
Abstract
The “Goldilocks Zone”, a term borrowed from astrophysics, describes the optimal range where conditions are just right to support life. In healthcare, this metaphor captures the imperative to balance underuse and overuse of medical services, ensuring care is neither excessive nor insufficient but instead maximally effective, equitable, and sustainable. As health systems confront rising costs, workforce constraints, and growing demands for person-centred care, the search for this balance has become increasingly urgent. This review explores how the concept of the Goldilocks Zone can be operationalized in modern healthcare systems. We examine two core dimensions that define this balance: person-centredness and operational efficiency. Person-centredness requires attention to accessibility, patient satisfaction, and equity. Drawing on global data, we explore how barriers such as cost, geography, and social inequality limit access to care, and we highlight the role of robust primary care systems and tailored wait-time benchmarks in ensuring responsive, equitable delivery. At the same time, we caution against the misuse of performance metrics that may obscure real disparities. Operational efficiency is evaluated across the continuum of screening, diagnosis, and care management. We review frameworks such as Wilson and Jungner’s screening principles and their modern adaptations, as well as diagnostic threshold models and strategies to reduce inappropriate care utilization. Key indicators, including avoidable hospitalizations and ambulatory care-sensitive condition rates, offer insight into system inefficiencies and opportunities for reform. We propose a practical framework for identifying whether a healthcare system is within the Goldilocks Zone and recommend policy levers to help maintain or widen this zone. Ultimately, the Goldilocks Zone is not a fixed destination but a dynamic and evolving balance that requires continual adaptation. As healthcare systems grow more complex, the value of this metaphor lies in guiding both conceptual thinking and concrete policy design.
Keywords
Introduction
The “Goldilocks Zone”, a concept borrowed from astrophysics, describes the optimal range of conditions that can sustain life, being neither too hot nor too cold. In healthcare, this metaphor has been adapted to represent a balanced space where medical interventions are neither excessive nor insufficient, and health policies deliver maximum value to patients. 1 This aligns with the ongoing shift from volume-driven, fee-for-service models to high-value, cost-conscious care that emphasizes meaningful outcomes and addresses individual patient priorities.
Ziebland et al 1 first introduced the idea of a healthcare Goldilocks Zone in their 2019 essay, highlighting the dilemma individuals face in deciding when it is “just right” to seek medical care. They argued for a truly person-centred system—one that is responsive when people choose to consult and provides a safety net for those with potentially serious but undiagnosed symptoms. 1 This metaphor resonated widely but lacked operational clarity: how can health systems achieve this balance in practice, especially in today’s complex and resource-constrained environments?
In the aftermath of the Coronavirus Disease 2019 (COVID-19) pandemic and amidst escalating healthcare costs, workforce shortages, and widening health inequities, 2 the question of how to achieve this delicate balance has become even more urgent. Health systems today face unprecedented pressures to do more with less while ensuring care remains accessible, equitable, and patient-focused. While Ziebland et al 1 offered a compelling patient-level metaphor, their essay lacked specific system-level metrics or policy guidance to support operationalization. We noted that their focus was on illustrating the dilemma of patients navigating between too much and too little care, whereas our review extends this by proposing a framework of measurable indicators and relevant policy considerations. In this review, we revisit the Goldilocks Zone concept through a contemporary and pragmatic lens, exploring how health systems can translate it into practice by integrating person-centredness with operational efficiency, using actionable metrics to balance accessibility, responsiveness, equity, and resource utilization.
We argue that two core pillars—person-centredness and operational efficiency—must anchor this effort. Person-centredness ensures that care is relevant and acceptable to individuals, while operational efficiency ensures that care is delivered sustainably, without waste or inequity. When balanced effectively, they delineate a zone where care is not only clinically appropriate but also meaningful to those receiving it.
This review explores each of these dimensions in turn, offering international examples, evaluative metrics, and policy implications to guide health systems toward the elusive but essential Goldilocks Zone.
Methods
This article is intended to be a narrative review, designed to advance the conceptual and operational understanding of the “Goldilocks Zone” in healthcare. While not a systematic review, we adopted a methodical approach to identify relevant literature and policy documents. Two authors (HYKL and CEY) conducted exploratory searches across three main databases: PubMed, Scopus, and Google Scholar, for relevant documents published up to end April 2025. The following search terms and Boolean operators were used in various combinations: “Goldilocks Zone”, “healthcare utilization”, “health system performance”, “person-centred care”, “health equity”, and “access to care”. We included English-language publications such as empirical studies, narrative reviews, conceptual papers, and major policy reports that discussed the balance between healthcare over- or under-use, health system optimization, or metrics related to equity, access, efficiency, or person-centredness. The final selection of sources was guided by relevance to the two core pillars of the Goldilocks Zone, person-centredness and operational efficiency, as well as illustrative value across diverse health system contexts, to ensure conceptual continuity and policy applicability. All authors reviewed the selected literature and contributed to interpreting key themes, frameworks, and examples. In particular, the broader author team (JCHY, KXZ, IKSN and QXN) guided the conceptual framing, critically assessed how the findings aligned with real-world policy applications, and helped refine the synthesis, bringing disciplinary expertise from health systems and policy, surgery, clinical medicine, and public health, respectively. This review does not aim to be exhaustive or provide the depth of a full assessment but seeks to synthesize key themes and frameworks that are most relevant to operationalizing the Goldilocks Zone across healthcare systems.
Person-Centredness of the Goldilocks Zone
At the heart of the Goldilocks Zone in healthcare lies the principle of person-centredness—the idea that care should be tailored to the unique needs, values, and preferences of each individual. 3 Person-centred care refers to a healthcare approach that respects and responds to individual patient preferences, needs, and values, ensuring that these guide all clinical decisions. 4 This model reorients the role of patients from passive recipients to active partners in their care, and healthcare professionals from directive authorities to collaborators and facilitators. 4 We avoid using the narrower term patient-centredness here, which some authors differentiate as a more clinical or provider-focused construct, while person-centredness is broader and system-oriented. There are undoubtedly variations in how person-centredness is conceptualized and operationalized across health systems and research groups, and these perspectives help contextualize differences in application.5,6 For care to truly fall within the “just right” zone, it must be both contextually relevant to the individual and equitably delivered across populations. While this concept is widely endorsed, operationalizing it remains a challenge. We propose that a truly person-centred healthcare system must balance three critical dimensions: accessibility, patient satisfaction, and equity. Together, these factors determine whether individuals experience care that is “just right”—not only in its timing and delivery but also in its capacity to meet personal and societal expectations.
Nevertheless, the perception and delivery of quality care are deeply embedded in social context, with quality itself often understood as a socially constructed concept, co-produced by individuals, families, communities, and healthcare providers. 7 In some countries, quality is closely tied to advanced technologies and specialist access, whereas in others, it is measured by continuity of care, trust in providers, and responsiveness to individual needs. These differences shape what patients expect from the health system and how care is “produced”, which means that metrics such as utilization or satisfaction must be interpreted cautiously and in light of local expectations and values.
Accessibility ensures that people can meaningfully engage with the healthcare system, both financially and logistically. Although unmet healthcare needs are low on average in countries of the Organization for Economic Cooperation and Development (OECD), significant disparities persist based on a 2023 OECD report. 8 For instance, in OECD countries with lower GDP per capita such as Estonia and Greece, 8.1% and 6.4% of the population respectively reported unmet care needs, compared to under 0.5% in higher-income countries like Germany and the Netherlands. 8 Within countries, lower-income groups often face greater barriers to access. In Latvia, individuals in the lowest income quintile were five times more likely to report unmet medical needs (8.5%) compared to those in the highest income quintile (1.7%). 8 Even in high-income nations such as the United States, 36% of adults delayed or skipped necessary care in the past 12 months due to cost, based on survey data in May 2025.9,10 Beyond financial constraints, logistical barriers including inadequate transport infrastructure and rural-urban healthcare disparities also limit access. A study by Hailu et al 11 found that pregnant women residing in rural areas had more than a tenfold increase in the odds of delivering at home compared to their urban counterparts. Patterns of delayed or skipped care are often shaped by the underlying healthcare financing model. In insurance-based systems with limited reimbursement or high deductibles, out-of-pocket payments can present a direct financial barrier. 11 However, even in tax-funded systems with broad coverage, indirect costs such as transportation, time away from work, or childcare responsibilities can deter timely access, and long waiting lists may further delay care despite low point-of-care costs. Consequently, financial protection must be considered beyond formal coverage alone, and interventions should be tailored to the unique barriers imposed by each system’s funding structure.
Patient satisfaction reflects how well the healthcare system responds to individual needs, particularly through timely and appropriate care. Excessive wait times may indicate system inefficiency, while extremely short wait times could suggest overcapacity and resource misallocation. Many health systems have established benchmarks for wait times, such as the NHS Constitution’s 4-hour target for emergency department (ED) visits. 12 Non-urgent waits, such as for elective surgeries, vary widely; OECD data show that median wait times for routine cataract surgery are under 40 days in Italy and Denmark but exceed 180 days in Estonia and Poland. 13 While benchmarks are useful, policymakers should also consider what patients perceive as socially and medically acceptable wait times. Some systems have introduced disease-specific targets, such as the United Kingdom (UK)’s Faster Diagnosis Standard, which mandates that patients with suspected cancer receive a diagnosis within 28 days of referral. 14 Responsiveness further requires robust primary care networks that triage patients effectively, reducing avoidable ED visits and preventable hospital admissions.
Finally, equity is critical to ensuring that person-centred care benefits all segments of society, regardless of socioeconomic status, education level, geography, or ethnicity. Even in countries with universal healthcare coverage, significant pro-rich inequities in healthcare utilization persist, with wealthier individuals often accessing specialists more frequently relative to their health needs. 15 Such disparities have been documented globally, across both high- and low-income countries.16-18 Policymakers should employ robust equity measures, including the concentration index 19 and utilization ratios stratified by income quintiles. 20 However, they must also remain mindful of Goodhart’s Law—that when a measure becomes a target, it may cease to be a good measure. 21 Overemphasis on meeting numerical targets can lead to unintended consequences, such as artificially limiting specialist visits among higher-income groups without addressing underlying structural inequities. To advance equity, some countries have introduced universal healthcare schemes (eg, the UK’s National Health Service), 22 while others have developed targeted programs such as Thailand’s 30-baht health scheme 23 and Brazil’s community health worker initiatives. 24 Widening the Goldilocks Zone will require a dynamic balance between societal priorities, economic constraints, and political will.
While accessibility, satisfaction, and equity are core pillars of person-centredness, they can also serve as indirect signals of potential overuse or underuse within the system. For instance, extremely short wait times, particularly for non-urgent procedures, may reflect excess capacity or even unnecessary care, whereas persistently high levels of unmet need suggest underprovision. Importantly, healthcare utilization is not a perfect proxy for health need; patients with similar clinical conditions often receive vastly different amounts of care, reflecting variations in social norms, resource availability, and systemic incentives rather than differences in underlying health status. 25
Operational Efficiency of the Goldilocks Zone
Beyond person-centredness, operational efficiency is a critical dimension of a healthcare system operating within the Goldilocks Zone. This involves optimizing resources across key stages of care—screening, diagnosis, and management—while ensuring that services remain both clinically appropriate and economically sustainable.
Population screening programs must strike a delicate balance between early disease detection and the risk of overdiagnosis. Overly aggressive screening policies can strain health systems, generate unnecessary follow-up investigations, and expose patients to psychological and financial burdens. 26 Conversely, under-screening leads to missed opportunities for prevention and early intervention, disproportionately affecting vulnerable populations.
Foundational screening principles outlined by Wilson and Jungner in 1965 27 (Table 1) remain influential but are increasingly seen as insufficient in addressing modern challenges of resource distribution and health inequities.
Summary of Wilson and Jungner’s Principles. 27 .

In addition to person-centredness, we argue that a healthcare system in the Goldilocks zone is marked by its operational efficiency with appropriate resource utilization. This will be analyzed at three main stages of healthcare delivery: screening, diagnosis, and management. These principles focused on the health problem’s importance, the screening tool’s performance, and the evidence for treatment efficacy.
While Wilson and Jungner’s 27 principles provide a foundational framework for evaluating screening programs, they fall short in addressing the complex realities of modern health systems. These include unequal access, variable implementation fidelity, and the dynamic allocation of limited resources. For example, principles 7 and 8 state that there should be an accepted treatment for patients with recognized disease and facilities for diagnosis and treatment should be available. However, they fail to consider patients’ varied access to healthcare settings and how reliably the healthcare systems can deliver indicated care. 28 Using a more concrete example, modern genomic screening for predisposition to complex diseases challenges the classical criteria, as the risk information is often probabilistic, and no definitive intervention may be available, which also contravenes the principle that there must be an accepted treatment for the condition identified. Similarly, AI-enabled screening tools, such as those used in diabetic retinopathy, continuously evolve based on new data inputs, which undermines the criterion of a stable and validated screening test. Recognizing these gaps, recent efforts, such as those by Dobrow et al, 29 have sought to consolidate and modernize screening principles to reflect contemporary challenges in effectiveness, efficiency, and equity.
Dobrow et al 29 conducted a comprehensive review and consensus process to modernize screening principles, identifying 12 consolidated principles across three domains: disease/condition, test/intervention, and program/system. These principles provide a practical framework for designing screening programs that balance effectiveness, efficiency, and equity, which are hallmarks of the Goldilocks Zone.
At the disease level, screening should target well-defined, significant health conditions with an adequately understood natural history and a detectable preclinical phase. Target populations must be clearly defined and reachable to ensure equitable access.
For screening tests and interventions, programs should ensure that tests are accurate, reliable, acceptable to the population, and feasible to administer safely and cost-effectively. There must be clear protocols for follow-up actions when tests yield positive results, with accessible and effective pathways for diagnosis, treatment, and ongoing care.
At the programmatic level, successful screening initiatives require adequate infrastructure and integration with broader health systems to ensure continuity of care. Ethical considerations must guide program design, including informed choice and protection of participants’ rights. Programs should also undergo rigorous evaluation to assess benefits and harms, supported by high-quality evidence and regular economic evaluations to justify continued investment.
Policy implications include establishing dedicated national screening committees, like the UK National Screening Committee, to review and update guidelines regularly, 30 ensuring that screening remains aligned with health system priorities and resource availability. Such governance structures help prevent resource waste, mitigate health inequities, and promote population-level health gains.
Healthcare funding models shape not only how services are delivered but also how they are accessed and valued. In fee-for-service systems, financial incentives often align with volume, potentially encouraging overutilization of diagnostic tests and procedures. 31 In contrast, capitated or budget-based models may promote restraint but risk under-provision. Beyond system-level payment structures, patient-facing fee arrangements such as copayments, coinsurance, and deductibles influence healthcare-seeking behaviour. 32 While low point-of-care costs can increase demand, this effect is not unique to tax-funded systems, and many Beveridge-style systems actually report lower per-capita utilization than neighbouring Bismarck-type systems. 33 Such systems also deploy non-price mechanisms including gatekeeping and waiting lists to moderate service use. Policymakers must therefore calibrate these different levers to encourage high-value care while minimizing both financial barriers and equity harms.
At the diagnostic level, decision thresholds are critical in mitigating subjective and varied judgements across medical professionals in medical decision-making. Policies should support the development of national or regional clinical pathways that embed diagnostic thresholds informed by both evidence and economic considerations. While the Pauker and Kassirer 34 threshold model provides a conceptual framework for diagnostic decision-making, real-world policies must also address the cognitive biases and systemic factors that drive overdiagnosis and underdiagnosis. 35
Policy measures such as value-based payment models and diagnostic stewardship programs can incentivize appropriate test utilization. For instance, pay-for-performance schemes tied to the avoidance of low-value tests have shown promise in curbing unnecessary investigations. 31 Additionally, integrating decision-support tools into electronic health records can standardize diagnostic thresholds and reduce unwarranted practice variation.
Inappropriate healthcare utilization, particularly avoidable ED visits and hospital admissions, remains a significant source of system inefficiency. In 2011, it was estimated that more than 20% of healthcare expenditure in the United States was wasted, and this was attributed to overtreatment, failures of care coordination, failures in execution of care processes, administrative complexity, pricing failures, and fraud and abuse. 36 All of these categories of waste provide opportunities for improvement in resource utilization. A significant proportion of these inappropriate visits are ambulatory care-sensitive conditions (ACSCs), defined as health issues where timely and effective outpatient care, typically in primary healthcare, can potentially prevent hospitalizations or reduce their severity. In a hospital at the East Midlands of England, a 5% increase in patient reports of being able to consult a primary doctor resulted in a corresponding 3.5% decrease in emergency admissions. 37 The same cross-sectional study from a specific region in England also recorded reduced admissions for diabetes following the provision of specialist diabetes services in primary care, whilst higher admission rates for asthma were associated with smaller general practice sizes. 37 Similar trends were observed in Mexico after interventions for acute and chronic conditions were improved in their primary care over 2010 to 2017, resulting in a decrease in avoidable hospitalizations for ACSCs from 13% to 10.7%. 38 Strong primary care networks can be used to triage patients appropriately and prevent excess patient load at the secondary/hospital level. A healthcare system operating within the Goldilocks Zone should prioritize strengthening primary care services to act as the first point of contact and effectively manage chronic conditions before they escalate.
Policy options to improve care management include expanding gatekeeping mechanisms in primary care, as seen in France’s médecin traitant system, which successfully reduced unnecessary specialist consultations; 39 implementing financial incentives to encourage timely primary care visits and chronic disease management, thereby reducing preventable hospitalizations; and enhancing community-based care and transitional care models to improve post-discharge outcomes and reduce readmissions. Finally, policymakers should institutionalize the routine monitoring of ACSC admission rates and avoidable ED visits as performance indicators of primary care effectiveness. Such metrics offer actionable insights into system bottlenecks and can inform resource reallocation toward preventive and community-based services.
As aforementioned, the way healthcare is funded strongly influences how services are accessed and used. In tax-funded systems with minimal point-of-care costs, patients may overuse services unless guided by gatekeeping mechanisms. In contrast, high out-of-pocket systems can deter needed care, contributing to underuse. Fee-for-service models may incentivize overprovision of services, while capitation or bundled payment schemes promote more prudent resource use. These differences in financing structures can push health systems out of their Goldilocks Zone, either toward inefficiency or inequity.
Together, these three domains (screening, diagnosis, and management) form the operational backbone of a system that seeks to operate within the Goldilocks Zone. Efficiency is not about doing less, but about doing what matters most, for those who need it most, in a timely and sustainable manner.
Metrics and Governance for Maintaining the Goldilocks Zone
Translating the Goldilocks Zone from a conceptual metaphor into a functioning policy framework requires robust metrics and sound governance. Without clear indicators and accountability structures, efforts to achieve the “just right” balance in healthcare risk becoming vague aspirations rather than actionable strategies.
Metrics are essential for assessing whether a healthcare system is delivering value—defined not just in economic terms but in health outcomes, equity, and user experience.40,41 To reflect the dual priorities of person-centredness and operational efficiency, health systems need a dashboard of indicators that track performance across multiple domains. For instance, metrics that weigh cost against health benefit such as QALYs, can help decision-makers prioritize interventions that offer the best value for money, while monitoring administrative overhead helps identify non-clinical inefficiencies. Recent consensus-building efforts, such as a Delphi study on centredness, 42 and related work developing quality indicators for person-centred health systems, further clarify how measurement can align with values of responsiveness, equity, and engagement. These strengthen the case for multidimensional monitoring.
We present a set of illustrative metrics to evaluate person-centredness, drawn from existing practices in health system performance monitoring. These are not intended to be exhaustive but to offer a starting point for operationalizing the Goldilocks Zone concept. For person-centredness, relevant metrics include:
Continuity of care (eg, proportion of patients with a consistent primary care provider or named care coordinator);
Proportion of the population reporting unmet healthcare needs, stratified by income, ethnicity, and geography;
Use of shared decision-making tools in routine care;
Population health literacy levels (eg, via validated instruments like the Health Literacy Questionnaire);
Patient-reported outcome measures (PROMs) and patient-reported experience measures (PREMs) to capture satisfaction and perceived quality;
Respect and dignity (eg, being treated with compassion, derived from validated patient experience surveys); and
Concentration indices and utilization ratios to detect pro-rich or pro-urban biases in service use.
For operational efficiency, systems should monitor:
Rates of avoidable hospitalizations and emergency department visits for ambulatory care-sensitive conditions;
Cost per quality-adjusted life year (QALY) gained, particularly for high-cost or discretionary interventions.
Relative administrative overhead as a proportion of total health expenditure.
Use of cost-effectiveness thresholds in coverage or reimbursement decisions;
Utilization of low-value diagnostic tests and procedures; and
Compliance with evidence-based clinical pathways and time-to-treatment benchmarks.
Additional metrics can and should be incorporated based on local priorities, health system maturity, and patient expectations. As Goodhart’s Law warns, overly rigid adherence to targets can distort provider behaviour and undermine care quality. 21 To support policymakers and health system leaders in assessing and navigating their position within the Goldilocks Zone, Table 2 provides a simplified framework of key domains, evaluative metrics, and policy recommendations. This synthesis draws directly from the themes discussed in earlier sections—person-centredness and operational efficiency—and offers a practical guide for system calibration. These dimensions, while distinct, are interdependent.
The Goldilocks Zone in Healthcare, with Examples of Illustrative Metrics and Policy Recommendations.
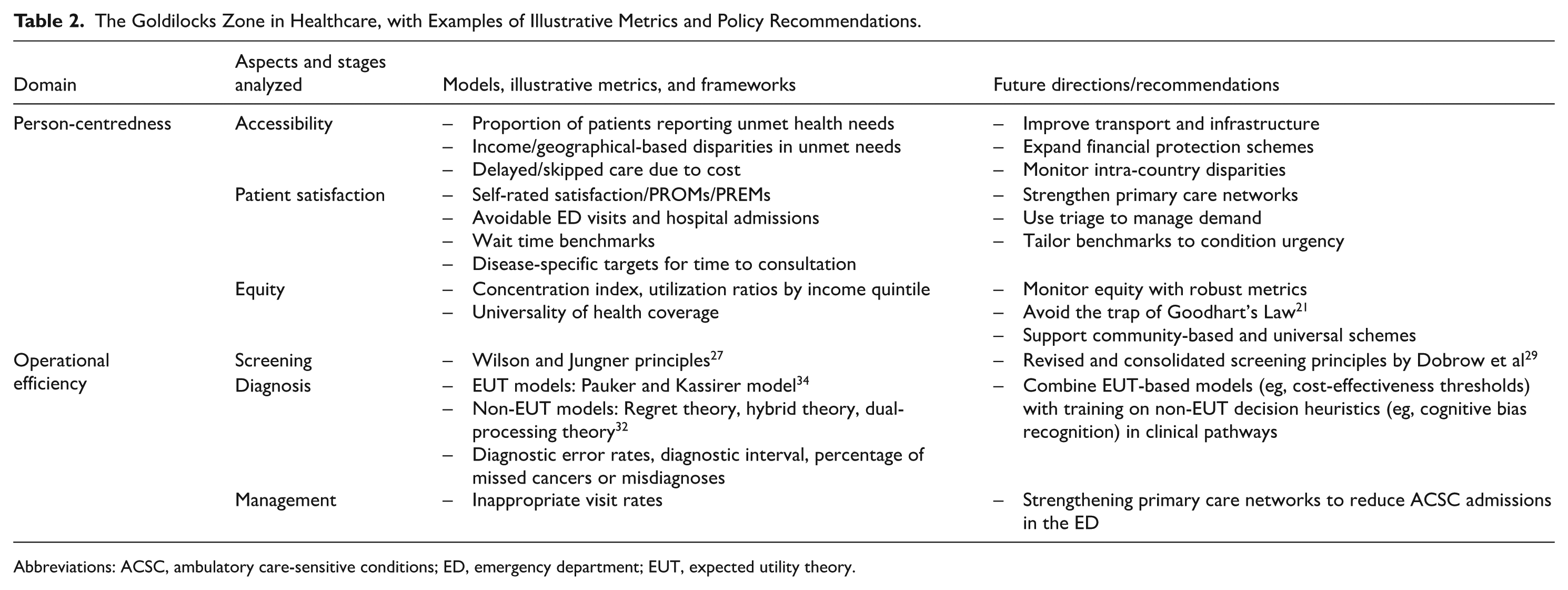
Abbreviations: ACSC, ambulatory care-sensitive conditions; ED, emergency department; EUT, expected utility theory.
Each domain is matched with specific stages of care (eg, screening, diagnosis, management) and measurable indicators that can serve both as diagnostic tools (to identify system misalignments) and intervention targets (to guide reform). For instance, within the domain of accessibility, Table 2 highlights the use of metrics such as unmet healthcare need proportions, stratified by income or geography. These can help flag systemic inequities or logistical gaps in service reach.
In terms of equity, Table 2 references tools such as the concentration index and utilization ratios by income quintile, which are essential for evaluating whether service distribution reflects underlying health needs or reinforces existing disparities. Recognizing the pitfalls of Goodhart’s Law, 21 the table recommends using these metrics as performance signals, complemented by qualitative insights and equity audits rather than strict targets.
The operational efficiency column aligns each stage of care with relevant theoretical or policy frameworks, for example, the Wilson and Jungner criteria 27 and the updated Dobrow et al 29 screening principles are referenced under the screening domain. For diagnosis, the table incorporates both expected utility theory (EUT) and non-EUT models, acknowledging the complexity of clinical decision-making in real-world practice. Improving diagnostic appropriateness may benefit from combining EUT-based cost-effectiveness thresholds with insights from behavioural science. For instance, clinical decision support systems can be embedded with local cost-effectiveness thresholds to guide test ordering, while clinicians receive training on common diagnostic heuristics and biases, such as premature closure or anchoring, that may contribute to over- or under-investigation. This dual approach bridges normative and descriptive models of decision-making and can reduce both unnecessary testing and missed diagnoses. For care management, indicators like ACSC admission rates and avoidable ED visits serve as system-level barometers of primary care effectiveness. 43
Nonetheless, the adoption of these metrics should be tailored to local data infrastructure and evaluated for measurement validity and relevance, using criteria such as those proposed by Bojke et al. 44 We acknowledge the importance of using a structured framework for selecting quality indicators. While the proposed evaluative metrics offer conceptual alignment with the focus domains of person-centredness and operational efficiency, their feasibility varies considerably across health systems. For example, the use of PROMs and PREMs in routine practice faces challenges, resulting in a paucity or limited application of these measures. 45 In many countries, they are collected for only a limited range of procedures and are not routinely used in community or primary care settings. Continuity of care measures often require longitudinal data linkages that may not be readily available. Meanwhile, some metrics such as avoidable hospitalizations or emergency visits are more widely implemented but remain sensitive to case-mix adjustment and reporting timeliness.
Implications and Future Work
Our proposed Goldilocks Zone model complements but is conceptually distinct from comprehensive frameworks such as the World Health Organization (WHO)’s 2022 Health System Performance Assessment: A Framework for Policy Analysis (HSPA). 42 While the HSPA framework clearly delineates system-level functions (eg, governance, financing, resource generation) and links them to broad health system goals, the Goldilocks Zone, as described here, offers a translational lens to assess whether care delivery is proportionate, neither excessive nor insufficient. The Goldilocks Zone model operationalizes two composite dimensions (person-centredness and operational efficiency) as dual dimensions through which service delivery is evaluated. This differs from the HSPA’s broader systems-level view by bringing a more micro-level orientation, especially relevant for primary care design, triage systems and care coordination. It also focuses specifically on calibrating health system responses to achieve “just right” care, especially in resource allocation and patient flow, rather than merely assessing function performance. HSPA provides a structural blueprint for system performance assessment while the Goldilocks Zone helps health systems interrogate overuse and underuse at the service and patient interface, using existing indicators such as access gaps, inappropriate admissions, or screening intensity. It may be especially useful as an investigative tool in guiding triage system reform, service integration efforts, or resource allocation decisions that seek to refine the balance between healthcare quality, equity and sustainability.
Importantly, the framework and metrics outlined in Table 2 offer a structured menu of options that health systems can adapt based on their context, capacity, and priorities. The framework is intended as a heuristic tool—a scaffold for policy discussion and further adaptation, rather than a prescriptive or exhaustive model—as it does not fully capture the complexity and contextual variation inherent in health systems. By making explicit the connections between policy levers, performance metrics, and desired outcomes, the table serves as a bridge between theory and implementation.
Achieving the Goldilocks Zone in healthcare requires more than the passive tracking of metrics, it calls for deliberate and responsive policy action that can translate measurement into meaningful improvement. While metrics help identify deviations from optimal care, it is policy that determines whether and how health systems respond. The policy levers outlined in Table 2 are guided by several key considerations.
First, incentives must be aligned to support value-based care. Payment models play a critical role in shaping provider behaviour, and blended approaches such as combining capitation with performance-based bonuses can promote continuity, equitable access, and appropriate resource use.
Second, health systems must invest in robust data infrastructure. Interoperable electronic health records and linked administrative datasets are essential to enable the tracking of metrics such as care continuity, avoidable hospitalizations, and patient-reported outcomes.
Third, capacity for patient engagement should be strengthened. Empowering individuals through improved health literacy, activation and shared decision-making requires not only the availability of tools like decision aids, but also cultural change within clinical environments that supports partnership in care. Fourth, structural determinants must be addressed. Reducing pro-rich or pro-urban biases requires policy interventions at the system level, including proactive geographic service planning and community-based outreach strategies.
Finally, systems should embed continuous evaluation through audit and feedback cycles. Using timely data on healthcare utilization, outcomes, and patient experiences allows health systems to iteratively refine resource allocation and care pathways. Together, these policy strategies help operationalize the Goldilocks Zone by aligning system structures with the goal of delivering care that is neither too much nor too little, but just right.
Governance also encompasses community and patient involvement in system design. Co-production approaches, where service users are involved in planning, evaluating, and refining healthcare services, have been shown to improve both legitimacy and effectiveness. Ensuring that marginalized voices are included, such as ethnic minorities, rural residents, and those with disabilities, is essential to avoiding narrow definitions of what constitutes “just right”.
No system remains in the Goldilocks Zone by chance or permanence. Healthcare is dynamic, shaped by demographic changes, emerging diseases, shifting technologies, and political cycles. Thus, staying in the Zone requires adaptive learning. At the same time, while the Goldilocks Zone offers a helpful conceptual lens for evaluating balance in healthcare delivery, it is not without criticism. A rigid pursuit of “just right” utilization may inadvertently lead to overly prescriptive pathways that do not accommodate clinical complexity or patient variability. Innovation could also be constrained if systems are penalized for deviating from defined thresholds, even when such deviations are contextually appropriate. Therefore, application of the framework should emphasize flexibility, person-centredness, and continuous learning, rather than rigid benchmarking.
Limitations of Review
This review was intentionally designed as a conceptual narrative synthesis to invite discourse on how health systems might operationalize the “Goldilocks Zone” between underuse and overuse. However, this approach entails several important limitations. First, the review did not follow a formal systematic methodology. While we drew from a wide range of published literature, we did not conduct a systematic review based on established methodologies. This limits the transparency and reproducibility of our review process and may introduce selection bias, particularly in terms of which frameworks, metrics, and examples were highlighted. Second, the selection of evaluative metrics and policy levers was not guided by a formal consensus process. The proposed domains and measures may not fully reflect the lived experiences, cultural contexts, or operational realities across different healthcare settings. Last but not least, the feasibility of implementing certain metrics (eg, PROMs or continuity of care indicators) varies widely across countries and care levels, especially in low-resource settings. While we acknowledge these challenges, a more detailed feasibility assessment, drawing from health informatics, implementation science, and system readiness frameworks, was beyond the scope of this paper.
Future work should build on this foundation by engaging in structured consensus-building methods, such as Delphi panels, co-design workshops, and participatory policy dialogues, to refine and validate the framework. Additionally, empirical studies that test the framework’s application in real-world health system evaluations would help assess its utility, adaptability, and impact.
Conclusions
The concept of the Goldilocks Zone in healthcare offers a compelling metaphor—but more importantly, a practical heuristic—for guiding health services research and policymaking. In an era marked by rising costs, evolving novel technologies, demographic shifts and mounting pressures for accountability, the challenge is no longer just about delivering more care, but delivering the right care to the right people at the right time, using the right amount of resources. This review has explored how the Goldilocks Zone can be operationalized through two key pillars: person-centredness and operational efficiency. We have examined empirical data and conceptual frameworks that enable health systems to assess accessibility, responsiveness, equity, and resource utilization across the care continuum from screening to diagnosis to long-term management. For the field of health services research, the Goldilocks Zone provides a valuable integrative lens, one that links normative ideals (such as equity and person-centredness) with systems-level metrics and performance management. It invites researchers to go beyond siloed evaluations of cost, quality, or access, and to consider how these dimensions interact dynamically in complex health ecosystems. Moreover, it opens up opportunities for implementation research, particularly in understanding how governance structures, performance feedback loops, and frontline innovations can be harnessed to maintain this balance over time. For policy and practice, the Goldilocks Zone encourages an adaptive, learning-oriented approach to system design, one that recognizes variation in population needs, avoids over-reliance on blunt targets, and builds resilience into care delivery. Tools such as the concentration index, avoidable hospitalization rates, patient-reported outcomes, and updated screening principles can help track whether systems are moving closer to or further from this optimal zone.
Additionally, maintaining a health system within the Goldilocks Zone is not a one-time achievement but a continuous process requiring regular recalibration, evidence-informed decision-making, and sustained investment in primary care, equity, and community-based delivery models. As healthcare practitioners and health services and systems researchers seek to advance scholarly discourse and practical innovation in service delivery and system performance, this framework provides both a diagnostic tool and a strategic compass. Future research should explore how this model can be applied in specific contexts (across low-, middle-, and high-income countries) and how real-time data systems and participatory governance can help make the Goldilocks Zone not only a guiding metaphor but a measurable reality.
Footnotes
Author Contributions
QXN and IKSN: Conceptualization and design; HYKL, CEY, JCHY, KXZ, IKSN, and QXN: Analysis and interpretation of data; HYKL, CEY, IKSN, and QXN: Writing—original draft; HYKL, CEY, JCHY, KXZ, IKSN, and QXN: Writing—review and editing; JCHY and QXN: Supervision. All authors read and approved the final manuscript. The authors alone are responsible for the content and writing of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.