
Abstract
In contrast to leisure time physical activity, occupational physical activity may have adverse health effects—a phenomenon known as the “Physical activity paradox”. Characteristics such as long duration, low intensity, static and restricted movement, body position and insufficient recovery are possible explanations as to why physical activity in the occupational context may “wear one out” rather than provide health benefits. We emphasise the role of low cardiorespiratory fitness as a potential contributor to the physical activity paradox, and present data suggesting that only 25% to 50% of Swedish workers in occupations with higher aerobic demands may have “sufficient” cardiorespiratory fitness to maintain good health during their employment. More research is needed to fully understand the complexity of the role of other confounding factors when examining the relationship between cardiorespiratory fitness and occupational workload. However, we believe that there is an increasing need for general awareness amongst Swedish authorities, employees and employers of the potential health consequences of low levels of cardiorespiratory fitness, especially among workers with high occupational workloads. Importantly, when developing interventions targeting the working situation and/or cardiorespiratory fitness levels among workers, researchers should actively involve the relevant population in the design of the study in order to maximize the effect of the interventions on health outcomes.
Keywords
Introduction
Global guidelines on physical activity (PA) and sedentary behaviour recommend regular aerobic and muscle-strengthening activities, as well as limiting time spent sitting, for health promotion and disease prevention [1]. The recommendations are based primarily on evidence of the broad health benefits of leisure time PA and exercise. In contrast, no consensus has been reached as to the role of occupational PA (OPA) for health benefits. A phenomenon referred to as the “Physical activity paradox” has been proposed, implying that PA in the occupational context does not confer the same benefits as PA during leisure time, and may even induce detrimental health effects [2]. An umbrella review from 2018 found a lower risk of several cancer forms, cardiovascular disease and poor mental health with higher OPA [3], while data from a Norwegian study suggested that moderate to high OPA contributes to longevity in men [4]. Contrary to these findings, two meta-analyses found no association between OPA and overall cardiovascular mortality, as well as a non-significant increase in the risk of mortality from ischemic heart disease [5], and an increased risk of early mortality in men [6]. Methodological differences between the studies, and the influence of residual confounding associated with different lifestyles, environmental exposure and socioeconomic status between the occupational groups need to be more closely considered [7,8]. Efforts have been made to target the latter, where even after taking into consideration various lifestyle-, health-, living- and socioeconomic-related factors, the detrimental association between higher OPA and the incidence of cardiovascular disease and all-cause mortality remained [6,9,10].
Mechanisms to explain the physical activity paradox
A next, crucial step to consider in the PA paradox discussion is possible mechanisms. Some suggestions have been made that are related to the general characteristics and context in which OPA is performed [2, 11]. While leisure time PA usually constitutes dynamic and unrestricted movement and body positions with short duration (30–60 min), higher intensity and sufficient recovery between sessions, as well as the activity often being chosen by the individual, OPA generally has the opposite characteristics. These include long duration (⩾8 h), lower/moderate intensities, static and restricted movement and body position, insufficient recovery and less autonomy of the activity performed. In total, these characteristics may increase the likelihood of “wearing the worker out” rather than providing health benefits. This has been elucidated in several cross-sectional studies [12,13]. Using 24-h blood pressure measurements, workers with high OPA had higher mean systolic blood pressure at work, at home and while sleeping. This was in contrast to workers with large amounts of leisure time exercise, where significantly lower mean systolic blood pressure over 24 h was seen [13]. Moreover, in approximately 13,000 participants, those engaging in high levels of leisure PA had lower odds ratios of having elevated levels of high-sensitivity C-reactive protein (marker of inflammation) [12]. On the contrary, participants with high levels of OPA had higher odds ratios, which further increased for those with high OPA and low leisure time PA.
Cardiorespiratory fitness—an important factor for healthy employment?
Another possible explanation for the prevalence of adverse outcomes in workers with high OPA is insufficient cardiorespiratory fitness in relation to the aerobic demands of the occupation. Cardiovascular fitness, often assessed as maximal oxygen consumption (VO2max), is an independent predictor for several non-communicable diseases and premature mortality [14, 15]. A moderate-to-high VO2max is a prerequisite for aerobic endurance performance [16] and, as such, also for engaging in prolonged exercise activities and daily life activities [17]. VO2max is likewise crucial for the average, relative workload during the working day. Daily average workload in 497 blue-collar workers was measured and expressed as a percentage of heartrate reserve (interpretable as percentage of VO2max) [18]. Workers with higher fitness had lower average daily workloads, as well as less time spent above the recommended upper limit of average daily workload (~30% of heartrate reserve [19]). Translating this into possible adverse health effects, a study including blue-collar workers showed that more time spent above this recommended upper limit of average, relative work load was associated with lower heartrate variability and a higher average heartrate the following night [20]. Both these variables may indicate an imbalanced autonomic cardiac modulation in response to a high occupational workload, which could partly explain the higher incidence of cardiovascular disease reported in these occupational groups.
Declining trend in cardiorespiratory fitness
We recently presented data from occupational health profile assessments in over 350,000 men and women from the Swedish working population that showed a decline in cardiovascular fitness over the last few decades [21]. This trend was confirmed in a systematic review including over 2.5 million adults from high- and upper-to-middle income countries [22]. The decline was more pronounced in men, younger age-groups [21,22], and in blue-collar or low-skilled occupations [23]. Prognostic analyses forecast a continued downward trend of cardiovascular fitness, especially in low-skilled white-collar and blue-collar occupations [23]. This may be counterintuitive, as many consider PA at work to be a “work-out”, while it often has too low intensity to improve cardiovascular fitness [18,24,25]. In addition, the long durations of PA at a high mean intensity during working hours may be sufficiently tiring for the individual, leading to less engagement in vigorous fitness-enhancing leisure-time PA—as often seen in individuals with heavy occupational loads [26,27].
Are today’s workers fit for work?
It would be highly relevant to reveal the proportion of workers from different occupational groups who have “sufficient” cardiovascular fitness in relation to their work task. Unfortunately, no published data are available on this subject. However, to get an estimate, we used data from a recent publication on the average workload of different occupational groups [28], as well as data on estimated VO2max from the health profile assessments referred to above [21,23]. A randomly selected matched sample, concerning sex, age and self-reported workload (N = 50,000, 2015–2020), was drawn from the cohort of health profile assessments, and matched to the cohort with the average workload data. The same definitions of occupational groups (International Standard Classification of Occupations) were used.
In Figure 1, we present the proportion of workers (right y axis) in different occupational groups (x axis) with “sufficient” VO2max levels in relation to estimated VO2max required for the average daily workload of each occupational group (left y axis). A “sufficient” VO2max was defined as having a VO2max level so that the average daily workload did not exceed 30% of VO2max [18].
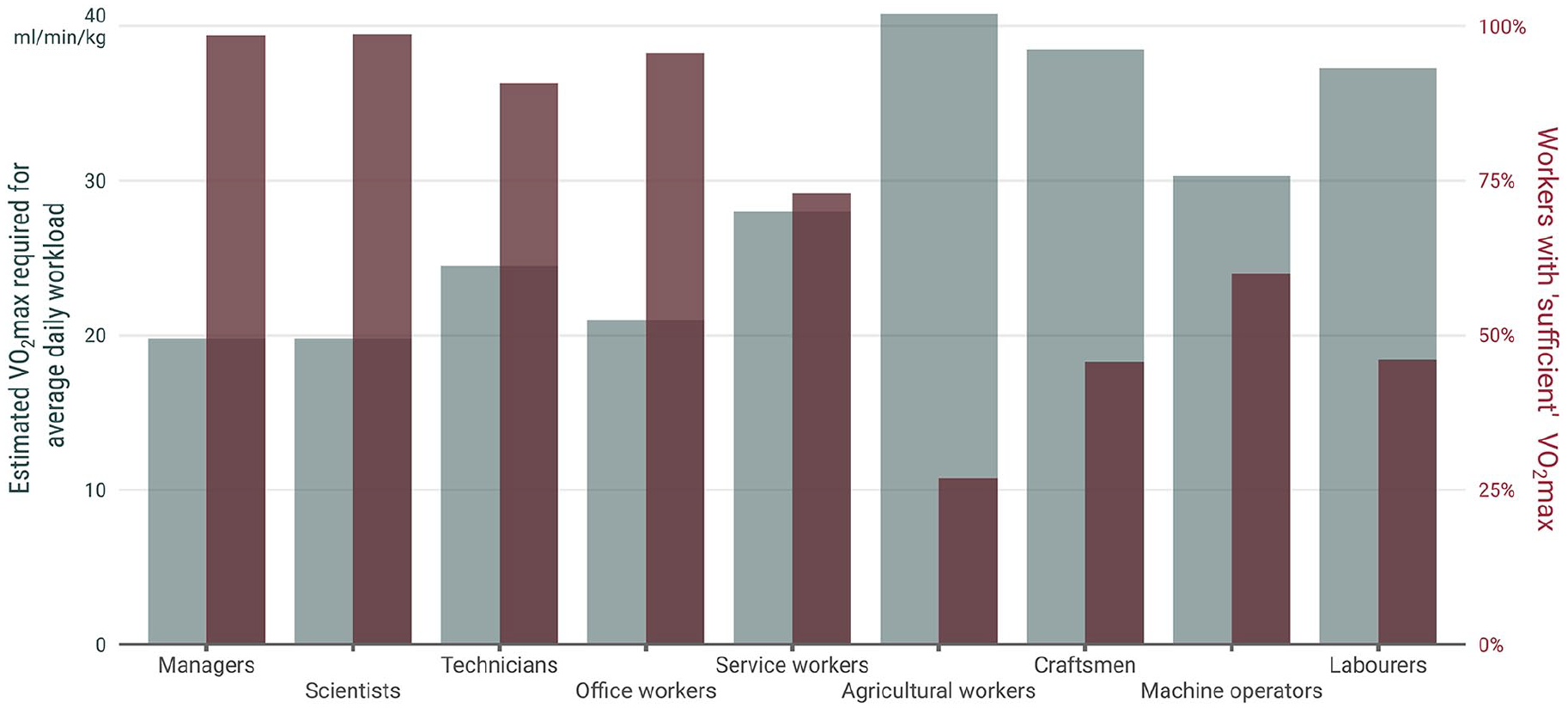
The estimated VO2max required for average daily workload not exceeding 30% of maximal capacity in different occupational groups, and the proportion of workers with “sufficient” VO2max in relation to their workload. The workload in each occupational group was reported by Brighenti-Zogg et al. [28] in metabolic equivalents (METs), which in turn was transformed into relative VO2max (ml min−1 kg−1) by multiplying the MET value with its conventional equivalent 3.5 ml min−1 kg−1. The estimated VO2max required was then calculated by dividing the average daily workload in ml min−1 kg−1 by 0.30. This proportion represents the recommended level (30% of VO2max) that average daily workload should not exceed [18] (Formula Whole = Part/Proportion). The average workload in percentage of VO2max was calculated for each participant by dividing the transformed workload in ml min−1 kg−1 by estimated VO2max in ml min−1 kg−1.
A large majority (91%–99%) of workers in occupations with low workloads (managers, scientists, technicians and office workers) had a sufficient VO2max relative to their work tasks. However, among occupations with higher average workloads (agricultural workers, craftsmen, machine operators and labourers), only every fourth to every second employee had a sufficient VO2max. This indicates that an insufficient VO2max may be a contributor to the adverse health outcomes in these groups, which is in addition to the above-described characteristics of long duration, static and restricted movement and insufficient recovery associated with high OPA. This is of particular concern among the aging population. In a recent publication, older construction- and healthcare workers had lower cardiorespiratory fitness than their younger colleagues, regardless of similar or higher physical demands [25]. This warrants future research on how to also organize work in relation to age and aerobic capacity so as to enable sustainable employment.
Conclusion, and what then?
Although many occupations have developed and become less physically demanding in the last few decades, a large part of the workforce still works in occupations with high aerobic demands. Although some thought-provoking research points to a potential PA paradox, further investigation is needed to confirm whether this is true, and for whom, and when high OPA may be detrimental. Based on basic principles of work physiology and previous epidemiological evidence on the importance of cardiovascular fitness for health and performance in general, the potentially negative role of low cardiorespiratory fitness should be a target for improving sustainable work participation. More research is warranted on the absolute and relative strain among different occupational groups, and to understand the complexity of the issue. However, in light of the large numbers of Swedish workers in our sample with “insufficient” cardiorespiratory fitness, it is a matter of urgency to create awareness of the issue, and for authorities and employees to develop preventative strategies. Using the workplace as an arena for improving the health of workers, as opposed to general community-based health-promoting interventions, has been suggested as a more effective strategy to reach and include groups that might otherwise be difficult to motivate. Importantly, when designing interventions targeting the working situation and/or cardiorespiratory fitness levels among workers, researchers should actively involve the relevant population in the design of the study in order to maximize the effect of the interventions on health outcomes [29]. Some promising research and initiatives have already been suggested [30–32], but more research is required before these can be implemented on a larger scale.
Footnotes
Acknowledgements
None
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.