
Abstract

Hospitals are amazing places. Whether big or small, shiny or otherwise, hospitals provide rapid and urgent access to multi-professional healthcare specialists, diagnostics, treatments and interventions. But hospitals are inherently dangerous places – filled with iatrogenic risks and over-filled with patients, such that they are bursting at the seams. Imagine if we could look after people in their own homes instead? With Hospital at Home (H@H), perhaps we can (see Figure 1).
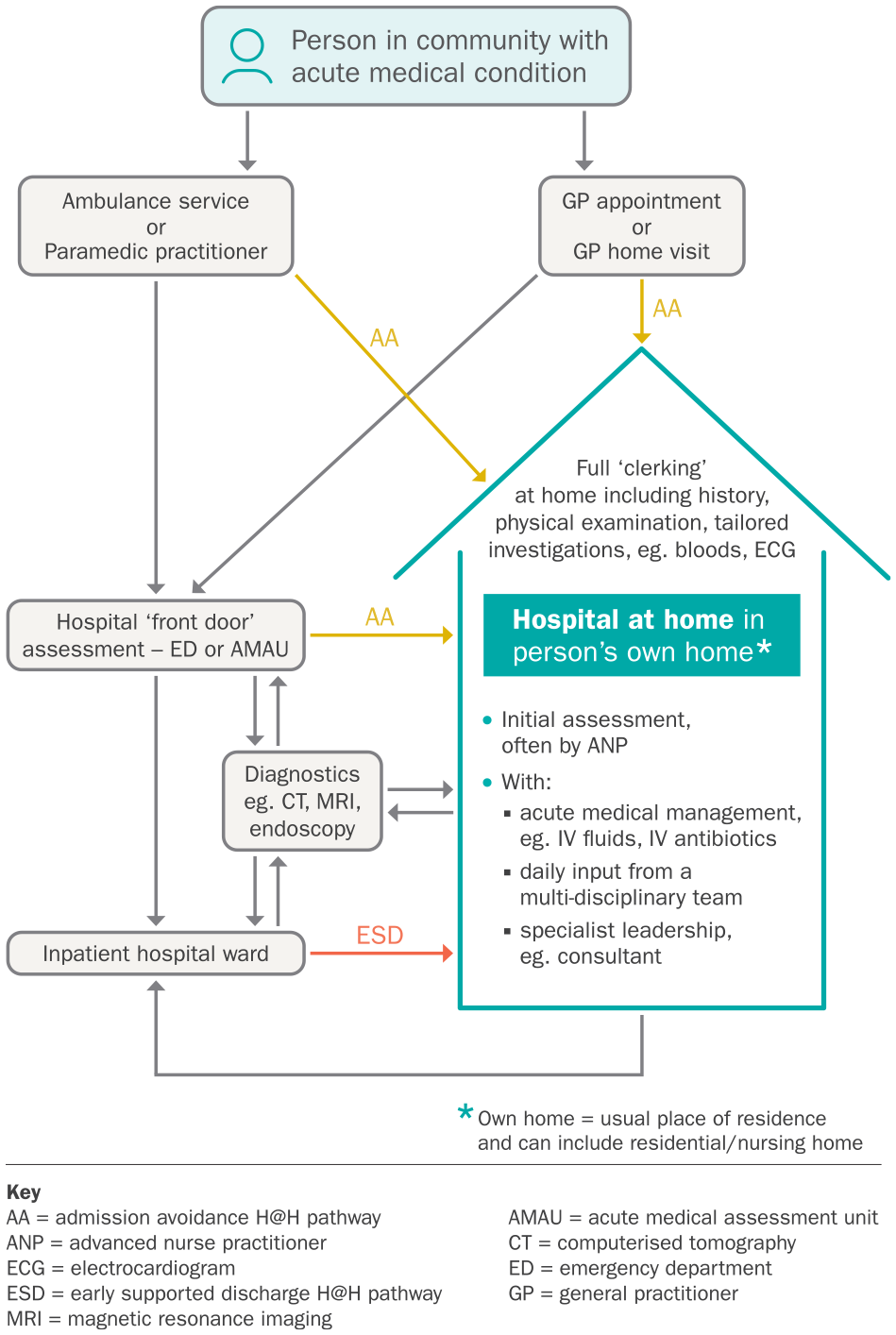
Hospital at home admission pathways.
What is hospital at home?
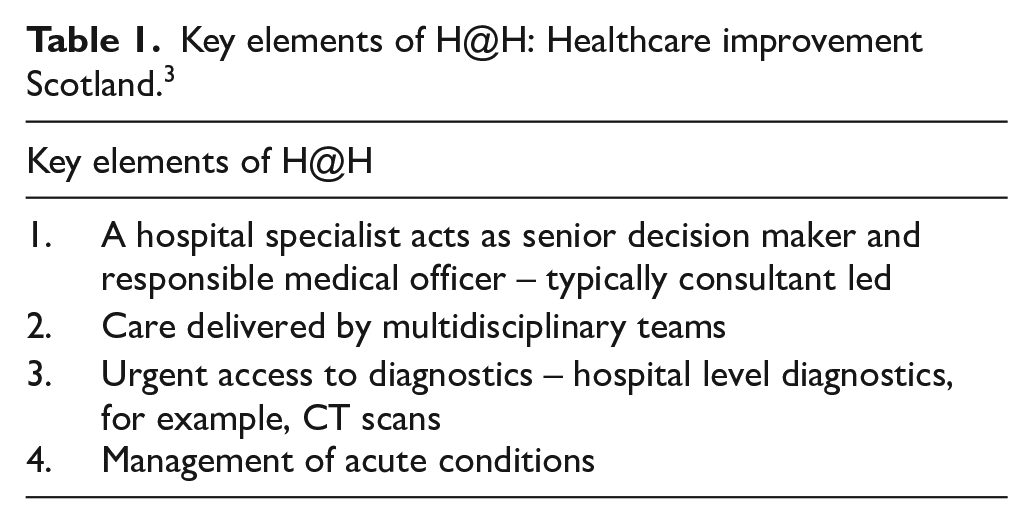
H@H services have been a basic idea in a number of countries for 25 years. 1 The UK H@H society definition states: ‘H@H provides intensive, hospital-level care for acute conditions that would normally require an acute hospital bed, in a patient’s home for a short episode through multidisciplinary healthcare teams.’ 2 Scotland has been developing H@H since 2011. 1 Healthcare Improvement Scotland identifies four defining characteristics of H@H, which distinguish it from other services (see Table 1). 3
Key elements of H@H: Healthcare improvement Scotland. 3
There is heterogeneity between different H@H services.4 –8 Each H@H service has inclusion and exclusion criteria, and a defined target population, for example, paediatric, age >18, age >65; and treats specific conditions, for example, chronic obstructive pulmonary disease (COPD), heart failure, frailty syndromes, mixed medical conditions. H@H teams provide a time limited, short-term intervention equivalent to inpatient hospital care, but services may differ in terms of: 6
- team composition (e.g. lead clinician, nurse practitioners, pharmacists, allied health professionals e.g. physiotherapy, occupational therapy, speech and language therapy, dietician, etc.)
- co-ordination of the team (e.g. hospital-based or community-based)
- programme components (e.g. additional educational programme for patients and carers)
- availability of out-of-hours support
- specific medical home-based interventions (e.g. oxygen, iv fluids, iv therapies)
- number of home visits per day
What hospital at home is not
H@H is not: 8
- community-based management of chronic disease
- outpatient parenteral antimicrobial therapy
- community nursing
- a package of social care
- a hospital prevention programme
- solely virtual care or remote telemonitoring
There was a drive to provide virtual care at home in the context of COVID-19, but H@H is not virtual care. 8 Terminology surrounding virtual wards (particularly in NHS England) is very confusing.9,10 NHS England has guidance for two virtual ward pathways: ‘acute respiratory infection virtual wards’ and ‘frailty virtual wards otherwise known as H@H’. 10 It states that ‘virtual wards should be fully technology-enabled’. 10 Sometimes the terms ‘virtual ward’ and ‘H@H’ are used interchangeably, but they are not the same thing.8,9 This article focuses on H@H, which is more clearly defined, and has a more established evidence base.8,11
H@H is not about avoiding hospital admission – it is a valid and person-centred alternative to hospital admission. 8 Research literature does use the term ‘admission avoidance’. This is to differentiate:
- Admission avoidance (AA): patients who are admitted directly to H@H from the community (e.g. GP referral or ambulance services), or front door services (emergency department or acute medical assessment unit). Also termed ‘step-up’ model of care; from
- Early supported discharge (ESD): patients who have an accelerated discharge from an inpatient hospital ward to H@H, for a condition that would have otherwise required continuation of hospital inpatient care. Also termed ‘step-down’ model of care (See Figure 1).
Evidence base
A recent systematic review has endeavoured to compare AA H@H with ESD H@H, but the quality of evidence is not strong enough to draw firm conclusions. 6 However, the authors made two interesting observations. Firstly, COPD-specific reviews reported low recruitment rates with only 11–39% of patients across trials meeting eligibility criteria for H@H; and 56–88.5% of eligible patients consenting to receive H@H. 6 Secondly, caregiver availability was an eligibility criteria in a third to a half of studies. 6
A 2016 Cochrane review of AA H@H included 1,814 participants from 16 randomised controlled trials (RCTs): three COPD, two stroke, six mixed medical conditions (mainly age > 65), five other medical conditions. 4 Most trials had an average age of 70 to >80. In summary, for the clinical outcomes of mortality and hospital transfer/re-admission, there was no significant difference between AA H@H versus inpatient hospital care. There was variable evidence of the impact of AA H@H on length of stay. AA H@H was associated with a reduced likelihood of living in residential care at 6 months. 4
A 2017 Cochrane review of ESD H@H included 32 RCTs and 4,746 participants. 5 The results were divided into three groups of studies that recruited people:
- recovering from stroke (average age mainly > 70)
- with a mix of medical conditions (mainly age > 65) or with COPD (who also had an average age >65)
- following elective surgery (mainly orthopaedic; also hernia repair, varicose veins, coronary artery bypass graft)
In all three groups, ESD H@H probably makes little or no difference to mortality, although in COPD studies there was insufficient information to determine the effects on mortality. 5 There was insufficient data in the surgical group, but in the other two groups ESD H@H may lower the risk of living in an institutional setting at 6 months. 5
Whilst H@H can potentially provide care to people of any age, why do many H@H services and associated research target older people, particularly those with frailty? Firstly, my personal experience is that older people frequently exert a strong preference for being at home. Secondly, older people living with frailty are at greatest risk of hospital-related harms including functional decline and delirium. 1 It stands to reason that these people have the greatest potential benefit of receiving hospital level care in the comfort of their own homes.
Clinical effectiveness of H@H comprehensive geriatric assessment
In a UK-wide, multisite, RCT with >1,000 participants (mean age 83), Shepperd et al found that AA H@H comprehensive geriatric assessment (CGA) was non-inferior for measures of clinical effectiveness versus hospital care with CGA when available. 7
H@H was non-inferior versus hospital care for the following outcome measures at 6 months:
- Living at home (RR 1.05, 95% CI: 0.95–1.15, p = 0.36)
- Mortality (RR 0.98, 95% CI: 0.65–1.47, p = 0.92)
H@H resulted in better outcomes versus hospital care for the following measures:
- Living in long-term residential at 6 months (RR 0.58, 95% CI: 0.45–0.76; p < 0.001)
- Delirium at 1 month (RR 0.38, 95% CI: 0.19–0.76; p = 0.006)
These outcomes must be interpreted with caution. In the comparator arm, CGA was delivered only when available: 18.6% of the hospital group received specialist care without CGA; and for 7.3% the type of hospital care was not recorded. 7 The baseline prevalence of delirium in all study participants was very low (7%). 7 This suggests gross under-detection, and therefore I would consider the study’s findings regarding delirium to be uninterpretable.
Cost-effectiveness
An accompanying economic evaluation to the above RCT found a cost saving for H@H compared to inpatient care. 12 However, much of the savings focused on social care costs, and took into account the reduced cost of living at home rather than in residential care at 6 months. Elsewhere, it has been suggested that studies overestimate the cost effectiveness of H@H.9,11 Or that results on cost effectiveness are uncertain due to methodological issues.6,11
Typically, in order to make financial savings hospital wards must be closed – but twenty new H@H beds may not save twenty hospital inpatient beds. H@H might be meeting an unmet need, and therefore not reducing the occupancy of inpatient beds.
We must also not forget the cost implications to informal carers and family members in H@H settings. Many studies lack evidence or disregard this area.9,11
Patient satisfaction
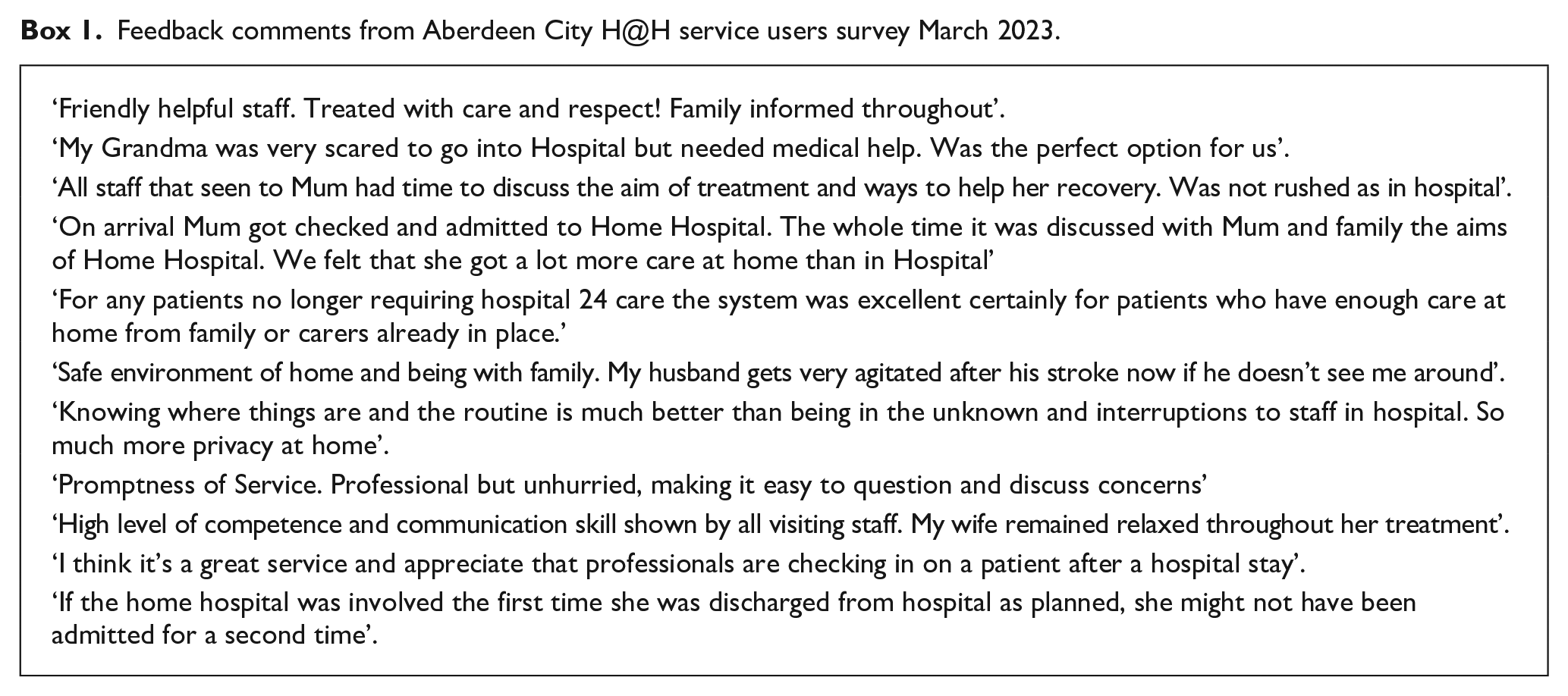
Patient satisfaction of H@H may be higher than inpatient hospital care.4,5,11 Patient testimonies can be hugely positive and powerful (see Box 1). However, some data are from a highly selected patient group who were not ‘blinded’ and therefore we cannot infer that all patients would prefer H@H. 9 From my experience, most patients value H@H and yet others have found the multiple visits from different professionals to be overwhelming and intrusive. If the clinical effectiveness of H@H is equivalent to inpatient care, then patient preference is paramount.
Feedback comments from Aberdeen City H@H service users survey March 2023.
Caregivers
More research is needed about carer experience.4,11 H@H can be associated with increased carer stress, burden, and risk of burnout. 11 Studies highlight a need to involve carers throughout the admission process to H@H, and to mitigate the impact upon them. The decision for H@H ‘admission’, rather than hospital admission, is often taken with staff and patients, with less consideration to the view of families or carers. 11 Carers living separately from the patient have expressed concerns about the lack of ‘round the clock care’ with H@H, citing that H@H is not a substitute for 24 h nursing presence. 13 In addition to emotional and psychological costs, there are potential financial implications for caregivers. 11
Staff, systems and services
Staff involved in H@H delivery generally express high satisfaction. 11 There is, however, a limited supply of staff working throughout health and social care. If H@H services are to be resourced with the necessary specialist staff, then these staff are unavailable to other hospital or community-based services. The NHS has pledged to increase the provision of H@H,1,14,15 but it is difficult to increase the scale of a service when there are finite resources that are already stretched beyond capacity. The financial, staffing and training investment in H@H means a disinvestment in other services.
Personal reflections: Opportunity knocks and opportunity costs
I had the opportunity to work in a H@H service for nearly 3 years from October 2020; splitting my clinical time between H@H and the acute hospital. When I visited people at home, I would regularly receive spontaneous praise from patients and their families about the ‘wonderful’ H@H service (see Box 1). I never receive such delightful feedback during an inpatient ward round! H@H developed my skills in risk management, especially when visiting people who lived alone. I learnt how to close the door behind me, knowing that there was no bedside nurse in my wake. I developed a greater appreciation of colleagues working in primary care. I think that we could all improve our skills by working in a H@H team. But I never felt efficient. I might visit three people at home per day, but in the hospital I could see more than 20.
There is a current drive in H@H to increase efficiency through greater use of remote consultations. 15 But given the nature of the client group, I felt that the biggest value was my face-to-face assessment and conversations. Neither do I believe that further investment in point-of-care testing will facilitate the desired expansion of H@H. In my experience, laboratory blood results were returned sufficiently fast, and ultimately there were more important factors when discussing the place of care and desired interventions.
The inclusion and exclusion criteria of H@H services means that H@H cannot replace the unselected medical take. In the RCT by Shepperd et al, participants were excluded if they were ‘considered by the clinical staff to be at too high risk for home-based care’, including having an unsafe home environment, for example, ‘one in which a delirious patient was at risk from falling, the house stairs were too steep or lacked a handrail’. 7 I believe that we should challenge classical H@H exclusion criteria. For example, I have effectively looked after a number of people with an acute stroke in H@H, despite acute stroke being a common exclusion criteria of H@H services.7,16 I have also looked after countless people at home with delirium and a high risk of falls – after all, their risk of falling would be even higher in hospital! If a patient really wants to be at home, then we can have important, individualised conversations about the pros and cons.
H@H provides a safe and effective, person-centred, alternative to acute hospital admission for people who want to be at home. If people wish to be in hospital, or if their families think they should be admitted to hospital, then H@H doesn’t work. H@H services are not an excuse to deny people access to hospital based care when needed. H@H has been moving healthcare in a positive, person-centred direction, albeit with opportunity costs. If I were a patient, I’d much rather receive hospital level care at home. But will H@H save the NHS? In a word. . . No.