
Abstract
The purpose of this study was to assess the behavioral and physiological health-related risk factors in college students. A cross-sectional study was conducted in 1620 college students (21.3 ± 1.7 years, 897 males, and 723 females). Physical activity (PA), sitting time, body composition, cardiorespiratory fitness (CRF), muscular endurance (ME), and blood test were assessed. In the total sample, 15.2% were not meeting PA guidelines, 33% were sedentary, 13.3% were obese, 10.7% had low CRF, 36.8% had poor ME, 33.7% had dyslipidemia and 5.9% presented with prediabetes. Obesity and poor CRF were more prevalent in male students, whereas inactivity was more prevalent in female students. Individuals with poor CRF were more likely to be obese (odds ratio = 5.2, 95% CI = 3.5-7.8, P = .007 for male students, and 9.4, 95% CI = 1.5-57.8, P = .021 for female students). Sitting time positively correlated with fat percentage (fat%) and inversely with lean body mass (LBM) in male students, whereas ME inversely correlated with fat% and positively with LBM in female students. Although most students were active, significant prevalence of health-related risk factors were observed. Sedentary behavior and poor fitness were associated with a compromised body composition in both sexes. Improving fitness and reducing sedentary behavior in college students could be a public health strategy for health promotion and chronic diseases prevention.
‘In this regard, systematic reviews and meta-analyses have demonstrated that sedentary behaviors, mainly prolonged sitting time, are associated with abnormal glucose and lipid metabolism . . .’
Introduction
Globally, approximately 40 million people die (70% of all deaths) annually from chronic diseases such as cardiovascular disease, cancer, respiratory diseases, and diabetes. 1 In the United States, nearly half of the adult population (117 million) has at least 1 chronic condition, and 1 in 4 adults present with multiple chronic conditions.2-4 The actual cause for these morbidities, and ultimately mortality, is largely attributed to modifiable lifestyle risk factors such as cigarette smoking, poor diet, physical inactivity, and obesity.5,6 Health data from the US Department of Health and Human Services show that 39% of adults in the United States are obese, and approximately 80% of the population do not meet the combined aerobic and muscle strengthening national physical activity (PA) guidelines.4,7
Emerging data from recent years also suggest that sedentary behaviors, mainly prolonged sitting and poor cardiorespiratory and muscular fitness, are important health-related risk factors, which are independent from PA.8-15 In this regard, systematic reviews and meta-analyses have demonstrated that sedentary behaviors, mainly prolonged sitting time, are associated with abnormal glucose and lipid metabolism; muscle atrophy; gain in fat mass; increased risk for morbidity and mortality from type 2 diabetes, cancer, and cardiovascular diseases; and all-cause mortality.8,9,12,13,16 Poor cardiorespiratory and muscular fitness have been also demonstrated to be associated with substantial morbidity and mortality, including compromised cardiometabolic risk factor profiles, cardiovascular disease and events, developing of functional limitations, incidence of many chronic conditions, and mortality attributed to various diseases.9-11,14,15,17 These conditions and diseases are known to be developed from a young age and slowly progress for several decades until clinical manifestation. 18
Although previous studies among young adults, such as college students, attempted to characterize the risk factor profile, the findings were inconsistent and had methodological limitations that were challenging to generalization and public health implications.19-24 These limitations include a small sample size described in the studies, a compromised evaluation of body composition in utilizing body mass index (BMI) measures, and a lack of objective fitness assessment. In particular, the muscular fitness component has been rarely assessed and is considered a powerful prognostic marker for morbidity and mortality.10,11,15,19-23
College students are a relatively large subgroup of young adults, comprising approximately 20 million (6%-6.5%) of the total US population. 25 College years are a critical period when lifelong behaviors are formed and may have an impact on the development of chronic conditions later in life. 26 Exploring these topics and having a better understanding seems to be the key for developing primary prevention strategies in young adult college students. Therefore, the present study aimed to assess the behavioral and physiological health-related risk factors in male and female college students.
Methods
Participants
This cross-sectional study consisted of 1620 college students (18-24 years old) enrolled in Physical Activity and Nutrition classes of general education at a University in the Mid-Atlantic region of the United States between September 2013 and April 2016. As a part of course requirements, students were assessed for PA and sedentary behavior surveys, blood biomarkers, body composition, and physical fitness tests. The study was approved by the institutional review board of the university, and all students provided written informed consent to use their data for research. The study is a part of an ongoing prospective evaluation of college students designed to address physiological, clinical, and behavioral lifestyle factors and their association with health determinants. All participants were assessed during a 1-day visit between 8:00
Physical Activity and Sedentary Behavior
The Global Physical Activity Questionnaire (GPAQ) has been electronically utilized to assess PA and sedentary behavior. GPAQ is a reliable and validated tool developed by the World Health Organization (WHO) and has been tested on large population-based surveys in adults.27,28 The questionnaire consists of 16 items collecting information on PA participation in 3 settings (work, travel to or from places, and recreational activities). GPAQ also contains a specific question on sedentary behaviors (sitting time). According to GPAQ’s manual, total PA was calculated in metabolic equivalent (MET)-minutes per week units. The sum of the total activity multiplied by the constant level of intensity (4 METs for moderate and 8 METs for vigorous) multiplied by the number of minutes performed per day and by the number of days performed per week was obtained. Sitting time was calculated in average hours per day. Total PA of ≥600 METs-min/wk was considered as meeting the minimal weekly PA guidelines. 17 Sedentary behavior was defined as sitting time ≥6 h/d, as was previously described.29,30 This threshold has been previously demonstrated to be associated with increased risk of cancer, diabetes, and all-cause and cardiovascular and cancer-specific mortality among men and women.29-31
Blood Samples
Blood samples were collected after overnight fasting condition in the morning. Careful sterilization was performed, and 40 µL of capillary blood was collected via finger stick and injected into a commercially available analyzer (Cholestech LDX, Abbott Labs, Abbott Park, IL). Total cholesterol (TC), low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides (TG), and fasting glucose (FG) were measured. Normal values, according to established guidelines, were as follows: TC < 200 mg/dL; LDL < 130 mg/dL; HDL ≥ 40 mg/dL; TG < 150 mg/dL; and FG < 100 mg/dL. 17
Anthropometrics and Body Composition
Height and weight were measured using standard DETECTO medical scale (Webb city, MO). BMI was calculated according to the WHO established equation [weight (kg)/height (m)2]. 17 WHO categories were applied for normal (18.5 to 24.99 kg/m2), overweight (25 to 29.99 kg/m2), and obesity (≥30 kg/m2) BMI values. 17 Body composition of lean body mass (LBM) and body fat percentage (fat%) were measured using bioelectrical impedance analysis (BIA; Omron BF306, Omron Global, Lake Forest, IL). All participants were instructed to follow previously recommended guidelines for body composition testing 3 hours before the test. These include maintaining normal hydration and refraining from eating, consumption of highly caffeinated products, smoking, and intensive PA.17,32
Fitness Tests
Cardiorespiratory fitness (CRF) was assessed using a well-established YMCA submaximal exercise test on a cycle ergometer (Monark 828e, Vansbro, Sweden). 17 The test consisted of two to four 3-minute stages of incremental exercise following a warm-up stage of 150 kgm/min load. The test was terminated when the participant achieved ≥85% of age-predicted maximal heart rate (220 − Age). Work rates, heart rate, and blood pressure were monitored during the test, and data from each test were entered into the Fitness Analyst software package (BSDI, Califon, NJ) to estimate maximal oxygen consumption (VO2max). According to the test protocol, the software extrapolated the achieved submaximal heart rate and work rates to maximal predicted values based on age and test performance and calculating VO2max values (in mL/kg/min). 17 VO2max values <29.5 mL/kg/min for men and<19.3 mL/kg/min for women were considered as poor CRF based on normative values. 33
Muscular endurance (ME) was assessed using an established 1-minute maximum repetition push-up test. Female participants performed the modified push-up test where knees were placed on the floor. The score for both men and women was based on the number of push-up repetitions achieved during the test. 17
Health-Related Risk Factors Determination
The well-established Guidelines for Exercise Testing and Prescription recommended by American College of Sports Medicine (ACSM) were utilized for determination of health-related risk factors. 17 Obesity was defined as body fat% ≥25 for men and body fat% ≥35 for women.17,34 Dyslipidemia was defined as one or more abnormal blood lipids according to Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) adopted by ACSM. 17 Prediabetes was considered when FG levels ranged between 100 and 125 mg/dL, as previously recommended. 17 Risk factor for low CRF was considered if VO2max values were <29.5 mL/kg/min for men and<19.3 mL/kg/min for women.14,17,33 Performance less than 16 repetitions for men and 9 repetitions for women is considered as poor ME on the push-up test and was defined as a risk factor.10,11,17 Risk factor for inactivity was considered as PA <600 METs-min/wk, levels that correspond to 150 min/wk of moderate-intensity activity, a minimal recommended PA level.4,17 Sitting time ≥6 h/d was defined as health-related risk factor of sedentary behavior as previously described.29-31
Statistical Analysis
SPSS (IBM, Chicago, IL) version 23 was used for statistical analyses. The significance level was set at P <.05. Data of the participants are presented as mean ± SD for continuous variables and percentages for categorical variables. Comparison between male and female students was performed using the independent-sample t-tests for continuous variables and χ2 tests for categorical data. Pearson correlations were conducted for behavioral and physiological continuous variables. Odds ratios between risk factors were calculated. Exploratory analysis of Cohen’s κ agreement test was performed between obesity defined as BMI ≥30 kg/m2 and obesity defined as fat% ≥25 for men or fat% ≥35 for women.17,34 Missing data were considered as missing completely at random and analyzed using complete case methods. 35 The Bonferroni method was applied for correction of significant P values to address multiple testing in correlation and risk factor analyses. 36
Results
The study included 1620 college students (21.3 ± 1.7 years, 897 males, 723 females). Demographic, behavioral, and physiological characteristics are presented in Table 1. In the total sample, 81.3% were Caucasian non-Hispanic, 5% were African American, 8.7% were Asian, and 2.4% Hispanic. The average BMI was 24.8 ± 7.6 kg/m2; PA levels were 2391 ± 2120 MET-min/wk; and sitting time was 5.1 ± 2.2 h/d. PA recommendations were not met by 15.5%; 33% were sedentary; and low ME was prevalent in 36.8% and dyslipidemia in 33.7% (Table 2). Obesity and low CRF were more prevalent in male compared with female students (17.2% vs 6.8%, P = .017) and (13.6% vs 0.7%, P < .001), respectively (Table 2). Individuals with low CRF were more likely to be obese: OR = 5.2, 95% CI = 3.5-7.8, P = .007, and OR = 9.4, 95% CI = 1.5-57.8, P = .021 for male and female students, respectively. Sitting time was correlated with fat% (r = 0.13; P = .009) and LBM (r = −0.20; P = .009) in male students, whereas ME was correlated with fat% (r = −0.31; P = .01) and LBM (r = 0.18; P = .01) in female students.
Participants’ Characteristics.
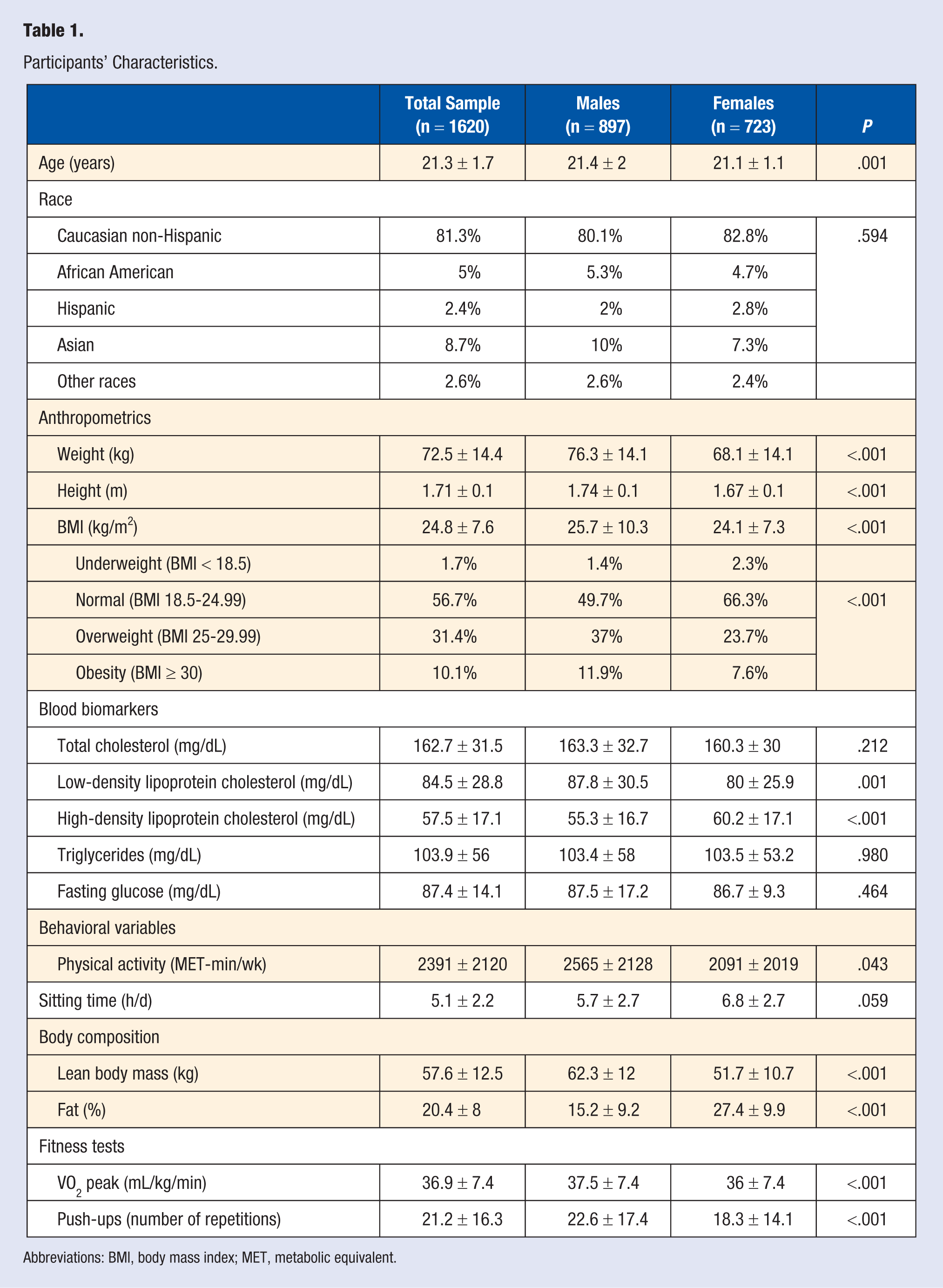
Abbreviations: BMI, body mass index; MET, metabolic equivalent.
Prevalence of Health-Related Risk Factors in College Students.
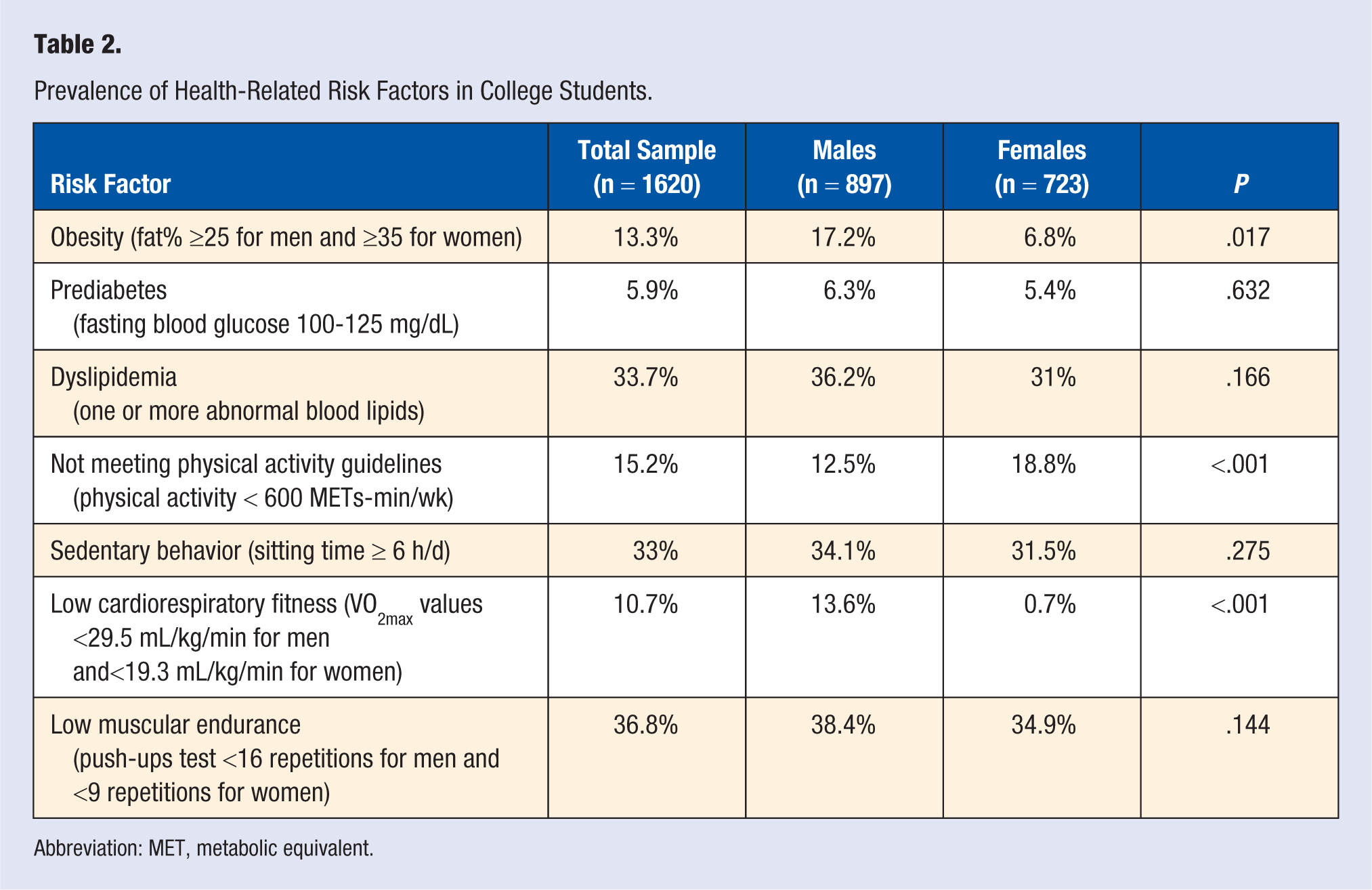
Abbreviation: MET, metabolic equivalent.
Approximately one-third of male students and a quarter of female students exhibited 2 health-related risk factors (Figure 1). Among male students, there was low agreement between obesity defined by the BMI ≥30 kg/m2 threshold and obesity defined by fat% ≥25 threshold measured with BIA (Cohen’s κ = 0.27; χ2 = 68.62; P < .001). Among female students, there was moderate agreement between obesity defined by the BMI ≥30 kg/m2 threshold and obesity defined by fat% ≥35 threshold measured with BIA (Cohen’s κ = 0.45; χ2 = 14.4; P < .001).
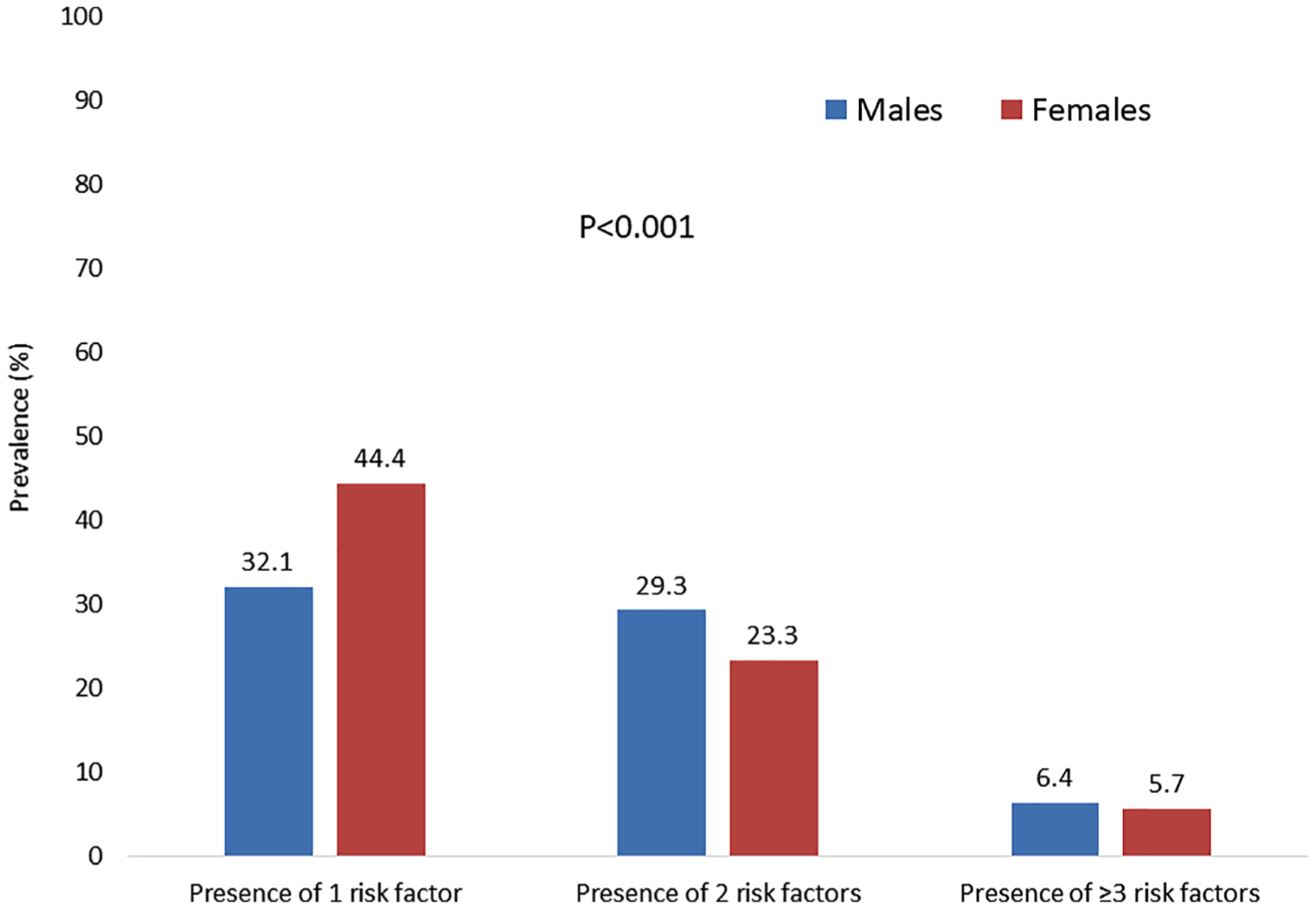
Prevalence of number of risk factors in college students.
Discussion
In the current study, we sought to assess the behavioral and physiological health-related risk factors among male and female college students. The main findings indicate that although most students were meeting the PA guidelines, a considerable prevalence of and interrelationships between behavioral and physiological health-related risk factors were observed. The results showed that approximately one-third of male students and a quarter of female students exhibited 2 health-related risk factors, a fact that requires further attention and development of preventive strategies for college students (Figure 1). In addition, sedentary behavior and poor ME were prevalent in more than one-third of the students, and were correlated with higher fat% and lower LBM. Both sexes who presented with poor CRF had a high likelihood of being obese. Given that most chronic diseases are caused by prolonged exposure to health-related risk factors that are initiated at a young age, 18 the current findings have important public health implications for general health promotion and primary prevention programs of college students. Particularly, considering that higher cardiorespiratory and muscular fitness levels and lower sedentary time are strongly associated with favorable health outcomes,4,9,10,12-17 the current study underscores the potential health benefits of reducing sedentary behaviors and achieving higher fitness levels as a preventive strategy to combat the later development of chronic diseases among young adult college students.
The findings of the current study are consistent with previous observations of cardiometabolic risk factors, PA, and sedentary behaviors in college students.19-24,37,38 The study also adds several insights, which further reinforce the issue of sedentary behaviors and promoting fitness in young adults. The current study utilizes the well-established cardiometabolic risk factor criteria for assessing the prevalence of health risk factors in college students. 17 The study is one of few studies in college students measuring muscular fitness as a health risk factor,39,40 a powerful prognostic marker of mortality.10,11,15,17 Additionally, obesity assessment using BIA in college students was not widely utilized in this population, an established method for obesity evaluation, which has been validated with dual energy X-ray absorptiometry and underwater weighing. 41 The results highlight the relatively high prevalence of health-related risk factors as well as the prevalence of sedentary behavior and poor muscular fitness despite normal PA levels. It was previously demonstrated that people can meet or exceed the PA guidelines and yet spend the majority of their waking hours in sedentary behaviors (active couch potatoes). 42 This behavioral pattern has been shown to be associated with increased risk for morbidity and mortality even after adjustment for PA levels.8,9,12,13 A recent study among male firefighters found that ME assessed by push-up exercise capacity was inversely associated with cardiovascular events during a 10-year follow-up. 43 In line with this report, the relatively high prevalence of poor ME observed in the current study is further proof of the importance of muscular strengthening activities for maintenance and improvement of muscular fitness and reduction of risk for chronic diseases and adverse events.4,10,15,17 In addition, several risk factors observed in the current study were significantly correlated with a compromised body composition and high likelihood of being obese, factors that have been shown to increase the risk of developing chronic diseases later in life. 18 For instance, a large prospective cohort of approximately 2 million men and women have demonstrated that obesity during young adulthood was associated with significantly increased incidence of colorectal cancer diagnosed later in adulthood. 44
The concerning observation in the current study related to the fact that a substantial proportion of students exhibited more than 1 health-related risk factor (Figure 1). This observation aligns with previous reports, showing that unhealthy lifestyle factors tend to be present as a cluster and have a synergistic negative effect on health.45,46 The findings also demonstrate sex disparities with respect to the prevalence of these risk factors (Table 2, Figure 1). Particularly, in the current study, male students showed a higher prevalence of obesity, low CRF, and low ME compared with female students (Table 2). However, the presence of only 1 health-related risk factor was more prevalent in female compared with male students (Figure 1). This topic requires further investigation and exploration in future studies. Interestingly, exploratory analyses showed that there was only mild to moderate agreement (27% to 45%) between obesity detected by BMI ≥30 kg/m2 and obesity detected by fat% using BIA. These results provide further support that a more accurate measure than BMI is required for detecting obesity in young and active adults. 17
Potential behavioral and physiological mechanisms may explain these findings. Prolonged sitting is associated with abnormal glucose and lipid metabolism, muscle atrophy, obesity, type 2 diabetes, cancer, cardiovascular disease, and mortality.8,13,16,23 The sex variation in the risk factors profile we observed is possibly related to the behavioral and physiological differences in this student population. It is likely that because female students were somewhat less active and with higher prevalence of not meeting PA guidelines, presence of 1 risk factor was higher compared with male students. However, male students presented with higher prevalence of obesity, poor ME, and higher prevalence of 2 risk factors compared with female students (Figure 1, Tables 1 and 2). This observation was not fully understood given the descriptive nature of the current study, although the results support the substantial body of evidence showing only moderate correlation between PA and fitness. 47 Future experimental and observational studies are needed to further explore and better understand this phenomenon.
The strengths of the study include a robust methodology with comprehensive evaluation of behavioral and physiological health-related risk factors, utilizing well-established tools for assessment, which significantly increases the internal validity of the study.17,27,28,32,34 A relatively large sample size of students that exceeds previous reports in this population is also an important strength that enhances the external validity and generalizability.19-22 Additional strengths are the inclusion of both male and female participants and using a wide range of statistical analyses for a comprehensive evaluation of the health-related risk factors profile. The study also has several limitations. First, although consistent with previous reports, data on diet habits, smoking, and alcohol consumption were not available in the current study.19,22,23 However, the findings are consistent with previous systematic reviews and meta-analyses, supporting the external validity of the study and providing reasonable confidence for generalization.8,9,12,13 Second, despite the fact that PA and sitting time were collected by self-report questionnaires, this method is well established and accepted to assess lifestyle behaviors.8,9,12,13 The questionnaire utilized in the current study (GPAQ) was developed by the WHO and has strong validity and reliability for assessing PA and sedentary behaviors in different adult populations.27,28 Finally, the results of the current study provide significant associations between behavioral and physiological health risk factors, although cause and effect relationship cannot be drawn. This fact too is consistent with all epidemiological studies of lifestyle, fitness, and health outcomes.8,9,12,13,46
Conclusions
Although most students were physically active, considerable prevalence and interrelationship between behavioral and physiological health-related risk factors were observed. Poor ME, dyslipidemia, sedentary behavior, and obesity were the most prevalent risk factors, with some sex disparities. The results support reducing sedentary behavior, achieving higher fitness levels, and maintaining a healthy body composition as a public health strategy for health promotion and chronic disease prevention in college students.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Review Board of the Pennsylvania State University.
Informed Consent
All participated students provided written informed consent to use their data for research.
Trial Registration
Not applicable, because this article does not contain any clinical trials.