
Abstract
We examined how obese children perceive a maximal cardiorespiratory fitness test compared with a submaximal cardiorespiratory fitness test. Twenty-one obese children (body mass index ≥95th percentile, ages 10–17 years) completed maximal and submaximal cardiorespiratory fitness tests on 2 separate occasions. Oxygen consumption (VO2) and overall perceived exertion (Borg 15-category scale) were measured in both fitness tests. At comparable workloads, perceived exertion was rated significantly higher (P < 0.001) in the submaximal cardiorespiratory fitness test compared with the maximal cardiorespiratory fitness test. The submaximal cardiorespiratory fitness test was significantly longer than the maximal test (14:21 ± 04:04 seconds vs. 12:48 ± 03:27 seconds, P < 0.001). Our data indicate that at the same relative intensity, obese children report comparable or even higher perceived exertion during submaximal fitness testing than during maximal fitness testing. Perceived exertion in a sample of children and youth with obesity may be influenced by test duration and protocol design.
Introduction
Childhood obesity is a complex condition that can lead to a plethora of health problems including decreased fitness, metabolic complications, and psychological comorbidities. 1 Obesity is characterized by a greater than average increase in adiposity over time and is denned in the pediatric population as a body mass index (BMI) ≥95th percentile. 2 If left untreated, obesity-related comorbidities may develop in children at an early age that include sleep apnea, 3 cardiovascular disease risk factors, 4 type 2 diabetes, 5 and mental health issues. 6 Additional evidence suggests that it is highly likely that obese children will carry their excess weight into adulthood and thus have an increased risk of becoming obese adults in the absence of intervention. 7 It has been demonstrated that obese children have poorer maximal cardiorespiratory fitness levels than their normal weight peers, given the increased effort required to move a larger mass. 8 This is troublesome as physical fitness (ie, cardiorespiratory fitness [CRF] or VO2max) has been shown to be a modifiable health indicator in children and adolescents that may prevent the onset of metabolic complication, independent of the presence of excess adiposity. 9 As a result, the physical fitness of obese children warrants further investigation, as it may serve to be a valuable component of clinical assessment of health risk in an obese pediatric population.
Evaluating cardiorespiratory fitness in a population of children struggling with excess weight may be challenging for exercise physiologists unfamiliar with the complexities of obesity. A measure of maximal CRF, or VO2max, is defined as the maximum ability of the human body to transport and consume oxygen during sustained aerobic work. 10 Such levels of maximal exertion are seldom attained in untrained individuals, due to the strict criterion that define VO2max (ie, plateau in oxygen consumption despite increases in workload, elevated lactic acid in blood, elevated respiratory exchange ratio [RER]). 10 When a maximal CRF test is completed with too few or none of these aforementioned VO2max criteria, VO2peak is more appropriate to report. 11 Recently, Breithaupt et al found that only 18 obese children participants (n = 62) were able to attain a true VO2max, reinforcing the notion that VO2peak is a more realistic outcome in obese children. 12 There may also be instances where a submaximal CRF test is preferable in children with obesity, for example, to account for limited exercise experience or reduced familiarity with vigorous physical exertion. It has also been suggested that obese children may perceive various intensities of physical exertion differently than their normal weight counterparts.13–15 One study has previously illustrated that obese children rated their perceived exertion on an incremental treadmill test significantly higher than a normal weight control group. 16 However, there is very limited research available for evaluating rate of perceived exertion during graded exercise tests in obese children and no available research on perceived exertion for submaximal graded exercise tests in this population. Despite this finding, previous research has found that children are successful at reporting subjective measures of physical exertion during graded exercise tests, 17 and this may also be true for obese children. To our knowledge, no study has compared how obese children from a clinical cohort perceive their exertion while completing both maximal and submaximal graded fitness tests.
Therefore, the purpose of this study was to examine how obese children perceive their exertion during a maximal CRF test compared with a submaximal CRF test. It is hypothesized that in a group of children struggling with obesity, a higher perceived exertion will be reported in the maximal CRF test compared to the submaximal CRF test when normalized for intensity.
Methods
Participants
Children with a body mass index (BMI) greater than or equal to the 95th percentile 2 from the Children's Hospital of Eastern Ontario (CHEO) pediatric endocrinology clinic were asked to take part in the Physiological and Psychological Predictors and Determinants of Metabolic Complications of Pediatric Obesity (POC) study from July 2008 – October 2010. Any child undergoing an obesity assessment at the pediatric endocrinology clinic was invited to participate. As part of the POC study assessments, participating children completed a maximal CRF test. Of the POC subjects who completed the maximal CRF test and met VO2peak criteria, 18 21 subjects accepted an invitation to complete a submaximal CRF test on an additional day. 12 Both fitness tests were conducted in the same laboratory using the same equipment and were performed in similar conditions (ie, air temperature) at similar times of the day. Children were also given similar instructions for food intake prior to performing both tests. Written, informed consent (for participants >16 years of age) or parental and child assent (for participants <16 years of age) were attained prior to completing the submaximal fitness test. Both the maximal and submaximal fitness test protocols were approved by the Children's Hospital of Eastern Ontario Research Ethics Board.
Anthropometric measures
Subject body mass (kg) was measured utilizing a medical-grade SECA 634 digital scale to the nearest 0.1 kg. Subject height (cm) was measured with a SECA 222 stadiometer. Measurements were taken with subjects’ clothes on and shoes removed. BMI (kg/m2) was calculated for each subject.
Cardiorespiratory fitness measures
For both maximal and submaximal CRF tests, oxygen consumption (VO2) was measured breath-by-breath with a MedGraphics Ultima metabolic cart (MedicalGraphics Corporation, St. Paul, MN, USA). After determining VO2peak, percent VO2peak was calculated in all subjects for each stage completed in both CRF tests as follows:%VO2peak = (stage VO2 [mL/O2/min]/VO2peak) × 100.
A Polar F6 heart rate monitor (Polar Electro Oy, Kempele, Finland) was worn by participants for a 3-minute rest period prior to testing to determine resting heart rate (HR). Both fitness tests were supervised by a certified exercise physiologist.
Fitness test 1: progressive maximal treadmill test
A progressive maximal treadmill test developed by Gutin et al 18 commenced with a 4-minute warm-up, whereby the subject selected his or her self-pace walk (SPW) speed. The first 2-minute stage began at a grade of 0% and increased to a speed of 2.0, 2.5, 3.0, or 3.5 miles per hour depending on the subject's SPW speed (ie, SPW speed 2.2 mph for warm up, stage 1 speed = 2.5 mph). In the second 2-minute stage, the treadmill speed increased by 0.5 miles per hour and was capped at that speed, while grade remained at 0%. Starting at the third stage, treadmill grade increased by 2.0% every 2 minutes until the subjects indicated that they could not continue. A 2-minute cool down period was provided for each subject to regulate heart rate.
Fitness test 2: HALO submaximal treadmill protocol
The recently validated HALO submaximal treadmill test, developed by Breithaupt et al 12 and influenced by Nemeth et al, 19 was conducted on all subjects. SPW speed was selected by each subject for a 4-minute warm-up period, and this remained stable for the remainder of the test. Upon conclusion of the warm-up, grade increased by 3.0% every 4 minutes for a maximum of 6 stages. Testing was complete when the subjects attained a HR ≥ 85% of theoretical maximal HR (HRmax = 220 – age), completed 20 minutes of exercise (excluding warm-up), or indicated they could no longer continue the test due to injury. A 2-minute cool down period was provided for each subject to regulate heart rate.
Perceived exertion measure
The Borg 15-category (6–20) scale was used to measure overall rate of perceived exertion for each stage completed in both CRF tests. 20 Overall RPE was administered 10 seconds prior to the next exercise stage beginning. A percentage of effort was assigned to each category value, for data analyses purposes, after all tests were completed.20,21
Statistical analysis
Descriptive statistics were used to summarize subject anthropometric and demographic variables. A 1-sample t test was used to test for significant difference in test time duration between the submaximal and maximal protocol. To examine the relationship between perceived exertion and percent VO2peak, a linear mixed effects model for perceived exertion was used, which accounted for the repeated measurements within subjects for the different stages of each protocol. The initial model allowed for different slope and intercept for the two protocols. A likelihood ratio test of significance of the slope-by-protocol interaction was performed. Statistical significance was denned to be a 2-sided P value < 0.05. Statistical analyses were performed using R (version 2.15.1, R Core Team, Vienna, Austria).
Results
Twenty-one subjects completed this study. Anthropometric and demographic characteristics are presented in Table 1. Ten subjects were boys (mean age, 14 ± 2 yrs; mean BMI, 35 ± 3.0 kg/m2) and 11 subjects were girls (mean age, 14 ± 2 yrs; mean BMI, 35.4 ± 4.3 kg/m2). There were no significant differences between boys and girls at baseline for anthropometric or demographic measures.
Sample characteristics.

A summary of both CRF test outcomes is displayed in Table 2. Mean percent VO2 and ratings of perceived exertion were recorded for each stage for both CRF tests. Mean absolute perceived exertion at test termination, as measured by Borg scale, was 18 (±2) in the maximal test compared with 14 (±3) in the submaximal test. Mean test duration time was significantly longer (P < 0.001) in the submaximal test (14:21 ± 04:04 seconds) than in the maximal test (12:48 ± 03:27 seconds).
Percent of peak VO2, perceived exertion, absolute perceived exertion, and duration in maximal and submaximal CRF tests (n = 21).

A linear mixed effects model for perceived exertion was fitted, accounting for repeated measurements of subjects over the different stages of each of the 2 protocols Figure 1. The slope was not found to differ significantly between the two protocols (P = 0.86). However, across levels of percent VO2, the submaximal protocol exhibited a 5.8% higher average perceived exertion compared to the maximal protocol (P < 0.001). Starting at 10 on the Borg scale, a 5% difference in perceived effort equates to 1 point higher on the Borg Scale (ie, at the same workload, submaximal Borg value 14 and maximal Borg value 13). One subject's trajectories were selected for display purposes in (Fig. 1); however, these trajectories should not be taken as representative of the entire sample population. It is important to note that if a subject selected the same perceived exertion score for 2 or more stages, a brief plateau can occur.
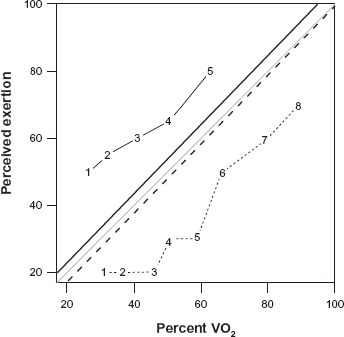
Perceived exertion comparison for the submaximal and maximal cardiorespiratory fitness tests.
Discussion
The major finding of this study was that obese children perceived the maximal and submaximal CRF tests differently. This observed difference, however, was contrary to our hypothesis that obese children would report higher perceived exertion at the same relative intensity in the maximal fitness test when compared with the submaximal test. Although higher mean absolute perceived exertion score was demonstrated in the maximal fitness test (18 on 20 on the 15 point Borg Scale) compared with the submaximal fitness test (14 on 20 Borg Scale), this sample of obese children perceived intensities during the submaximal protocol to be significantly more exerting than equivalent intensities during the maximal protocol (ie, when comparing RPE reported during both tests normalized for intensity,% VO2peak) (Fig. 1).
This is the first study to illustrate that obese children perceive their exertion differently in submaximal and maximal CRF tests. In order to explain this observed difference, the CRF test protocols were examined more thoroughly. Although the submaximal protocol was designed to contain fewer stages than the maximal protocol, each submaximal stage was 4 minutes in duration compared with the 2-minute maximal stages. The results in Table 2 indicate significantly higher test duration in the submaximal CRF test compared with the maximal CRF test. The longer time spent exercising in the submaximal CRF test may be a possible explanation for the higher ratings of perceived exertion at the same relative intensity, as this population may be unaccustomed to the physiological responses to moderate and vigorous exertion (ie, sweating, fatigue, increased respiratory rate, and higher body temperature). Also, the submaximal protocol was designed to have the treadmill grade increase by 3.0% after each stage was completed. A steeper incline coupled with longer stage time durations may have accounted for the participants higher ratings of perceived exertion in the submaximal test. Perceived exertion, when normalized for intensity, in this sample of obese children may be more influenced by the cardiorespiratory test's duration. Another factor that may have affected these findings is the amount of exercise experience in this sample of children with obesity. Little to no experience with longer bouts of continuous exercise (ie, distance running) may have played a role in the higher rating of perceived exertion in the submaximal protocol. These findings, however, cannot be generalized to all obese children since this study's sample stemmed from a clinical treatment program.
Despite it being perceived as more physically exerting when normalized for intensity, specifically percentage of VO2peak, the submaximal test exhibited lower absolute or final ratings of perceived exertion compared with the maximal fitness test. However, the submaximal CRF test was completed by all subjects according to the protocol's outlined termination criteria. 12 This was a beneficial scenario for the test administrator and clinical team, as a prematurely terminated fitness test provides many interpretative challenges.
Limitations and future research
A limitation of this study's design is that the CRF testing order was not randomized, as the submaximal fitness test was always completed after the maximal fitness test. This may have influenced this study's findings. For example, it is possible that the subjects understood the concept of RPE better during the second test (submaximal protocol), and, as a result, rated their exertion higher in the submaximal test. Additionally, the authors of this study recognize that not comparing these findings with a nonobese control group is a limitation. Future research examining perceived exertion in different graded-treadmill exercise tests in children with obesity should increase the sample size and include a lean control group to strengthen potential findings. Furthermore, future studies should stratify children with obesity based on their exercise experience (ie, experienced and non-experienced groups) to account for any differences between groups.
Conclusion
Contrary to popular belief, our examination indicated that, according to RPE data, obese children did not perceive a submaximal fitness test to be less challenging than a maximal fitness test when normalized for intensity. These higher ratings of perceived exertion observed in the submaximal test may have been due to the longer test duration. We suggest that clinical exercise physiologists, or clinical health professionals executing pediatric fitness testing, gauge their protocol selection based on the subjects’ medical history and familiarity with physical exertion.
Author Contributions
Conception of the research experiment: KBA. Collected the data: PB, JR. Analyzed the data: KB, NB. Wrote the first draft of the manuscript: KB. Contributed to the writing of the manuscript: KB, ZMF, RCC, KBA. Made concrete revisions to the manuscript: PB, ZMF, JR, SH, RCC, KBA. All authors reviewed the final manuscript.
Funding
This work was funded by the Canadian Diabetes Association Innovation Grant #IG-1-07-2307-KA, and equipment was supplied through a CFI/ORF Leaders Opportunity Fund Grant awarded to K.B.A. K.B.A is a recipient of CIHR new investigator award.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgements
The authors would like to thank Allana Leblanc and Alysha Harvey for their assistance with this project. The authors also thank CHEO's pediatric endocrinology department and the Centre for Healthy Active Living for their support. The abstract of this paper was previously published as a poster presentation in Canadian Journal of Diabetes 2013;37 Suppl 2:S260.