
Abstract
Excessive weight gain in infancy is an established risk for childhood obesity. Primary healthcare professionals have regular contact with infants and are well placed to monitor their growth. This review explores primary healthcare professionals’ practice in monitoring growth for infants from birth to 2 years, addressing assessment methods, practitioner confidence and interventions for unhealthy weight gain. Reviewers searched four databases for studies of primary healthcare professionals working in high-income countries that reported on practice monitoring infant growth. Thirty-six eligible studies documented health professionals’ practice with infants. While most clinicians regularly weighed and measured infants, some did not record measurements comprehensively. Growth monitoring occurred regularly during well-child visits but was less common during unscheduled visits. Some participants were less proficient at interpreting growth trajectories or lacked confidence in detecting excessive weight gain and in communicating concerns to parents. Few interventions addressed unhealthy growth among infants. Primary healthcare professionals require support to monitor growth trajectories effectively, to communicate appropriately with parents and to engage them in developing healthy behaviours early. Strategies are also required to monitor infants not regularly attending primary health care.
Background
Excessive weight gain in infancy is an established risk factor for later obesity and overweight in childhood. This highlights the importance of early identification and timely intervention to detect potential problems during infancy and work with families to help reverse unhealthy weight gain (Woo Baidal et al., 2016).
In high-income countries, infants regularly attend primary healthcare professionals (PHPs) who monitor infant health and development and undertake health promotion activities such as immunisation. Many children attend well-child checks at key development stages as well as unscheduled visits for illness (Office for Health Improvement and Disparities, 2022). Health professionals in primary care include general practitioners (GPs), family physicians, community nurses, child and family health (CFH) nurses, general practice nurses, dietitians and others with regular contact with young families. Given their regular contact, these practitioners have opportunity to detect early signs of unhealthy weight gain, including under-nutrition and over-nutrition, during routine consultations (Ray et al., 2022). An extensive review of literature on PHPs’ role in preventing and treating childhood obesity in clinical and community settings highlighted several activities. PHPs assessed and monitored weight status, and also promoted healthy lifestyles, developed health professional skills, built capacity in primary care, enhanced multisector collaboration and advocated for policy change (Vine et al., 2013).
The current study explored literature on PHPs’ role in monitoring infant growth and what action they take specifically regarding infants with unhealthy weight gain or feeding practices. Growth monitoring is vital to prevent childhood obesity, requiring specific resources and professional expertise (Carsley et al., 2018). These authors indicate that growth monitoring ‘consists of serial measurement of weight, height/length and calculation of body mass index, with plotting these measures on a growth chart’ (2018: 405). However, in addition to weighing and measuring infants and recording these results, effective growth monitoring also requires health professionals to interpret weight trajectories, communicate with parents about fluctuations, and implement interventions if indicated (Sachs et al., 2005).
Considerable research has examined the practices and self-efficacy of PHPs in preventing and managing childhood obesity, although these studies largely focus on growth assessment for older children or do not distinguish specific practice with infants from more general paediatric populations. For instance, Abdin and colleagues reviewed 26 qualitative studies on health professionals’ perspectives on weight-related discussions with children and their families. Although some studies included health professionals working with preschool children, none specifically addressed discussing weight with parents of infants (Abdin et al., 2021). Another review synthesised 13 qualitative studies exploring barriers and facilitators to effective communication with parents about child weight management. No studies focused specifically on discussions about infant weight gain, although some investigated PHPs whose practice included infants under 2 years in wider paediatric clientele (Bradbury et al., 2018). Similarly, an integrative review of literature on relationships between health professionals and parents in managing paediatric weight did not identify studies on the families of infants under two (Farnesi et al., 2012).
Studies of weight monitoring largely focused on children over 2 years. For example, a narrative review of programs to assess children’s weight status was limited to school-based programs for children aged 4–12 years (Davidson et al., 2018). A systematic review of knowledge, attitudes and practices related to childhood obesity among primary care physicians included 11 studies, although most did not specify the age of children seen nor whether their practice was specific to age (Van Gerwen et al., 2009). A comprehensive systematic review examined obesity prevention practices in primary care and identified factors that enabled or impeded implementation of recommended practice by PHPs (Ray et al., 2022). It synthesised evidence from studies on obesity prevention amongst PHPs working with children up to age five. However, we are aware of no literature specifically exploring practitioners’ approaches to monitoring growth and feeding among infants only.
Aim
To explore the practice of healthcare professionals in primary care settings regarding infant growth and infant feeding, focusing specifically on actions and interventions prior to 2 years of age. This review addresses five questions: 1. How do PHPs currently assess infant growth and monitor infant feeding? 2. Do they carry out these activities routinely? 3. How confident do PHPs feel in assessing infant growth and advising on infant feeding? 4. What actions do PHPs take if they identify infants with unhealthy weight gain or feeding practices? 5. What additional skills or training do PHPs believe they need to assess infant growth and monitor infant feeding effectively?
Methods
Study design
Given these varied research questions and our aim to explore evidence on practice with a limited age group across a broad literature, we adopted a scoping review methodology. Scoping reviews assess wide-ranging literature and illuminate gaps and the scope for innovative developments (Levac et al., 2010). We undertook six scoping review stages: identifying research question/s; identifying relevant studies; selecting studies; charting data; collating, summarising and reporting results (Arksey and O'Malley, 2005). Review findings will inform a study of GPs and practice nurses about their confidence, practice and learning needs in assessing infant growth and undertaking timely intervention.
The protocol (not registered) outlined population, concepts and context. Search terms were refined iteratively following greater familiarity with the literature (Arksey and O’Malley, 2005). Results are presented using a PRISMA-ScR checklist for scoping reviews (Supplementary Material 4).
Search strategy
Scoping review inclusion criteria.
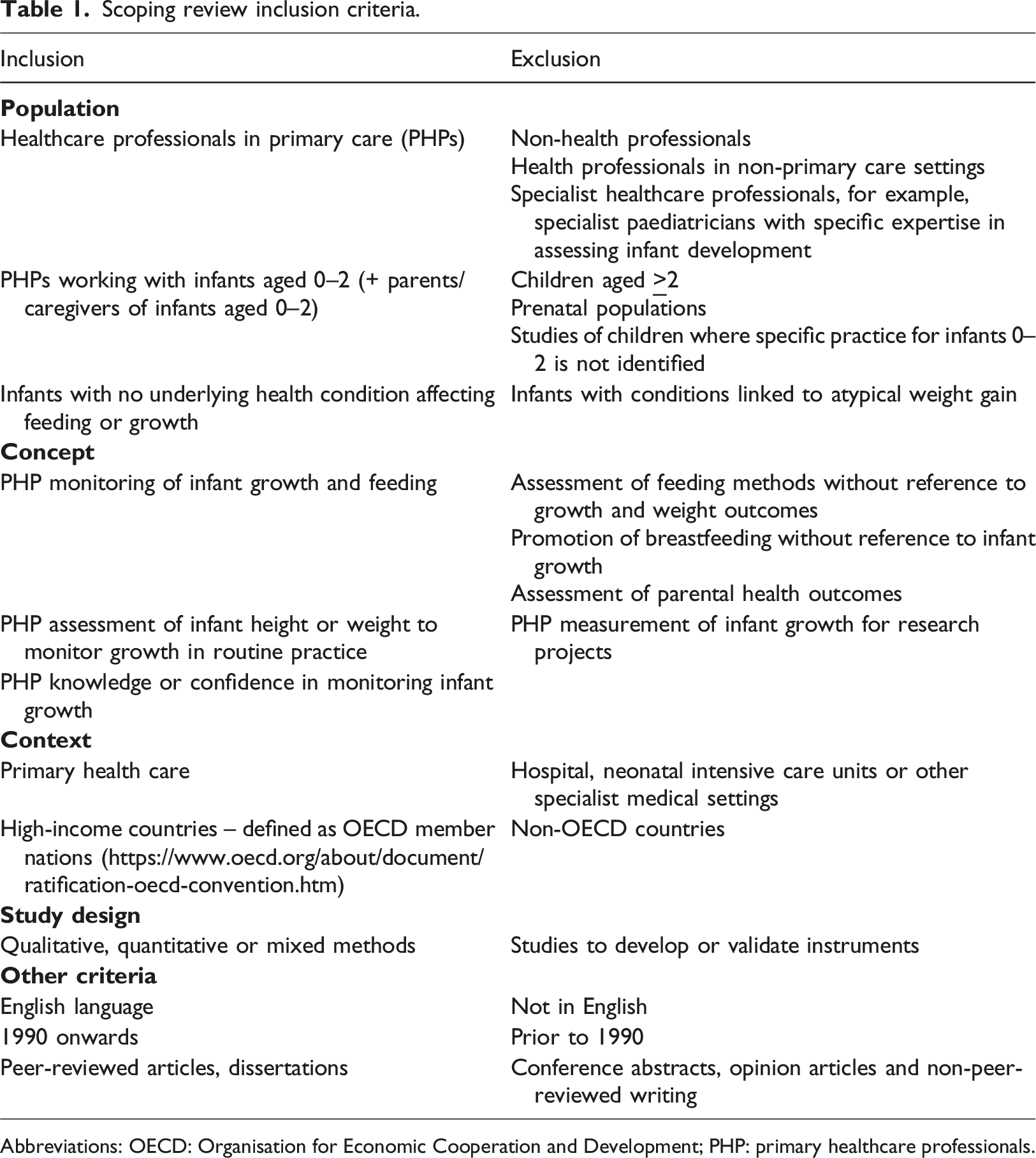
Abbreviations: OECD: Organisation for Economic Cooperation and Development; PHP: primary healthcare professionals.
Information sources
We focused on literature published since 1990 given large increases in childhood overweight and obesity over recent decades. Four databases were searched during June–July 2021: Cumulative Index of Nursing and Allied Health Literature (CINAHL), Medline, Embase and ProQuest Health and Medicine. We further hand-searched references and citation lists of selected studies using Scopus, to identify other potentially relevant titles.
Search terms
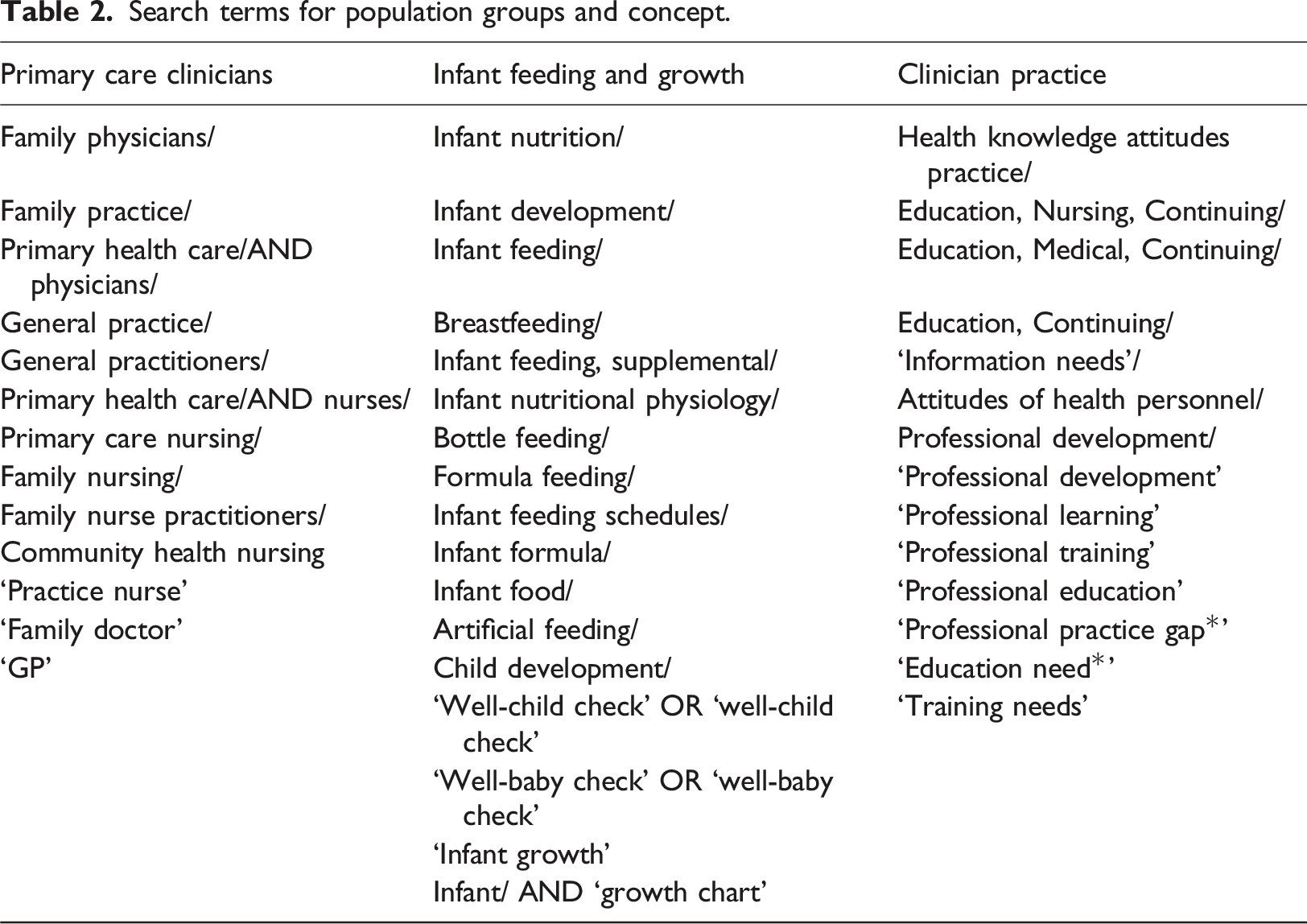
Search terms for population groups and concept.
Selection of studies
Database search results were uploaded to Covidence systematic review software (Veritas Health Innovation, Melbourne Australia. www.covidence.org) for management and review. Two authors (HC and CR) screened all titles and abstracts for potential inclusion and resolved any conflicting decisions by consensus. These authors then reviewed full text articles against inclusion criteria. Conflicts were resolved by a third author (EDW).
Data extraction
Selected studies were summarised by one author (CR) and reviewed by a second (HC), using a table developed specifically for this review and revised after initial testing. Data items included author/s; publication date; title; source of research funding; country; research design and date of data collection; study aim; type of provider; sample description and size; setting; findings and recommendations (relevant to review questions). Extracted data are included in Supplementary Material 2.
We did not assess studies for quality or risk of bias as this is not required for scoping reviews. All relevant potential sources on these topics were considered regardless of quality.
Data synthesis
Synthesis of findings of included studies by review question (N = 36). [See Supplementary Materials 2 and 3 for more detail and results from all studies].
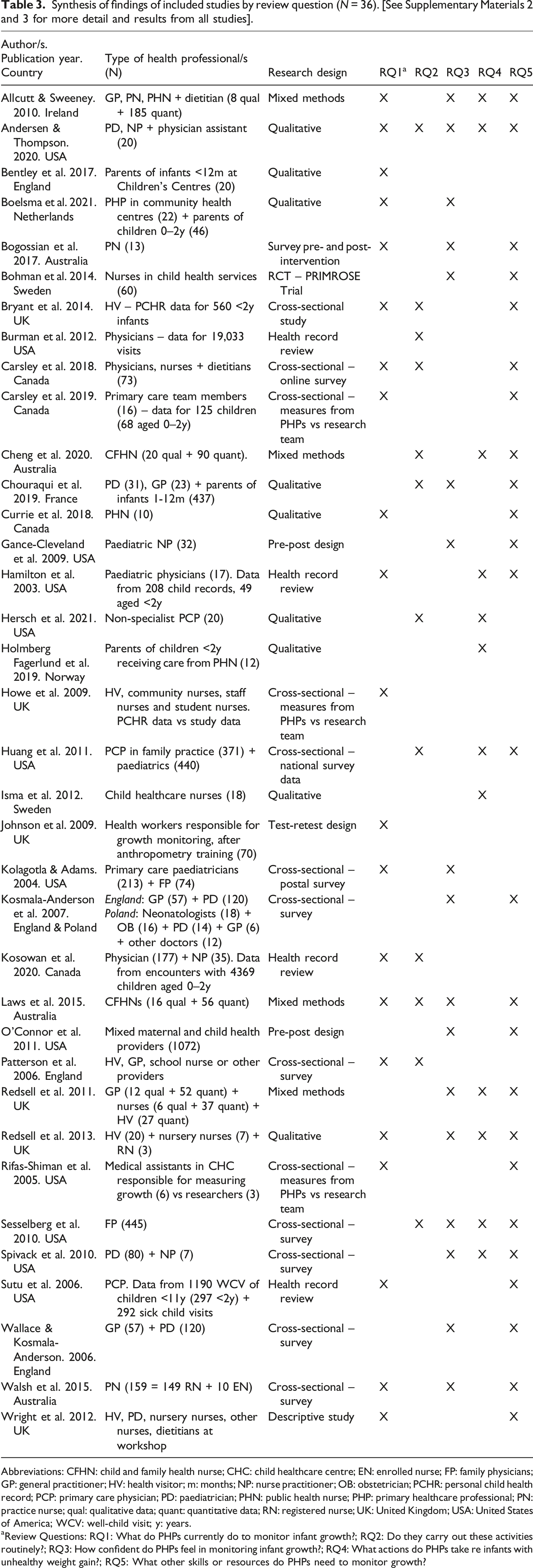
Abbreviations: CFHN: child and family health nurse; CHC: child healthcare centre; EN: enrolled nurse; FP: family physicians; GP: general practitioner; HV: health visitor; m: months; NP: nurse practitioner; OB: obstetrician; PCHR: personal child health record; PCP: primary care physician; PD: paediatrician; PHN: public health nurse; PHP: primary healthcare professional; PN: practice nurse; qual: qualitative data; quant: quantitative data; RN: registered nurse; UK: United Kingdom; USA: United States of America; WCV: well-child visit; y: years.
aReview Questions: RQ1: What do PHPs currently do to monitor infant growth?; RQ2: Do they carry out these activities routinely?; RQ3: How confident do PHPs feel in monitoring infant growth?; RQ4: What actions do PHPs take re infants with unhealthy weight gain?; RQ5: What other skills or resources do PHPs need to monitor growth?
Results
Database searching yielded 838 potential references; subsequent handsearching located another 289. Figure 1 summarises screening and review processes. PRISMA flowchart – scoping review search and review process.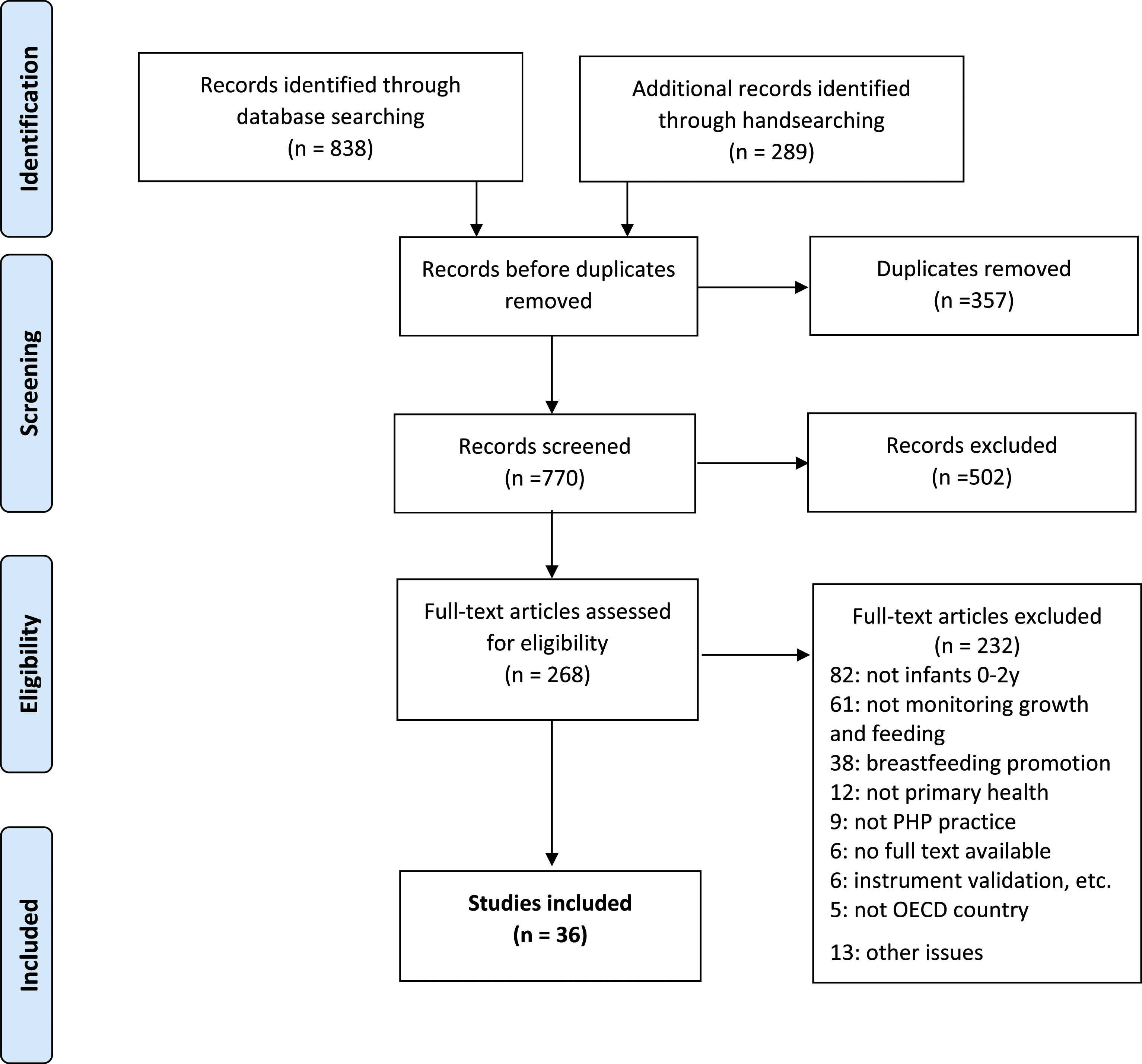
Thirty-six eligible studies addressed at least one review question, dating from 2003 to 2021. Table 3 summarises studies and which review questions each addressed (Supplementary Material 2 and 3 contain further detail and summary findings). Twelve studies were conducted in United States (US), eight in Britain, four in both Canada and Australia, two in Sweden, one in each of France, Ireland, Netherlands and Norway. One study surveyed PHPs in both Poland and England. Most studies were funded by university or government research grants, or by charitable foundations.
Identified studies were diverse, varying in scope and focus. Eleven studied nurses (including general practice nurses, CFH nurses, health visitors and nurse practitioners) and 10 studied doctors (including GPs, primary care physicians, primary care paediatricians). Twelve studies included mixed health professions working in primary health care and one ‘medical assistants’. Three studied parents as participants.
Studies addressed different scoping review questions with a variety of methods. Nine used mail or online surveys, eight used qualitative methods, six analysed existing health records, five used mixed methods, four quasi-experimental or pre-post designs, one randomised controlled trial and three examined methodological reliability and utility of anthropometry methods used in primary care (Table 3).
The most common growth monitoring activity reported in these studies was measuring infant weight and length and recording these measures (Table 3). A review of records from Canadian primary care clinics found that weight was measured more frequently than length and head circumference. Two-thirds of infants had at least one visit with all three measures recorded. However, only 13.7% of infants had complete growth measures at each recommended well-child interval (Kosowan et al., 2020).
Results varied not only in frequency of infant measurement, but also in whether and how PHPs used measures to ascertain risk of overweight. An Irish study found that only 65% of PHPs used centile charts to monitor growth (Allcutt and Sweeney, 2010). A review of records in community health clinics found that 10 of 49 infants under 2 years had measurements that put them at risk of overweight, but none documented this risk nor plans for further evaluation or intervention (Hamilton et al., 2003). A survey of family physicians and primary care paediatricians found a majority compared length and weight to identify overweight and obesity in children aged under 3 years. Around 19% of family physicians and 8% paediatricians relied on children’s ‘general appearance’ to determine weight status (Kolagotla and William, 2004). An Australian study found that while most CFH nurses (85.2%) regularly measured length and weight of infants, only 77.8% plotted results on infant growth charts. Fewer than 60% used growth or BMI charts to identify risk of overweight, although this figure applies to all children (0–5 years) not only infants (Laws et al., 2015). A similar study reported slightly higher rates of measurement (92%) and plotting on infant growth charts (89.7%), but comparable proportions who regularly used growth charts to identify risk of overweight and obesity (56%) (Cheng et al., 2020). One qualitative study identified concerns that growth charts did not adequately account for variable growth trajectories among infants under two; participants reported difficulty in definitively diagnosing excess weight gain (EWG) in this age group using existing resources. Despite consistent methods to assess weight, the resulting identification of EWG varied (Andersen and Thompson, 2020).
Some studies assessed PHPs’ accuracy in anthropometric measurement. Most found that measurements were reliable (Carsley et al., 2019; Johnson et al., 2009; Sutu et al., 2006), although some PHPs over-estimated length (Rifas-Shiman et al., 2005) especially in infants aged between 12 and 24 months (Bryant et al., 2015) or among taller children (Howe et al., 2009). An assessment of equipment used by PHPs found that although most used digital scales for infant weight, only 21% used the most accurate means of measuring length (Carsley et al., 2018).
Some practitioners may consciously avoid monitoring infants’ weights. For instance, PHPs in one study delayed determining growth trajectories until after 12 or 24 months in recognition of variable growth patterns in infancy (Andersen and Thompson, 2020).
Several studies documented variations in growth monitoring frequency. In surveys, PHPs reported measuring infants regularly (Cheng et al., 2020; Huang et al., 2011; Laws et al., 2015; Sesselberg et al., 2010). A survey of US physicians found high proportions who reported ‘regularly’ calculating and plotting infant weight-for-age, length-for-age and weight-for-length (WFL). Nearly half stated they recorded BMI for this cohort (Huang et al., 2011). However, research using other methods found evidence of missing documentation. For instance, a US review of health records found that over 20% of paediatric encounters did not record weight or height. Only half of visits recorded complete growth measures; rates were higher for infants under 7 months, but diminished with infant age (Kosowan et al., 2020). A similar trend of diminishing documentation with age was identified in English primary care trusts (Patterson et al., 2006).
Canadian PHPs reported that, while they frequently measured growth at well-child visits, they rarely assessed infant growth at unscheduled visits (Carsley et al., 2018). Similarly, interviews with primary care physicians indicated that they typically discussed infant weight issues with parents at annual well-child visits rather than at acute visits or at a family’s first consultation (Hersch et al., 2021). Yet, Canadian research revealed that over 20% of infants did not attend well-child visits (Kosowan et al., 2020).
PHPs report varying degrees of confidence in monitoring and advising on infant growth. Survey-based research found limited knowledge of recommendations from professional bodies such as American Academy of Pediatricians on preventing and treating overweight in children (Kolagotla and William, 2004; Spivack et al., 2010; Sesselberg et al., 2010). Yet, another study reported that PHPs were hampered by lack of evidence-based standards to help identify EWG in infants under two (Andersen and Thompson, 2020). A cross-national study found that Polish doctors rated themselves as competent or expert in detecting abnormal growth rates more often (63%) than English doctors (50.3%) (Kosmala-Anderson et al., 2007). Australian CFH nurses reported universal confidence in measuring children and plotting on growth charts. However, three-quarters were confident in using charts to identify obesity risk and only one half could readily identify risk of overweight (Laws et al., 2015).
Allcutt and Sweeney found that approximately two-thirds of PHPs reported being confident advising parents on weaning (2010). Australian practice nurses reported limited confidence advising parents, responding to queries on growth and development, or making recommendations for breastfeeding or introducing solid food (Walsh et al., 2015). One US survey found that only 15% of family physicians and 30% of primary care paediatricians rated their skills in obesity counselling as ‘good’ or ‘excellent’ (Kolagotla and William, 2004). Another survey found that while most family physicians were comfortable counselling families about overweight, far fewer (43%) believed that they were effective (Sesselberg et al., 2010). A British study found that PHPs’ confidence advising parents was not necessarily associated with obesity-related knowledge. They reported limited training on preventing and managing childhood obesity and difficulty identifying children with EWG at unscheduled visits if parents did not bring personal health records (Redsell et al., 2011). Further, health visitors reported problems identifying young children with obesity and difficulties discussing this with parents (Redsell et al., 2013). Dutch child health nurses indicated that resources provided did not assist them to tailor information to families’ circumstances (Boelsma et al., 2021).
Four studies explored education programs for PHPs. These yielded greater self-reported confidence and competence in advising parents and monitoring infant growth among Australian practice nurses (Bogossian et al., 2017), child health nurses in Sweden (Bohman et al., 2014), CFH nurses (O'Connor et al., 2011) and US paediatric nurse practitioners (Gance-Cleveland et al., 2009).
Relatively few studies examined PHP actions for children identified with unhealthy weight gain. Australian CFH nurses reported referring children up to 5 years old at risk of overweight to dietitians and weight management clinics, although not infants specifically (Cheng et al., 2020). Further, a survey of primary care physicians did not report on assessment or parental counselling practice for infants under two (Huang et al., 2011).
Several studies explored PHPs’ approaches to communicating with parents about infant weight (not necessarily in response to detection of risk factors for obesity). They highlighted the importance of establishing rapport with parents, assessing parental perceptions about their child’s weight status and gauging their readiness to change their behaviour (Andersen and Thompson, 2020); PHPs were also concerned not to jeopardise relationships with potentially vulnerable families by raising sensitive topics about weight (Redsell et al., 2011). A qualitative study of primary care physicians highlighted that their practice with infants at risk of overweight took a different approach to older children, focussing on discussing dietary intake with parents (Hersch et al., 2021).
English PHPs indicated that they were reluctant to intervene if infants under 12 months demonstrated EWG, although some health visitors referred larger infants to other healthcare professionals (Redsell et al., 2011, 2013). Child health nurses in Sweden reported refraining from discussing EWG with parents until children were aged over two; some did not consider excess weight as a health concern until school age (Isma et al., 2012). US physicians did not discuss infant weight during a family’s initial visit (Hersch et al., 2021).
There was limited information on practice specifically with infants with EWG. One survey of PHPs explored topics discussed with parents of infants at well-child visits, but not in relation to infants’ weight status (Spivack et al., 2010). More specifically, one US study identified no evaluation or intervention for infants under two whose measurements clearly placed them at risk of overweight, despite greater provider awareness and action for older children with similar risks (Hamilton et al., 2003). In a qualitative Norwegian study, parents reported that growth rates were rarely discussed; no parents mentioned counselling on overweight (Holmberg Fagerlund et al., 2019). An Irish study of PHPs’ advice to parents on weaning indicated that only 21% of practitioners took account of weight gain velocity and 15% noted whether infants’ growth crossed centile lines. Among GPs surveyed, 30% advised weaning earlier than officially recommended (Allcutt and Sweeney, 2010).
An English study of parents of infants found that, although they valued advice from healthcare staff, most believed that parents should identify EWG rather than PHPs (Bentley et al., 2017). Further, some Dutch parents found PHP advice too general and irrelevant to their needs or cultural background (Boelsma et al., 2021).
Many studies highlighted training or resources needed to support PHPs effectively monitor infant growth. Researchers recommended further education on topics including infant feeding and introduction of solid food (Allcutt and Sweeney, 2010; Chouraqui et al., 2019; Kosmala-Anderson et al., 2007; Redsell et al., 2013; Wallace and Kosmala-Anderson, 2006), obesity-related assessment of infant growth and detection of those at risk of obesity (Bryant et al., 2015; Huang et al., 2011; Isma et al., 2012; Kosmala-Anderson et al., 2007; Laws et al., 2015; Redsell et al., 2011, 2013; Sesselberg et al., 2010), causes and consequences of EWG (Cheng et al., 2020; Redsell et al., 2011), infant growth patterns (O'Connor et al., 2011), counselling parents to promote obesity prevention or behaviour change (including recognition of cultural norms and differences) (Boelsma et al., 2021; Cheng et al., 2020; Huang et al., 2011; Laws et al., 2015), accurate measurement and documentation (Hamilton et al., 2003; Johnson et al., 2009; Wright et al., 2012) and responding to parents with non-mainstream needs and beliefs about child nutrition (Holmberg Fagerlund et al., 2019). Several requested evidence-based guidance on effective interventions for preventing obesity and managing infants with EWG (Andersen and Thompson, 2020; Hamilton et al., 2003; Redsell et al., 2011, 2013).
Several studies recommended providing additional resources including standardised growth monitoring and centile charts (Allcutt and Sweeney, 2010), simplified assessment tools (Andersen and Thompson, 2020), standard equipment and procedures to improve accurate measurement and diagnosis of risk of overweight (Burman et al., 2012; Carsley et al., 2018, 2019; Rifas-Shiman et al., 2005; Sesselberg et al., 2010; Spivack et al., 2010; Wright et al., 2012), and additional consultation time to address weight issues routinely (Andersen and Thompson, 2020; Spivack et al., 2010). Parent-focused resources included appropriate information for parents (Allcutt and Sweeney, 2010; Cheng et al., 2020; Spivack et al., 2010), tools to assist sensitive communication with parents and promote healthy behaviours (Andersen and Thompson, 2020; Bentley et al., 2017; Holmberg Fagerlund et al., 2019; Redsell et al., 2011) and greater understanding of nutritional needs among late preterm infants (Currie et al., 2018).
Studies that examined training programs for PHPs reported improved skills and confidence in caring for mothers and infants (Bogossian et al., 2017), encouraging behaviour change among parents (Bohman et al., 2014; Gance-Cleveland et al., 2009), and understanding infant growth in breastfed infants (O'Connor et al., 2011).
Discussion
The aim of this scoping review was to explore PHPs’ practice in monitoring growth among infants under 2 years, given its importance for early identification of EWG and prevention of subsequent obesity. We examined data from 36 studies from high-resource countries that responded to five review questions. These addressed practices not only in routinely measuring infants, but also in understanding growth trajectories and working with parents to manage unhealthy weight gain. Our initial search process yielded many other articles addressing childhood obesity that did not specifically consider practice with this youngest age group. This demonstrates that research on PHP practice specifically with infants is relatively scant.
Sachs and colleagues (2005) proposed five elements of growth monitoring for infant wellbeing. Our review certainly located evidence on the first two elements they described – which tools are used (growth charts, scales) and how they are used. Many studies documented measurement frequency and accuracy. Researchers reported widespread measurement of infant weight in primary health, undertaken by various PHPs. Our analysis identified that survey-based research with PHPs reported that measurement was conducted more regularly than was demonstrated in research using health record reviews. Although most PHPs weighed infants accurately, some miscalculated infant length (often due to inappropriate equipment). Over-estimating length can potentially fail to identify EWG if an inflated denominator reduces WFL scores. Other studies noted that, although they measured infants routinely, PHPs plotted measurements on growth charts less frequently; many health records had incomplete documentation of infant growth over time. Of particular concern was that, despite regular growth monitoring at scheduled well-child visits, PHPs rarely assessed infants at non-routine consultations (Carsley et al., 2018; Hersch et al., 2021). Infants who do not attend primary care, or only do so for illness, may be at particular risk due to inadequate records of their growth trajectories.
The remaining three elements outlined by Sachs and colleagues (2005) – interpretation of charted weight trajectories, communication with parents about growth fluctuations, and interventions used when growth rates are of concern – were rarely addressed in studies of PHP practice with infants. Few indicated whether PHPs used growth charts or other techniques to interpret infants’ weight trajectories. This practice was less common than plotting infants’ weights and nurses reported lower confidence in determining overweight or obesity risk (Cheng et al., 2020; Laws et al., 2015). Another study found that despite using similar measurement approaches, clinicians varied in their identification of EWG amongst infants (Andersen and Thompson, 2020).
Although research has explored PHPs’ confidence in conversing with parents or conducting obesity counselling for pre-schoolers or older children (Bradbury et al., 2018; Farnesi et al., 2012), few selected studies addressed communication about growth trajectories specifically with parents of infants. One English study of PHPs working with parents of infants found that those professions who were most frequently consulted about infant feeding were less knowledgeable about health risks associated with obesity than other PHPs (Redsell et al., 2011). These health visitors reported difficulty discussing infants’ risk of obesity with parents, consistent with studies with older cohorts on how complex and sensitive PHPs found weight-related discussions with parents of young children (Abdin et al., 2021). Research has identified important considerations such as PHP knowledge and competence, parental motivation and perceptions of their child’s weight status, cultural and individual preferences, and practitioners’ fear of undermining positive therapeutic relationships, especially with vulnerable families. These are compounded by limited time, resources and organisational support in primary care settings (Bradbury et al., 2018; Farnesi et al., 2012; Ray et al., 2022).
There was little evidence of interventions to manage EWG specifically among infants. One study determined that paediatric physicians took no action despite infants being at risk of overweight (Hamilton et al., 2003). Some PHPs in qualitative studies indicated that they refrained from determining that weight gain was excessive or initiating action until infants were older (12 or even 24 months). Several studies highlighted training and information needs for PHPs regarding evidence-based interventions for preventing obesity during infancy and managing EWG amongst infants.
We endeavoured to explore patterns of practice by country. However, divergent study types and procedures made this difficult. Many studies on practice amongst family physicians and paediatricians were conducted in North America and the United Kingdom, including several examining frequency and accuracy of growth assessment amongst doctors, using surveys or health record reviews from England (Bryant et al., 2015; Patterson et al., 2006), Canada (Carsley et al., 2018, 2019; Kosowan et al., 2020), and USA (Burman et al., 2012; Hamilton et al., 2003; Huang et al., 2011). Some US studies found limited knowledge of relevant professional guidelines (Kolagotla and William, 2004; Sesselberg et al., 2010; Spivack et al., 2010). Qualitative research with nurses and other PCPs was more common in Europe (Boelsma et al., 2021; Holmberg Fagerlund et al., 2019; Isma et al., 2012; Redsell et al., 2013) and Australia (Cheng et al., 2020; Laws et al., 2015), providing insight into their confidence in monitoring growth and initiating conversations with parents about regarding EWG.
Limitations
This scoping review had a broad focus, resulting in wide-ranging studies on different aspects of PHP practice. This was related to the number and scope of review questions. Diverse research designs, practitioner groups and outcome measures made synthesis of results difficult. Our approach of categorising findings under different review questions attempted to focus results from a disparate body of research. However, it is difficult to extrapolate results more generally, given that many studies were conducted with small or mixed samples, or in particular locations. It has not been possible to analyse, for example, distinct patterns of practice among different health professions, in different countries or over time.
Several included studies were dated, meaning that some findings may be superseded, also limiting further generalisation. PHPs may have increased their scope or clinical expertise, for instance, and more recent development of professional guidelines may have improved provider awareness and practice. However, participants in a recent qualitative study continued to report the absence of evidence-based standards to help identify and manage EWG in infants under 2 years (Andersen and Thompson, 2020).
Our review possibly failed to locate relevant references on this topic. However, the broad search terms and extensive handsearching provided a comprehensive process. Excluding studies reporting on PHP practice that did not stratify results by child age may have led to overlooking some potentially relevant information.
Implications for practice and research
Limited evidence of consistent proactive growth monitoring for infants suggests that PHPs need further support in promoting optimal development during infancy. This includes education, incentives, and referral options to enable them to identify and intervene with infants with unhealthy growth, and guidance on effective communication with parents to promote healthy behaviour. Studies also highlighted resources needed for both PHPs and parents to better understand issues associated with infant growth and feeding. Standardised growth monitoring and centile charts, as well as appropriate anthropometric equipment (e.g. length boards) are also essential in primary care settings, as is the time necessary to address infant weight during well-child visits.
Reported use of WFL to assess weight gain was limited. Further, relatively few study participants reported familiarity with recommendations from professional bodies. A similar trend was reported in a wider review of PHP growth assessment practice with children aged under 5 years. It found low usage of BMI or WFL calculations to initiate weight-related conversations with parents, and unfamiliarity with guidelines and tools (Ray et al., 2022). This suggests that PHPs require education and guidance on interpreting documented growth and identifying EWG risk.
Strategies are also required to monitor growth among infants who do not regularly attend primary health care. These children may be at particular risk of later obesity if unhealthy weight gain is not assessed and managed early. Innovative and inclusive programs, including opportunistic assessment at sick child visits and drop-in visits at setting such as pharmacies are necessary to increase access to early childhood health care and to promote healthy weight gain respectfully.
Limited evidence on early interventions for PHPs to support parents whose infants demonstrate EWG indicates that new models of care that include provider training, early intervention and frequent follow-up, PHC-based strategies plus referral are urgently needed. Research is necessary to explore effective initiatives and promote the expansion of successful models.
Conclusion
These findings suggest limited involvement amongst PHPs in early intervention for infants whose growth demonstrates potential risk of overweight. Despite knowledge of established links between early rapid weight gain and later childhood obesity and widespread measurement of infant growth, it appears that an important opportunity to reverse early trends has been missed during the critical window of infancy.
Supplemental Material
Supplemental Material - Primary healthcare professionals’ role in monitoring infant growth: A scoping review
Supplemental Material for Primary healthcare professionals’ role in monitoring infant growth: A scoping review by Chris Rossiter, Heilok Cheng and Elizabeth Denney-Wilson in Journal of Child Health Care
Supplemental Material
Supplemental Material - Primary healthcare professionals’ role in monitoring infant growth: A scoping review
Supplemental Material for Primary healthcare professionals’ role in monitoring infant growth: A scoping review by Chris Rossiter, Heilok Cheng and Elizabeth Denney-Wilson in Journal of Child Health Care
Supplemental Material
Supplemental Material - Primary healthcare professionals’ role in monitoring infant growth: A scoping review
Supplemental Material for Primary healthcare professionals’ role in monitoring infant growth: A scoping review by Chris Rossiter, Heilok Cheng and Elizabeth Denney-Wilson in Journal of Child Health Care
Supplemental Material
Supplemental Material - Primary healthcare professionals’ role in monitoring infant growth: A scoping review
Supplemental Material for Primary healthcare professionals’ role in monitoring infant growth: A scoping review by Chris Rossiter, Heilok Cheng and Elizabeth Denney-Wilson in Journal of Child Health Care
Footnotes
Acknowledgements
The authors are grateful to Isabelle Raisin, Academic Liaison Librarian at the University of Sydney.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.