
Abstract
Aims:
The aim of this study was to explore healthcare leaders’ perceptions of the contribution of artificial intelligence (AI) to person-centred care (PCC).
Methods:
The study had an explorative qualitative approach. Individual interviews were conducted from October 2020 to May 2021 with 26 healthcare leaders in a county council in Sweden. An abductive qualitative content analysis was conducted based on McCormack and McCance’s framework of PCC. The four constructs (i.e. prerequisites, care environment, person-centred processes and expected outcomes) constituted the four categories for the deductive analysis. The inductive analysis generated 11 subcategories to the four constructs, representing how AI could contribute to PCC.
Results:
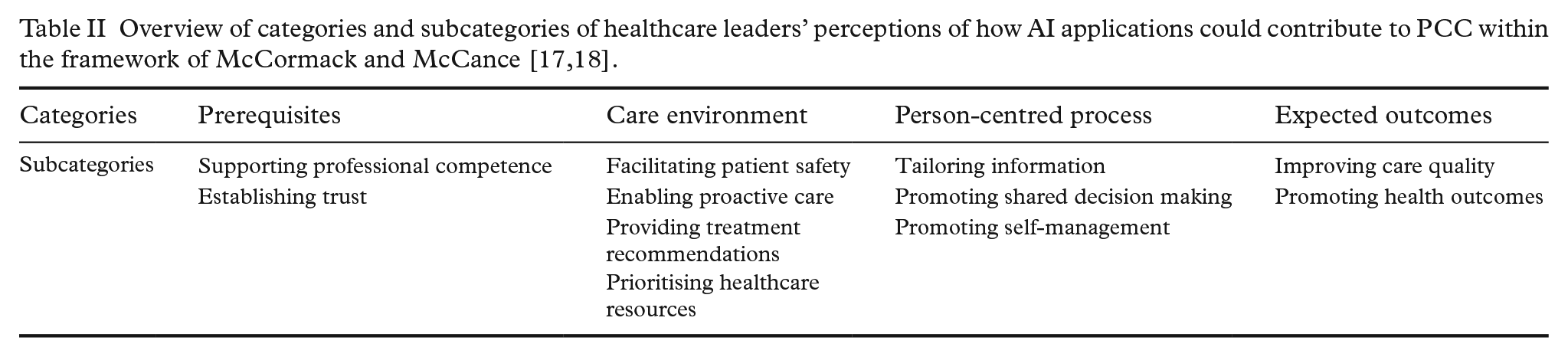
Healthcare leaders perceived that AI applications could contribute to the four PCC constructs through (a) supporting professional competence and establishing trust among healthcare professionals and patients (prerequisites); (b) including AI’s ability to facilitate patient safety, enable proactive care, provide treatment recommendations and prioritise healthcare resources (the care environment); (c) including AI’s ability to tailor information and promote the process of shared decision making and self-management (person-centred processes); and (d) including improving care quality and promoting health outcomes (expected outcomes).
Conclusions:
Keywords
Introduction
Artificial intelligence (AI) is often thought of as a technology that will transform healthcare. AI can be defined as a machine-based system capable of making predictions, recommendations or decisions that impact real or virtual environments, all based on a specified set of human-defined objectives and operating with varying levels of autonomy. This definition highlights the multifaceted nature of AI, emphasising its ability to analyse data and adapt to different situations while serving specific goals determined by human users [1]. AI applications are argued to improve healthcare quality through improvements in diagnostics, monitoring, access, advanced decision making and virtual consultations [2,3]. However, less focus has been placed on how AI can improve outcomes in public health [4,5], healthcare services [6] and person-centred care (PCC) [7]. The implementation of AI applications can contribute to PCC by redefining patient and physician relationships [6] and by enhancing person-centric and personalised healthcare [7]. The anticipated potential is based on the ability of AI applications to process and learn from large volumes of available healthcare data and to identify complex patterns beyond human comprehension [8]. These abilities raise questions about responsibilities related to the level of autonomy granted to AI applications [9]. Research has anticipated that AI and precision medicine have the potential to revolutionise healthcare by identifying patients with special care needs through insights and learning from complex data [10], supporting clinical work [11] and increasing the efficiency and effectiveness of processes in health services [4] and giving healthcare professionals the ‘gift of time’ to build relationships with patients [12]. This aligns with the objectives of PCC. PCC emphasises the recognition of the patient as an expert on their illness and life situation [13]. Patient experiences, clinical effectiveness and patient safety are cornerstones of healthcare quality. Data from patient experiences can identify strengths and weaknesses in the care provided [14]. Thus, implementing AI applications in healthcare could contribute value to PCC [15].
PCC is essential across healthcare settings, from public health prevention to clinical treatment. In public health, PCC focuses on empowering individuals through self-care and health promotion, whereas in clinical care, PCC emphasises patient engagement in decision making and personalised treatment [16]. To ensure effective implementation, PCC must be addressed at multiple levels, as outlined in McCormack and McCance’s framework for PCC, which includes four constructs: prerequisites, care environment, person-centred processes and expected outcomes [17,18]. Prerequisites refer to professional competence, commitment to the job, clarity of beliefs and values, self-knowledge and advanced interpersonal skills to enhance communication. The care environment involves the healthcare context, including a supportive organisation, an appropriate mix of skills, effective staff relationships, shared decision-making systems, power sharing, potential for innovation and the physical environment. Person-centred processes focus on delivering care that aligns with patients’ values and beliefs, inviting patients to share in decision making, engaging authentically, being sympathetically present and providing holistic care. Expected outcomes represent the results of effective PCC, such as a positive experience of care, patient involvement in care, a sense of well-being and a healthful culture [17,18]. Successful PCC adoption depends on aligning healthcare structures, processes and culture with person-centred values at prevention and treatment levels [16]. Implementing PCC in healthcare necessitates a deep understanding of patients’ values and preferences, fostering shared decision making and ensuring seamless coordination among healthcare professionals. This approach underscores the importance of supportive leadership and cultivating an organisational culture prioritising respect, dignity and patient empowerment, ultimately leading to improved health outcomes and patient satisfaction [19]. Research indicates that the implementation of AI in healthcare can contribute to PCC by strengthening patients’ autonomy [15], enabling patients to process their own data to promote health [20], giving healthcare professionals more time to spend with patients [7], redefining physician–patient relationships [7] and promoting personalised healthcare [21].
However, empirical evidence of the success of the application of how to succeed with implementing AI in healthcare is scarce and not in proportion with the current needs in practice [22]. Recent systematic literature reviews show a lack of empirically grounded research on AI implementation in healthcare and the need for methodological development to support implementation processes [22,23]. The transformative potential of AI applications in healthcare is significant. Yet, delays in their implementation and adoption postpone the realisation of practical benefits. In this context, it is essential to understand the perceptions of healthcare leaders, given their key role in the AI implementation process. More knowledge is needed on the value of AI applications from healthcare leaders’ perceptions and understanding of healthcare leaders’ roles as gatekeepers and facilitators of successful implementation [24]. In the context of PCC, research considering healthcare leaders’ perceptions of AI applications’ contribution to PCC is scarce, and more knowledge is thus needed.
Aim
This study aimed to explore healthcare leaders’ perceptions of the contribution of AI to PCC.
Methods
Study design and context
This qualitative study has an explorative design with an abductive qualitative content analysis approach [25] and adheres to the Consolidated Criteria for Reporting Qualitative Research (COREQ) 32-item checklist [26]. The study was approved by the Swedish Ethical Review Authority (no. 2020-06246), conformed to the principles outlined in the Declaration of Helsinki [27] and fulfilled the ethical requirements of research: informed consent, confidentiality and participant safety [28]. None of the authors worked in the county council. Over the past 10 years, this county council has committed significant resources to enhancing its ability to organise and analyse healthcare data for the improvement of care [29]. When the current study was conducted, the organisation was in the initial stages of AI deployment, and no AI applications had yet been implemented.
Participants
The purposeful recruitment of study participants from the county council focused on high-level leaders in a position to potentially influence the implementation of AI. The study included 26 healthcare leaders who had knowledge about AI and clinical practice in a county council in the south-west of Sweden (Table I). A group of 28 healthcare leaders were invited using snowball recruitment. Two declined, leaving 26 participants. Initially, five individuals were chosen for their expertise and experiences. After their interviews, they recommended other leaders to be interviewed.
Participants’ characteristics (N=26).

Data collection
Individual semi-structured interviews were conducted, via face-to face or video communication, between October 2020 and May 2021. Neither of the two researchers (L.P. and D.T.) who conducted the interviews had any previous relationship with the participants. The interviews were based on an interview guide concerning beliefs surrounding and attitudes towards using AI applications to support healthcare improvements with questions such as: What are the possibilities and opportunities to use AI in your part of the organisation as you see it, from your perspective and with your knowledge about the technology? Could you describe any areas of care that would have an added potential for care improvement? What type of improvement might one expect in these areas of care? Potential results? Influence on patients/population? Influence on employees? The informants in the interviews did not discuss AI in relation to any specific or concrete applications. Instead, their views were shaped by a broader understanding of AI, influenced by the county councils’ investments in data infrastructure and advanced analytics capacity aimed at enhancing clinical decision support, care pathway optimisation, resource allocation and delivering more precise, person-centred care. This context framed their discussions. The interviews lasted between 30 and 120 minutes, with a total length of 23 hours and 49 minutes, and were audio-recorded and transcribed verbatim.
Data analysis
An abductive qualitative content analysis was conducted manually by the researchers through a series of iterative steps [25]. Initially, an inductive phase involved multiple readings by the first (I.L.) and last (L.P.) authors to establish familiarity. Subsequently, meaningful phrases relevant to the aim of the study were identified, condensed into meaning units, abstracted and coded [25]. In the deductive phase, the codes were then organised into the four constructs outlined in the PCC framework: prerequisites, care environment, person-centred processes and expected outcomes [17,18]. Within each construct, an inductive process was employed, resulting in the formation of four categories. Codes were compared based on similarities and differences and subsequently regrouped into 11 subcategories. After the 15th interview, no new substantial content or subcategories emerged, indicating that adequate material had been gathered for the study. However, the subsequent 26 interviews provided more profound insights and variations in descriptions within the different subcategories. These subcategories encapsulated the manifest content that had emerged from the interviews regarding the impact of AI implementation on PCC. Throughout this analytical process, continuous discussions and reflections among all authors were held to ensure consensus [25] and to guard against the omission of meaningful data. The research group was interdisciplinary and had experiences in PCC, information-driven care and qualitative methods.
Results
The analysis resulted in 11 subcategories within the four categories (prerequisites, care environment, person-centred processes and expected outcome) in the PCC framework [17,18], representing healthcare leaders’ perceptions of how AI applications could contribute to PCC (Table II).
Prerequisites
Healthcare leaders perceived that AI applications could contribute to PCC by creating prerequisites to support professional competence and establish trust among healthcare professionals and patients.
Supporting professional competence
Healthcare leaders described that AI applications could contribute to PCC by enhancing professional competence. They viewed AI as acting like experienced colleagues, available for healthcare professionals to consult for advice and support in clinical work. For example, nurses could consult the AI application before seeking input from a physician, ensuring timely and accurate information that enhances PCC.
Doctor James [the AI application] can serve as advice to the nurse. Instead of running to Doctor Sarah [the physican] and bothering her, the nurse starts with Doctor James first. I think it should be seen as a second opinion. A colleague with limited experience will initially let Doctor James make a second opinion. (Leader no. 7)
Leaders highlighted the usefulness of AI as a decision support tool, providing a valuable second opinion in various assessments. AI applications were perceived to be beneficial. They allowed the leaders to avoid unnecessary consultations with specialists, aiding general practitioners and supporting younger and less experienced physicians. AI applications could also assist healthcare professionals when dealing with patients facing complex and challenging treatment by offering an overall picture of patients’ health status and suggesting appropriate treatment options.
Establishing trust
Healthcare leaders emphasised the need for thorough preparation of AI implementation in healthcare to ensure confidence in AI-assisted assessments. They highlighted that trust, a key prerequisite for PCC, is equally essential for the effective use of AI in healthcare and that transparency is crucial to building trust.
If you want to build trust, you have to know that what you’re working on actually gives me the information I need and that I can trust the information. That’s essential; otherwise, it’s all over. (Leader no. 4)
Leaders expressed the need for healthcare professionals and patients to be informed about how AI operates and the reliability of its outputs. Clear and detailed communication about the functionalities, data sources and decision-making processes of AI applications fosters trust in AI.
Care environment
Healthcare leaders perceived that AI applications could contribute to PCC in the care environment, built on AI’s ability to facilitate patient safety, enable proactive care, provide treatment recommendations and prioritise healthcare resources.
Facilitating patient safety
Healthcare leaders perceived that AI applications could enhance PCC by providing conditions for value-creating and safe patient care encounters. A valuable care encounter was described as one where patient assessments were informed by credible risk scores that could be generated by AI algorithms, ensuring more accurate and personalised care. They noted that AI applications could identify patterns in patient care history by integrating data from various healthcare settings, providing a comprehensive overview of patients with multimorbidity. This capability could enhance patient safety and support PCC by ensuring a holistic understanding of patients’ health status.
I think AI has an opportunity to see the whole person in that amount of data. Proposing and finding probabilities. (Leader no. 1)
Enabling proactive care
Healthcare leaders expressed that AI applications could be crucial to proactive care by predicting health outcomes and diagnoses, such as identifying rare data patterns which can highlight previously overlooked patients. Such applications can monitor and analyse data on factors such as fatigue, a sedentary lifestyle and symptoms of depression, thereby providing healthcare professionals with valuable insights. AI could also act as a warning system in the care environment, alerting healthcare professionals to potential issues that require their attention and ensuring that resources are directed to those patients who are most in need.
The AI application raises a flag. Now, this patient has diabetes. The blood sugar has been fine but suddenly drops or rises, and a warning appears. In this way, healthcare can catch it before it goes too far . . . Then, the patients who really need that help come to care. (Leader no. 15)
As decision support tools, AI could enhance the standardised diagnosis of diseases in fields such as radiology, dermatology and oncology. The leaders highlighted that utilising AI applications as a decision support tool in proactive care could add substantial value and increase the quality of clinical interactions with patients.
Providing treatment recommendations
Healthcare leaders described the value of AI applications in providing individually tailored treatment recommendations. They also suggested that AI could support a gender-neutral perspective on diseases that manifest differently in females and males, ensuring tailored treatment recommendations for patients.
Suppose everyone at our healthcare centres gets a health watch [a smart watch] at home and registers, for example, fatigue, depression or less physical activity. In that case, we can discover that there is a person at risk of becoming depressed. . . . Then the watch could send a signal and say, ‘Hey, please make an appointment here’ or ‘Fill in this form on the watch’. (Leader no. 13)
Prioritising healthcare resources
AI applications were described as decision support tools that could efficiently prioritise healthcare resources. Healthcare leaders highlighted potential priority areas, such as AI triage in primary care, which could change existing workflows and enhance efficiency. For example, AI could handle patient anamnesis at home, ensuring healthcare professionals see only those patients for whom a visit is necessary, thereby eliminating unnecessary appointments. By optimising resource allocation, AI ensures that care is tailored to individual needs and circumstances, thus contributing to PCC. Implementing AI applications as decision support at the organisational level could enhance various care processes, improving overall efficiency and strengthening the person-centred approach to healthcare delivery by ensuring that resources are directed where they are most needed.
More people can receive care in less time and we can also find people earlier than our human ears and eyes, and so on, can do, and perhaps you, as a patient, are very satisfied. It is probably the greatest success when I, as a patient, when I am in the hospital, feel safe and satisfied and have received help on time. (Leader no. 13)
Person-centred processes
Healthcare leaders perceived that AI applications could contribute to PCC in the person-centred process by leveraging AI’s capability to tailor information, thereby facilitating shared decision making and promoting self-management among patients.
Tailoring information
Healthcare leaders described how AI applications could tailor information to individual patient needs and preferences. These perceptions are based on AI algorithms leveraging large amounts of data to provide personalised information and assessments. AI applications could deliver tailored information by monitoring diseases and treatments, assisting patients in understanding and evaluating this data and thus empowering patients to make informed decisions about their health and treatment options.
What we are moving into now is precision medicine. ‘With your particular conditions and background, this support seems to be the best for you’. Yes, you have high blood pressure, so you get high blood pressure medication. Yes, but how do we know it works for you and your conditions, genetics, and way of responding to medicines? We are using AI, among other things, to tailor care. (Leader no. 2)
Promoting shared decision making
Healthcare leaders described that AI applications could potentially foster shared decision-making processes. They elaborated on how AI could facilitate this by providing patients with valuable and adequate information and empowering them to participate actively.
I am passionate about giving patients the power to make individual decisions, then some form of feedback is required. You can ask based on the data you generate, and you could get that feedback from our data warehouse. If it’s a technical set-up, it’s incredibly complex, but it’s no more complicated than getting stock market robots to play along. (Leader no. 14)
Leaders anticipated that AI applications would enhance communication between patients and healthcare professionals. By enabling patients to make independent decisions in investigations, assessments and treatments, smart and efficient AI solutions can streamline care, ensuring that more patients receive timely and effective care.
Promoting self-management
Healthcare leaders expressed that AI has the potential to contribute to person-centred processes by promoting self-management among patients, thereby facilitating committed patient participation in care processes. AI applications could achieve this by recommending self-care advice or empowering patients to make decisions. Self-monitoring at home presents an opportunity to enhance care processes.
I believe a lot in self-monitoring as soon as we can get a technology that can communicate with our electronic health records, which I know is terribly difficult, but when we can. As a patient, you must self-monitor at home to ensure that your measurements are entered and that you have them in the electronic health records. (Leader no. 15)
However, leaders also had concerns that not all patients (e.g. elderly patients and patients with severe diseases) would benefit from AI applications or use them to the same extent as patients with more self-monitoring capacity.
Expected outcomes
Healthcare leaders perceived that AI applications could contribute to PCC with the expected outcomes of improving care quality and promoting health.
Improving care quality
Healthcare leaders expressed high expectations that AI applications could enhance the quality of care for patients through streamlined clinical workflows and more personalised and customised care experiences. Integrating AI into healthcare systems is poised to streamline administrative tasks, freeing healthcare professionals’ time and energy to focus more on direct patient care. Leaders perceived that implementing AI applications in healthcare has the potential to offer patients evidence-based, effective and personalised care, ultimately enhancing health outcomes and overall patient well-being.
The success will be when we see that investments and collaborations [in AI] substantially increase quality for our patients and residents. (Leader no. 8)
Promoting health outcomes
The leaders emphasised the potential of AI to enhance personalised treatment for each patient, ultimately improving their health outcomes by increasing treatment adherence and reducing disease symptoms. AI algorithms were seen as valuable tools for identifying changes in patient health status and prompting contact with healthcare professionals about issues beyond the primary concern for the visit, thus further improving patient health. This proactive approach allows for personalised care, ultimately promoting patient health. Utilising AI for health promotion enables healthcare systems to enhance PCC and attain better health outcomes.
If you can get the whole picture of the entire resident, then maybe primary care can take care of the individual resident completely differently. ‘I see that you don’t need to come here to check your sugar, but on the other hand, you probably need to go and have your mammogram or I think you should check your heart’. (Leader no. 15)
Discussion
The principal findings of this study indicate that healthcare leaders perceive that implementing AI applications in healthcare could significantly contribute to PCC. Implementing AI applications into professionals’ daily work is seen as supporting professional competence, providing access to advice and support for clinical decisions and fostering trust between healthcare professionals and patients. These are all essential prerequisites for PCC. Furthermore, AI is expected to enhance the care environment by facilitating patient safety, enabling proactivity, supporting treatment recommendations and prioritising healthcare resources. Additionally, AI’s ability to tailor and customise information is seen as a key factor in facilitating shared decision making and promoting self-management among patients [7,13]. Healthcare leaders believe that integrating AI into healthcare can substantially improve care quality and promote patient health. Research indicates that there are various opportunities to enhance clinical competence through support from AI [30] by virtue of the fact that AI offers data-driven guidance and second opinions in ways that are similar to experienced colleagues but with greater availability and speed [31], which is highly appreciated by patients [32]. Access to accurate and timely information ensures a more knowledgeable and competent workforce [30], which is key to effective PCC [7]. Additionally, AI can facilitate continuous professional development by providing up-to-date and real-time medical knowledge and guidelines, thereby benefiting less experienced healthcare professionals and offering continuous learning [31]. Transparency regarding AI functionalities, data sources and the reliability of outcomes is essential to the establishment and building of trust among healthcare professionals [33] and patients [32]. It is central to the successful integration of AI in healthcare. By delving deeper into these aspects, healthcare providers will be enabled to ensure that AI implementation both improves clinical outcomes and fosters a person-centric approach [7,13].
In the current study, the leaders emphasised that AI applications promise to improve patient safety through comprehensive data analysis, risk assessments, identification of patterns in patient care history and a holistic view of patients with multimorbidity. These capabilities closely align with the fundamental principles of PCC [13]. Research shows that appropriately implemented AI applications used as decision support systems can enhance patient safety by refining error detection, patient stratification and medication management [34]. The leaders perceived AI to be valuable to decision support, enabling earlier illness detection, supporting diagnostic decisions and providing personalised treatment recommendations. Additionally, they regarded AI as a tool for resource optimisation, aiding decision making at the organisational level. These perceptions align with earlier research that demonstrates AI’s usefulness in patient data management, advanced diagnostic and treatment planning, predictive medicine, clinical decision making and health service management [35 –37]. Furthermore, leveraging AI applications in administrative functions can enhance efficiency and optimise resource allocation, thus fostering proactive and personalised healthcare [21].
AI’s ability to tailor information to patients’ needs and preferences is crucial to PCC [13]. By processing vast amounts of data, AI can provide personalised assessments and treatment proposals, potentially empowering patients to understand their health conditions and to make informed decisions about their treatment options [30]. In person-centred processes, healthcare professionals may need to assist patients in understanding the information provided [38]. This empowerment is vital for patients’ health [39], allowing them to take control of their well-being with AI support. Thus, tailoring health information to patients by AI applications can promote patients’ health literacy, enabling them to participate in person-centred processes [7,32]. However, the risk of using AI platforms in improving health literacy has been highlighted [40], and there is a need for research and activities that build evidence to support the development. By offering comprehensive and understandable information, AI tools can enable patients to participate actively in their care and make informed decisions [32]. This collaborative approach aligns treatment plans with patients’ values and preferences, thereby leading to better health outcomes and increased patient satisfaction. With the anticipated shortage of healthcare professionals, AI can bridge gaps by equipping patients with tools for independent health decisions and ensuring timely and effective care delivery [41]. AI applications can provide personalised self-care advice and facilitate self-monitoring, enabling proactive management of chronic conditions [42]. This approach can improve patient engagement and adherence to treatment plans and reduce complications and clinical visit frequency. However, it is essential to address accessibility concerns, particularly for elderly patients and those with severe conditions, who may struggle with AI technologies [41].
Integrating AI into healthcare systems is expected to increase care quality by streamlining clinical workflows and administrative tasks, allowing healthcare professionals to focus more on direct patient care [43]. By utilising patient-provided information on health conditions and management, PCC impacts outcomes by linking healthcare services to results and integrating systematic data, assessments and recommendations into clinical practice, thereby improving care quality [19]. AI algorithms can monitor patient health status in real time, identifying subtle changes that may require medical attention. This proactive approach ensures that patients receive timely care for emerging issues [21]. By leveraging AI, healthcare systems can support PCC more effectively and can tailor interventions to individual patient needs and improve overall health outcomes. This aligns with the goals of PCC by addressing barriers to healthcare access, ensuring that patients receive timely and preferred care, promoting better health outcomes and reducing system costs [19].
Methodological considerations
In qualitative research, credibility, dependability, confirmability and transferability are used to describe trustworthiness [25]. Involving a purposeful sample of leaders with various experiences from the healthcare sector, alongside the researchers’ extensive experience in the methodology, facilitated an in-depth analysis and strengthened the credibility. The analysis was intentionally designed to reflect the informants’ responses and reflections to the interview questions. Throughout the process, the researchers did not contest or challenge the informants’ views during the interviews or in the subsequent analysis. This was a deliberate approach, as the primary aim of the study was to capture and describe the leaders’ perspectives based on their knowledge and perceptions of AI, particularly in relation to PCC. By allowing their viewpoints to remain uncontested, we aimed to present a clear and unfiltered representation of their understanding and insights on AI in this context. A limitation for the transferability could be that all participants work in the same county council. Dependability was enhanced by employing an interview guide to ensure consistency across all participants. The interviews were performed either remotely, using the Microsoft Teams application, or face to-face. The variation might be a limitation. However, remote interviewing with videoconferencing services, such as Microsoft Teams, could be beneficial and even preferred [44]. Confirmability was strengthened by incorporating selected quotations from the data to illustrate and enrich the descriptive text within each subcategory.
Conclusions
In conclusion, healthcare leaders perceive that AI applications could contribute to PCC across various healthcare levels, thereby enhancing care quality and patient health outcomes. AI applications are proposed to create prerequisites for PCC by supporting professional competence and trust. Within the care environment, AI holds the potential to enhance patient safety, enable proactive care, offer tailored treatment recommendations and optimise resource allocation. AI applications could also facilitate tailored information, shared decision making and patient self-management in person-centred processes. The expected outcome of AI implementation is to improve care quality and patient health outcomes. Future studies should examine healthcare professionals’ perceptions of how specific AI applications enhance PCC across various clinical settings, emphasising real-world implementation and outcomes. Additionally, research should explore the role of AI in promoting patient engagement and shared decision making, integrating insights from both healthcare providers and patients to identify effective best practices. It is vital to investigate the barriers and facilitators healthcare leaders, professionals, and patients face when adopting AI technologies for PCC. Furthermore, understanding patients’ perspectives on AI-driven interventions will be essential in assessing their impact on patient satisfaction and health outcomes, especially among diverse populations, to ensure inclusivity in care.
Footnotes
Acknowledgements
The authors would like to thank Daniel Tyskbo for conducting interviews and the participants who contributed with their experiences.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: FORTE (grant number: 2022-01357) and the Swedish Research Council for Sport Science (grant number: 2020/3, P2021-0065). The funders of this study are the Swedish Government Innovation Agency Vinnova (grant no. 2019–04526) and the Knowledge Foundation (grant no. 20200208 01H). The funders were not involved in any aspect of study design, collection, analysis, interpretation of data or the writing or publication process.