
Abstract
Adolescents face issues regarding physical health, mental health, sexual health, drug and alcohol problems, stress, and peer pressure. Little is known about adolescents’ help-seeking behaviours in relation to health concerns. The general practitioner (GP) is usually the first point of contact for adolescents. The aim of this systematic review was to identify, describe, and summarize evidence on barriers and enablers experienced by adolescents when accessing GP-led primary care services. Systematic searches using four electronic databases (PsycINFO, MEDLINE, CINAHL, and SocINDEX) were conducted and the quality of the included studies was appraised. Six studies were included in this review. Findings indicate that barriers to GP access relate to trust, confidentiality, privacy, and communication. Adolescents also reported barriers such as transport, cost, and lack of information. Adolescents reported enablers being services that are sensitive to their needs, healthcare professionals who understand them, and services that are flexible regarding out of hours access. Listening to and acting on the voice of adolescents is important to developing youth-friendly services.
Keywords
Introduction
Adolescence is one of the most rapidly changing phases of human development (World Health Organization (WHO), 2023). It can be a time when considerable risks to health can arise (WHO, 2023). Although many adolescents make transition to adulthood in good health, others may experience health concerns (Glasner et al., 2020; Schrader et al., 2021).
Adolescence is a period of experimentation where adolescents begin to engage in health risk behaviours which can have a major impact on their health when transitioning into adulthood (Glasner et al., 2020; Kendra and Coker, 2018; Romer et al., 2017). Such engagement can adversely impact their ability to grow and develop and can have detrimental effects on their health, both in the short term and long term (WHO, 2017). Health risk behaviours include drug and alcohol abuse, unprotected sex leading to sexually transmitted infections, unwanted pregnancies, and lack of physical activity (Glasner et al., 2020).
Unintentional injuries are the leading cause of death and disability among adolescents (WHO, 2017). In 2019, nearly 100,000 adolescents aged 10 to 19 years died as a result of road traffic accidents (WHO, 2017). Half of all mental health disorders in adulthood start by the age of 14 years, but most cases are undetected and untreated (WHO, 2023). Worldwide, a quarter of all adolescents aged 15 to 19 years are current drinkers (WHO, 2023). The prevalence of heavy episodic drinking among adolescents aged 15 to 19 years was 13.6% in 2016, with males most at risk (WHO, 2023). Cannabis is the most widely used psychoactive drug among adolescents with about 4.7% of people aged 15 to 16 years using it at least once in 2018 (WHO, 2023). Globally, at least 1 in 10 adolescents aged 13 to 15 years use tobacco (WHO, 2023).
Access to primary care is regarded as an important component of healthcare focusing on preventative health education for young people (Ryan et al., 2023). Previous research found that adolescents are reluctant to seek medical help for health problems for a number of reasons including fear of their parents finding out (Al Omari et al., 2022; Hutton and Jackson, 2014), difficulty getting time off school/work, long waiting times, scheduling issues (Al Omari et al., 2022; Barakat-Haddad and Siddiqua, 2015; Hutton and Jackson, 2014), fear and anxiety surrounding visiting the Family Physician (i.e. General Practitioner (GP)), or feelings of embarrassment due to sensitive health matters (Barakat-Haddad and Siddiqua, 2015; Hutton and Jackson, 2014).
Negative past experiences also prevent adolescents from seeking help (DeJonckheere et al., 2020). Some adolescents try to deal with problems themselves (Turner et al., 2017), while others engage with friends or someone they can trust (Corry and Leavey, 2017). Although primary care is the first point of contact for help-seeking, adolescents often view the GP as a healthcare professional who can deal with their physical illness but not their emotional and mental health needs (Leavey et al., 2011). There is a need to better understand indicators of youth-friendly healthcare to support adolescent engagement with health services (Haller et al., 2007; Thomson et al., 2022).
For almost two decades, the need for adolescent/youth-friendly healthcare has gained international recognition, through the work of the WHO. Publications by the WHO (2002, 2012, 2015, 2017) demonstrated national quality standards to make health services adolescent friendly. In 2017, the WHO published a seminal report titled ‘Global Accelerated Action for the Health of Adolescents (AA-HA!): Guidance to support country implementation’. According to this report, adolescent-friendly health services should be accessible, acceptable, equitable, appropriate, and effective (WHO, 2017). These standards can be applied within the national health service of any country in an endeavour to meet the needs of adolescents today. A systematic review by Ambresin et al. (2013) identified perspectives of young adults on youth-friendly healthcare in tertiary care settings. This review identified eight core domains of healthcare important to adolescents including accessibility, respect, communication, medical competency, confidentiality, age appropriate, involvement, and health outcomes (Ambresin et al., 2013). To the best of the authors’ knowledge, there have been no comparable systematic reviews exploring adolescents’ experiences of healthcare in GP-led primary care services.
Aim
To identify, describe, and summarize evidence on barriers and enablers experienced by adolescents when accessing GP-led primary care services.
Methods
This systematic review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist (Page et al., 2021) (Supplementary File 1).
Eligibility criteria
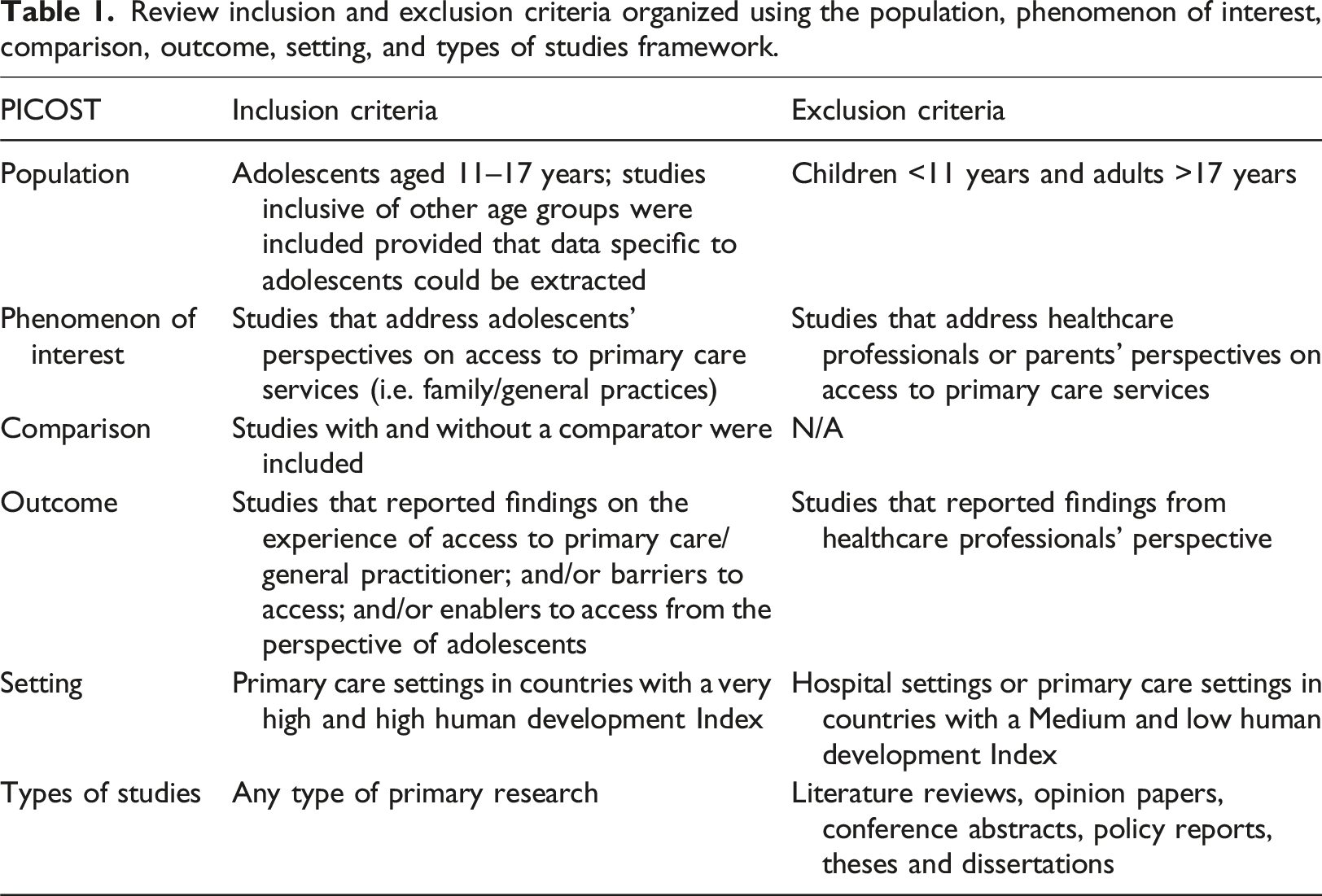
Review inclusion and exclusion criteria organized using the population, phenomenon of interest, comparison, outcome, setting, and types of studies framework.
Search strategy
Four electronic databases (American Psychological Association PsycINFO, MEDLINE, Cumulated Index to Nursing and Allied Health Literature, and SocINDEX) were searched. The following keywords were truncated, searched within title or abstract, and combined using Boolean terms ‘AND’ and ‘OR’: (adolescen* OR teen* OR ‘young person’ OR ‘young people’) AND (‘primary care’ or ‘primary health*’ OR community OR ‘general pract*’ OR GP OR ‘family doctor’ OR ‘family pract*’ OR ‘family physician’) AND (‘help seeking’ OR help-seeking OR access* OR utilis* OR utiliz* OR ‘service user*’). The search was conducted in English and covered the publishing period of April 2009 to April 2019. The search was subsequently updated on March 31st 2022 to source the latest evidence.
Study selection
Records identified from the search were exported to EndNote software (Version X9.2; Clarivate Analytics, 2019). All records were then imported into Covidence (Veritas Health Innovation, 2023), an online software used to produce systematic reviews. Duplicates were deleted automatically in Covidence. Records were first screened based on title and abstract. The full text of potentially eligible papers was then obtained and screened further against the review eligibility criteria. Title, abstract, and full text screenings were conducted by two independent reviewers. Disagreements were resolved by a third independent reviewer.
Data extraction and quality review
Data extraction table outlining key study characteristics and results.
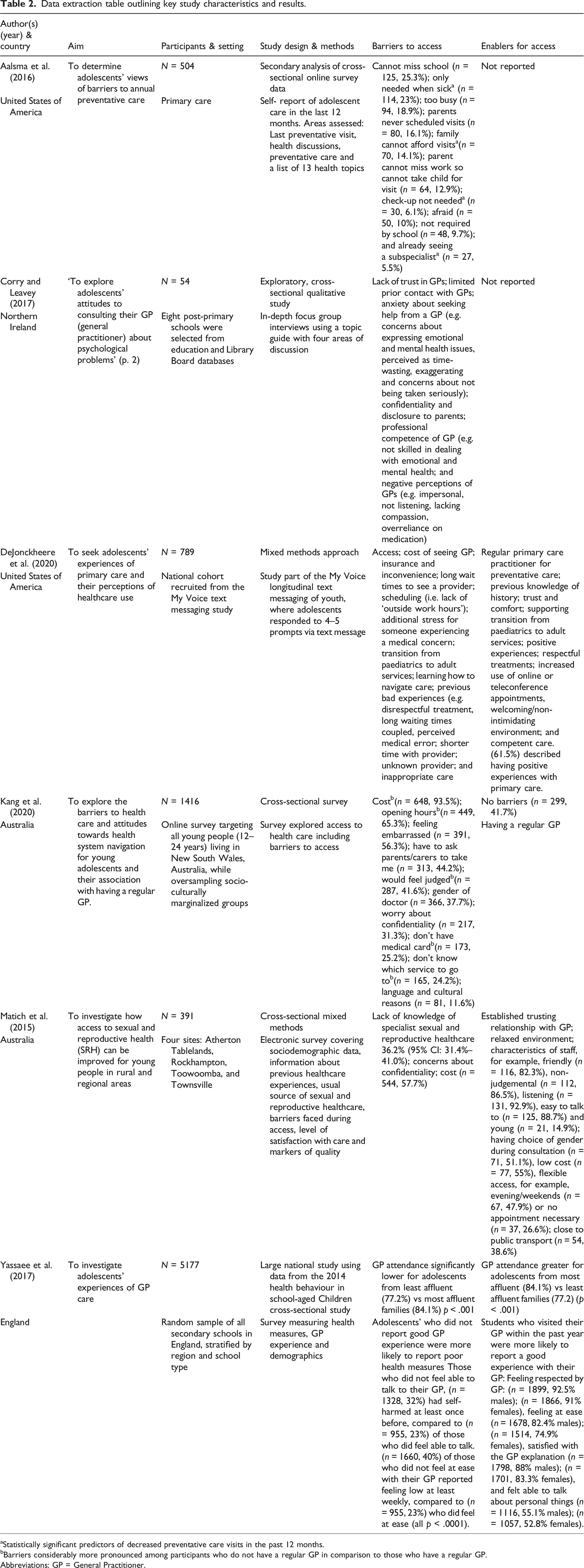
aStatistically significant predictors of decreased preventative care visits in the past 12 months.
bBarriers considerably more pronounced among participants who do not have a regular GP in comparison to those who have a regular GP.
Abbreviations: GP = General Practitioner.
Data synthesis
Due to clinical and methodological heterogeneity, a narrative approach to data synthesis was undertaken (Popay et al., 2006). Therefore, results from the included studies were synthesized in accordance with review aim under the following headings: (i) Barriers experienced by adolescents when accessing GP-led primary care services and (ii) enablers experienced by adolescents when accessing GP-led primary care services.
Results
Study selection
A total of 2964 articles were identified in the search. Following removal of duplicates (n = 860), 2104 records were selected for further review. The full text was obtained for 199 papers; of those, six papers met the review inclusion criteria. A hand search of the reference lists of included studies was conducted and yielded no additional studies. Therefore, a total of six studies were included in this review. The study selection process is illustrated in Figure 1. Record identification, screening and selection process.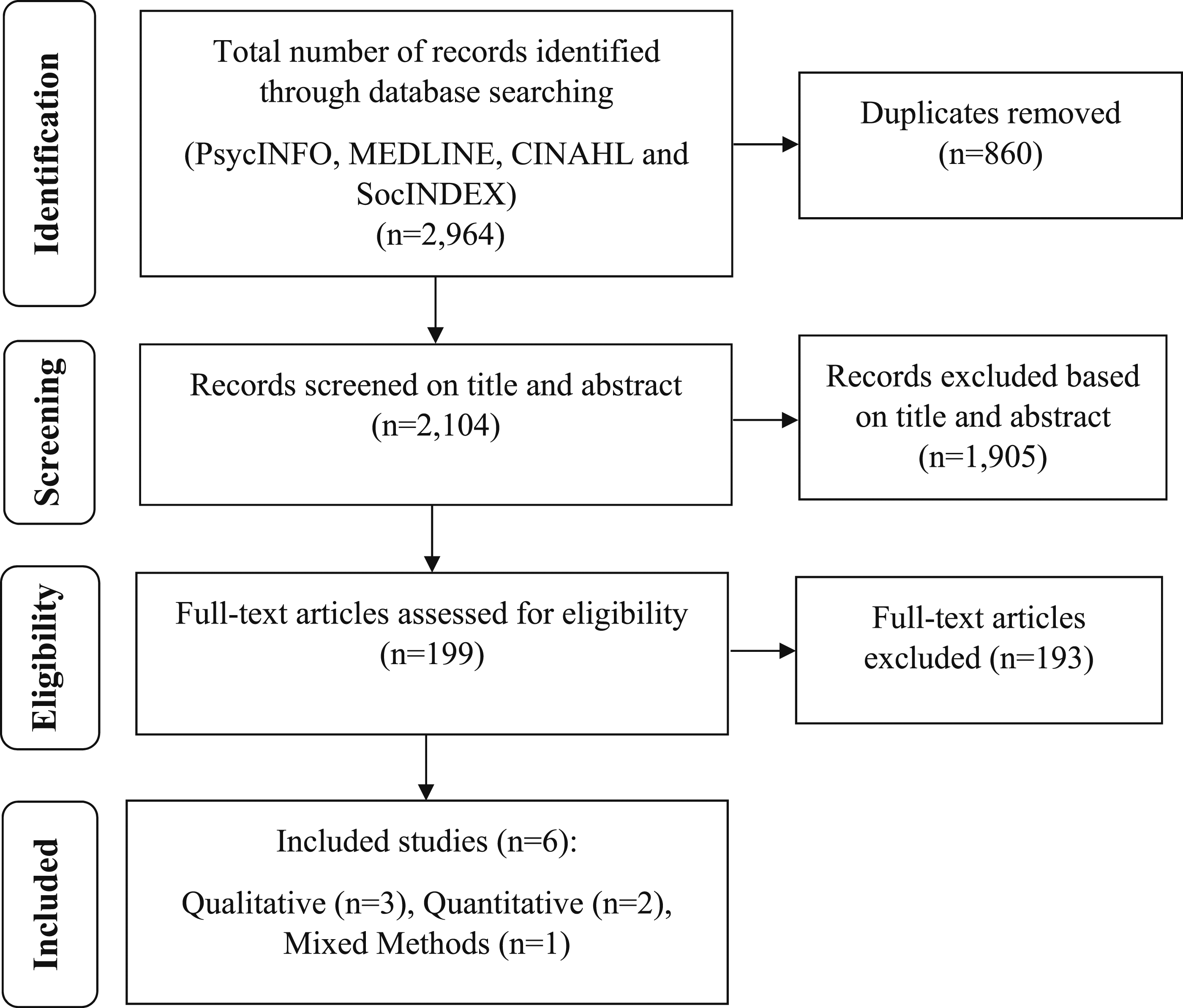
Study characteristics
Countries represented across studies include Australia (n = 2), the United States of America (USA) (n = 2), England (n = 1), and Northern Ireland (n = 1). Four studies used surveys to collect data through online (Aalsma et al., 2016; Kang et al., 2020; Matich et al., 2015) or during class time (Yassaee et al., 2017). An open text messaging forum was used in a study by DeJonckheere et al. (2020), and in-depth focus group interviews were conducted in a school setting in one study (Corry and Leavey, 2017). The number of participants ranged from 54 (Corry and Leavey, 2017) to 5177 (Yassaee et al., 2017).
Methodological quality
One study was assessed using the MMAT (Matich et al., 2015). This study had clear research questions and an appropriate method of data collection. The mixed method study considered researchers’ influence but failed to adequately report quantitative and qualitative data analysis and interpretation of results. The quality of two studies was assessed using the JBI checklist for qualitative research (Corry and Leavey, 2017; Dejonckheere et al., 2020). Overall, studies were methodologically rigorous with congruity between research methodology, study objectives, methods used to collect data, and interpretation of results. Three studies were assessed against the JBI checklist for analytical cross-sectional studies (Aalsma et al., 2016; Kang et al., 2020; Yassaee et al., 2017). It was unclear in two of the studies if exposure was measured in a valid and reliable way (Kang et al., 2020; Yassaee et al., 2017). It was unclear in three of the studies if confounding factors were identified and if strategies to deal with confounding factors were used (Aalsma et al., 2016; Kang et al., 2020; Yassaee et al., 2017). Quality appraisal of the included studies is presented in Supplementary File 2.
Synthesis of results
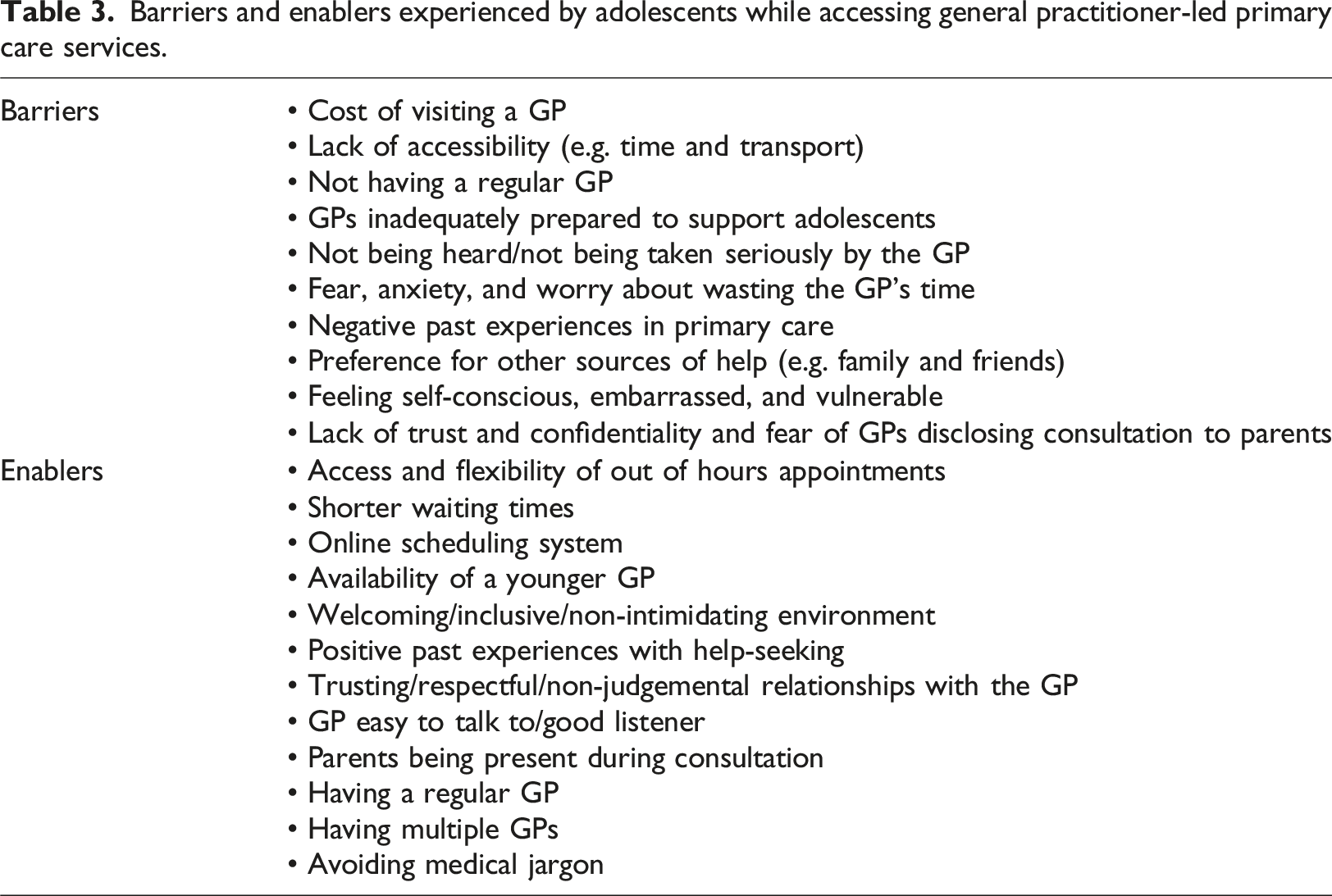
Barriers and enablers experienced by adolescents while accessing general practitioner-led primary care services.
Barriers experienced by adolescents when accessing GP-led primary care services
Barriers experienced by adolescents when accessing GP-led primary care services can be categorized as follows: cost of visit to a GP, lack of accessibility (e.g. time and transport), lack of trust and confidentiality, not having a regular GP, fear, anxiety, feeling self-conscious, embarrassed, vulnerable, and fear of GPs disclosing consultation to parents. These barriers were reported in six studies. The most frequently reported barrier was cost of seeing a GP (Aalsma et al., 2016; DeJonckheere et al., 2020; Kang et al., 2020; Matich et al., 2015). Aalsma et al. (2016) found that 70 (14.1%) adolescents believed that their family cannot afford services.
Three studies reported access barriers which included trying to get time off school/work, long waiting times, and scheduling issues (Aalsma et al., 2016; DeJonckheere et al., 2020; Kang et al., 2020). According to Aalsma et al. (2016), 125 (25.3%) participants reported that they cannot miss school and 114 (23%) reported only needing primary care when sick.
Three studies described barriers regarding fears/anxiety (Corry and Leavey, 2017) and feelings of embarrassment (Kang et al., 2020; Matich et al., 2015) while visiting the GP. More than half (n = 391, 56.3%) of adolescents with a regular GP reported that they would feel embarrassed to access care. According to Aalsma et al. (2016), adolescents stated that, when attending their GP, they felt embarrassed and vulnerable. Another issue related to concerns about wasting the GP’s time (Corry and Leavey, 2017). Adolescents also reported being concerned about confidentiality. Kang et al. (2020) found that 217 (31.3%) adolescents were worried about confidentiality and disclosure to parents, yet 313 (44.2%) would have to ask parents/carers to take them to an appointment.
Negative past experiences have prevented adolescents from seeking help (DeJonckheere et al., 2020). Adolescents' physical and mental health outcomes were poorer when they did not report having a positive GP experience. In a study by Yassaee et al. (2017), 1660 (40%) adolescents did not feel at ease with their GP and reported feeling low at least weekly. According to studies, several adolescents thought GPs were uncaring and judgemental when they visited them for consultations. As a result, they felt fear, embarrassment, and shame (Corry and Leavey, 2017; Yassaee et al., 2017). Adolescents who said they could not really talk to their doctor had a self-harm rate of 1328 (32%) compared to 955 (23%) of those who felt comfortable talking to their doctor (Yassaee et al., 2017).
According to a study by Corry and Leavey (2017), participants did not consider a GP as an appropriate source of help: “They think everything is just about being a teenager and you’re going through a phase” (p. 4). “Doctors don’t take you seriously at our age because they see us as naïve and they wouldn’t -unless you were an adult they wouldn’t question it-just write stuff down” (p. 4).
Seeing a GP was a last resort and adolescents hoped the problem would go away by itself (Corry and Leavey, 2017). Some adolescents felt that GPs were inadequately educated regarding young people’s issues (Corry and Leavey, 2017; DeJonckheere et al., 2020; Kang et al., 2020). Barriers expressed by adolescents included GPs not being skilled in dealing with emotional and mental health problems (DeJonckheere et al., 2020; Matich et al., 2015), lack of advice (Matich et al., 2015), and lack of compassion for adolescents’ needs (Corry and Leavey, 2017). DeJonckheere et al. (2020) found that adolescents felt time with the GP can often be rushed, felt they were not being heard, and they perceived GPs were ill-informed about adolescents’ needs.
A study by Corry and Leavey (2017) found that seeing a GP was perceived as time-wasting and adolescents felt they were not being taken seriously. In keeping with perceived lack of respect, Matich et al. (2015) reported an adolescent’s perspective of GPs: “I find that they do not respect and take younger people seriously. . .people under 20, maybe they believe that they are too young and this comes through as a prejudgment, particularly if they do not know the client” (p. 235).
In DeJonckheere et al.’s (2020) study, one adolescent reported: “I brought my thought of feeling transgender and I felt like my doctor sort of brushed it off” (p. 814).
More than half of participants (n = 427, 61.5%) in the study by Kang et al. (2020) reported having a regular GP, but occasionally had to see a different GP at the same practice because their normal doctor was not available or was too popular, which resulted in unreasonable waiting times for an appointment. One adolescent stated: “My preferred doctor is very popular and to get in you need to make an appointment months ahead, so when I am sick, I need to go to a different one with more availability” (Kang et al., 2020: p. 6).
Likewise, in a study by DeJonckheere et al. (2020), one adolescent stated: “I go to my school clinic and school nurse. My primary care doctor always books appointment out a whole month at least. So, I use the resources available to me that are quicker” (p. 816).
Adolescents reported uncertainties of making appointments in the absence of their parents (Corry and Leavey, 2017) and feared that GPs would disclose purpose and content of their consultations to their parents: “It's all recorded so it could get you in trouble for it - if you went on your own to the doctor without a parent. They would know about it because your GP would obviously tell them because you were underage so you really wouldn't want that” (Corry and Leavey, 2017: p.4).
Knowing that GPs could involve the parents at their discretion was a particular source of distrust among participants: “Yeah, there's like a trust barrier ‘cos you don't know if you can trust them or if they're going to keep it confidential or if they're going to respect you” (Corry and Leavey, 2017: p. 4).
Many adolescents expressed a fear of repercussions at home as a result of their GP informing their parents.
Nevertheless, it was believed that GPs would be obliged to inform parents while adolescents are under the age of 18 years (Corry and Leavey, 2017; Yassaee et al., 2017): “You might not want to tell your parents about it and then going near a GP and talking about it, it's going to start something up at your house because you didn't tell them first” (Corry and Leavey, 2017: p. 4).
Adolescents agreed there are situations in which it may be more helpful for adolescents to see the GP by themselves, rather than having parents come along, in particular if parents are part of the problem for which they are seeking help: “Because like you might not be able to let everything out with your parents beside you” (Corry and Leavey, 2017: p. 4).
Corry and Leavey (2017) reported that adolescents would prefer talking to a parent or friend rather than seeing a GP. However, adolescents reported that they would only provide selective information to parents or friends and would not discuss some problems such as suicidal thoughts. Adolescents also suggested that without their parents being present they feared not being heard or being misunderstood by their GP: “If my mum and dad knew, I would bring them” (Corry and Leavey, 2017: p. 4).
Enablers experienced by adolescents when accessing GP-led primary care services
Enablers experienced by adolescents when accessing GP-led primary care services included access and flexibility of out of hours appointments, shorter waiting times, online scheduling system, availability of a younger GP, welcoming/inclusive/non-intimidating environment, trusting/respectful/non-judgemental relationships with the GP, avoiding medical jargon, GP easy to talk to/good listener, and parents being present during consultation. Such enablers were presented in four studies. Participants who had a regular GP were less likely to cite cost as an issue (Kang et al., 2020; Matich et al., 2015). In a study by Matich et al. (2015), 77 (55%) adolescents reported low cost as being a very important element in a service. Access and flexibility of out of hours were reported as being particularly important in a service. DeJonckheere et al. (2020) asked participants what would facilitate doctor appointments. It was found that 618 (55%) participants mentioned convenience-related factors, including increased availability of appointment dates and options (n = 251, 22.3%), decreased appointment wait times (n = 225, 20.1%), online scheduling possibilities (n = 113, 10%), and more accessible and practical locations (n = 33, 2.9%). In a study by Matich et al. (2015), 67 (47.9%) adolescents suggested flexible access (e.g. evening/weekends) and 37 (26.6%) suggested that no appointment being necessary. Participants (n = 54, 38.6%) suggested the need for practices being close to public transport (Matich et al., 2015). Adolescents felt that improving convenience would make accessing GP-led primary care easier with a broader range of appointment options, shorter waiting times and a preferred online scheduling system: “Allow me to make appointments either online or through text” (Dejonckheere et al., 2020: p. 814).
Those with a regular GP were more likely to report ‘no barriers’ compared to those without a regular GP. The benefit of having a trusted GP was reported in four studies (DeJonckheere et al., 2020; Kang et al., 2020; Matich et al., 2015; Yassaee et al., 2017). Adolescents described trust, comfort, and respect as key components in a GP-client relationship (DeJonckheere et al., 2020). In a study by Yassaee et al. (2017), 3766 (91%) of those who visited a GP in the past year felt they were treated with respect compared to 684 (77.6%) of those who had not visited a GP in the last year. Participants (n = 21, 14.9%) reported that having the availability of a younger doctor was seen an important component when accessing the GP-led service and 71 (51.1%) participants suggested that choosing the gender of the GP was also important.
The importance of having a GP who is easy to talk to and who is a good listener were reported in two studies (Matich et al., 2015; Yassaee et al., 2017). Participants in the study by Matich et al. (2015) listed positive traits of GPs as follows: friendly (n = 116, 82.3%), non-judgemental (n = 112, 86.5%), good listener (n = 131, 92.9%), and easy to talk to (n = 125, 88.7%).
Over half of participants (n = 651, 61.5%) in a study by Dejonckheere et al. (2020) described having positive experiences with primary care providers. Two studies reported that adolescents were satisfied with their GP explanations, continuity of care, level of help, and advice they received during general practice consultations (Kang et al., 2020; Yassaee et al., 2017). According to Yassaee et al. (2017), 3766 (91.8%) adolescents felt treated with respect, 3192 (78.7%), felt at ease, 3499 (85.7%) were satisfied with their GP’s explanations, and 2173 (53.9%) felt able to talk about things. According to Dejonckheere et al. (2020), adolescents suggested that having a regular GP was less likely to be associated with being judged: “A regular primary care physician, can know your history and treat you like family. I feel at home in my doctor's office” (p. 814).
According to Dejonckheere et al. (2020), adolescents described respectful treatment and a welcoming environment as key to improving GP-led primary care visits for youths. Environments that are not intimidating, competent, and can provide care for all gender identities were also highlighted as positive entities: “Create a positive atmosphere for patients: Establishing a strong repertoire between doctor and patient is a way to further care into something that goes beyond” (Dejonckheere et al., 2020: p. 817).
Kang et al. (2020) found that adolescents preferred having access to multiple doctors: “I like to have multiple doctors to visit as one it is more convenient if one is away and also different doctors give different advice. For example, I find one of my doctors more drug orientated to solve my health issues whereas another doctor takes more of a lifestyle change approach. I once had a suspected iron deficiency and one doctor told me to write down everything I ate for a week and told me to visit her in a week and another ordered a blood test. The second was much more convenient as we live in busy lifestyles and demand quick fix solutions” (p. 6).
Aalsma et al. (2016) also found that frequent health care discussions with parents were associated with frequent health care visits with GPs.
Discussion
Findings from this study suggest that adolescents experience both positive and negative experiences when accessing GP-led primary care services. This study contributes to a small but growing body of research on adolescent and youth-friendly services. In the present review, we identified a range of perceived barriers to accessing GP-led primary care services. Perceived lack of confidentiality (Corry and Leavey, 2017; Dejonckheere et al., 2020; Matich et al., 2015), trust (Corry and Leavey, 2017; Kang et al., 2020; Matich et al., 2015) and cost (Dejonckheere et al., 2020; Kang et al., 2020; Matich et al., 2015) were the most commonly identified barriers to help-seeking and access. Issues raised by adolescents also related to concerns about feeling embarrassed (Kang et al., 2020) and fear of wasting the GP’s time (Corry and Leavey, 2017).
Consistent with other literature (Ambresin et al., 2013; Garney et al., 2021; Gulliver et al., 2010; Ryan et al., 2023), we also identified organizational barriers to the utilization of services including long wait times (DeJonckheere et al., 2020) and a lack of coordinated care (Dejonckheere et al., 2020; Kang et al., 2020; Matich et al., 2015). These barriers were structural and prohibited adolescents from accessing timely, youth-friendly services. Paying for these services (Levesque et al., 2013) and the cost of seeing a GP also presented a significant barrier to obtaining healthcare services (DeJonckheere et al., 2020; Garney et al., 2021; Kang et al., 2020; Matich et al., 2015).
Our findings are consistent with findings by Ambresin et al. (2013), who also reported that clinicians’ attitudes, such as lack of respect, lack of friendliness, and perceived medical incompetency were also reported as barriers. Lack of trust was identified through professional competence and negative perceptions of professionals (Corry and Leavey, 2017). Adolescents suggested that GPs who were judgemental failed to create warmth and interest and seemed detached (Dejonckheere et al., 2020; Kang et al., 2020). Findings also suggest that the attitude of GPs provoked a sense of disregard, lack of compassion, and left adolescents feeling that they were not being heard (Corry and Leavey, 2017).
Findings from this study also suggest that adolescents experience positive experiences when accessing primary care services. Confidentiality and friendliness were common indicators and were expressed as being important by many adolescents in various settings (Matich et al., 2015). Adolescents placed great value on services that are youth friendly, welcoming, attentive, and non-judgemental. These findings are consistent with previous studies on help-seeking among young adults (Ambresin et al., 2013; Dalton et al., 2023), whereby positive attitudes and positive perceptions of contact with their GP facilitated help-seeking.
GPs can play an important role in providing guidance and advice to adolescents who seek help. Therefore, communicating with adolescents requires specific knowledge, experience, and skills. According to the WHO (2017), a youth-friendly service should consist of a healthcare system offering flexibility, confidentiality, affordability, and quality health care. It appears from the review that when a positive relationship is experienced, adolescents feel more satisfied with the service.
The overall findings indicate that adolescents want GP services that are non-judgemental, accessible, acceptable, appropriate, effective, and youth friendly. Therefore, there needs to be a shift beyond clinic-based care and a move towards adolescent designed, integrated, interventions on risk, awareness, and help-seeking advice.
School-based interventions have recently been highlighted as being effective in enhancing adolescents’ knowledge, attitudes, and health behaviours, and in creating healthy environments (Xu et al., 2020). This demonstrates the necessity of expanding the accessibility of youth-friendly services, support, and help-seeking activities among adolescents in schools. The involvement of school community members such as parents, teachers, and principals may contribute to a sustainable mechanism for programme implementation on risk health behaviour and help-seeking (Shackleton et al., 2016).
In recent years, there has been increasing demands for participation of adolescents and young people in programme and policy development (Chandra-Mouli et al., 2018). Their participation as co-researchers demands ample resources from GP-led primary care services. Therefore, adolescents should not only be viewed as participants, but also as equal partners and contributors in planning and implementation of such interventions (Fløtten et al., 2020).
Study limitations
The reviewed studies have some methodological limitations. Studies were conducted in High and Very High-income countries. Such countries were chosen as healthcare systems differ among Medium, Low, and Very Low Human Development Index countries. This limits generalizability of findings. Self-reported data from studies also limit generalizability of findings. The search strategy may not have captured all relevant studies since only four databases were searched. We did not include unpublished articles and excluded studies published in other languages, and hence, there is a possibility that we may not have included all studies conducted in this area. There is also possibility of outcome reporting bias since only findings relating to barriers and enablers for access to GP-led services were extracted and synthesized. Future studies in this area need to be designed taking such limitations into consideration to ensure high-quality evidence that is reproducible and generalizable.
Implications for practice
Review findings indicate that services can be improved by providing longer operating hours, walk-in services, free services, central locations, and non-judgemental care. Findings from this review provide important guidance for GPs who wish to improve ways they respond to adolescents’ needs. Adolescents should be involved in the process of change and service delivery. Our findings show that primary care services require a more adolescent-friendly approach, addressing confidentiality and privacy. A final component is provision of interventions that are designed to reduce stigma associated with accessing primary care services and delay or failure in utilizing early adolescent development services. Nevertheless, barriers and enablers may vary across different points of help-seeking process; therefore, a longitudinal study is needed at each level of the help-seeking process to advance development of youth-friendly services.
Conclusion
Adolescents often face issues of trust, confidentiality, and uncertainty when accessing GP-led primary care services, which may lead to reluctance and lack of engagement with GPs. This, coupled with structural barriers such as cost and long waiting times, may impede help-seeking for various health concerns. Findings from this review highlight the need for appropriate and affordable youth-friendly services. Such services require approachable and respectful staff, hours operating outside of school time, private waiting rooms, and well-informed GPs with good communication skills. Adolescents’ perspectives ought to be elicited to better understand the best approaches to develop and deliver youth-friendly primary care services. This can be achieved by sourcing creative and sustainable ways for involving adolescents in service development.
Supplemental Material
Supplemental Material - Adolescents’ perspectives and experiences of accessing general practitioner services: A systematic review
Supplemental Material for Adolescents’ perspectives and experiences of accessing general practitioner services: A systematic review by Stephanie M Lawrence, Mohamad M Saab, Eileen Savage, Josephine Hegarty, and Serena Fitzgerald in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.