% of this population is affected. 1 Recent studies have highlighted the increasing role of schools as crucial locations for early intervention in addressing these mental health issues. 2 The implementation of comprehensive school health programs to support students’ physical, mental, and social welfare is considered essential in managing mental health challenges in this demographic.
Globally, the most prevalent mental health issues among students include eating disorders, anxiety, depression, and substance abuse. 3 These challenges have far-reaching consequences, including academic difficulties, increased risk of substance addiction, social isolation, and physical health problems. 4 In response, various prevention and management strategies have been developed, such as implementing school health systems, universal screening for mental health issues, and promoting mental health literacy among students, teachers, and parents. 5
Several countries have implemented successful intervention programs. For instance, Canada’s Resilience Project aims to prevent mental health problems in adolescents, while the Friends for Life program, based on cognitive-behavioural therapy, has been implemented in Canada, China, South Africa, and the United Kingdom. 6 Finland’s well-being program, addressing children’s social, emotional, and physical needs, and New Zealand’s positive behaviour for learning program, provide further examples of effective school-based interventions.7,8
In Africa, adolescents face several mental health challenges, primarily depression, anxiety, and trauma. 9 These issues can lead to school dropout, lower academic performance, social isolation, and increased risk of substance abuse. 10 Poverty, violence, and poor access to mental health services are identified as primary contributing factors. 11 Various strategies have been employed to address these challenges in Africa. Telehealth interventions have shown promise in enhancing mental health outcomes. 12 School-based programs such as the U-Rise program in South Africa and the Friends for Life program in Mozambique focus on improving the emotional well-being and life skills of adolescents. 13 In Malawi, the introduction of a policy on mental health and psychosocial support in schools has led to increased teacher training and improved mental health support for students. 14
In Zimbabwe, the 2019 Multiple Indicator Survey revealed that one in five adolescents reported experiencing symptoms of anxiety, while one in ten reported signs of depression. 15 A subsequent report by UNICEF indicated that among adolescents aged 15 to 17 years, 2% suffered from depression and 3% from anxiety. 16 These mental health challenges have significant consequences, including poor academic performance, social isolation, and increased risk of substance abuse and suicide.17,18
The Zimbabwean government has introduced the National School Health Policy to provide a framework for integrated health services within the education system, recognising it as a strategic investment to enhance both health and educational outcomes. 19 This policy mandates the implementation of a coordinated school health program, which includes core components such as: (1) health education integrated into the curriculum; (2) guidance and counselling services; (3) physical education and co-curricular activities; (4) establishing health clubs; and (5) creating partnerships with local health facilities for support and referral. 19
However, the implementation and effectiveness of this policy in real-world, resource-constrained settings like rural Zimbabwe remain poorly understood. Available literature suggests significant challenges. For instance, studies indicate that even teachers designated as guidance and counselling officers often lack adequate training, leading to a poor understanding of mental health issues and difficulty in identifying and referring students in need. 20 Furthermore, systemic barriers such as inadequate funding, overcrowded classrooms, and competing academic priorities often sideline health programs, reducing them to peripheral activities rather than core functions. 21 There is a critical gap in understanding the on-the-ground operation, student engagement with, and constraints facing school health systems in managing mental health disorders, particularly in the Zimbabwean context. Therefore, this paper aimed to explore (1) the mental health challenges and help-seeking needs of students, (2) the utilisation of and access to the existing school health system, and (3) the perceived barriers and potential strategies for improving the system at Mapanzure High School in Masvingo District.
Methodology
Study Area
The study was conducted in Mapanzure, a rural secondary school located 56 km from Masvingo town in the Masvingo district of Zimbabwe. The area comprises of a single rural health clinic. According to 2023 enrolment statistics, the school had a total population of 642 students. A map of the study area is shown in Figure 1.
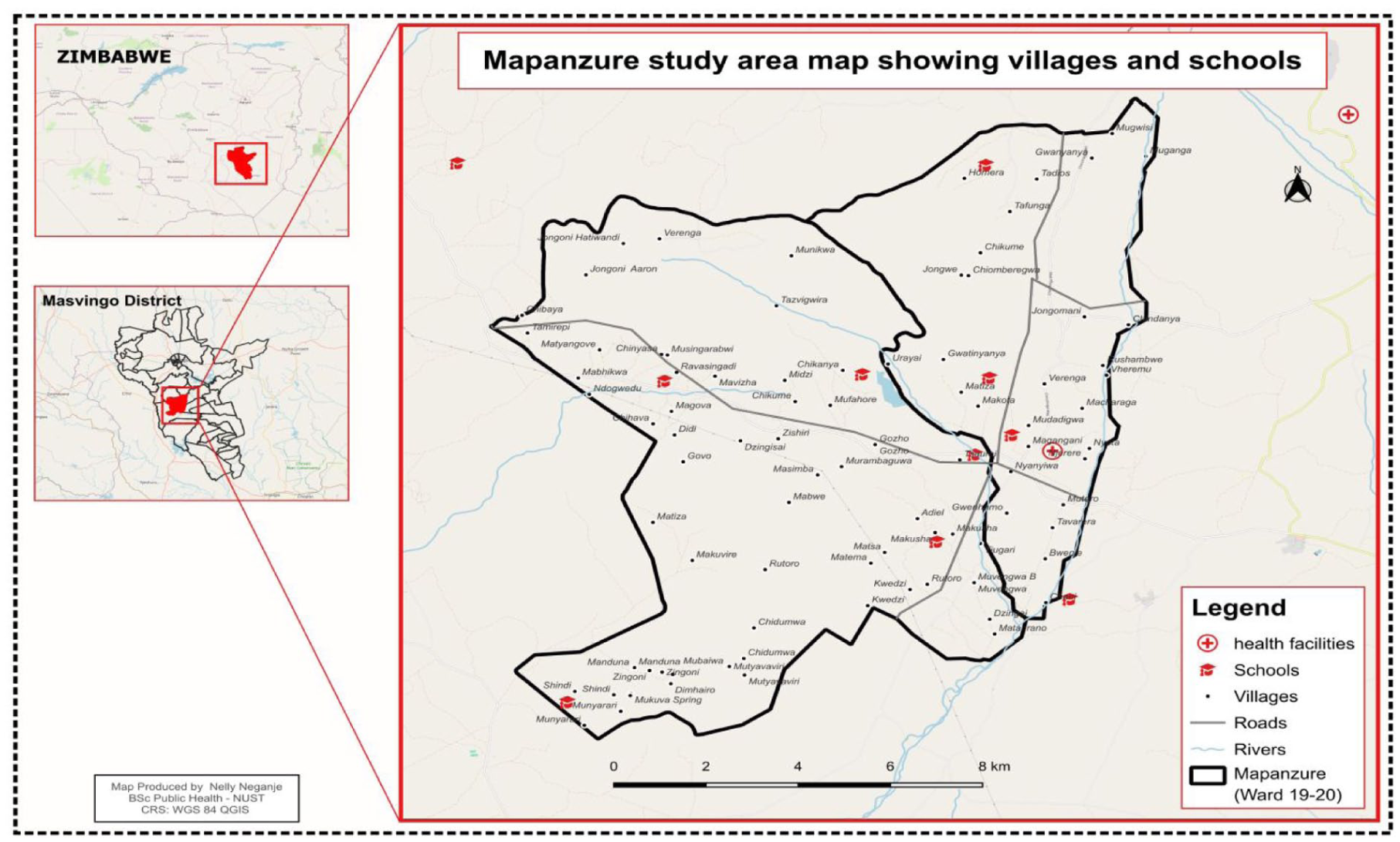
Study area map.
Study Design
This study employed a mixed-methods approach to generate both quantitative and qualitative data, allowing for a comprehensive examination of mental health challenges and school health systems in Mapanzure, Zimbabwe. The research design was carefully structured to address the multifaceted nature of the research questions and to provide a nuanced understanding of the subject matter.
Target Population and Sampling
The primary target population for the quantitative component consisted of all 642 students enrolled at Mapanzure High School. This population was selected due to their direct experience with potential mental health challenges and their engagement with school health systems. For the qualitative component, the target population included key stakeholders in the school health system: three teachers, two nurses, two school health masters, and two school administrators. These participants were all staff members of Mapanzure High School. These participants were chosen based on their professional expertise and close interaction with students, providing valuable insights into the functioning of school health systems and the mental health challenges faced by students.
For the quantitative component, a stratified random sampling technique was employed to ensure representation across different grade levels. Students from Forms 1 to 3 (equivalent to grades 8-10) were sampled separately from those in Forms 4 to 6 (equivalent to grades 11-13) to achieve equal representation. The sampling process involved a color-coded system, with separate selection pools for male and female students to ensure gender balance. The final sample size was 62 students, determined using a margin of error of 10%, a confidence level of 90%, and a response distribution of 50%, given the total population of 642 students. Furthermore, purposive sampling was utilised to select participants for interviews based on their potential to provide rich, relevant data. This non-probability sampling method was chosen to ensure that the most knowledgeable and experienced individuals were included in the study, thus maximising the quality and depth of the qualitative data collected.
Inclusion and Exclusion Criteria
The study applied specific inclusion and exclusion criteria to ensure the selection of appropriate participants. For the quantitative component, students were included if they were currently enrolled at Mapanzure High School, aged 12 to 20 years, and willing to provide assent (with parental consent for minors). Students with severe cognitive impairments or language barriers preventing comprehension of the questionnaire were excluded. For the qualitative component, key stakeholders (teachers, nurses, school health masters, and administrators) were included based on their direct involvement in student welfare and school health systems, while those with less than 1 year of experience in their roles were excluded to ensure informed perspectives. These criteria helped maintain the relevance and reliability of the collected data.
Data Collection Procedures and Tools
Quantitative data was collected using a structured questionnaire administered through KoboCollect software. The questionnaire was designed to capture socio-demographic information (age, sex, education level, and religion) as well as specific mental health indicators, perceptions of school health program effectiveness, and suggestions for improvement.
The mental health screening section was adapted from standardised modules used in adolescent health surveys, drawing on items from the WHO’s Global School-Based Student Health Survey (GSHS) and the Shona Symptom Questionnaire (SSQ) to ensure cultural relevance and contextual appropriateness for Zimbabwean adolescents. 15 This approach allowed for the assessment of symptom clusters associated with common mental health challenges without conducting clinical diagnoses. The questionnaire was pre-tested with a small group of students (n = 5) not included in the final sample to check for clarity, comprehension, and relevance. Internal consistency for the piloted mental health modules was calculated using Cronbach’s Alpha, yielding a score of .79, which indicates acceptable reliability for a screening tool. Adjustments were made to wording and question structure based on this pilot feedback. The questionnaire was designed to capture students’ self-reported experiences and perceptions; it was not used as a clinical diagnostic tool for mental health conditions. Symptom scores were calculated for depression, anxiety, attention deficit, mood disorders, and self-esteem, with predetermined cut-off scores established based on a review of similar screening approaches in the literature (Table 1).
Determining and Characterising Mental Health Challenges.

Qualitative data was gathered through in-depth, semi-structured interviews with the selected stakeholders to gather data on their perspectives regarding the implementation of school health systems, observed mental health challenges among students, and barriers to effective service delivery. The interview guide was piloted and refined to ensure clarity and relevance of questions. Interviews were conducted face-to-face to allow for observation of non-verbal cues and to establish rapport with participants. Data saturation was achieved through the use of an appropriate sample size and the selection of information-rich participants. These interviews were audio-recorded with participant consent and later transcribed for analysis.
Data Management and Analysis
Quantitative data was analysed using descriptive and inferential statistical methods. Scores for various mental health indicators (depression, anxiety, attention deficit, mood disorders, and self-esteem) were calculated based on participants’ responses. The analysis of mental health indicators served to establish the prevalence and burden of need within the student population. The predetermined cut-off scores for each challenge (detailed in Table 1) were established based on a review of similar screening approaches in the literature. 22 A challenge was considered “present” if a participant’s score met or exceeded this threshold. This method of using a symptom count threshold is a common screening approach to identify individuals at high risk who may require further assessment. The tool captured current self-reported experiences and did not account for students who might be on treatment, as the study aimed to assess the current burden of symptomatic experiences within the student population at the time of the survey Chi-square tests and cross-tabulations were performed to examine relationships between variables, such as self-esteem and attention deficit. Results were presented using tables, graphs, and pie charts to effectively communicate findings.
Additionally, qualitative data was analysed using a systematic thematic analysis approach. Thematic analysis followed the six-phase approach by Braun and Clarke (2006) 23 After transcription, two researchers independently familiarised themselves with the data and generated initial codes. Codes were then collated into potential themes, which were reviewed and refined iteratively to ensure they formed a coherent pattern. To enhance validity, emerging themes were discussed with the research team (peer debriefing) and a summary of findings was shared with two key informants for feedback (member checking), ensuring the analysis accurately reflected their experiences. The analysis process involved multiple iterations of coding and theme refinement to ensure the robustness of the findings.
Validity and Reliability
The research proposal was reviewed by the National University of Science and Technology Institutional Review Board (NUST IRB) to obtain approval (NUST/IRB/2024/016) for this study. Both the methodology and data collection instruments were adjusted according to the input received. A pre-test was conducted to sample the feasibility of data collection using the interview guide.
Ethical Consideration
Ethical approval for this study was granted by the Institutional Review Board of the National University of Science and Technology (NUST IRB), Zimbabwe (Clearance Number: NUST/IRB/2024/016). Written informed consent was obtained from all participants aged 18 years and above, while for minors (below 18 years), written consent was provided by parents or legally authorised representatives (LARs), along with written assent from the students themselves. Stakeholders, including teachers, nurses, and administrators, also provided written consent prior to participation. The consent process ensured participants were fully informed of the study’s purpose, procedures, confidentiality measures, and their right to withdraw without consequence. All data were anonymised to protect participant identities, and no personally identifiable information was collected. Participation was entirely voluntary, with no penalties for withdrawal. The study adhered to strict confidentiality protocols, with data stored securely on password-protected systems. The NUST IRB reviewed and approved all consent procedures, and no waivers were required as full written consent was obtained in all applicable cases.
Findings
Mental Health Challenges Faced by Students
To establish the context and burden of mental health need that the school health system is tasked with addressing, students were screened for self-reported symptoms of common mental health challenges. A challenge was considered present if half or more of the associated symptoms were reported. The assessment covered depression, anxiety, mood disorders, self-esteem issues, and attention deficit. Figure 2 illustrates the self-reported burden of mental health symptoms among the sampled students. Anxiety (69.4%, n = 43), attention deficit (62.9%, n = 39), and self-esteem issues (72.6%, n = 45) emerged as the most prevalent challenges, with self-esteem issues and attention deficit affecting the largest number of students. Depression was found to be less common in comparison (33.9%, n = 21).

Self-reported burden of mental health symptoms among students.
Attention Deficit
Out of 62 participants, females showed a higher prevalence of attention deficit (n = 23) compared to males. The age group 17 to 19 years had the highest number of students with attention deficit (n = 18), while the 13 to 14 years age group had the lowest (n = 8). There was an equal distribution between Form 1-2 and Form 3-4 students (n = 14 each). Chi-square analysis revealed a significant gender difference (P = .0123) but no significant differences across age groups or education levels (Table 2).
Cross Tabulation for Demographic and Attention Deficit.

Abbreviation: f, frequency (count of students).
Self-Esteem Issues
Self-esteem issues were almost equally distributed between males (n = 23) and females (n = 22). The 17 to 19 age group showed the highest prevalence (n = 27), while the 13 to 14 age group had the lowest (n = 7). Form 5 to 6 students had the highest number of self-esteem issues (n = 18). Chi-square analysis showed no significant differences across gender, age groups, or education levels (Table 3).
Cross-Tabulation for Demographics and Self-Esteem.

Abbreviation: f, frequency (count of students).
Utilisation of the School Health System
Despite the high self-reported symptom burden, utilisation of the existing school health system was low. Only 40.3% (n = 25) of the 62 students reported having ever used the system for mental health support. The primary reason cited by the majority of non-users (59.7%, n = 37) was a lack of awareness of the services available or how to access them.
Curriculum and Content Service Package of School Health Systems
The qualitative data revealed that the school’s health system curriculum is primarily delivered through two main themes: Health Clubs and Guidance and Counselling. Additionally, five subthemes arose from these key themes. Interviews with staff outlined the various functions and modes of delivery for these components. Health clubs were described as a versatile platform for mental health education, operating through after-school and after-lunch programs. A teacher noted their importance for engagement: “After school programs like health clubs are very important as students engage and come together and do dammars that help in learning” (T1). Their role was seen as threefold: to educate, entertain, and foster interaction, thereby creating a less formal environment for learning. As one administrator explained, “They assist in giving education in a manner that gives entertainment and interaction with teachers, students and the nurses” (A2).
Regarding Guidance and Counselling (G&C), a key finding was the lack of specialised personnel. Instead, the responsibility is distributed among all teachers. A teacher highlighted this challenge: “Used to have a teacher specifically for guidance and counselling. . . currently all teachers are doing it” (T2). Despite this constraint, the school has formally integrated G&C into the weekly timetable “just like other subjects” (A1), signalling its institutional priority. The core purpose of this service was to equip students with knowledge to manage mental health challenges. A health master stated the goal was to “equip students with knowledge on mental health and give advice to all on how best to deal with the mental challenge before and after it has occurred” (HM3). These themes and supporting quotations are further detailed in Table 4.
Curriculum or Content Service Package of School Health Systems Aimed at Dealing with Different Mental Health Challenges.

Barriers to Implementation and Optimal Functioning of School Health Systems
Several barriers to effectively implementing school health systems were identified. Poverty was a predominant theme, directly hindering the system’s reach. Key informants explained that a lack of school fees and limited resources at home prevent students from attending school consistently, thereby excluding them from accessing any school-based services. As one administrator noted, “learners not going to school because of lack of school fees will not come to school for services” (A2). Beyond access, poverty also cripples the educational component of the system through a lack of resources. A teacher lamented the “lack of qualified resource personnel and reading material,” expressing a desire for basic materials “like pamphlets so that we can distribute to our learners and teachers” (T1). These findings are presented in Table 5.
Barriers to the Optimal Functioning of School Health Systems in Managing Mental Health Challenges.

Substance use and abuse was another critical barrier, directly impairing the system’s effectiveness by reducing student engagement and receptiveness to interventions. Informants reported that substance use, driven by peer pressure and academic stress, leads to negative thoughts and disengagement. Peer pressure was a significant driver, with students believing substance use was a prerequisite for social acceptance and academic success, such as the false notion that “smoking marijuana can help you pass difficult subjects like maths” (A1). Furthermore, the intense pressure of a heavy academic workload was cited as a key trigger. A health master stated reported observing “rampant drug due to pressure of work,” explaining that students to turn to drugs “thinking they will reduce the pressure” (HM1), which in turn impairs their ability to benefit from support services (Table 5).
Strategies for Improving School Health Systems
Participants proposed multiple strategic improvements, which can be categorised into proactive engagement activities and systemic structural changes.
Key informants (staff) strongly advocated for increasing physical activities and institutional tours. They argued that physical activities serve multiple purposes: they “refresh the mind of students and foster interaction” (A2), keep students occupied, and reduce tendencies towards substance use. Institutional tours to mental health facilities were proposed as a powerful, tangible deterrent. The value was in making the consequences of poor mental health real for students by allowing them to “hear testimonies from others concerning consequences of mental health challenges” (A1) or to “actually see those who will be mentally challenged and they will be told how they got to be in this situation” (T1).
Students, when asked for improvement strategies, focused on structural enhancements to the system itself (Figure 3). The most frequent suggestion (54.84%) was the need for more trained staff, highlighting the perceived insufficiency of the current model where all teachers provide counselling. This was closely followed by a call for increased funding (40.32%) to address resource limitations, and the integration of social-emotional learning (SEL) programs (48.39%) into the curriculum for a more skills-based approach. Additionally, half of the students (50%) identified improved access to counselling as a key priority. Further details on suggested strategies, including workshops and awareness campaigns proposed by staff, are compiled in Table 6. Participants suggested various strategies to enhance the effectiveness of school health systems in managing mental health challenges. Key informants emphasised proactive strategies such as increasing physical activities and institutional tours to mental health facilities. They argued that physical activities “refresh the mind of students and foster interaction” (A2), keeping them occupied and reducing tendencies towards substance use. Tours to institutions like Ngomahuru were proposed so students could “hear testimonies from others concerning consequences of mental health challenges” (A1), making the risks more tangible. These strategies are detailed in Table 6.

Strategies for improving school health systems.
Strategies for Improving School Health Systems and Aiding Their Performance in the Management of Mental Health Challenges.

Discussion
Mental Health Challenges Faced by Students
The results indicated that attention deficit disorder and low self-esteem were the two most frequently experienced mental health conditions among students. This finding aligns with recent research by Sella et al, 24 which reported similar prevalence rates for these conditions. However, the context differs, as our study focuses on a rural secondary school, suggesting these challenges are pervasive across both urban tertiary and rural secondary educational environments in different countries. 24 A cross-tabulation of attention deficit with gender revealed a higher proportion of female students experiencing attention deficit compared to male students. This gender disparity is consistent with findings by Rucklidge, 25 who reported a higher likelihood of attention deficit disorder among adolescents identifying as female. This similarity across studies from New Zealand and Zimbabwe indicates a potential transnational pattern in gender presentation of ADHD symptoms that merits further investigation.
The study found that attention deficit disorder peaked in frequency around the age of 18, with higher prevalence in the 17 to 19 age group. This age-related pattern is supported by Zendarski et al (2017) 26 , who observed a higher incidence of attention deficit among students in forms 5 to 6 (grade 12-13). This parallel suggests that academic pressure in critical exam years may be a universal trigger for attention difficulties, regardless of the country’s economic status. Regarding educational attainment, equal numbers of students in forms 3 to 4 (grade 11-12) and 5 to 6 exhibited attention deficit disorders. Cross-tabulation of self-esteem revealed higher levels among male students compared to female students. This finding is consistent with Gentile et al, 27 who reported significantly higher self-esteem levels in male adolescents. The replication of this finding in a rural African context underscores the robustness of this gender difference in self-esteem across diverse cultural settings. The study also found a substantial proportion of students with high self-esteem in the 17 to 19 age bracket, corroborating the work of Orth et al, 28 who identified this age range as having the highest levels of self-esteem relative to other age groups. This suggests a possible developmental universality in the trajectory of self-esteem. The results showed a higher prevalence of high self-esteem among students in forms 5 and 6, aligning with Poorthuis et al, 29 who reported stronger self-esteem in these advanced educational levels. This may be attributed to growing maturity and a stronger sense of identity, which appears to be a common experience for older adolescents across different educational systems.
School Health Systems’ Curriculum or Content Service Aimed at Addressing Mental Health Challenges
The findings highlighted health clubs as part of the curriculum service package addressing various mental health issues. This approach is supported by Kakunje, 30 who demonstrated the effectiveness of health clubs in increasing peer support, reducing stigma associated with mental health issues, and enhancing mental health awareness. Hurley et al 31 further emphasised the role of health clubs in providing a space for peer support and education, particularly beneficial in addressing adolescent mental health concerns. The positive perception of health clubs in both a well-resourced country like Australia and a resource-constrained setting like rural Zimbabwe highlights their adaptability and potential as a low-cost, high-engagement intervention.
Guidance and counselling were also identified as key components of school health systems’ curricula for addressing mental health issues. This finding is supported by Subhan Iswahyudi et al, 32 who emphasised the utility of guidance and counselling services in providing individualized support and interventions for mental health difficulties in Indonesia. A key difference, however, is the implementation. While the Indonesian study likely refers to specialised counsellors, the study found that “all teachers are giving guidance and counselling” (T2) due to a lack of dedicated personnel. This highlights a critical resource gap between policy aspiration and on the ground reality in rural Zimbabwe.
Barriers to Implementation and Optimal Functioning of School Health Systems
The results identified poverty as a significant barrier to the effective implementation of school health systems. This finding is consistent with Mohlabi et al, 33 who highlighted poverty as a major obstacle to accessing mental health care in schools, particularly for disadvantaged and marginalised groups. Substance use and abuse were also identified as hindrances to the implementation and effectiveness of school health systems. Waller et al 34 corroborated this finding, noting that substance use and abuse can significantly impede the efficacy. Substance abuse reduces student engagement and receptiveness, making them less likely to participate in or benefit from the existing support structures, like health clubs and counselling, thereby rendering the system less effective. 34
Strategies for Improving School Health Systems and Enhancing Their Performance
The study identified increasing physical activity as a strategy for improving the efficacy of school health systems. This approach is supported by Barcelona et al, 35 who emphasised the crucial role of physical activity in enhancing mental health and overall well-being among adolescents, particularly in educational settings. 35 This suggests that the mental health benefits of physical activity are a universal principle, though the infrastructure to support it may differ greatly between settings. Institutional visits were highlighted as a potential tactic for enhancing school health programs. Mann et al 36 support this finding, demonstrating that visits to mental health institutions can positively influence attitudes toward mental health in school health systems. Awareness campaigns were identified as another strategy to improve school health programs. This approach is endorsed by Kolbe 37 and Moussi et al, 38 who recognise the effectiveness of awareness campaigns in increasing knowledge and understanding of mental health issues among students and teachers. Implementing campaigns would thus serve to bridge the gap between the system’s existence and its accessibility to students.
The study found that 54.84% of students believed that increasing staff would enhance the effectiveness of school health systems. This perception aligns with Brener et al, 39 who emphasised the importance of adequate school mental health staff in providing effective care. This suggestion from students directly tackles the barrier of overburdened staff identified by key informants, who noted that “all teachers are giving guidance and counselling” (T2) due to a lack of dedicated personnel. Hiring trained staff would professionalise the service and increase its capacity. Littlecott et al 40 further support this finding, noting that higher staff-to-student ratios in mental health at educational institutions are associated with improved quality of mental health services. Half of the students identified access to counselling as a strategy for enhancing school health systems. This finding is supported by Kolbe, 37 who reported that school-based counselling effectively reduced student behavioural issues, anxiety, and depression.
Conclusion and Recommendations
It can be concluded from the results obtained that students at Mapanzure High School are experiencing a significant burden of mental health symptoms, and key informants generally view the intended school health systems as helpful. However, the potential of the school health system to address this burden is limited by critical obstacles, including poverty and substance use and abuse, and a stark lack of awareness and resources, leading to low utilisation. These results may help create a supportive and inclusive environment that values student health and emotional wellbeing, that can lead to improved academic outcomes and a positive life for students.41,42
Recommendations
To bridge the gap between these findings and the goal of creating a supportive and inclusive environment, several recommendations can be proposed.
Integrating mental health literacy into the core curriculum through structured Social-Emotional Learning (SEL) programs would directly address the lack of awareness, destigmatise help-seeking behaviour, and build student resilience.
Investing in specialised human resources by training and deploying dedicated guidance personnel, even if shared across school clusters, would provide more professional and consistent support than the current model of relying on all teachers as counsellors. Additionally, allocating targeted funding for resource-poor schools would enable the procurement of essential materials and sustain core activities like health clubs and awareness campaigns.
Formalising community-school partnerships with local health facilities and social services would create a holistic support system and referral pathway to help mitigate the impact of poverty on student attendance and access to care.
Implementing these recommendations would translate the study’s results into concrete actions, directly addressing the identified barriers and leveraging the existing system to promote a school environment that genuinely supports student wellbeing and academic success.
Limitations
This study has several limitations that should be considered when interpreting the results. The cross-sectional design provides a snapshot of the situation at a single point in time and cannot establish causality between the school health system and mental health outcomes. Additionally, the study was conducted in a single rural secondary school in Zimbabwe, which limits the generalisability of the findings to urban schools or other regions with different socio-economic and cultural contexts. The sampling frame also excluded adolescents who were not enrolled in or attending school, a group that may experience a disproportionate burden of mental health challenges and face even greater barriers to care. Their perspectives are therefore missing from this analysis.
The assessment of mental health challenges was based on self-reported symptoms using a screening tool, not a clinical diagnostic interview. This likely captures symptomatic burden but may not equate to formal diagnoses. Furthermore, the tool did not account for students who might already be on treatment and thus potentially less symptomatic. Finally, while the mixed-methods approach is a strength, the qualitative sample, though purposively selected, is small and represents the views of specific stakeholders within one school, which may not capture the full range of experiences and barriers.
Footnotes
Author Note
NNN is a former undergraduate student in the Department of Environmental Science and Health at NUST. MYK holds a MSc degree in Environmental Health and is a Lecturer in the Department of Environmental Health at the National University of Science and Technology (NUST) in Bulawayo in Zimbabwe. WNN is an Associate Professor in the Department of Environmental Health at the University of Botswana. The author is also a post-doctoral research fellow at the Department of Public Health at the University of the Free State, South Africa.
Ethical Considerations
Ethical approval for this study was granted by the National University of Science and Technology in Bulawayo, Zimbabwe (NUST IRB). (Ethics Clearance Number: NUST/IRB/2024/035). Permission to conduct the survey was also sought from participating companies.
Consent to Participate
Written informed consent was obtained from all participants aged 18 years and above, while for minors (below 18 years), written consent was provided by parents or legally authorised representatives (LARs), along with written assent from the students themselves. Stakeholders, including teachers, nurses, and administrators, also provided written consent prior to participation. The consent process ensured participants were fully informed of the study’s purpose, procedures, confidentiality measures, and their right to withdraw without consequence.
Author Contributions
NNN conceptualised the research idea, collected the data, and drafted the initial manuscript. MYK coordinated the research, guided the data analysis, and coordinated the manuscript writing process. WNN and MYK provided significant intellectual input in the interpretation of data, restructuring, and critical revision of the manuscript for important academic content. All authors reviewed, edited, and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.